Parental Self-Efficacy as a Predictor of Children’s Nutrition and the Potential Mediator Effect between the Health Promotion Program “Join the Healthy Boat” and Children’s Nutrition


 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Intervention
2.2. Study Design
2.3. Ethics Approval and Consent to Participate
2.4. Study Population
2.5. Instruments
2.6. Data Analysis
3. Results
3.1. Parental Self-Efficacy as a Predictor of Children’s Nutrition
3.1.1. Parental Self-Efficacy as a Predictor of Children’s Fruit and Vegetable Intake
3.1.2. Parental Self-Efficacy as a Predictor of Children’s Consumption of Sugar Sweetened Beverages
3.2. Parental Self-Efficacy as a Mediator between the Intervention “Join the Healthy Boat” and Children’s Nutrition
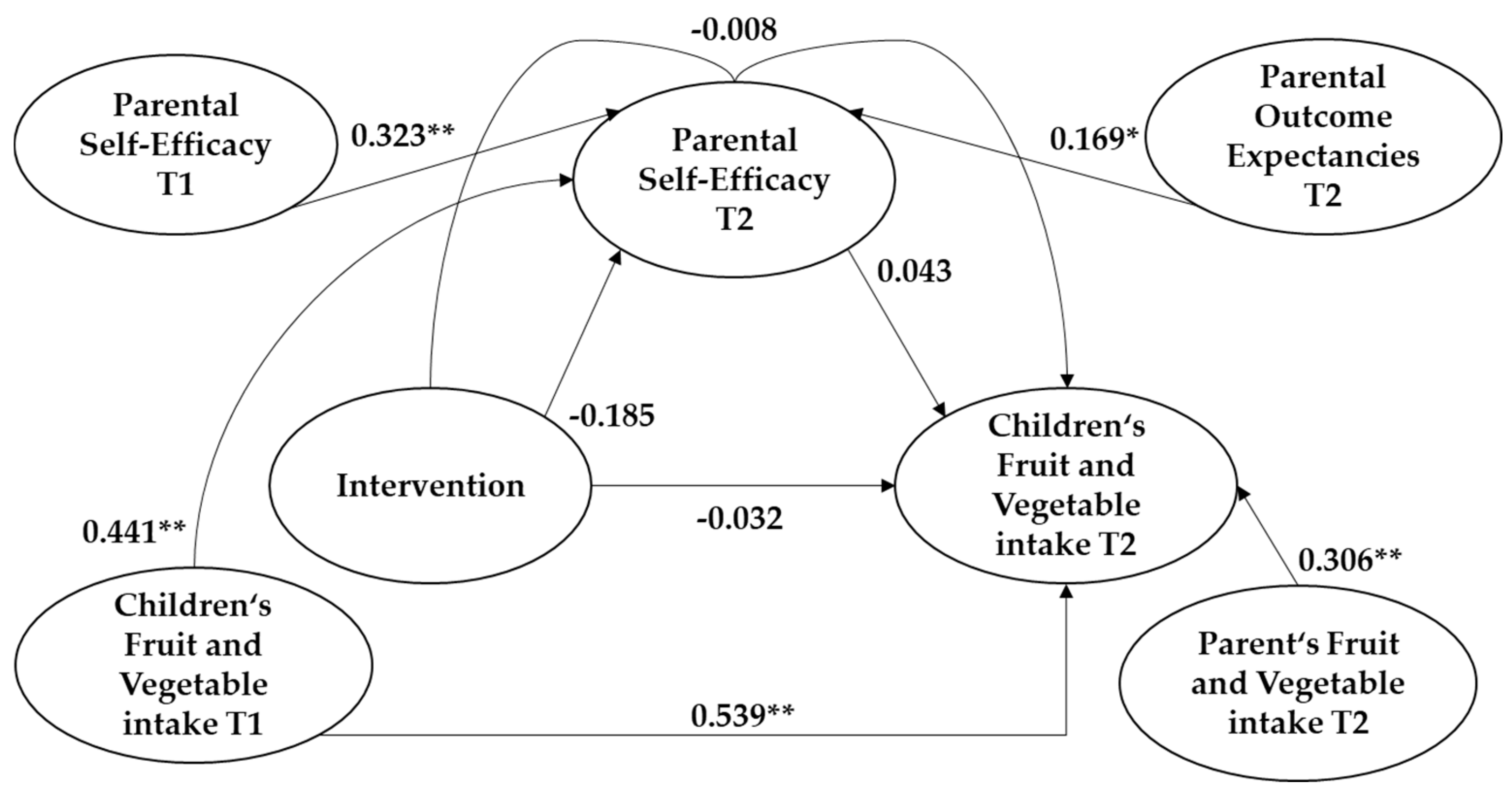
3.2.1. Parental Self-Efficacy as a Mediator between the Intervention “Join the Healthy Boat” and Children’s Fruit and Vegetable Intake
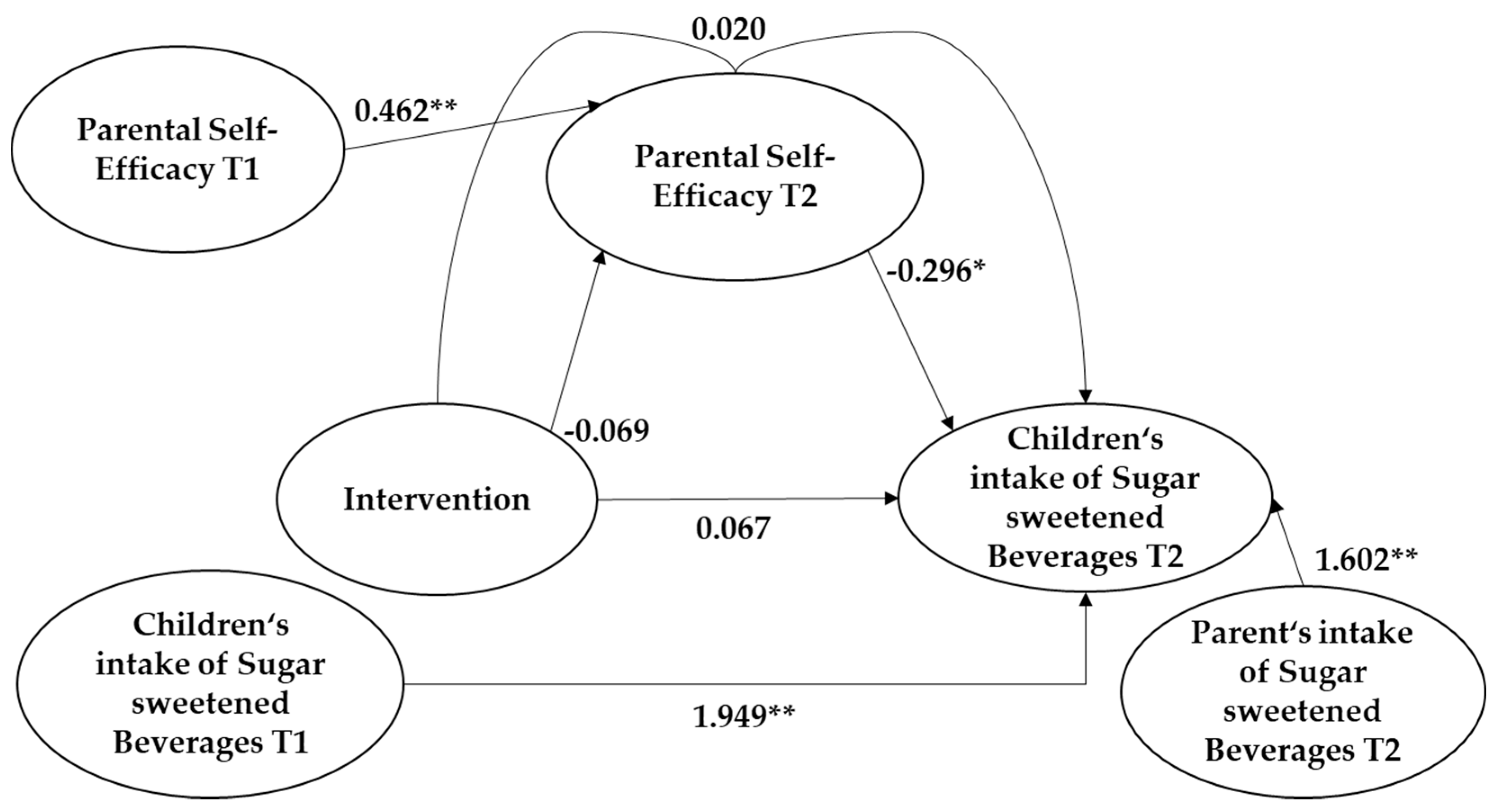
3.2.2. Parental Self-Efficacy as a Mediator between the Intervention “Join the Healthy Boat” and Children’s Fruit and Vegetable Intake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases: Country Profiles 2018; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/nmh/publications/ncd-profiles-2018/en/ (accessed on 14 October 2020).
- World Health Organization. World Health Organization. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2014; Available online: http://www.who.int/nmh/publications/ncd-status-report-2014/en/ (accessed on 14 October 2020).
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Nour, M.M.; Lutze, S.A.; Grech, A.; Allman-Farinelli, M. The Relationship between Vegetable Intake and Weight Outcomes: A Systematic Review of Cohort Studies. Nutrients 2018, 10, 1626. [Google Scholar] [CrossRef] [Green Version]
- Yingli, F.; Fan, Y.; Zhang, X.; Hou, W.; Tang, Z. Fruit and vegetable intake and risk of type 2 diabetes mellitus: Meta-analysis of prospective cohort studies. BMJ Open 2014, 4, e005497. [Google Scholar] [CrossRef] [Green Version]
- Robertson, A.; Tirado, C.; Lobstein, T.; Jermini, M.; Knai, C.; Jensen, J.H.; Ferro-Luzzi, A.; James, W.P.T. Food and Health in Europe: A New Basis for Action; World Health Organization: Copenhagen, Denmark, 2004; pp. 7–91. Available online: https://www.euro.who.int/__data/assets/pdf_file/0005/74417/E82161.pdf (accessed on 14 October 2020).
- Miedema, M.D.; Petrone, A.; Shikany, J.M.; Greenland, P.; Lewis, C.E.; Pletcher, M.J.; Gaziano, J.M.; Djoussé, L. Association of Fruit and Vegetable Consumption During Early Adulthood With the Prevalence of Coronary Artery Calcium After 20 Years of Follow-Up: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Circulation 2015, 132, 1990–1998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Hu, F.B. Sugar-Sweetened Beverages, Obesity, Type 2 Diabetes Mellitus, and Cardiovascular Disease Risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Fox, C.S.; Jacques, P.F.; Speliotes, E.K.; Hoffmann, U.; Smith, C.E.; Saltzman, E.; McKeown, N.M. Sugar-sweetened beverage, diet soda, and fatty liver disease in the Framingham Heart Study cohorts. J. Hepatol. 2015, 63, 462–469. [Google Scholar] [CrossRef] [Green Version]
- Robert-Koch-Institut. Gesundheit in Deutschland; Robert-Koch-Institut: Berlin, Germany, 2015; pp. 194–201. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GesInDtld/gesundheit_in_deutschland_2015.pdf?__blob=publicationFile (accessed on 14 October 2020).
- Nyaradi, A.; Li, J.; Hickling, S.; Foster, J.; Oddy, W.H. The role of nutrition in children’s neurocognitive development, from pregnancy through childhood. Front. Hum. Neurosci. 2013, 7, 97. [Google Scholar] [CrossRef] [Green Version]
- Koletzko, M.B.; Speer, C.P.; Gahr, M. Grundlagen der Ernährung im Kindes- und Jugendalter. In Pädiatrie, 3rd ed.; Speer, C.P., Gahr, M., Eds.; Springer Medizin: Heidelberg, Germany, 2009; pp. 67–83. [Google Scholar]
- Gale, C.R.; Martyn, C.N.; Marriott, L.D.; Limond, J.; Crozier, S.R.; Inskip, H.M.; Godfrey, K.M.; Law, C.; Cooper, C.; Robinson, S.; et al. Dietary patterns in infancy and cognitive and neuropsychological function in childhood. J. Child Psychol. Psychiatry 2009, 50, 816–823. [Google Scholar] [CrossRef] [Green Version]
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, 4–85. [Google Scholar] [CrossRef]
- Schienkiewitz, A.; Brettschneider, A.K.; Damerow, S.; Schaffrath-Rosario, A. Overweight and obesity among children and adolescents in Germany. Results of the cross-sectional KiGGS Wave 2 study and trends. J. Health Monit. 2018, 3, 16–23. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Wabitsch, M.; Moss, A.; Kromeyer-Hauschild, K. Unexpected plateauing of childhood obesity rates in developed countries. BMC Med. 2014, 12, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of Obesity and Severe Obesity in US Children, 1999–2016. Pediatric 2018, 141, e20173459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the Development of Children’s eating behaviors: From Infancy to Adolescence. Can. J. Dietic Pract. Res. 2007, 68, 1–56. [Google Scholar]
- Jones, R.E.; Jewell, J.; Saksena, R.; Salas, X.R.; Breda, J. Overweight and Obesity in Children under 5 Years: Surveillance Opportunities and Challenges for the WHO European Region. Front. Public Health 2017, 5, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaglioni, S.; Arrizza, C.; Vecchi, F.; Tedeschi, S. Determinants of children’s eating behavior. Am. J. Clin. Nutr. 2011, 94, 2006S–2011S. [Google Scholar] [CrossRef]
- Zahid, A.; Davey, C.; Reicks, M. Beverage Intake among Children: Associations with Parent and Home-Related Factors. Int. J. Environ. Res. Public Health 2017, 14, 929. [Google Scholar] [CrossRef] [Green Version]
- Østbye, T.; Malhotra, R.; Stroo, M.; Lovelady, C.; Brouwer, R.; Zucker, N.; Fuemmeler, B. The effect of the home environment on physical activity and dietary intake in preschool children. Int. J. Obes. 2013, 37, 1314–1321. [Google Scholar] [CrossRef] [Green Version]
- Harris, T.; Ramsey, M. Paternal modeling, household availability, and paternal intake as predictors of fruit, vegetable, and sweetened beverage consumption among African American children. Appetite 2015, 85, 171–177. [Google Scholar] [CrossRef]
- Cooke, L.J.; Wardle, J.; Gibson, E.L.; Sapochnik, M.; Sheiham, A.; Lawson, M. Demographic, familial and trait predictors of fruit and vegetable consumption by pre-school children. Public Health Nutr. 2004, 7, 295–302. [Google Scholar] [CrossRef]
- Jones, T.L.; Prinz, R.J. Potential roles of parental self-efficacy in parent and child adjustment: A review. Clin. Psychol. Rev. 2005, 25, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy. In Encyclopedia of Human Behavior; Ramachaudran, V.S., Ed.; Academic Press: New York, NY, USA, 1994; Volume 4, pp. 71–81. [Google Scholar]
- Herschbach, P. Gesundheitsverhalten. In Gesundheitsverhalten; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 1999; pp. 26–85. [Google Scholar]
- Hohmann, C.; Schwarzer, R. Selbstwirksamkeitserwartung. In Handbuch der Gesundheitspsychologie und Medizinischen Psychologie; Bengel, J., Jerusalem, M., Eds.; Hogrefe: Goettingen, Germany, 2009; pp. 61–67. [Google Scholar]
- Schwarzer, R.; Renner, B. Health-specific Self-Efficacy Scales. 2009. Available online: https://userpage.fu-berlin.de/~health/healself.pdf (accessed on 14 October 2020).
- Hevey, D.; Smith, M.; McGee, H. Self-efficacy and health behaviour: A review. Ir. J. Psychol. 1998, 19, 248–273. [Google Scholar] [CrossRef]
- Albanese, A.M.; Russo, G.R.; Geller, P.A. The role of parental self-efficacy in parent and child well-being: A systematic review of associated outcomes. Child Care Health Dev. 2019, 45, 333–363. [Google Scholar] [CrossRef] [PubMed]
- Coleman, P.K.; Karraker, K.H. Self-Efficacy and Parenting Quality: Findings and Future Applications. Dev. Rev. 1998, 18, 47–85. [Google Scholar] [CrossRef]
- Finlayson, T.L.; Siefert, K.; Ismail, A.I.; Sohn, W. Maternal self-efficacy and 1–5-year-old children’s brushing habits. Community Dent. Oral Epidemiol. 2007, 35, 272–281. [Google Scholar] [CrossRef] [PubMed]
- Rohde, J.F.; Bohman, B.; Berglind, D.; Hansson, L.M.; Frederiksen, P.; Mortensen, E.L.; Heitmann, B.L.; Rasmussen, F. Cross-sectional associations between maternal self-efficacy and dietary intake and physical activity in four-year-old children of first-time Swedish mothers. Appetite 2018, 125, 131–138. [Google Scholar] [CrossRef]
- Erkelenz, N.; Schreiber, A.C.; Kobel, S.; Kettner, S.; Drenowatz, C.; Steinacker, J.M. Relationship of parental health-related behaviours and physical fitness in girls and boys. J. Public Health 2014, 22, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Russell, C.G.; Worsley, A. Why don’t they like that? And can I do anything about it? The nature and correlates of parents’ attributions and self-efficacy beliefs about preschool children’s food preferences. Appetite 2013, 66, 34–43. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.; Hesketh, K.; Silverii, A.; Abbott, G. Maternal self-efficacy regarding children’s eating and sedentary behaviours in the early years: Associations with children’s food intake and sedentary behaviours. Pediatr. Obes. 2010, 5, 501–508. [Google Scholar] [CrossRef]
- Rübenach, S. 2.2. Kindertagesbetreuung. In Auszug aus dem Datenreport 2018: Familie, Lebensformen und Kinder; Statistisches, B., Ed.; Statistisches Bundesamt: Wiesbaden, Germany, 2018; pp. 66–68. Available online: https://www.wzb.eu/system/files/docs/sv/iuk/dr2018_Kap_12_nachspann_1.pdf (accessed on 14 October 2020).
- Zimmer, R. Gesundheitsförderung im Kindergarten. Bundesgesundheitsblatt-Gesundh.-Gesundh. 2002, 45, 964–969. [Google Scholar] [CrossRef]
- Bartholomew, L.K.; Parcel, G.S.; Kok, G.; Gottlieb, N.H. Intervention mapping steps. In Planning Health Promotion Programs: An Intervention Mapping Approach, 2nd ed.; Bartholomew, L.K., Parcel, G.S., Kok, G., Gottlieb, N.H., Eds.; Jossey-Bass: San Francisco, CA, USA, 2006; pp. 191–472. [Google Scholar]
- Bandura, A. Social Cognitive Theory: An Agentic Perspective. Asian J. Soc. Psychol. 1999, 2, 21–41. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ökologische Sozialisationsforschung–Ein Bezugsrahmen. In Handbuch Bildungs- und Erziehungssoziologie; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2012; pp. 167–176. [Google Scholar]
- Wartha, O.; Kobel, S.; Lämmle, O.; Mosler, S.; Steinacker, J.M. Entwicklung eines settingspezifischen Gesundheitsförderprogramms durch die Verwendung des Intervention-Mapping-Ansatzes: Komm mit in das gesunde Boot–Kindergarten. Prävention Gesundh. 2016, 11, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Wartha, O.; Lämmle, C.; Kobel, S.; Wirt, T.; Steinacker, J.M. Aufbau des Bewegungsmoduls des schulbasierten Gesundheitsförderprogramms Komm mit in das gesunde Boot. Ger. J. Sports Med. 2017, 2017, 20–26. [Google Scholar] [CrossRef]
- Kobel, S.; Wartha, O.; Wirt, T.; Dreyhaupt, J.; Lämmle, C.; Friedemann, E.-M.; Kelso, A.; Kutzner, C.; Hermeling, L.; Steinacker, J.M. Design, Implementation, and Study Protocol of a Kindergarten-Based Health Promotion Intervention. BioMed Res. Int. 2017, 2017, 4347675. [Google Scholar] [CrossRef]
- Kobel, S.; Wartha, O.; Lämmle, C.; Dreyhaupt, J.; Steinacker, J.M. Intervention effects of a kindergarten-based health promotion programme on obesity related behavioural outcomes and BMI percentiles. Prev. Med. Rep. 2019, 15, 100931. [Google Scholar] [CrossRef] [PubMed]
- Kurth, B.M.; Kamtsiuris, P.; Hölling, H.; Schlaud, M.; Dölle, R.; Ellert, U.; Kahl, H.; Knopf, H.; Lange, M.; Mensink, G.B.; et al. The challenge of comprehensively mapping children’s health in a nation-wide health survey: Design of the German KiGGS-Study. BMC Public Health 2008, 8, 196. [Google Scholar] [CrossRef] [Green Version]
- Bohman, B.; Rasmussen, F.; Ghaderi, A. Development and psychometric evaluation of a context-based parental self-efficacy instrument for healthy dietary and physical activity behaviors in preschool children. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 110. [Google Scholar] [CrossRef] [Green Version]
- Statistisches Bundesamt (DESTATIS). Population and Employment. Population with Migration Background. Results of the Microcensus. 2018. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Migration-Integration/Publikationen/Downloads-Migration/migrationshintergrund-2010220187004.pdf?__blob=publicationFile (accessed on 10 May 2020).
- Settelmeyer, A.; Erbe, J. Migrationshintergrund: Zur Operationalisierung des Begriffs in der Berufsbildungsforschung; Schriftenreihe des Bundesinstituts für Berufsbildung Bonn: Bonn, Germany, 2010; Volume 112, pp. 5–39. Available online: https://www.bibb.de/dokumente/pdf/wd_112_migrationshintergrund.pdf (accessed on 14 October 2020).
- Brauns, H.; Steinmann, S. Educational reform in France, West-Germany and the United Kingdom: Updating the CASMIN educational classification. ZUMA Nachr. 1999, 23, 7–44. Available online: https://nbn-resolving.org/urn:nbn:de:0168-ssoar-208169 (accessed on 14 October 2020).
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; SAGE: London, UK, 2009; pp. 131–315. [Google Scholar]
- Backhaus, K.; Erichson, B.; Plinke, W.; Weiber, R. Regressionsanalyse; Springer: Berlin/Heidelberg, Germany, 2015; pp. 63–134. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson: Edinburgh, UK, 1983; pp. 153–555. [Google Scholar]
- Schenk, L.; Anton, V.; Baer, N.-R.; Schmitz, R. Ernährungsmuster von Kindern und Jugendlichen mit Migrationshintergrund: Ergebnisse der KiGGS-Studie. Public Health Forum 2016, 24, 205–208. [Google Scholar] [CrossRef]
- Hayes, A.F. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modelling. White Paper. 2012. Available online: http://ww.afhayes.com/public/process2012.pdf (accessed on 14 October 2020).
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F.; Cai, L. Using heteroskedasticity-consistent standard error estimators in OLS regression: An introduction and software implementation. Behav. Res. Methods 2007, 39, 709–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krug, S.; Finger, J.D.; Lange, C.; Richter, A.; Mensink, G.B.M. Sport- und Ernährungsverhalten bei Kindern und Jugendlichen in Deutschland–Querschnittergebnisse aus KiGGS Welle 2 und Trends. J. Health Monit. 2018, 3, 3–22. [Google Scholar] [CrossRef]
- Kuntz, B.; Waldhauer, J.; Zeiher, J.; Finger, J.D.; Lampert, T. Soziale Unterschiede im Gesundheitsverhalten von Kindern und Jugendlichen in Deutschland–Querschnittergebnisse aus KiGGS-Welle 2. J. Health Monit. 2018, 3, 45–63. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsJ/Focus/JoHM_02_2018_Unterschiede_Gesundheitsverhalten_KiGGS-Welle2.pdf?__blob=publicationFile (accessed on 14 October 2020).
- Kleiser, C.; Mensink, G.B.M.; Scheidt-Nave, C.; Kurth, B.-M. HuSKY: A healthy nutrition score based on food intake of children and adolescents in Germany. Br. J. Nutr. 2009, 102, 610–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabenberg, M.; Mensink, G. Limo, Saft & Co–Konsum zuckerhaltiger Getränke in Deutschland; Robert, K.-I., Ed.; GBE kompakt: Berlin, Germany, 2013; Volume 4, pp. 1–9. [Google Scholar] [CrossRef]
- Kleiser, C.; Mensink, G.B.M.; Neuhauser, H.; Schenk, L.; Kurth, B.-M. Food intake of young people with a migration background living in Germany. Public Health Nutr. 2009, 13, 324–330. [Google Scholar] [CrossRef] [Green Version]
- Schenk, L.; Neuhauser, H.; Ellert, U.; Poethko-Müller, C.; Kleiser, C.; Mensink, G. Kinder- und Jugendgesundheitssurvey (KiGGS) 2003–2006: Kinder und Jugendliche mit Migrationshintergrund; Robert-Koch-Institut: Berlin, Germany, 2008; pp. 43–51. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsB/KiGGS_migration.pdf?__blob=publicationFile (accessed on 14 October 2020).
- Koschollek, C.; Bartig, S.; Rommel, A.; Santos-Hövener, C.; Lampert, T. The health of children and adolescents with a migration background in Germany—Results of the cross-sectional KiGGS Wave 2 study. J. Health Monit. 2019, 4, 7–28. [Google Scholar] [CrossRef]
- Schwarzer, R.; Fuchs, R. Changing risk behaviors and adopting health behaviors: The role of self-efficacy beliefs. In Self-Efficacy in Changing Societies; Cambridge University Press (CUP): Cambridge, UK, 1995; pp. 259–288. [Google Scholar]
- Williams, D.M. Outcome Expectancy and Self-Efficacy: Theoretical Implications of an Unresolved Contradiction. Pers. Soc. Psychol. Rev. 2010, 14, 417–425. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997; pp. 1–35. [Google Scholar]
- Corcoran, K.J.; Rutledge, M.W. Efficacy expectation changes as a function of hypothetical incentives in smokers. Psychol. Addict. Behav. 1989, 3, 22–28. [Google Scholar] [CrossRef]
- Kirsch, I. Efficacy expectations or response predictions: The meaning of efficacy ratings as a function of task characteristics. J. Pers. Soc. Psychol. 1982, 42, 132–136. [Google Scholar] [CrossRef]
- Dreyhaupt, J.; Koch, B.; Wirt, T.; Schreiber, A.; Brandstetter, S.; Kesztyüs, D.; Wartha, O.; Kobel, S.; Kettner, S.; Prokopchuk, D.; et al. Evaluation of a health promotion program in children: Study protocol and design of the cluster-randomized Baden-Württemberg primary school study [DRKS-ID: DRKS00000494]. BMC Public Health 2012, 12, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Rucker, D.D.; Preacher, K.J.; Tormala, Z.L.; Petty, R.E. Mediation Analysis in Social Psychology: Current Practices and New Recommendations. Soc. Pers. Psychol. Compass 2011, 5, 359–371. [Google Scholar] [CrossRef]
- Zhao, X.; Lynch, J.G.; Chen, Q. Reconsidering Baron and Kenny: Myths and Truths about Mediation Analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Krause, M.R.; Serlin, R.C.; Ward, S.; Rony, R.Y.Z.; Ezenwa, M.O.; Naab, F. Testing Mediation in Nursing Research. Nurs. Res. 2010, 59, 288–294. [Google Scholar] [CrossRef]
- Fritz, M.S.; MacKinnon, D.P. Required Sample Size to Detect the Mediated Effect. Psychol. Sci. 2007, 18, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F.; Scharkow, M. The Relative Trustworthiness of Inferential Tests of the Indirect Effect in Statistical Mediation Analysis. Psychol. Sci. 2013, 24, 1918–1927. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Missing Values | Intervention (n = 318) | Control (n = 240) | Total (n = 558) |
|---|---|---|---|---|
| Children | ||||
| Age at follow-up [m, sd] | 3 | 4.7 (0.6) | 4.6 (0.6) | 4.7 (0.6) |
| Boys [n, %] 1 | 113 (47.1) | 179 (56.3) | 292 (52.3) | |
| Migration background [n, %] 1 | 106 | 77 (30.6) | 74 (37.0) | 151 (33.4) |
| Fruit and vegetable intake * T1 [m, sd] | 92 | 2.5 (0.9) | 2.7 (0.7) | 2.6 (0.8) |
| Fruit and vegetable intake * T2 [m, sd] | 166 | 2.6 (0.8) | 2.7 (0.8) | 2.6 (0.8) |
| Sugar sweetened beverages once a week or more T1 [n, %] | 94 | 101 (38.5) | 77 (38.1) | 178 (38.4) |
| Sugar sweetened beverages once a week or more T2 [n, %] | 161 | 85 (38.6) | 60 (33.9) | 145 (36.5) |
| Parents | ||||
| Tertiary family education level [n, %] | 106 | 120 (47.2) | 100 (50.5) | 220 (48.7) |
| Fruit and vegetable intake * T2 [m, sd] | 168 | 2.4 (0.7) | 2.5 (0.7) | 2.4 (0.7) |
| At least one parent drinks sugar sweetened beverages once a week or more T2 [n, %] | 162 | 127 (57.7) | 106 (60.2) | 233 (58.8) |
| Self-efficacy on children’s fruit and vegetable intake T1 [m, sd] | 95 | 4.9 (1.6) | 4.9 (1.4) | 4.9 (1.5) |
| Self-efficacy on children’s fruit and vegetable intake T2 [m, sd] | 163 | 4.8 (1.4) | 5.0 (1.3) | 4.9 (1.4) |
| Self-efficacy on children’s sugar sweetened beverage intake T1 [m, sd] | 99 | 4.9 (1.5) | 5.0 (1.4) | 4.9 (1.4) |
| Self-efficacy on children’s sugar sweetened beverage intake T2 [m, sd] | 168 | 4.9 (1.4) | 5.1 (1.2) | 5.0 (1.3) |
| Outcome expectancies on children’s sugar sweetened beverage intake T1 [m, sd] | 162 | 6.3 (0.7) | 6.2 (0.8) | 6.3 (0.7) |
| Outcome expectancies on children’s fruit and vegetable intake T2 [m, sd] | 161 | 6.0 (0.8) | 5.8 (0.9) | 5.9 (0.8) |
| Variables | B [95% CI] | SE(B) | β | t | p |
|---|---|---|---|---|---|
| Constant | 0.744 [−0.126; 1.614] | 0.442 | 1.682 | 0.094 | |
| Parents | |||||
| Self-efficacy | 0.137 [0.083; 0.190] | 0.027 | 0.237 | 5.005 | <0.001 |
| Fruit and vegetable intake | 0.494 [0.391; 0.597] | 0.052 | 0.451 | 9.466 | <0.001 |
| Outcome expectancies | 0.015 [−0.071; 0.101] | 0.044 | 0.016 | 0.341 | 0.733 |
| Tertiary family education level | 0.090 [−0.050; 0.230] | 0.071 | 0.060 | 1.263 | 0.207 |
| Children | |||||
| Age | −0.034 [−0.152; 0.084] | 0.060 | −0.027 | −0.569 | 0.570 |
| Gender | 0.051 [−0.088; 0.190] | 0.071 | 0.034 | 0.727 | 0.468 |
| Migration background | 0.004 [−0.148; 0.156] | 0.077 | 0.002 | 0.053 | 0.958 |
| Variables | B(SE) | p | OR (95% CI) |
|---|---|---|---|
| Constant | 0.458 (1.587) | 0.773 | 1.581 |
| Parents | |||
| Self-efficacy | −0.318 (0.103) | 0.002 | 0.728 (0.594; 0.891) |
| Intake of sugar sweetened beverages | 1.972 (0.313) | <0.001 | 7.188 (3.896; 13.264) |
| Outcome expectancies | −0.110 (0.179) | 0.537 | 0.896 (0.631; 1.271) |
| Tertiary family education level | −0.540 (0.267) | 0.043 | 0.583 (0.345; 0.984) |
| Children | |||
| Age | 0.248 (0.224) | 0.269 | 1.281 (0.826; 1.988) |
| Gender | −0.758 (0.268) | 0.005 | 0.469 (0.277; 0.793) |
| Migration background | 0.452 (0.285) | 0.112 | 1.572 (0.900; 2.746) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Möhler, R.; Wartha, O.; Steinacker, J.M.; Szagun, B.; Kobel, S. Parental Self-Efficacy as a Predictor of Children’s Nutrition and the Potential Mediator Effect between the Health Promotion Program “Join the Healthy Boat” and Children’s Nutrition. Int. J. Environ. Res. Public Health 2020, 17, 9463. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249463
Möhler R, Wartha O, Steinacker JM, Szagun B, Kobel S. Parental Self-Efficacy as a Predictor of Children’s Nutrition and the Potential Mediator Effect between the Health Promotion Program “Join the Healthy Boat” and Children’s Nutrition. International Journal of Environmental Research and Public Health. 2020; 17(24):9463. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249463
Chicago/Turabian StyleMöhler, Ricarda, Olivia Wartha, Jürgen Michael Steinacker, Bertram Szagun, and Susanne Kobel. 2020. "Parental Self-Efficacy as a Predictor of Children’s Nutrition and the Potential Mediator Effect between the Health Promotion Program “Join the Healthy Boat” and Children’s Nutrition" International Journal of Environmental Research and Public Health 17, no. 24: 9463. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249463