Results of Nurse Case Management in Primary Heath Care: Bibliographic Review


 ,
,  , ,
, ,
Abstract
:1. Introduction
Background
2. Methods
2.1. Study Design
2.2. Search Strategy
2.3. Selection Criteria
2.4. Research Variables
2.5. Methodological Quality and Level Of Evidence
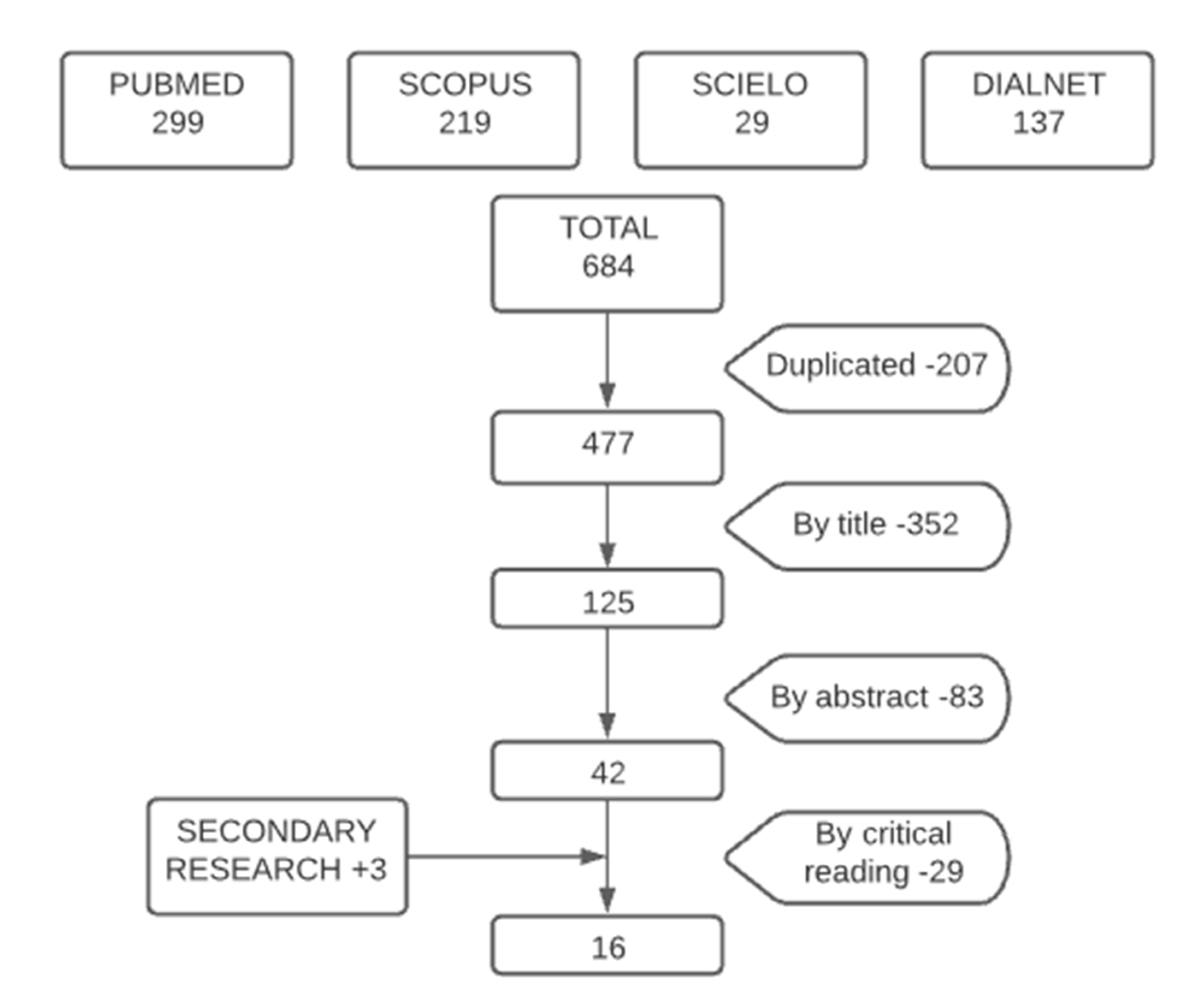
2.6. The Selection Process of the Studies
3. Results
3.1. Health Effects: Efficacy Results on Patients with Chronic Diseases
3.2. Profitability Results: Efficiency
4. Discussion
4.1. Health Results: Effectiveness
4.2. Profitability Results: Efficiency
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Consejo Económico y Social. Desarrollo Autonómico, Competitividad y Cohesión Social en el Sistema Sanitario. Madrid, 2010, 01. Available online: http://www.ces.es/documents/10180/18510/Inf0110/a13da181-b58e-4256-a90c-bb8693f215b8 (accessed on 15 August 2020).
- Consejo General de Enfermeria. Madrid: Consejo General de Colegios Oficiales de Enfermería de España. 2015. Available online: https://www.consejogeneralenfermeria.org/sala-de-prensa/noticias/item/16720-la-oms-ratifica-que-en-espana-faltan-enfermeras (accessed on 15 August 2020).
- Bernal-Delgado, E.; García-Arnesto, S.; Oliva, J.; Sánchez Martínez, F.; Repullo, J.R.; Peña-Longobardo, L.M.; Ridao-López, M.; Hernández-Quevedo, C. España: Informe del Sistema Sanitario. Sistemas Sanitarios en Transición 2018, 20, 1–179. Available online: https://www.mscbs.gob.es/biblioPublic/publicaciones/recursos_propios/resp/pdf/REVISION_SISTEMA_SANITARIO_ESPANOL_2018.pdf (accessed on 18 August 2020).
- Sánchez-Martín, C.I. Cronicidad y complejidad: Nuevos roles en Enfermería. Enfermeras de Práctica Avanzada y paciente crónico. Enferm. Clínic 2013, 24, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Gómez Sánchez, M.C. Intervención de la enfermera gestora de casos durante el ingreso hospitalario de pacientes con infección VIH. Rev. Esp. Salud. Pública 2011, 3, 237–244. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1135-57272011000300002 (accessed on 20 August 2020). [CrossRef] [PubMed] [Green Version]
- Morales-Asencio, J.M. Gestión de casos y cronicidad compleja: Conceptos, modelos, evidencias e incertidumbres. Enferm. Clínic 2013, 24, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Valverde Jiménez, M.R.; Hernández Corominas, M.A. Modelo de gestión de casos e investigación. Enferm. Glob. 2012, 11, 246–250. [Google Scholar] [CrossRef] [Green Version]
- Yeoh, E.K.; Wong, M.C.S.; Wong, E.L.Y.; Yam, C.; Poon, C.M.; Chung, R.Y.; Chong, M.; Fang, Y.; Wang, H.H.X.; Liang, M.; et al. Benefits and limitations of implementing Chronic Care Model (CCM) in PHC programs: A systematic review. Int. J. Cardiol. 2018, 1, 279–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uittenbroek, R.J.; van der Mei, S.F.; Reijneveld, S.A. Experiences of case manageners in providing person-centered and integrated care base on the Chronic care model: A qualitative study on embrace. PLoS ONE 2018, 13, e0207109. [Google Scholar] [CrossRef]
- Valverde Jiménez, M.R.; López Benavente, Y.; Hernández Corominas, M.A.; Gómez Ruiz, M.; Blázquez Pedrero, M.; Echevarría Pérez, P. Enfermera Gestora de Casos del Servicio Murciano de Salud: Un año de puesta en marcha del programa. Enferm. Glob. 2014, 13, 57–69. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1695-61412014000400004 (accessed on 25 August 2020). [CrossRef] [Green Version]
- García-Fernández, F.P.; Arrabal Orpez, M.J.; Rodríguez Torres, M.C.; Gila Selas, C.; Carrascosa García, I.; Laguna Parras, J.M. Influencia de las enfermeras gestoras de casos en la calidad de vida de las cuidadoras de pacientes pluripatológicos. Gerokomos 2014, 25, 68–71. [Google Scholar] [CrossRef] [Green Version]
- U.S. National Library of Medicine (NIH). Medical Subject Headings (MeSH). 2019. Available online: https://meshb.nlm.nih.gov/search (accessed on 20 August 2020).
- Centro Latinoamericano y del Caribe de Información en Ciencias de la Salud (BIREME). Descriptores en Ciencias de la Salud (DeCS). 2018. Available online: http://decs.bvs.br/E/homepagee.htm (accessed on 10 September 2020).
- Critical Appraisal Skills Programme Español (CASPe). 2018. Available online: http://www.redcaspe.org/ (accessed on 11 September 2020).
- Altman, D.G.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Declaración de la iniciativa STROBE (Strengthening the Reporting of Observational studies in Epidemiology): Directrices para la comunicación de estudios observacionales. Revisit. Esp. Salud Pública 2008, 22, 144–150. Available online: http://www.ee.lafe.san.gva.es/aulavirtual/file.php/95/CURSO_2017-2018/STROBE_short_Spanish.pdf (accessed on 20 August 2020).
- Scottish Intercollegiate Guidelines Network. Forming guideline recommendations. In SIGN 50: A Guideline Developer’s Handbook; SIGN: Edinburgh, Scotland, 2008; Available online: https://www.sign.ac.uk/assets/sign50_2011.pdf (accessed on 22 August 2020).
- López Vallejo, M.; Puente Alcaraz, J. El proceso de institucionalización de la enfermera gestora de casos en España. Análisis comparativo entre los sistemas autonómicos de salud. Enferm. Clinic 2019, 29, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Gómez, M.B.; Ramos-Santana, S.; Gómez-Salgado, J.; Sánchez-Nicolás, F.; Moreno-Garriga, C.; Duarte-Clíments, G. Benefits of advanced practice nursing for its expansion in the Spanish context. Int. J. Environ. Res. Public Health 2019, 16, 680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joo, J.Y.; Huber, D.L. Scoping Review of Nursing Case Management in the United States. Clin. Nurs. Res. 2017, 27, 1002–1016. [Google Scholar] [CrossRef] [PubMed]
- Reilly, S.; Miranda-Castillo, C.; Malouf, R.; Hoe, J.; Toot, S.; Challis, D.; Orrell, M. Case management approaches to home support for people with dementia. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Joo, J.Y.; Liu, M.F. Case management effectiveness in reducing hospital use: A systematic review. Int. Nurs. 2016, 64, 296–308. [Google Scholar] [CrossRef]
- Joo, J.Y.; Huber, D.L. Community-based case management effectiveness in populations that abuse substances. Int. Nurs. Rev. 2015, 62, 536–545. [Google Scholar] [CrossRef]
- Stokes, J.; Panagioti, M.; Alam, R.; Checkland, K.; Cheraghi-Sohi, S.; Bower, P. Effectiveness of case management for “At Risk” patients in PHC: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0132340. [Google Scholar] [CrossRef]
- Morales-Asencio, J.M.; Cuevas-Fernández-Gallego, M.; Morilla-Herrera, J.C.; Martín-Santos, F.J.; Silvano Arranz, A.; Batres Sicilia, J.P.; Delgado-Romero, A.; Palacios-Gómez, L.; Cejudo López, Á.; Kaknani-Uttumchandani, S. Características de la provisión del servicio de gestión de casos en el entorno comunitario en Andalucía a partir del registro RANGECOM. Enferm. Clin. 2019, 29, 67–73. [Google Scholar] [CrossRef]
- Tortajada, S.; Giménez-Campos, M.S.; Villar-López, J.; Faubel-Cava, R.; Donat-Castelló, L.; Valdivieso-Martínez, B.; Soriano-Melchor, E.; Bahamontes-Mulió, A.; García-Gómez, J.M. Case Management for Patients with Complex Multimorbidity: Development and Validation of a Coordinated Intervention Between Primary and Hospital Care. Int. J. Integr. Care 2017, 17, 4. [Google Scholar] [CrossRef] [Green Version]
- Castanho, R.; Mantovani, M.D.; Soriano, J. Nursing Case Management and Glycemic Control Among Brazilians with Type 2 Diabetes: Pragmatic Clinical Trial. Nurs. Res. 2015, 64, 272–281. [Google Scholar] [CrossRef]
- Ozpancar, N.; Pakyuz, S.C.; Topcu, B. Hypertension management: What is the role of case management? Rev. Esc. Enferm. USP 2017, 51, e03291. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Oh, S. Nurse Case Managers’ Experiences on Case Management for Long-term Hospitalization in Korea. Asian Nurs. Res. 2017, 11, 283–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherlowski Leal David, H.M.; Martínez-Riera, J.R.; Herraiz Mallebrera, A.; de Lima da Costa, M.F. A enfermeira gestora de casos na Espanha: Enfrentando o desafio da cronicidade por meio de uma prática integral. Ciênc. Saúde Coletiva 2020, 25, 315–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgel, B.J.; Devito, B.; Collins-Bride, G.; Sullivan, B.; Retzlaff, A.; Hyde, S. Nursing Case Management Strategies for Adults with Serious Mental Illness Seeking Dental Services. Issues Ment. Health Nurs. 2018, 39, 311–319. [Google Scholar] [CrossRef]
- Davisson, E.A.; Swanson, E.A. Patient and Nurse Experiences in a Rural Chronic Disease Management Program: A qualitative evaluation. Prof. Case Manag. 2018, 23, 10–18. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Data Base | Search Strings | Search Period | Obtained Articles | Selected Articles |
|---|---|---|---|---|
| PUBMED | (nurse) AND (case management) AND (chronic disease) AND (care management) | 2015–2020 | 299 | 6 |
| SCIELO | (nurse) AND (case manager) (nurse) AND (case management) (nurse) AND (case manager) AND (chronic disease) (case management) AND (nurse) | 2015–2020 | 0 + 7 + 1 + 21 = 29 | 1 |
| SCOPUS | (nurse) AND (case management) AND (chronic disease) | 2016–2020 | 219 | 4 |
| DIALNET | (nurse) AND (case management) (nurse) AND (case manager) AND (chronic disease) | 2015–2020 | 131 + 6 = 137 | 2 |
| SECONDARY SEARCH | 2014 *–2020 | 3 |
| Authors/Year/Country | Design/Sample | Aims | Variables | Results | Conclusions | Quality, Level of Evidence and Recommendation. |
|---|---|---|---|---|---|---|
| Valverde Jiménez et al., 2014. Spain. | Descriptive and cross-sectional, observational study.
|
| Sociodemographic and clinical profile of the target population. Caregiver overload. | Since the incorporation of the NCM, there has been an increase in the recording of both patient and caregiver assessments by patterns. |
| STROBE: 20/22 SIGN: 3 D |
| Castanho, de Fátima & Verdú, 2015. Brazil. | Clinical Trial. Sample: 80 patients, randomized sample. | Comparation nursing case management to usual care in the treatment of glycosylated hemoglobin in patients with type II diabetes mellitus. | Glycated hemoglobin at the beginning of the study, at 6 months and at 12 months. |
|
| CASPe: 7/11 SIGN: 1+ B |
| Stokes et al., 2015. United Kingdom. | Systematic review with meta-analysis. | To describe the effectiveness of the case management program in PHC risk patients. |
|
|
| CASPe: 9/10 SIGN: 1+ A |
| Reilly et al., 2015. United Kingdom. | Systematic review (only randomized controlled trials were included) | To summarize the results of health indicators of the health system. |
|
|
| CASPe: 9/10 SIGN: 1++ A |
| Joo & Liu, 2015. South Korea. | Systematic review (only randomized controlled trials were included). | To synthesize evidence of case management programs in patients with chronic diseases. |
|
|
| CASPe: 10/10 SIGN: 1+ A |
| Joo & Huber, 2016.United States. | Systematic review (only randomized controlled trials were included). | To summarize evidence of a substance abuse case management program in community settings. |
|
|
| CASPe: 9/10 SIGN: 1++ A |
| Tortajada et al., 2017 Spain. | Longitudinal cohort follow-up study Sample: 714 patients with complex multi-morbidity. | To analyze a case management program (patient assessment, education regarding prescribed medication or lifestyle, patient follow-up) |
|
|
| CASPe: 11/11 SIGN: 2++ B |
| López Vallejo & Puente Alcaraz, 2017. Spain. | Descriptive study
|
| Levels of NCM’s institutionalization: low, medium and advanced.
|
|
| STROBE: 16/22 SIGN: 4 D |
| Oh & Oh, 2017. South Korea. | Qualitative study Sample: 23 nurse case managers with three or more years of experience (in-depth interviews). |
|
|
|
| CASPe: 8/10 SIGN: 3 D |
| Joo & Huber, 2017.United States. | Scoping review. | To summarize the results of the case management. |
|
|
| CASPe: 9/10 SIGN: 2++ B |
| Ozpancar, Cinar & Topcu, 2017. Turkey. | Randomized clinical trial.
|
|
|
| Nurse-implemented case management resulted in a significant decrease in blood pressure in individuals with hypertension, improved adherence to treatment, and improved care for individuals with chronic diseases. | CASPe: 10/10 SIGN: 1++ A |
| Burguel et al., 2018. United States. | Qualitative and descriptive study.Sample: 80 patients with severe mental illness over 18 years old with at least one primary diagnosis, behavioral or emotional. | To promote a case management program to improve oral health. |
|
|
| CASPe: 7/10 SIGN: 3 D |
| Davisson & Swanson, 2018. United States. | Mixed study (observations, interviews and coding were used).Sample: 6 adults over 65 years old in a rural hospital. | To describe how the nurse-led “Living Well” case management program impacts the care of chronically ill patients. |
|
|
| CASPe: 8/10 SIGN: 3 D |
| Morales et al., 2019. Spain. | Longitudinal cohort follow-up study.-Sample: 835 patients. | To describe the characteristics of case management: interventions, service utilization, readmissions, pressure ulcers, falls |
|
|
| CASPe: 11/11 SIGN: 2++ B |
| Sánchez et al., 2019. Spain. | Scoping review. | Implementing the role of the Advanced Practice Nurse and measuring its impact on clinical practice and patient benefit |
|
|
| CASPe: 9/10 SING: 2++ B |
| Scherlowski et al., 2020. Spain and Brasil. | Mixed study: bibliographic review of papers and publications on the nurse case manager and qualitative approach of interviews to 7 teaching nurses. |
|
|
|
| Bibliographic review CASPe: 9/10 Qualitative study CASPe: 8/10 SIGN: 3 D |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doménech-Briz, V.; Gómez Romero, R.; de Miguel-Montoya, I.; Juárez-Vela, R.; Martínez-Riera, J.R.; Mármol-López, M.I.; Verdeguer-Gómez, M.V.; Sánchez-Rodríguez, Á.; Gea-Caballero, V. Results of Nurse Case Management in Primary Heath Care: Bibliographic Review. Int. J. Environ. Res. Public Health 2020, 17, 9541. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249541
Doménech-Briz V, Gómez Romero R, de Miguel-Montoya I, Juárez-Vela R, Martínez-Riera JR, Mármol-López MI, Verdeguer-Gómez MV, Sánchez-Rodríguez Á, Gea-Caballero V. Results of Nurse Case Management in Primary Heath Care: Bibliographic Review. International Journal of Environmental Research and Public Health. 2020; 17(24):9541. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249541
Chicago/Turabian StyleDoménech-Briz, Vicente, Rosario Gómez Romero, Isabel de Miguel-Montoya, Raúl Juárez-Vela, José Ramón Martínez-Riera, María Isabel Mármol-López, María Virtudes Verdeguer-Gómez, Álvaro Sánchez-Rodríguez, and Vicente Gea-Caballero. 2020. "Results of Nurse Case Management in Primary Heath Care: Bibliographic Review" International Journal of Environmental Research and Public Health 17, no. 24: 9541. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249541