In the Subtropical Monsoon Climate High-Density City, What Features of the Neighborhood Environment Matter Most for Public Health?


Abstract
:1. Introduction
2. Materials and Methods
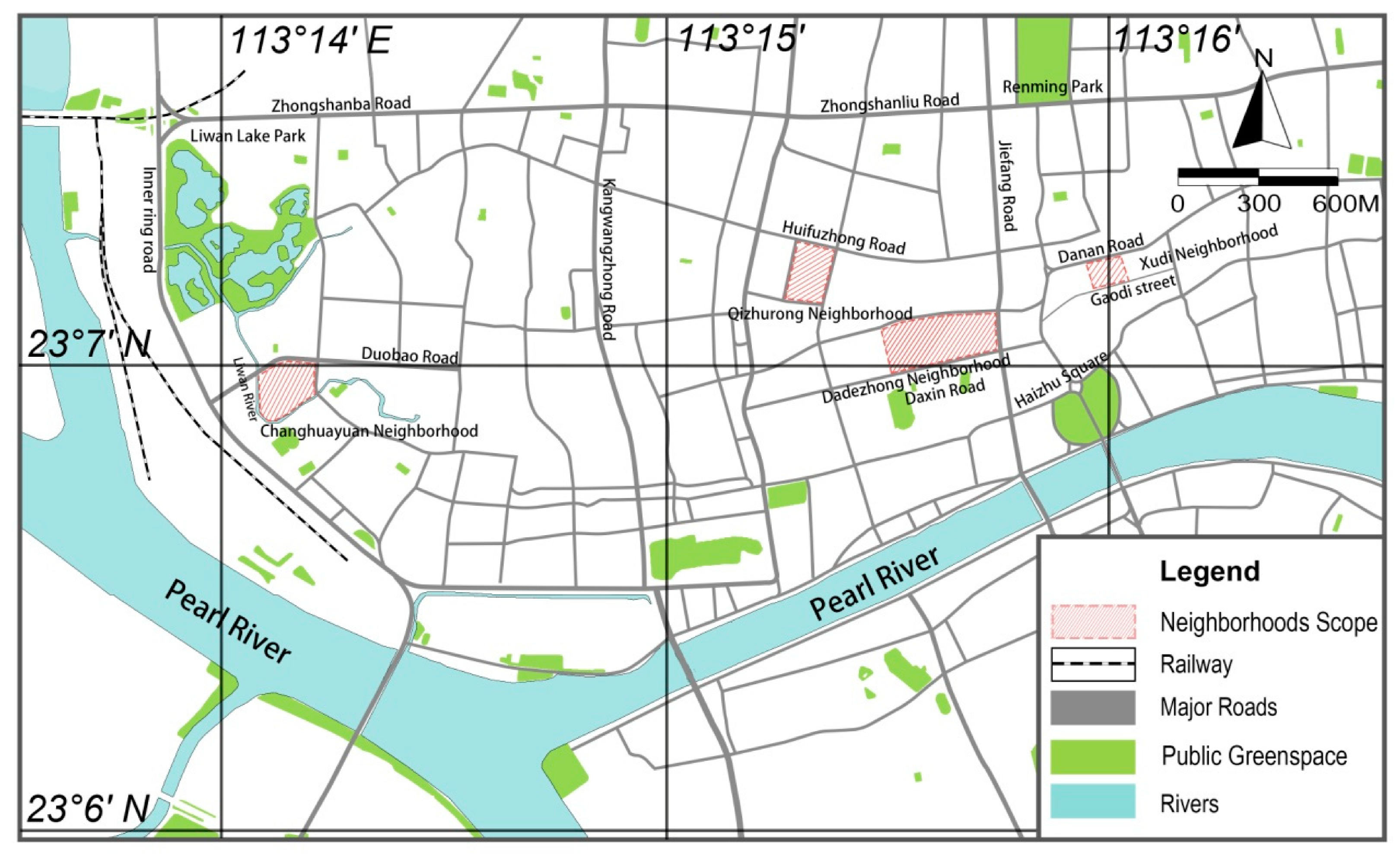
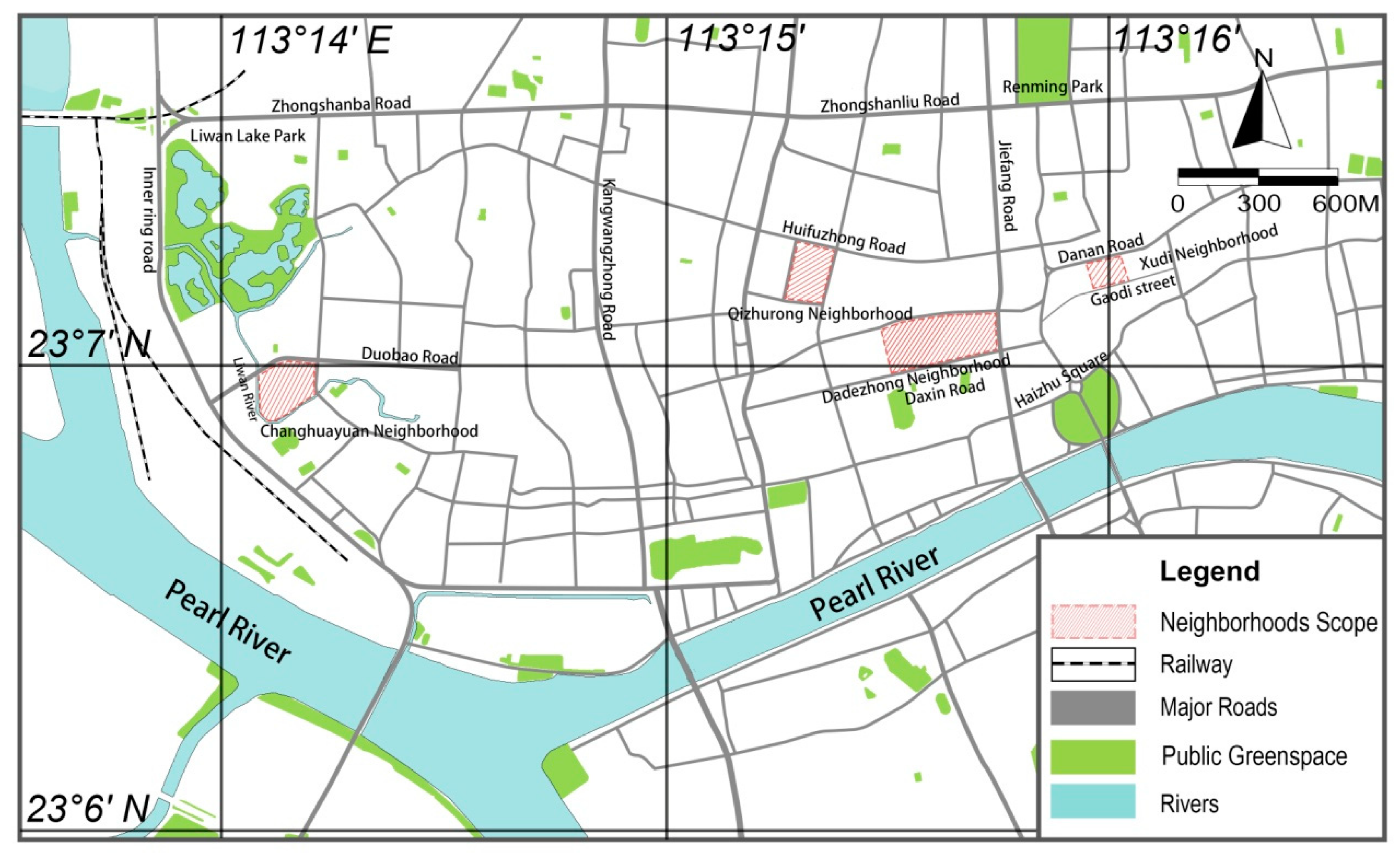
2.1. Study Site
2.2. Data Collection
2.2.1. Environmental Factor Measurement
2.2.2. Questionnaire Distribution and Recovery
2.3. Statistical Analysis
3. Results
3.1. Reliability and Validity Analysis of the SF-36
3.1.1. Reliability Analysis of the SF-36
3.1.2. Validity Analysis of the SF-36
3.2. Analysis of Variance
3.3. Correlation between Environmental Factors and Health
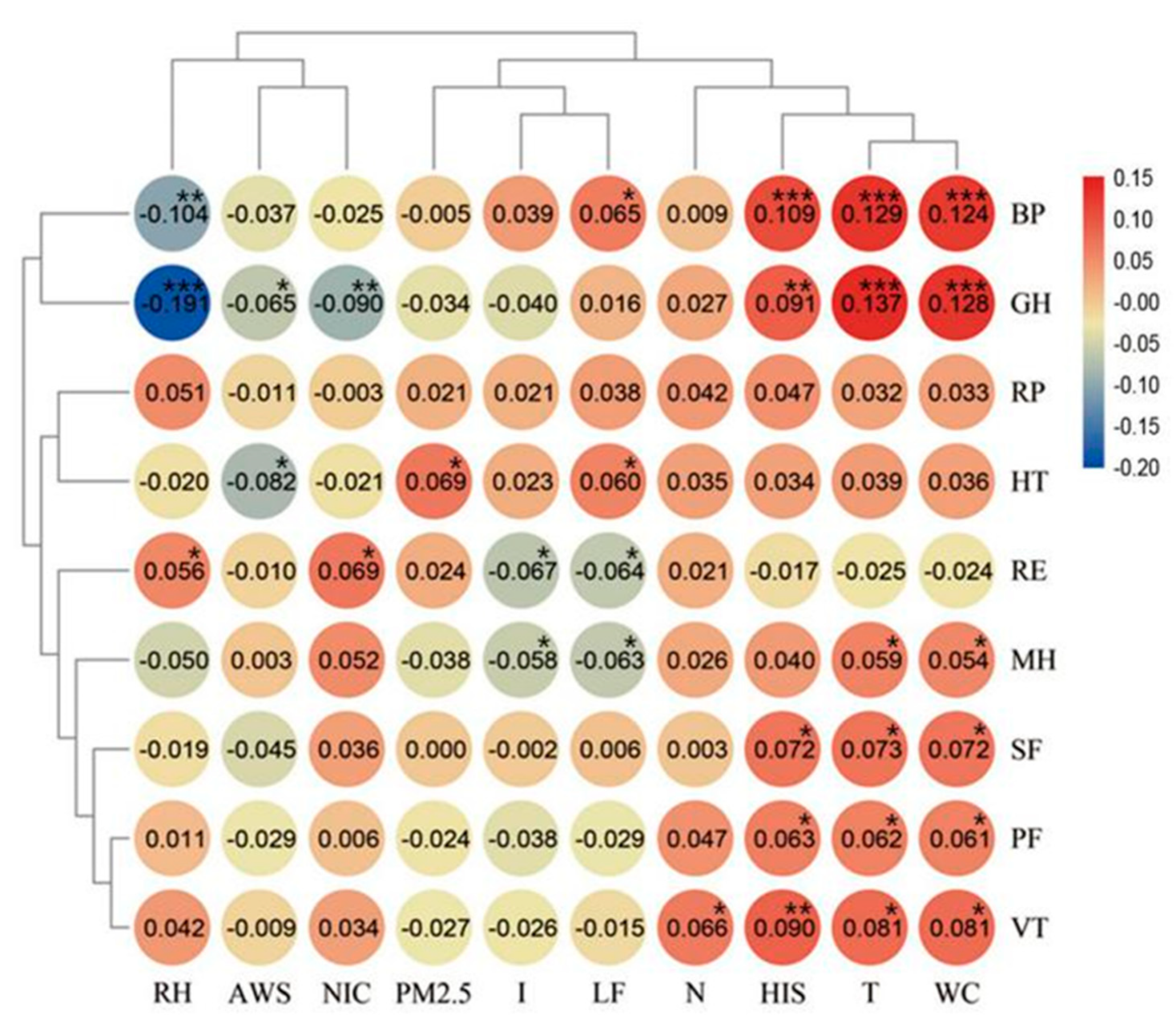
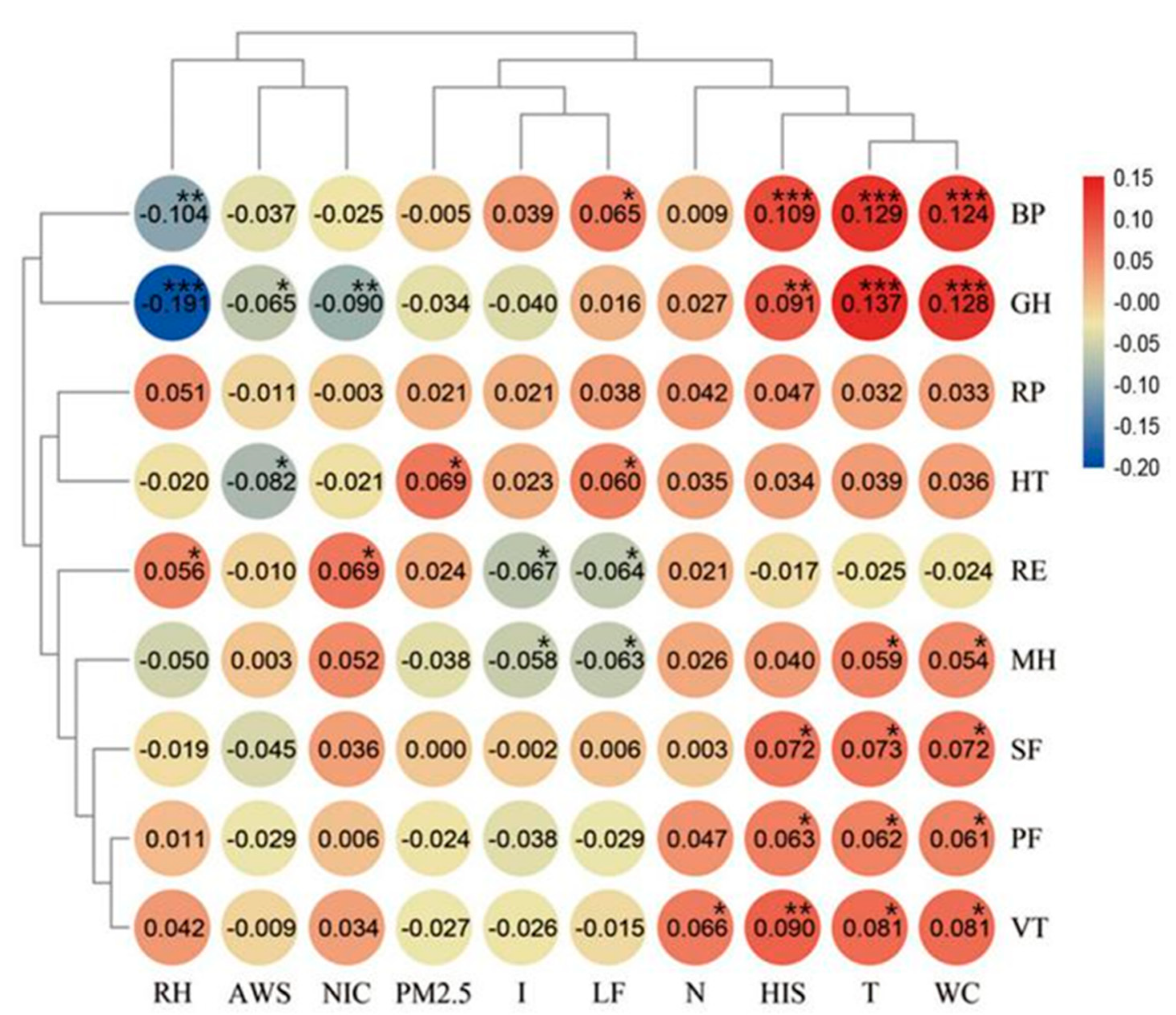
3.3.1. Correlation between Health Subscales and Environmental Factors
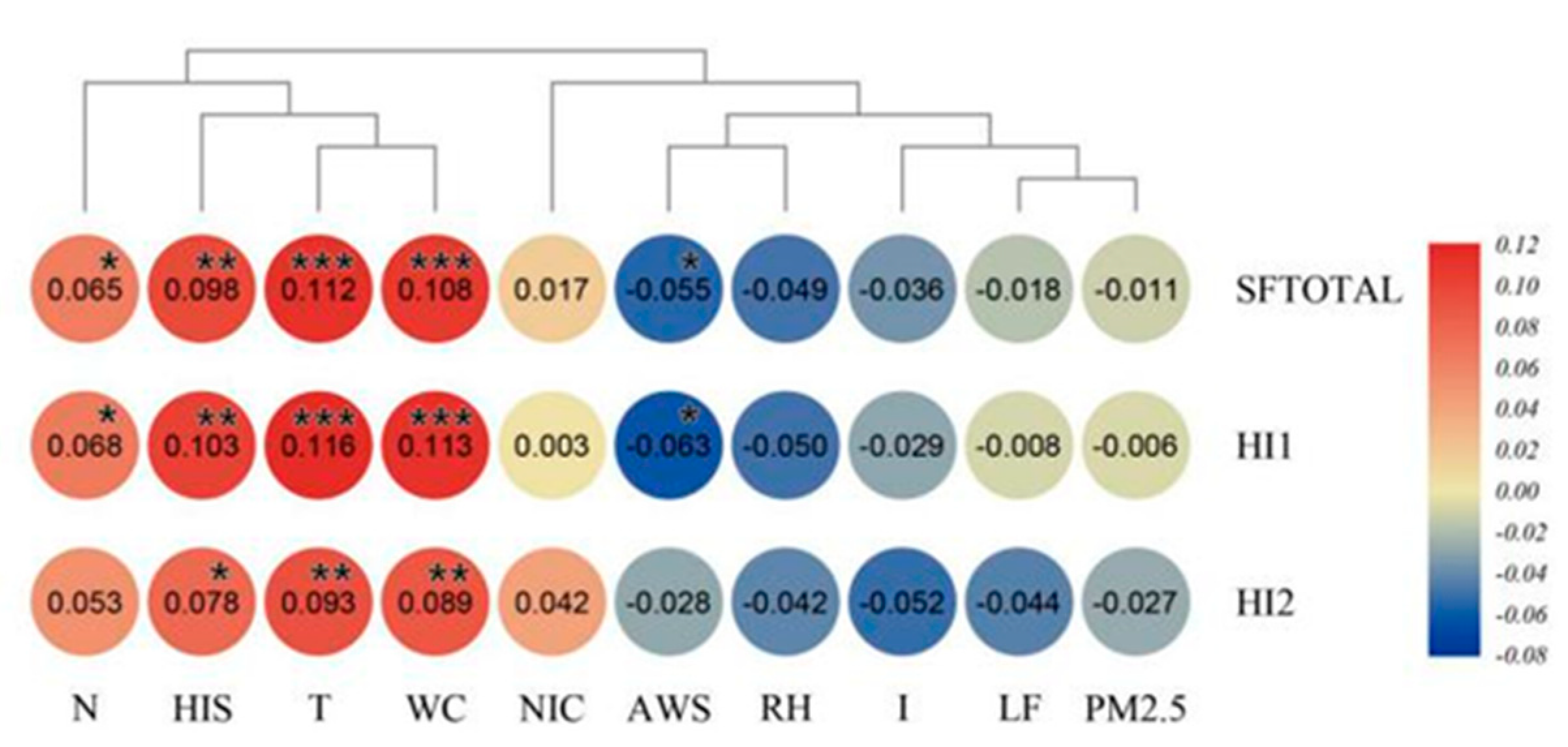
3.3.2. Correlation between Health Types and Environmental Factors
3.3.3. Path Analysis of Environmental Factors in Relation to Health
4. Discussion
4.1. There Is a Close Correlation between Public Health and the Outdoor Neighborhood Environment in Subtropical Monsoon Climate and High-Density Cities
4.2. Selecting Priorities for Environmental Renewal Work in Old Neighborhoods with the Intention of Improving Public Health Can Be Informed by Weighting the Different Environmental Factors
4.3. During Environmental Renewal of Old Neighborhoods, Weighting the Relative Importance of Different Factors in Relation to Health Can Be Helpful When Identifying Projects to Prioritize
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases Country Profles 2018. 2018, pp. 10–11. Available online: https://www.who.int/nmh/publications/ncd-profiles-2018/en/ (accessed on 6 June 2020).
- China Research Institute for Family Planning. 2017 White Paper on Mental Health of Chinese Urban Residents. 2020, p. 10. Available online: https://www.e-healthdata.cn/healthdata/xsbg/5807.jhtml (accessed on 2 February 2020).
- World Health Organization. Preventing Disease through Healthy Environments: A Global Assessment of the Burden of Disease from Environmental Risks. 2016, pp. 103–105. Available online: https://www.who.int/publications/i/item/9789241565196 (accessed on 28 October 2020).
- World Health Organization. Promoting Health: Guide to National Implementation of the Shanghai Declaration. 2018, pp. 11–13. Available online: https://www.who.int/publications/i/item/WHO-NMH-PND-18.2 (accessed on 28 October 2020).
- Renalds, A.; Smith, T.H.; Hale, P.J. A systematic review of built environment and health. Fam. Community Health 2010, 33, 68–78. [Google Scholar] [CrossRef]
- Bird, E.L.; Ige, J.O.; Pilkington, P.; Pinto, A.; Petrokofsky, C.; Burgess-Allen, J. Built and natural environment planning principles for promoting health: An umbrella review. BMC Public Health 2018, 18, 930. [Google Scholar] [CrossRef]
- Pascal, M.; Corso, M.; Chanel, O.; Declercq, C.; Badaloni, C.; Cesaroni, G.; Henschel, S.; Meister, K.; Haluza, D.; Martin-Olmedo, P.; et al. Assessing the public health impacts of urban air pollution in 25 European cities: Results of the Aphekom project. Sci. Total Environ. 2013, 449, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Aries, M.B.C.; Aarts, M.P.J.; van Hoof, J. Daylight and health: A review of the evidence and consequences for the built environment. Lighting Res. Technol. 2015, 47, 6–27. [Google Scholar] [CrossRef]
- Brown, A.L.; van Kamp, I. WHO Environmental Noise Guidelines for the European Region: A Systematic Review of Transport Noise Interventions and Their Impacts on Health. Int. J. Environ. Res. Public Health 2017, 14, 873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schinasi, L.H.; Benmarhnia, T.; De Roos, A.J. Modification of the association between high ambient temperature and health by urban microclimate indicators: A systematic review and meta-analysis. Environ. Res. 2018, 161, 168–180. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhong, B.; Vardoulakis, S.; Zhang, F.; Pilot, E.; Li, Y.; Yang, L.; Wang, W.; Krafft, T. Air Quality Strategies on Public Health and Health Equity in Europe-A Systematic Review. Int. J. Environ. Res. Public Health 2016, 13, 1196. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, X.L.; Duan, Y.X.; Jin, H.X. Research Review on Urban Landscape Micro-climate. Chin. Landsc. Archit. 2017, 33, 23–28. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=ZGYL201704005&DbName=CJFQ2017 (accessed on 28 November 2020).
- Venter, Z.S.; Krog, N.H.; Barton, D.N. Linking green infrastructure to urban heat and human health risk mitigation in Oslo, Norway. Sci. Total Environ. 2020, 709, 136193. [Google Scholar] [CrossRef]
- Lin, Y.; Chang, C.; Li, M.; Wu, Y.; Wang, Y. High-temperature indices associated with mortality and outpatient visits: Characterizing the association with elevated temperature. Sci. Total Environ. 2012, 427, 41–49. [Google Scholar] [CrossRef]
- Ho, H.C.; Lau, K.K.; Ren, C.; Ng, E. Characterizing prolonged heat effects on mortality in a sub-tropical high-density city, Hong Kong. Int. J. Biometeorol. 2017, 61, 1935–1944. [Google Scholar] [CrossRef] [PubMed]
- Huynen, M.M.T.E.; Martens, P.; Schram, D.; Weijenberg, M.P.; Kunst, A.E. The impact of heat waves and cold spells on mortality rates in the Dutch population. Environ. Health Perspect. 2001, 109, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.B.; Bell, M.L. Heat Waves in the United States: Mortality Risk during Heat Waves and Effect Modification by Heat Wave Characteristics in 43 U.S. Communities. Environ. Health Perspect. 2011, 119, 210–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, J.A.; Stewart, L.K. Heat-Related Illness. Am. Fam. Phys. 2011, 83, 1325–1330. Available online: http://0-apps-webofknowledge-com.brum.beds.ac.uk/full_record.do?product=UA&search_mode=GeneralSearch&qid=90&SID=5AzEIxeTa323lPybUyF&page=1&doc=7 (accessed on 27 November 2020).
- Yang, L.; Chen, P.Y.; He, J.F.; Chan, K.P.; Ou, C.Q.; Deng, A.P.; Peiris, J.S.M.; Wong, C.M. Effect modification of environmental factors on influenza-associated mortality: A time-series study in two Chinese cities. BMC Infect. Dis. 2011, 11, 342. [Google Scholar] [CrossRef] [Green Version]
- Wolkoff, P. Indoor air humidity, air quality, and health—An overview. Int. J. Hyg. Environ. Health 2018, 221, 376–390. [Google Scholar] [CrossRef]
- Shaman, J.; Pitzer, V.E.; Viboud, C.; Grenfell, B.T.; Lipsitch, M. Absolute Humidity and the Seasonal Onset of Influenza in the Continental United States. PLoS Biol. 2010, 8, e1000316. [Google Scholar] [CrossRef]
- Onozuka, D.; Hashizume, M. The influence of temperature and humidity on the incidence of hand, foot, and mouth disease in Japan. Sci. Total Environ. 2011, 410, 119–125. [Google Scholar] [CrossRef]
- Barreca, A.I.; Shimshack, J.P. Absolute Humidity, Temperature, and Influenza Mortality: 30 Years of County-Level Evidence from the United States. Am. J. Epidemiol. 2012, 1767, S114–S122. [Google Scholar] [CrossRef] [Green Version]
- Ding, N.; Berry, H.L.; Bennett, C.M. The Importance of Humidity in the Relationship between Heat and Population Mental Health: Evidence from Australia. PLoS ONE 2016, 11, e016419010. [Google Scholar] [CrossRef] [Green Version]
- Ham, W.A.; Ruehl, C.R.; Kleeman, M.J. Seasonal Variation of Airborne Particle Deposition Efficiency in the Human Respiratory System. Aerosol Sci. Technol. 2011, 45, 795–804. [Google Scholar] [CrossRef] [Green Version]
- Jia, M.; Jin, H.X.; Wang, S.F. On the Progress of Research of Landscape Plant Volatile Compounds and Their Influence on Human Health in Rehabilitation Landscape. Chin. Landsc. Archit. 2016, 32, 26–31. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=ZGYL201612006&DbName=CJFQ2016 (accessed on 4 November 2020).
- Csavina, J.; Field, J.; Felix, O.; Corral-Avitia, A.Y.; Saez, A.E.; Betterton, E.A. Effect of wind speed and relative humidity on atmospheric dust concentrations in semi-arid climates. Sci. Total Environ. 2014, 487, 82–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, R.P.; Lee, T.K. Adverse effects of ultraviolet radiation: A brief review. Prog. Biophys. Mol. Biol. 2006, 92, 119–131. [Google Scholar] [CrossRef]
- Watson, M.; Holman, D.M.; Fox, K.A.; Guy, G.P.; Seidenberg, A.B.; Sampson, B.P.; Sinclair, C.; Lazovich, D. Preventing Skin Cancer Through Reduction of Indoor Tanning Current Evidence. Am. J. Prev. Med. 2013, 44, 682–689. [Google Scholar] [CrossRef] [Green Version]
- Touitou, Y. Light at night pollution of the internal clock, a public health issue. Bull. Acad. Natl. Med. 2015, 199, 1081–1098. [Google Scholar] [CrossRef]
- Ising, H.; Kruppa, B. Health effects caused by noise: Evidence in the literature from the past 25 years. Noise Health 2004, 6, 5–13. Available online: http://0-apps-webofknowledge-com.brum.beds.ac.uk/full_record.do?product=UA&search_mode=GeneralSearch&qid=132&SID=5AzEIxeTa323lPybUyF&page=1&doc=1 (accessed on 25 September 2020).
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef] [Green Version]
- Fyhri, A.; Aasvang, G.M. Noise, sleep and poor health: Modeling the relationship between road traffic noise and cardiovascular problems. Sci. Total Environ. 2010, 408, 4935–4942. [Google Scholar] [CrossRef]
- Aletta, F.; Oberman, T.; Kang, J. Associations between Positive Health-Related Effects and Soundscapes Perceptual Constructs: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2392. [Google Scholar] [CrossRef] [Green Version]
- Skanberg, A.; Ohrstrom, E. Adverse health effects in relation to urban residential soundscapes. J. Sound Vib. 2002, 250, 151–155. [Google Scholar] [CrossRef]
- Zheng, Z.; Yang, L.L. Neighborhood Environment, Lifestyle, and Health of Older Adults: Comparison of Age Groups Based on Ecological Model of Aging. Sustainability 2019, 11, 2077. [Google Scholar] [CrossRef] [Green Version]
- Seo, S.; Choi, S.; Kim, K.; Kim, S.M.; Park, S.M. Association between urban green space and the risk of cardiovascular disease: A longitudinal study in seven Korean metropolitan areas. Environ. Int. 2019, 125, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Feng, X. Association of Urban Green Space with Mental Health and General Health among Adults in Australia. JAMA Netw. Open 2019, 2, e198209. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Harmer, P.A.; Cardinal, B.J.; Bosworth, M.; Acock, A.; Johnson-Shelton, D.; Moore, J.M. Built environment, adiposity, and physical activity in adults aged 50–75. Am. J. Prev. Med. 2008, 35, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Yuan, Y. The neighborhood effect of exposure to blue space on elderly individuals’ mental health: A case study in Guangzhou, China. Health Place 2020, 63, 102348. [Google Scholar] [CrossRef]
- China Meteorological Information Center. Guangdong Ground Accumulated Annual Value Data Set (1981–2010). 2012. Available online: http://data.cma.cn/data/cdcdetail/dataCode/A.0029.0001_440.html (accessed on 15 September 2020).
- Tang, H.T. Discussion on the Planning and Handling of the Remaining Problems of the Historical City Construction Project: Taking Guangzhou as an Example. In Proceedings of the 2016 China Urban Planning Annual Conference, Shenyang, China, 24 September 2016; p. 9. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=ZHCG201609008009&DbName=CPFD2017 (accessed on 27 September 2020).
- Liu, J.P. Urban Environment Physics, Chapter One Urban Environment Physics Foundation; China Architecture & Building Press: Beijing, China, 2011; pp. 1–3. ISBN 978-7-112-12492-3. [Google Scholar]
- Qiu, J.C.; Xu, J.; Feng, L.Y.; Lu, Y.; Wei, Q. Reliability and Validity of SF-36 in Health-Related Quality of Life Survey Among Civil Servants of Guangdong Province. Chin. Gen. Pract. 2012, 15, 386–389. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=QKYX201204014&DbName=CJFQ2012 (accessed on 17 November 2019).
- Jin, W.Z.; Yu, H.P. A study of the reliability and validity of SF-36 scale on evaluating health of population. Chin. Health Resour. 2012, 15, 265–267. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=WSZY201203040&DbName=CJFQ2012 (accessed on 19 November 2019).
- Rand Corporation. 36-Item Short Form Survey Instrument (SF-36). 2020. Available online: https://www.rand.org/health-care/surveys_tools/mos/36-item-short-form/survey-instrument.html (accessed on 3 November 2020).
- Ware, J.E.J.; Kosinski, M.; Bayliss, M.S.; McHorney, C.A.; Rogers, W.H.; Raczek, A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: Summary of results from the Medical Outcomes Study. Med. Care 1995, 33 (Suppl. 4), AS264–AS279. [Google Scholar] [CrossRef]
- Zhao, H.S.; Wang, K.; Jin, Y.L.; Huang, S.P. Reliability and validity of SF-36 in health survey among empty-nest elders in countryside. Chin. J. Public Health 2012, 28, 887–889. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=ZGGW201207004&DbName=CJFQ2012html (accessed on 25 September 2020).
- Bates, D.; Maechler, M.; Bolker, B.M.; Walker, S.C. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 19 August 2020).
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in Linear Mixed Effects Models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Revelle, W. Psych: Procedures for Personality and Psychological Research. 2018. Available online: https://www.rdocumentation.org/packages/psych (accessed on 3 March 2020).
- Felipe de Mendiburu. Agricolae: Statistical Procedures for Agricultural Research. 2020. Available online: https://CRAN.R-project.org/package=agricolae (accessed on 17 August 2020).
- Qiu, Y.; Liu, Y.Q.; Liu, Y.; Li, Z.G. Exploring the Linkage between the Neighborhood Environment and Mental Health in Guangzhou, China. Int. J. Environ. Res. Public Health 2019, 16, 3206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrett, J.K.; White, M.P.; Huang, J.; Ng, S.; Hui, Z.; Leung, C.; Tse, L.A.; Fung, F.; Elliott, L.R.; Depledge, M.H.; et al. Urban blue space and health and wellbeing in Hong Kong: Results from a survey of older adults. Health Place 2019, 55, 100–110. [Google Scholar] [CrossRef]
- Yu, R.; Wong, M.; Woo, J. Perceptions of Neighborhood Environment, Sense of Community, and Self-Rated Health: An Age-Friendly City Project in Hong Kong. J. Urban Health-Bull. N. Y. Acad. Med. 2019, 96, 276–288. [Google Scholar] [CrossRef]
- Yen, I.H.; Michael, Y.L.; Perdue, L. Neighborhood Environment in Studies of Health of Older Adults A Systematic Review. Am. J. Prev. Med. 2009, 37, 455–463. [Google Scholar] [CrossRef] [Green Version]
- Egan, M.; Kearns, A.; Mason, P.; Tannahill, C.; Bond, L.; Coyle, J.; Beck, S.; Crawford, F.; Hanlon, P.; Lawson, L.; et al. Protocol for a mixed methods study investigating the impact of investment in housing, regeneration and neighbourhood renewal on the health and wellbeing of residents: The GoWell programme. BMC Med. Res. Methodol. 2010, 10, 41. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; Saelens, B.E.; Frank, L.D.; Conway, T.L.; Slymen, D.J.; Cain, K.L.; Chapman, J.E.; Kerr, J. Neighborhood built environment and income: Examining multiple health outcomes. Soc. Sci. Med. 2009, 68, 1285–1293. [Google Scholar] [CrossRef] [Green Version]
- Blackman, T.; Harvey, J.; Lawrence, M.; Simon, A. Neighbourhood renewal and health: Evidence from a local case study. Health Place 2001, 7, 93–103. [Google Scholar] [CrossRef] [Green Version]
- Mohan, G.; Longo, A.; Kee, F. Evaluation of the health impact of an urban regeneration policy: Neighbourhood Renewal in Northern Ireland. J. Epidemiol. Community Health 2017, 71, 919–927. [Google Scholar] [CrossRef] [Green Version]
- Thomson, H.; Atkinson, R.; Petticrew, M.; Kearns, A. Do urban regeneration programmes improve public health and reduce health inequalities? A synthesis of the evidence from UK policy and practice (1980–2004). J. Epidemiol. Community Health 2006, 60, 108–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salata, F.; Golasi, L.; Petitti, D.; Vollaro, E.D.L.; Coppi, M.; Vollaro, A.D.L. Relating microclimate, human thermal comfort and health during heat waves: An analysis of heat island mitigation strategies through a case study in an urban outdoor environment. Sustain. Cities Soc. 2017, 30, 79–96. [Google Scholar] [CrossRef]
- Arnfield, A.J. Two decades of urban climate research: A review of turbulence, exchanges of energy and water, and the urban heat island. Int. J. Climatol. 2003, 23, 1–26. [Google Scholar] [CrossRef]
- Moudon, A.V. Real Noise from the Urban Environment How Ambient Community Noise Affects Health and What Can Be Done about It. Am. J. Prev. Med. 2009, 37, 167–171. [Google Scholar] [CrossRef]
- Vanos, J.K. Children’s health and vulnerability in outdoor microclimates: A comprehensive review. Environ. Int. 2015, 76, 1–15. [Google Scholar] [CrossRef]
- Shafaghat, A.; Keyvanfar, A.; Manteghi, G.; Bin Lamit, H. Environmental-conscious factors affecting street microclimate and individuals’ respiratory health in tropical coastal cities. Sustain. Cities Soc. 2016, 21, 35–50. [Google Scholar] [CrossRef]
- Feng, X.H.; Wei, Q.Q. Study on the near-surface flow field in urban areas of Guangzhou. Ecol. Environ. Sci. 2011, 20, 1558–1561. [Google Scholar] [CrossRef]
- China Meteorological Administration. The Grade of Wind. 2020. Available online: http://www.cma.gov.cn/2011xzt/20120816/2012081601/201208160101/201407/t20140717_252607.html (accessed on 28 June 2020).
- Teunissen, L.P.J.; de Haan, A.; de Koning, J.J.; Daanen, H.A.M. Effects of wind application on thermal perception and self-paced performance. Eur. J. Appl. Physiol. 2013, 113, 1705–1717. [Google Scholar] [CrossRef]
- Buonocore, C.; De Vecchi, R.; Scalco, V.; Lamberts, R. Influence of relative air humidity and movement on human thermal perception in classrooms in a hot and humid climate. Build. Environ. 2018, 146, 98–106. [Google Scholar] [CrossRef]
- Yu, C.X.; Deng, X.L.; Shi, C.E.; Wu, B.W.; Zhai, Q.; Yang, G.Y.; Huo, Y.F. The scavenging effect of precipitation and wind on PM2.5 and PM10. Acta Sci. Circumstantiae 2018, 38, 4620–4629. [Google Scholar] [CrossRef]
- Zhou, P.; Grady, S.C.; Chen, G. How the built environment affects change in older people’s physical activity: A mixed-methods approach using longitudinal health survey data in urban China. Soc. Sci. Med. 2017, 192, 74–84. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Environmental Factors | Minimum | Maximum | Mean | Standard Deviation | Coefficient of Variation (%) |
|---|---|---|---|---|---|
| N (db) | 50.46 | 61.55 | 54.96 | 3.63 | 6.61 |
| I (Lm) | 901.87 | 17,482.34 | 5215.39 | 3734.67 | 71.61 |
| LF (Lx) | 0.90 | 15.16 | 4.40 | 3.04 | 69.05 |
| AWS (m/s) | 0.12 | 0.91 | 0.53 | 0.22 | 40.92 |
| T (°C) | 16.22 | 33.80 | 25.07 | 5.14 | 20.51 |
| WCI | 16.24 | 33.83 | 25.08 | 5.34 | 21.28 |
| RH (%) | 60.55 | 83.21 | 69.95 | 7.02 | 10.04 |
| HSI | 16.15 | 44.89 | 28.03 | 9.03 | 32.23 |
| NOI | −2.56 | −0.44 | −1.41 | 0.64 | 45.88 |
| PM2.5 (μg/m3) | 23.42 | 88.80 | 51.59 | 19.09 | 37.01 |
| Age Range (Year) | 12–19 | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80–89 |
|---|---|---|---|---|---|---|---|---|
| Male | 31 | 95 | 78 | 90 | 135 | 95 | 37 | 17 |
| Female | 23 | 77 | 78 | 88 | 118 | 88 | 64 | 44 |
| Health Subscales | Minimum | Maximum | Mean | Standard Deviation | Coefficient of Variation (%) |
|---|---|---|---|---|---|
| BP | 21.00 | 100.00 | 82.91 | 16.74 | 20.20 |
| PF | 0.00 | 100.00 | 84.71 | 19.42 | 22.92 |
| RP | 0.00 | 100.00 | 76.67 | 33.47 | 43.65 |
| GH | 5.00 | 100.00 | 65.47 | 20.65 | 31.54 |
| VT | 10.00 | 100.00 | 72.92 | 16.74 | 22.96 |
| SF | 0.00 | 112.50 | 93.03 | 20.97 | 22.54 |
| RE | 0.00 | 100.00 | 77.22 | 33.75 | 43.71 |
| MH | 4.00 | 100.00 | 72.83 | 16.73 | 22.97 |
| HT | 0.00 | 100.00 | 50.67 | 21.02 | 41.47 |
| Health Subscales | BP | PF | RP | GH | VT | SF | RE | MH | HT |
|---|---|---|---|---|---|---|---|---|---|
| PF | 0.53 *** | ||||||||
| RP | 0.46 *** | 0.49 *** | |||||||
| GH | 0.53 *** | 0.52 *** | 0.44 *** | ||||||
| VT | 0.38 *** | 0.43 *** | 0.38 *** | 0.46 *** | |||||
| SF | 0.56 *** | 0.52 *** | 0.47 *** | 0.51 *** | 0.52 *** | ||||
| RE | 0.30 *** | 0.20 *** | 0.47 *** | 0.24 *** | 0.30 *** | 0.40 *** | |||
| MH | 0.26 *** | 0.21 *** | 0.24 *** | 0.32 *** | 0.59 *** | 0.44 *** | 0.34 *** | ||
| HT | 0.34 *** | 0.29 *** | 0.27 *** | 0.40 *** | 0.20 *** | 0.25 *** | 0.11 *** | 0.07 * | |
| Total | 0.68 *** | 0.73 *** | 0.62 *** | 0.78 *** | 0.77 *** | 0.75 *** | 0.46 *** | 0.66 *** | 0.39 *** |
| Subscales | Actual Model | Theoretical Model | ||
|---|---|---|---|---|
| F1 | F2 | Physiological Factors | Psychological Factors | |
| BP | 0.71 | 0.17 | ≥0.70 | r ≤ 0.30 |
| PF | 0.72 | 0.13 | ≥0.70 | r ≤ 0.30 |
| RP | 0.64 | 0.16 | ≥0.70 | r ≤ 0.30 |
| GH | 0.66 | 0.24 | 0.30 < r < 0.70 | 0.30 < r < 0.70 |
| VT | 0.46 | 0.55 | 0.30 < r < 0.70 | 0.30 < r < 0.70 |
| SF | 0.67 | 0.36 | 0.30 < r < 0.70 | ≥0.70 |
| RE | 0.36 | 0.38 | r ≤ 0.30 | ≥0.70 |
| MH | 0.12 | 0.99 | r ≤ 0.30 | ≥0.70 |
| Fixed Effects | Sum Square | Mean Square | Degree of Freedom | Denominator Degree | F Value | p Value |
|---|---|---|---|---|---|---|
| Neighborhood | 1177.00 | 392.34 | 3 | 911.83 | 1.96 | 0.117027 ns |
| Season | 3130.70 | 782.67 | 4 | 918.16 | 3.92 | 0.003613 ** |
| Neighborhood × season | 4079.30 | 509.91 | 8 | 909.80 | 2.55 | 0.009220 ** |
| Random Effects | Number of Parameters | Logical Value | Red Pool Information Rules | Degree of Freedom | p Value |
|---|---|---|---|---|---|
| <none> | 19 | −3937.8 | 7913.5 | ||
| Age | 18 | −3965.6 | 7967.3 | 1 | 8.175 × 10−14 *** |
| Gender | 18 | −3941.9 | 7919.8 | 1 | 0.003951 ** |
| Health Types | Environmental Factors | Correlation Coefficient | Direct Effects | R2 Total Contribution of Environmental Factors | Indirect Effects | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Adoption of N | Adoption of I | Adoption of LF | Adoption of AWS | Adoption of T | Adoption of WC | Adoption of RH | Adoption of HIS | Adoption of NIC | Adoption of PM2.5 | |||||
| SFTOTAL | N | 0.0651 | 0.0466 | 0.003 | 0.0185 | 0.1313 | −0.0941 | 0.0118 | 0.0031 | 0.0161 | 0.0044 | −0.0106 | −0.0075 | −0.036 | |
| I | −0.0362 | −0.4489 | 0.0163 | 0.4127 | −0.012 | 0.3651 | −0.0126 | 0.0168 | 0.0947 | −0.0035 | −0.0702 | −0.0075 | 0.0419 | ||
| LF | −0.0183 | 0.3781 | −0.0069 | −0.3964 | −0.0104 | −0.4391 | −0.0102 | 0.0171 | 0.0968 | −0.0044 | −0.0702 | −0.0103 | 0.0344 | ||
| AWS | −0.0552 | −0.0308 | 0.0017 | −0.0244 | −0.0191 | −0.2218 | 0.1506 | 0.0035 | 0.0242 | 0.004 | −0.0291 | −0.0028 | 0.0662 | ||
| T | 0.1121 | 0.037 | 0.0042 | 0.0751 | 0.0037 | −0.2173 | 0.1844 | −0.0026 | 0.2016 | −0.0073 | −0.1284 | 0.0031 | 0.0377 | ||
| WC | 0.1081 | 0.1997 | 0.0216 | −0.0916 | 0.0033 | −0.2128 | 0.1807 | −0.0031 | 0.0349 | −0.0069 | −0.1298 | 0.0034 | 0.0385 | ||
| RH | −0.0493 | 0.0176 | −0.0009 | −0.0669 | 0.0108 | 0.0951 | −0.0979 | −0.0061 | −0.015 | −0.0827 | 0.0318 | −0.0028 | 0 | ||
| HIS | 0.0982 | −0.1342 | −0.0132 | 0.2324 | 0.0033 | −0.2399 | 0.1995 | −0.0056 | 0.0339 | 0.1976 | −0.004 | 0.0025 | 0.0452 | ||
| NIC | 0.0172 | 0.0285 | 0.0005 | −0.0113 | −0.01 | 0.1086 | −0.1242 | 0.0023 | 0.0035 | 0.0222 | −0.0015 | −0.0106 | −0.0017 | ||
| PM2.5 | −0.0113 | −0.0851 | 0.001 | 0.0738 | 0.0179 | 0.2264 | −0.1543 | 0.0202 | −0.0157 | −0.0927 | 0 | 0.0715 | 0.0006 | ||
| HI1 | N | 0.0683 | 0.0215 | 0.0015 | 0.0468 | 0.1517 | −0.1519 | 0.0714 | 0.0553 | 0.0821 | 0.0886 | −0.1261 | −0.013 | −0.1113 | |
| I | −0.0292 | −0.5222 | 0.0152 | 0.493 | −0.0067 | 0.5892 | −0.0761 | 0.2951 | 0.4822 | −0.0716 | −0.8356 | −0.013 | 0.1295 | ||
| LF | −0.0081 | 0.6094 | −0.0049 | −0.6175 | −0.0058 | −0.5073 | −0.0621 | 0.3013 | 0.4924 | −0.0886 | −0.8356 | −0.0179 | 0.1062 | ||
| AWS | −0.0631 | −0.1583 | 0.01 | 0.0952 | −0.0107 | −0.2563 | 0.243 | 0.0615 | 0.1231 | 0.0818 | −0.3469 | −0.0049 | 0.2046 | ||
| T | 0.1161 | 0.6109 | 0.0709 | −0.4948 | 0.0021 | −0.251 | 0.2977 | −0.0155 | 1.0259 | −0.1465 | −1.5293 | 0.0054 | 0.1165 | ||
| WC | 0.1134 | 1.0293 | 0.1167 | −0.9159 | 0.0019 | −0.2458 | 0.2916 | −0.0186 | 0.6148 | −0.1397 | −1.5451 | 0.006 | 0.1191 | ||
| RH | −0.0502 | 0.3406 | −0.0171 | −0.3908 | 0.006 | 0.1098 | −0.1579 | −0.0373 | −0.2644 | −0.4206 | 0.3784 | −0.0049 | 0 | ||
| HIS | 0.1032 | −1.5734 | −0.1624 | 1.6766 | 0.0019 | −0.2772 | 0.3219 | −0.0341 | 0.5964 | 1.0054 | −0.0818 | 0.0043 | 0.1398 | ||
| NIC | 0.0031 | 0.0538 | 0.0002 | −0.0507 | −0.0056 | 0.1255 | −0.197 | 0.014 | 0.0615 | 0.1129 | −0.0307 | −0.1261 | −0.0052 | ||
| PM2.5 | −0.0062 | −0.2551 | 0.0016 | 0.2489 | 0.01 | 0.2615 | −0.2491 | 0.1226 | −0.2767 | −0.4719 | 0 | 0.8514 | 0.0011 | ||
| HI2 | N | 0.0532 | 0.0769 | 0.0041 | −0.0237 | 0.1153 | −0.0798 | 0.0087 | 0.0214 | −0.0011 | 0.0012 | −0.0142 | −0.0147 | −0.0605 | |
| I | −0.0521 | −0.3995 | 0.0208 | 0.3474 | −0.0214 | 0.3096 | −0.0093 | 0.1143 | −0.0064 | −0.001 | −0.0942 | −0.0147 | 0.0704 | ||
| LF | −0.0441 | 0.315 | −0.0139 | −0.3591 | −0.0184 | −0.3855 | −0.0076 | 0.1166 | −0.0065 | −0.0012 | −0.0942 | −0.0201 | 0.0577 | ||
| AWS | −0.0282 | −0.0171 | 0.0005 | −0.0111 | −0.0339 | −0.1947 | 0.1277 | 0.0238 | −0.0016 | 0.0011 | −0.0391 | −0.0055 | 0.1112 | ||
| T | 0.0933 | 0.2413 | 0.0225 | −0.148 | 0.0066 | −0.1908 | 0.1564 | −0.0019 | −0.0136 | −0.0019 | −0.1723 | 0.0061 | 0.0634 | ||
| WC | 0.0892 | −0.0144 | −0.0013 | 0.1036 | 0.0059 | −0.1868 | 0.1532 | −0.0023 | 0.238 | −0.0019 | −0.1741 | 0.0067 | 0.0648 | ||
| RH | −0.0421 | 0.0024 | −0.0001 | −0.0445 | 0.0192 | 0.0835 | −0.083 | −0.0045 | −0.1024 | 0.0056 | 0.0426 | −0.0055 | 0 | ||
| HIS | 0.0782 | −0.1794 | −0.014 | 0.2576 | 0.0059 | −0.2106 | 0.1691 | −0.0042 | 0.2309 | −0.0133 | −0.0011 | 0.0049 | 0.076 | ||
| NIC | 0.0423 | 0.0633 | 0.0027 | −0.021 | −0.0177 | 0.0954 | −0.1053 | 0.0017 | 0.0238 | −0.0015 | −0.0004 | −0.0142 | −0.0028 | ||
| PM2.5 | −0.0271 | −0.1379 | 0.0037 | 0.1108 | 0.0317 | 0.1987 | −0.1308 | 0.0149 | −0.1071 | 0.0062 | 0 | 0.0959 | 0.0012 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, W.; Tu, R.; Li, H.; Fang, Y.; Que, Q. In the Subtropical Monsoon Climate High-Density City, What Features of the Neighborhood Environment Matter Most for Public Health? Int. J. Environ. Res. Public Health 2020, 17, 9566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249566
Gao W, Tu R, Li H, Fang Y, Que Q. In the Subtropical Monsoon Climate High-Density City, What Features of the Neighborhood Environment Matter Most for Public Health? International Journal of Environmental Research and Public Health. 2020; 17(24):9566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249566
Chicago/Turabian StyleGao, Wei, Ruoxiang Tu, Hao Li, Yongli Fang, and Qingmin Que. 2020. "In the Subtropical Monsoon Climate High-Density City, What Features of the Neighborhood Environment Matter Most for Public Health?" International Journal of Environmental Research and Public Health 17, no. 24: 9566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249566