Physical Fitness in Upper Austrian Children Living in Urban and Rural Areas: A Cross-Sectional Analysis with More Than 18,000 Children


Abstract
:1. Introduction
2. Materials and Methods
2.1. Fitness Assessment
2.2. Living Environment
2.3. Statistical Analyses
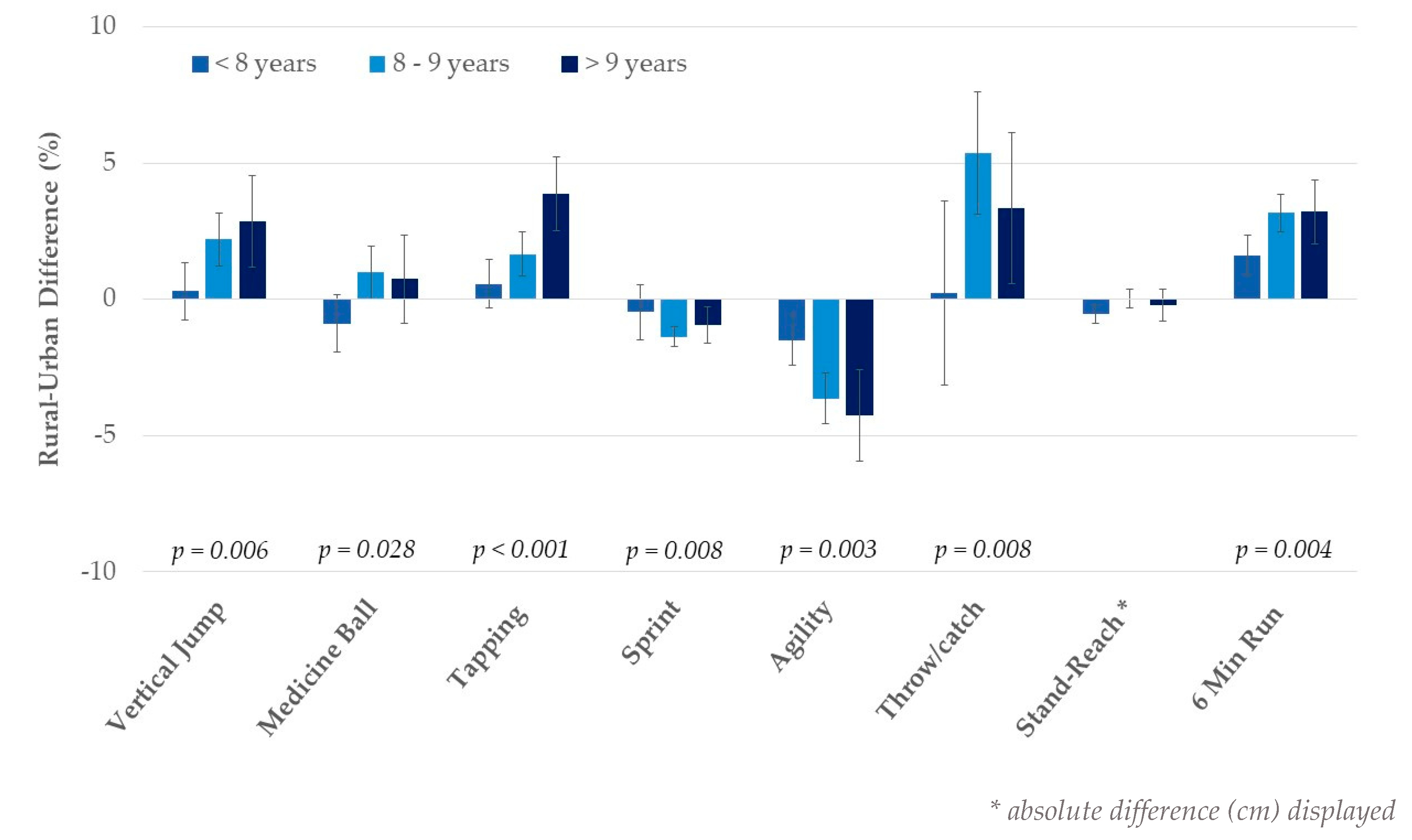
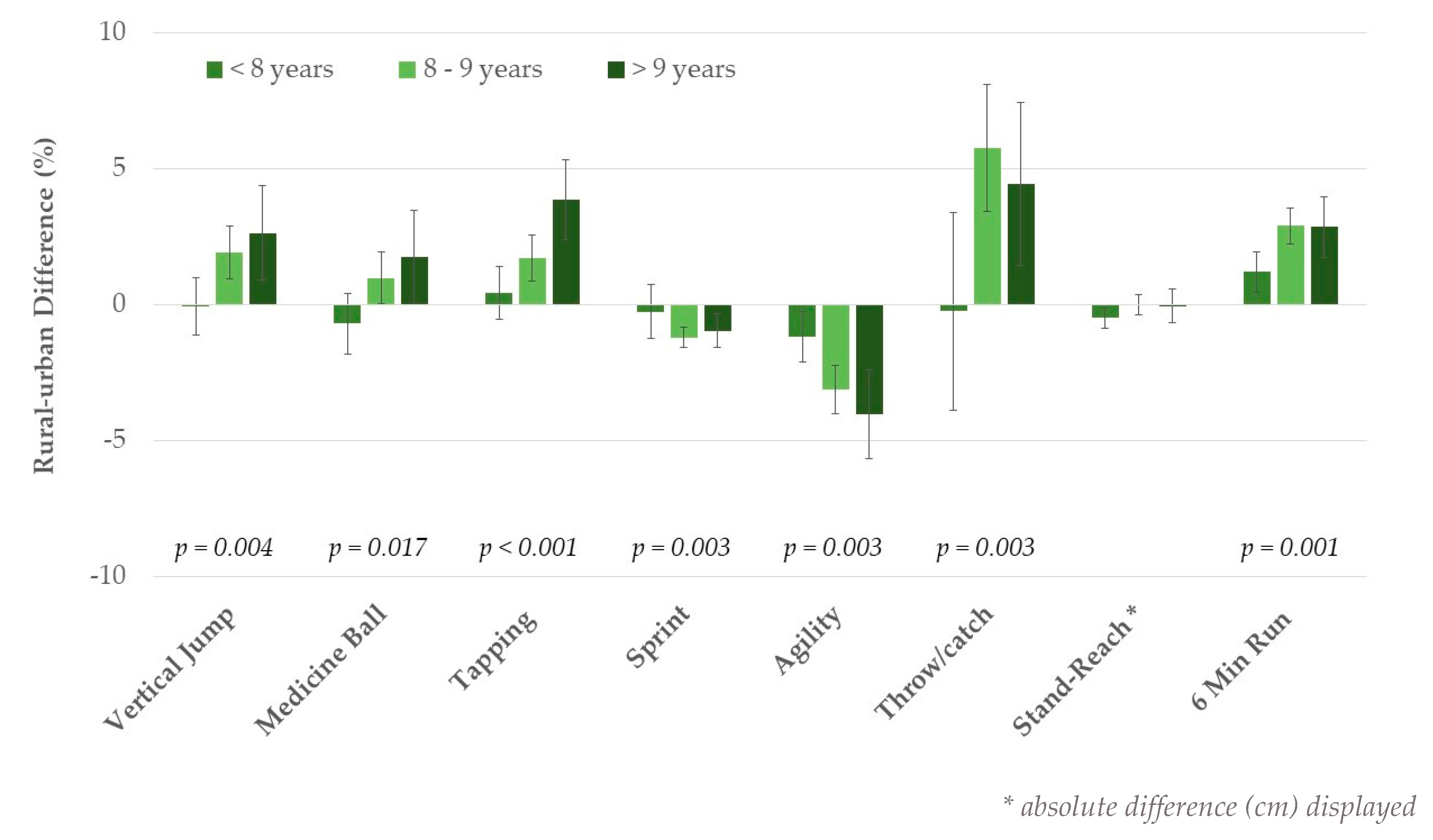
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McGranahan, G.; Satterthwaite, D. Urbanisation Concepts and Trends; IIED: London, UK, 2014. [Google Scholar]
- Machado-Rodrigues, A.M.; Coelho-E-Silva, M.J.; Mota, J.; Padez, C.; Martins, R.A.; Cumming, S.P.; Riddoch, C.; Malina, R.M. Urban-rural contrasts in fitness, physical activity, and sedentary behaviour in adolescents. Health Promot. Int. 2014, 29, 118–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eiben, O.; Barabas, A.; Nemeth, A. Comparison of growth, maturation, and physical fitness of Hungarian urban and rural boys and girls. J. Hum. Ecol. 2005, 17, 93–100. [Google Scholar] [CrossRef]
- Summerbell, C.D.; Waters, E.; Edmunds, L.D.; Kelly, S.; Brown, T.; Campbell, K.J. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2005, 3, CD001871. [Google Scholar] [CrossRef]
- Andrade Neto, F.; Eto, F.N.; Pereira, T.S.; Carletti, L.; Molina, M.D.C.B. Active and sedentary behaviours in children aged 7 to 10 years old: The urban and rural contexts, Brazil. BMC Public Health 2014, 14, 1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walhain, F.; van Gorp, M.; Lamur, K.S.; Veeger, D.H.; Ledebt, A. Health-Related Fitness, Motor Coordination, and Physical and Sedentary Activities of Urban and Rural Children in Suriname. J. Phys. Act. Health 2016, 13, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Muthuri, S.K.; Wachira, L.J.M.; Leblanc, A.G.; Francis, C.E.; Sampson, M.; Onywera, V.O.; Tremblay, M.S. Temporal trends and correlates of physical activity, sedentary behaviour, and physical fitness among school-aged children in Sub-Saharan Africa: A systematic review. Int. J. Environ. Res. Public Health 2014, 11, 3327–3359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabagambe, E.K.; Baylin, A.; Siles, X.; Campos, H. Comparison of dietary intakes of micro- and macronutrients in rural, suburban and urban populations in Costa Rica. Public Health Nutr. 2002, 5, 835–842. [Google Scholar] [CrossRef]
- Colic-Baric, I.; Kaifez, R.; Satalic, Z.; Cvjetic, S. Comparison of dietary habits in the urban and rural Croatian schoolchildren. Eur. J. Nutr. 2004, 43, 169–174. [Google Scholar] [CrossRef]
- Romero, A.J.; Robinson, T.N.; Kraemer, H.C.; Erickson, S.J.; Haydel, K.F.; Mendoza, F.; Killen, J.D. Are perceived neighborhood hazards a barrier to physical activity in children? Arch. Pediatr. Adolesc. Med. 2001, 155, 1143–1148. [Google Scholar] [CrossRef]
- Finn, K.; Johannsen, N.; Specker, B. Factors associated with physical activity in preschool children. J. Pediatr. 2002, 140, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Reimers, A.K.; Wagner, M.; Alvanides, S.; Steinmayr, A.; Reiner, M.; Schmidt, S.; Woll, A. Proximity to sports facilities and sports participation for adolescents in Germany. PLoS ONE 2014, 9, e93059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozdirenç, M.; Ozcan, A.; Akin, F.; Gelecek, N. Physical fitness in rural children compared with urban children in Turkey. Pediatr. Int. 2005, 47, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Gray, C.; Gibbons, R.; Larouche, R.; Sandseter, E.B.; Bienenstock, A.; Brussoni, M.; Chabot, G.; Herrington, S.; Janssen, I.; Pickett, W.; et al. What Is the Relationship between Outdoor Time and Physical Activity, Sedentary Behaviour, and Physical Fitness in Children? A Systematic Review. Int. J. Environ. Res. Public Health 2015, 12, 6455–6474. [Google Scholar] [CrossRef] [Green Version]
- Collins, P.; Al-Nakeeb, Y.; Nevill, A.; Lyons, M. The impact of the built environment on young people’s physical activity patterns: A suburban-rural comparison using GPS. Int. J. Environ. Res. Public Health 2012, 9, 3030–3050. [Google Scholar] [CrossRef] [Green Version]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S. Temporal trends in the cardiorespiratory fitness of children and adolescents representing 19 high-income and upper middle-income countries between 1981 and 2014. Br. J. Sports Med. 2019, 53, 478–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Runhaar, J.; Collard, D.C.; Singh, A.S.; Kemper, H.C.; van Mechelen, W.; Chinapaw, M. Motor fitness in Dutch youth: Differences over a 26-year period (1980–2006). J. Sci. Med. Sport. 2010, 13, 323–328. [Google Scholar] [CrossRef]
- Fraser, B.J.; Blizzard, L.; Tomkinson, G.R.; Lycett, K.; Wake, M.; Burgner, D.; Ranganathan, S.; Juonala, M.; Dwyer, T.; Venn, A.J.; et al. The great leap backward: Changes in the jumping performance of Australian children aged 11-12-years between 1985 and 2015. J. Sports Sci. 2019, 37, 748–754. [Google Scholar] [CrossRef]
- Malina, R.M.; Katzmarzyk, P.T. Physical activity and fitness in an international growth standard for preadolescent and adolescent children. Food Nutr. Bull. 2006, 27 (Suppl. 5), S295–S313. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. (Lond.) 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef]
- Grøntved, A.; Ried-Larsen, M.; Møller, N.C.; Kristensen, P.L.; Froberg, K.; Brage, S.; Andersen, L.B. Muscle strength in youth and cardiovascular risk in young adulthood (the European Youth Heart Study). Br. J. Sports Med. 2015, 49, 90–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, A.; Santos, D.A.; Hillman, C.H.; Sardinha, L.B. How does academic achievement relate to cardiorespiratory fitness, self-reported physical activity and objectively reported physical activity: A systematic review in children and adolescents aged 6–18 years. Br. J. Sports Med. 2018, 52, 1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mintjens, S.; Menting, M.D.; Daams, J.G.; van Poppel, M.N.M.; Roseboom, T.J.; Gemke, R.J.B.J. Cardiorespiratory Fitness in Childhood and Adolescence Affects Future Cardiovascular Risk Factors: A Systematic Review of Longitudinal Studies. Sports Med. 2018, 48, 2577–2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooke, H.L.; Corder, K.; Griffin, S.J.; van Sluijs, E.M. Physical activity maintenance in the transition to adolescence: A longitudinal study of the roles of sport and lifestyle activities in British youth. PLoS ONE 2014, 9, e89028. [Google Scholar] [CrossRef] [PubMed]
- Ried-Larsen, M.; Grøntved, A.; Kristensen, P.L.; Froberg, K.; Andersen, L.B. Moderate-and-vigorous physical activity from adolescence to adulthood and subclinical atherosclerosis in adulthood: Prospective observations from the European Youth Heart Study. Br. J. Sports Med. 2015, 49, 107–112. [Google Scholar] [CrossRef]
- Li, X.; Kearney, P.M.; Keane, E.; Harrington, J.M.; Fitzgerald, A.P. Levels and sociodemographic correlates of accelerometer-based physical activity in Irish children: A cross-sectional study. J. Epidemiol. Community Health 2017, 71, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Lutfiyya, M.N.; Lipsky, M.S.; Wisdom-Behounek, J.; Inpanbutr-Martinkus, M. Is rural residency a risk factor for overweight and obesity for U.S. children? Obesity (Silver Spring) 2007, 15, 2348–2356. [Google Scholar] [CrossRef]
- Ujević, T.; Sporis, G.; Milanović, Z.; Pantelić, S.; Neljak, B. Differences between health-related physical fitness profiles of Croatian children in urban and rural areas. Coll. Antropol. 2013, 37, 75–80. [Google Scholar]
- Howe, C.A.; Casapulla, S.; Shubrook, J.H.; Lopez, P.; Grijalva, M.; Berryman, D.E. Regional Variations in Physical Fitness and Activity in Healthy and Overweight Ecuadorian Adolescents. Children 2018, 5, 104. [Google Scholar] [CrossRef] [Green Version]
- Chillón, P.; Ortega, F.B.; Ferrando, J.A.; Casajus, J.A. Physical fitness in rural and urban children and adolescents from Spain. J. Sci. Med. Sport 2011, 14, 417–423. [Google Scholar] [CrossRef]
- Sandercock, G.R.H.; Ogunleye, A.; Voss, C. Comparison of cardiorespiratory fitness and body mass index between rural and urban youth: Findings from the East of England Healthy Hearts Study. Pediatr. Int. 2011, 53, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Tishukaj, F.; Shalaj, I.; Gjaka, M.; Ademi, B.; Ahmetxhekaj, R.; Bachl, N.; Tschan, H.; Wessner, B. Physical fitness and anthropometric characteristics among adolescents living in urban or rural areas of Kosovo. BMC Public Health. 2017, 17, 711. [Google Scholar] [CrossRef] [PubMed]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Mon. Kinderheilkd. 2001, 149, 807–818. [Google Scholar] [CrossRef] [Green Version]
- Bös, K. Handbuch Motorische Tests: Sportmotorische Tests, motorische Funktionstests, Fragebogen zur Körperlich-Sportlichen Aktivität und Sportpsychologische Diagnoseverfahren, 2nd ed.; Hogrefe: Göttingen, Germany, 2001. [Google Scholar]
- Bundesanstalt Statistik Österreich. Urban-Rural-Typologie; Statistik Austria: Vienna, Austria, 2016. [Google Scholar]
- Rauner, A.; Mess, F.; Woll, A. The relationship between physical activity, physical fitness and overweight in adolescents: A systematic review of studies published in or after 2000. BMC Pediatr. 2013, 13, 19. [Google Scholar] [CrossRef] [Green Version]
- Greier, K.; Drenowatz, C. Bidirectional association between weight status and motor skills in adolescents: A 4-year longitudinal study. Wien. Klin. Wochenschr. 2018, 130, 314–320. [Google Scholar] [CrossRef]
- Sylejmani, B.; Myrtaj, N.; Maliqi, A.; Gontarev, S.; Georgiev, G.; Kalac, R. Physical fitness in children and adolescents in rural and urban areas. J. Hum. Sport Exerc. 2019, 14, 866–875. [Google Scholar] [CrossRef]
- Kriemler, S.; Manser-Wenger, S.; Zahner, L.; Braun-Fahrländer, C.; Schindler, C.; Puder, J.J. Reduced cardiorespiratory fitness, low physical activity and an urban environment are independently associated with increased cardiovascular risk in children. Diabetologia 2008, 51, 1408–1415. [Google Scholar] [CrossRef] [Green Version]
- Tinazci, C.; Emiroglu, O. Physical fitness of rural children compared with urban children in North Cyprus: A normative study. J. Phys. Act. Health 2009, 6, 88–92. [Google Scholar] [CrossRef]
- Bürgi, F.; Meyer, U.; Granacher, U.; Schindler, C.; Marques-Vidal, P.; Kriemler, S.; Puder, J.J. Relationship of physical activity with motor skills, aerobic fitness and body fat in preschool children: A cross-sectional and longitudinal study (Ballabeina). Int. J. Obes. (Lond.) 2011, 35, 937–944. [Google Scholar] [CrossRef] [Green Version]
- Dencker, M.; Thorsson, O.; Karlsson, M.K.; Lindén, C.; Wollmer, P.; Andersen, L.B. Daily physical activity related to aerobic fitness and body fat in an urban sample of children. Scand. J. Med. Sci. Sports 2008, 18, 728–735. [Google Scholar] [CrossRef]
- Strong, W.B.; Malina, R.M.; Blimkie, C.J.; Daniels, S.R.; Dishman, R.K.; Gutin, B.; Hergenroeder, A.C.; Must, A.; Nixon, P.A.; Pivarnik, J.M.; et al. Evidence based physical activity for school-age youth. J. Pediatr. 2005, 146, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Malina, R.M.; Bouchard, C. Physical activity, physical fitness, and coronary heart disease risk factors in youth: The Québec Family Study. Prev. Med. 1999, 29 Pt 1, 555–562. [Google Scholar] [CrossRef]
- Huang, Y.C.; Malina, R.M. Physical activity and health-related physical fitness in Taiwanese adolescents. J. Physiol. Anthropol. Appl. Hum. Sci. 2002, 21, 11–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, F.B.; Ruiz, J.R.; Hurtig-Wennlöf, A.; Sjöström, M. Physically active adolescents are more likely to have a healthier cardiovascular fitness level independently of their adiposity status. The European youth heart study. Rev. Esp. Cardiol. 2008, 61, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.H.; Jones, S.J.; Sun, H.; Probst, J.C.; Merchant, A.T.; Cavicchia, P. Diet, physical activity, and sedentary behaviors as risk factors for childhood obesity: An urban and rural comparison. Child. Obes. 2012, 8, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Bell, L.; Ullah, S.; Olds, T.; Magarey, A.; Leslie, E.; Jones, M.; Miller, M.; Cobiac, L. Prevalence and socio-economic distribution of eating, physical activity and sedentary behaviour among South Australian children in urban and rural communities: Baseline findings from the OPAL evaluation. Public Health 2016, 140, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Drenowatz, C.; Greier, K. Cross-sectional and longitudinal association of sports participation, media consumption and motor competence in youth. Scand. J. Med. Sci. Sports 2019, 29, 854–861. [Google Scholar] [CrossRef]
- Pasek, M.; Szark-Eckardt, M.; Wilk, B.; Zuzda, J.; Żukowska, H.; Opanowska, M.; Kuska, M.; Dróżdż, R.; Kuśmierczyk, M.; Sakłak, W.; et al. Physical Fitness as Part of the Health and Well-Being of Students Participating in Physical Education Lessons Indoors and Outdoors. Int. J. Environ. Res. Public Health 2020, 17, 309. [Google Scholar] [CrossRef] [Green Version]
- Panczyk, W. Biolgoical-Medical and Didactic Results of Physical Education Class Held Outdoors or Indoors; ODN: Zamosc, Poland, 1999. [Google Scholar]
- McKenzie, T.; Feldman, H.; Woods, S.; Romereo, K.; Dahlstrom, V.; Stone, E.; Strikmiller, P.K.; Williston, J.M.; Harsha, D.W. Children’s activity levels and lessons context during third-grade physical education. Res. Q. Erxerc. Sport 1995, 66, 184–193. [Google Scholar] [CrossRef]
- Das, P.; Chatterjee, P. Urban-rural contrasts in motor fitness components of youngster footballers in West Bengal, India. J. Hum. Sport Exerc. 2013, 8, 797–805. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Bennett, K.J.; Harun, N.; Probst, J.C. Urban-rural differences in overweight status and physical inactivity among US children aged 10–17 years. J. Rural Health 2008, 24, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; O’Hara, B.J.; Rogers, K.; St George, A.; Bauman, A. Contribution of organized and nonorganized activity to children’s motor skills and fitness. J. Sch. Health 2014, 84, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Lawson, C.T. Do attributes in the physical environment influence children’s physical activity? A review of the literature. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molnar, B.E.; Gortmaker, S.L.; Bull, F.C.; Buka, S.L. Unsafe to play? Neighborhood disorder and lack of safety predict reduced physical activity among urban children and adolescents. Am. J. Health Promot. 2004, 18, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M.; Bouchard, C.; Bar-Or, O. Growth, Maturation, and Physical Activity, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total Sample (N = 18,168) | Urban (N = 4118) | Rural (N = 14,050) | p-value | |
|---|---|---|---|---|
| Overweight/obesity (%) | 14.7% | 15.8% | 14.3% | 0.015 |
| Age (years) | 8.4 ± 0.8 | 8.3 ± 0.7 | 8.4 ± 0.8 | <0.001 |
| Height (cm) | 132.2 ± 7.0 | 132.0 ± 6.9 | 132.3 ± 7.1 | 0.027 |
| Weight (kg) | 29.8 ± 7.1 | 29.8 ± 7.3 | 29.8 ± 7.1 | 0.503 |
| BMI percentile | 51.8 ± 29.7 | 52.8 ± 29.9 | 51.5 ± 29.7 | 0.013 |
| Vertical jump (cm) | 19.9 ± 3.8 | 19.6 ± 3.8 | 20.0 ± 3.9 | <0.001 |
| Medicine ball push (cm) | 351 ± 73 | 349 ± 72 | 351 ± 74 | 0.158 |
| Tapping (# in 6 s) | 45.0 ± 7.5 | 44.2 ± 7.5 | 45.2 ± 7.5 | <0.001 |
| 10 m sprint (s) | 2.28 ± 0.17 | 2.30 ± 0.17 | 2.27 ± 0.17 | <0.001 |
| Agility test (s) | 20.0 ± 3.6 | 20.5 ± 3.8 | 19.8 ± 3.6 | <0.001 |
| Throw and catch (# in 30 s) | 15.2 ± 7.7 | 14.5 ± 7.6 | 15.4 ± 7.7 | <0.001 |
| Stand-and-reach (cm) | 1.7 ± 6.6 | 1.9 ± 6.8 | 1.6 ± 6.6 | 0.031 |
| 6 min run (m) | 982 ± 134 | 961 ± 135 | 989 ± 133 | <0.001 |
| GIRLS | BOYS | |||
|---|---|---|---|---|
| Urban (N = 2039) | Rural (N = 6803) | Urban (N = 2079) | Rural (N = 7247) | |
| Vertical jump (cm) 1,2 | 19.0 ± 3.6 | 19.5 ± 3.7 | 20.1 ± 3.9 | 20.4 ± 3.9 |
| Medicine ball push (cm) | 321 ± 64 | 327 ± 66 | 372 ± 73 | 375 ± 75 |
| Tapping (# in 6 s) 1,2 | 42.0 ± 7.2 | 43.3 ± 7.4 | 46.4 ± 7.1 | 47.0 ± 7.2 |
| 10 m sprint (s) 1,2 | 2.34 ± 0.17 | 2.30 ± 0.17 | 2.26 ± 0.16 | 2.24 ± 0.17 |
| Agility test (s) 1,2 | 21.1 ± 3.7 | 20.3 ± 3.5 | 19.8 ± 3.8 | 19.4 ± 3.6 |
| Throw and catch (# in 30 s) 1 | 11.8 ± 7.1 | 13.3 ± 7.4 | 17.1 ± 7.2 | 17.4 ± 7.4 |
| Stand-and-reach (cm) 1 | 3.6 ± 6.6 | 3.2 ± 6.5 | 0.2 ± 6.5 | 0.1 ± 6.4 |
| 6 min run (m) 1,2 | 926 ± 122 | 956 ± 119 | 996 ± 138 | 1020 ± 138 |
| Non-Overweight | Overweight/Obese | |||
|---|---|---|---|---|
| Urban (N = 3466) | Rural (N = 12040) | Urban (N = 652) | Rural (N = 2010) | |
| Vertical jump (cm) 1 | 20.2 ± 3.5 | 20.5 ± 3.6 | 16.8 ± 3.2 | 17.0 ± 3.2 |
| Medicine ball push (cm) | 344 ± 60 | 346 ± 60 | 381 ± 80 | 381 ± 77 |
| Tapping (# in 6 s) 1 | 44.6 ± 7.0 | 45.4 ± 7.0 | 43.2 ± 6.9 | 43.9 ± 6.9 |
| 10 m sprint (s) 1,2 | 2.27 ± 0.16 | 2.25 ± 0.15 | 2.42 ± 0.18 | 2.39 ± 0.19 |
| Agility test (s) 1,2 | 19.9 ± 3.1 | 19.4 ± 3.1 | 23.3 ± 4.6 | 22.6 ± 4.5 |
| Throw and catch (# in 30 s) 1 | 14.6 ± 6.4 | 15.3 ± 6.4 | 15.6 ± 6.5 | 16.0 ± 6.5 |
| Stand-and-reach (cm) | 1.9 ± 6.4 | 1.7 ± 6.4 | 1.3 ± 6.7 | 0.9 ± 6.7 |
| 6 min run (m) 1,2 | 985 ± 118 | 1008 ± 118 | 846 ± 124 | 873 ± 125 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drenowatz, C.; Hinterkörner, F.; Greier, K. Physical Fitness in Upper Austrian Children Living in Urban and Rural Areas: A Cross-Sectional Analysis with More Than 18,000 Children. Int. J. Environ. Res. Public Health 2020, 17, 1045. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031045
Drenowatz C, Hinterkörner F, Greier K. Physical Fitness in Upper Austrian Children Living in Urban and Rural Areas: A Cross-Sectional Analysis with More Than 18,000 Children. International Journal of Environmental Research and Public Health. 2020; 17(3):1045. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031045
Chicago/Turabian StyleDrenowatz, Clemens, Franz Hinterkörner, and Klaus Greier. 2020. "Physical Fitness in Upper Austrian Children Living in Urban and Rural Areas: A Cross-Sectional Analysis with More Than 18,000 Children" International Journal of Environmental Research and Public Health 17, no. 3: 1045. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031045