Exhaled Breath Analysis in Diagnosis of Malignant Pleural Mesothelioma: Systematic Review


Abstract
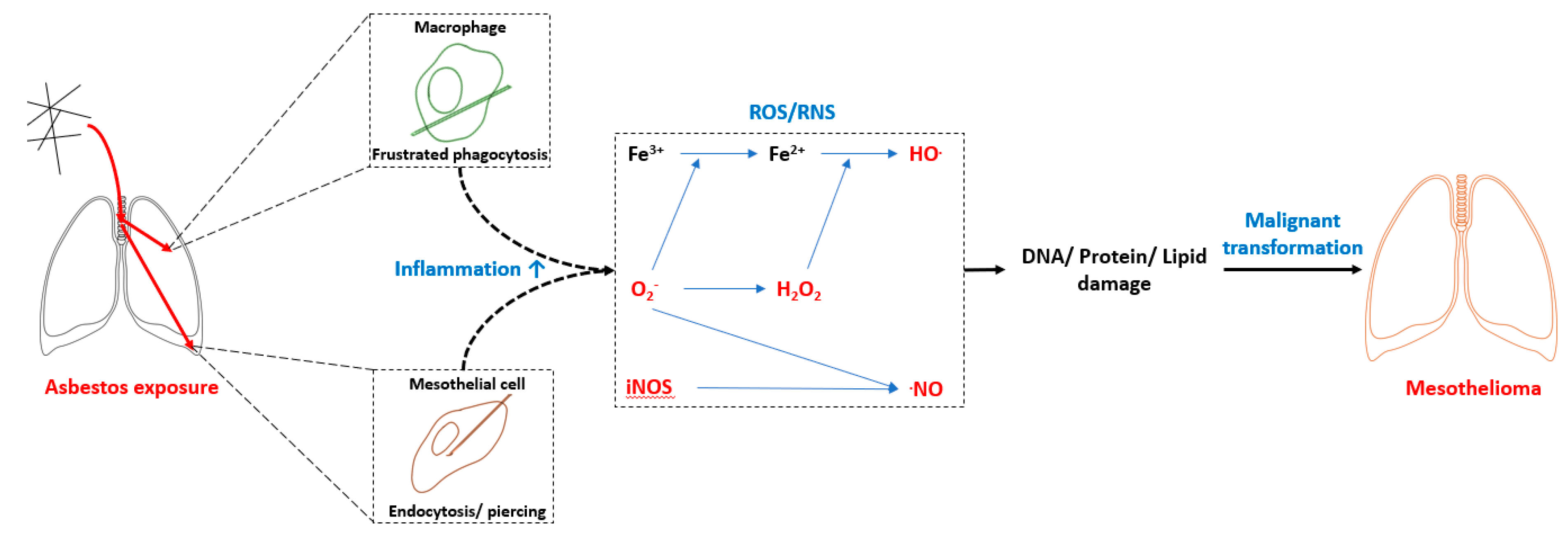
:1. Introduction
2. Exhaled Breath Analysis
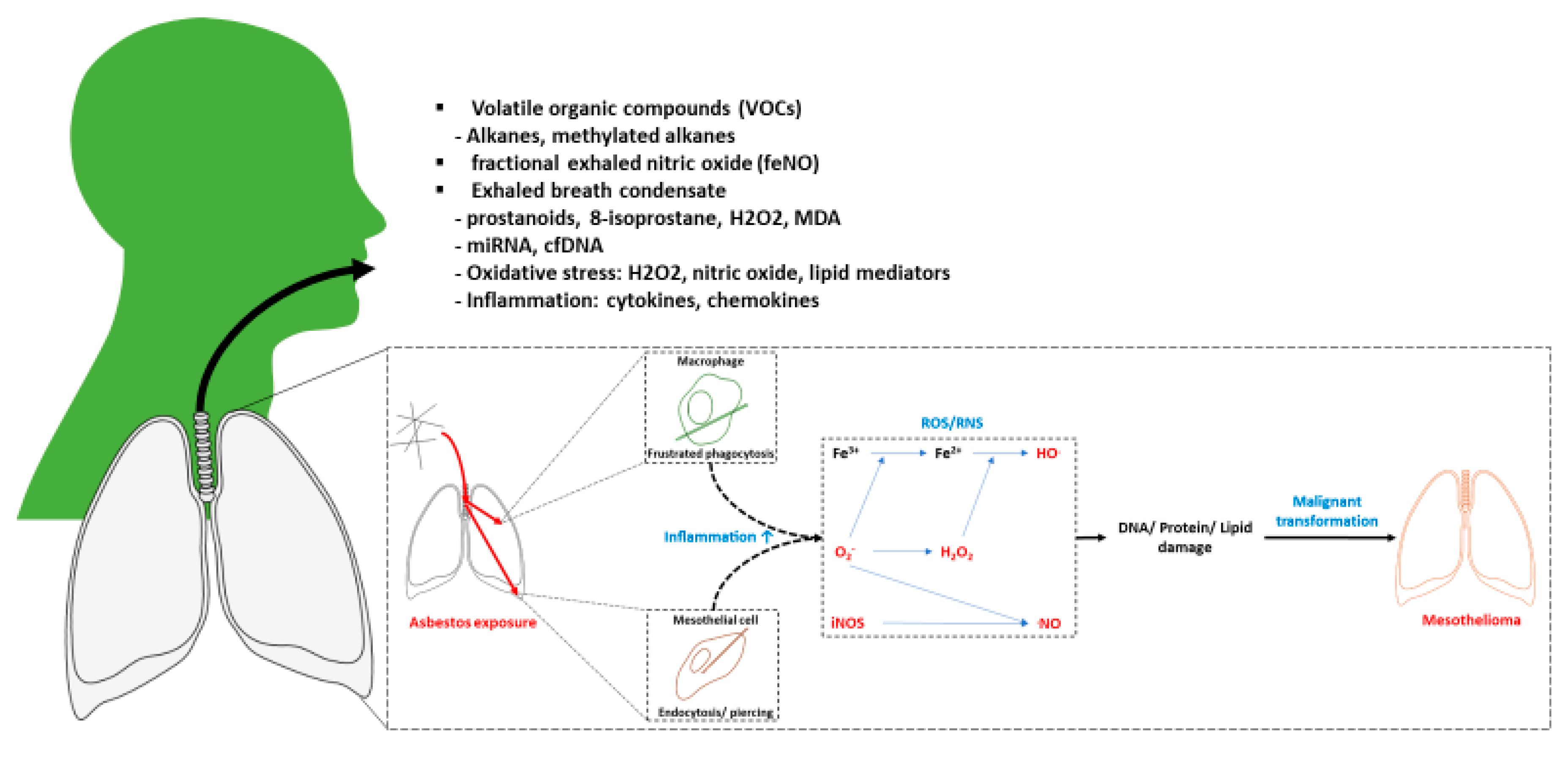
2.1. Exhaled Breath Composition
2.2. Sample Collection
2.3. Detection Methods
2.3.1. Analytical Methods
2.3.2. Pattern-Recognition-Based Methods
3. Methods
3.1. Search Strategy
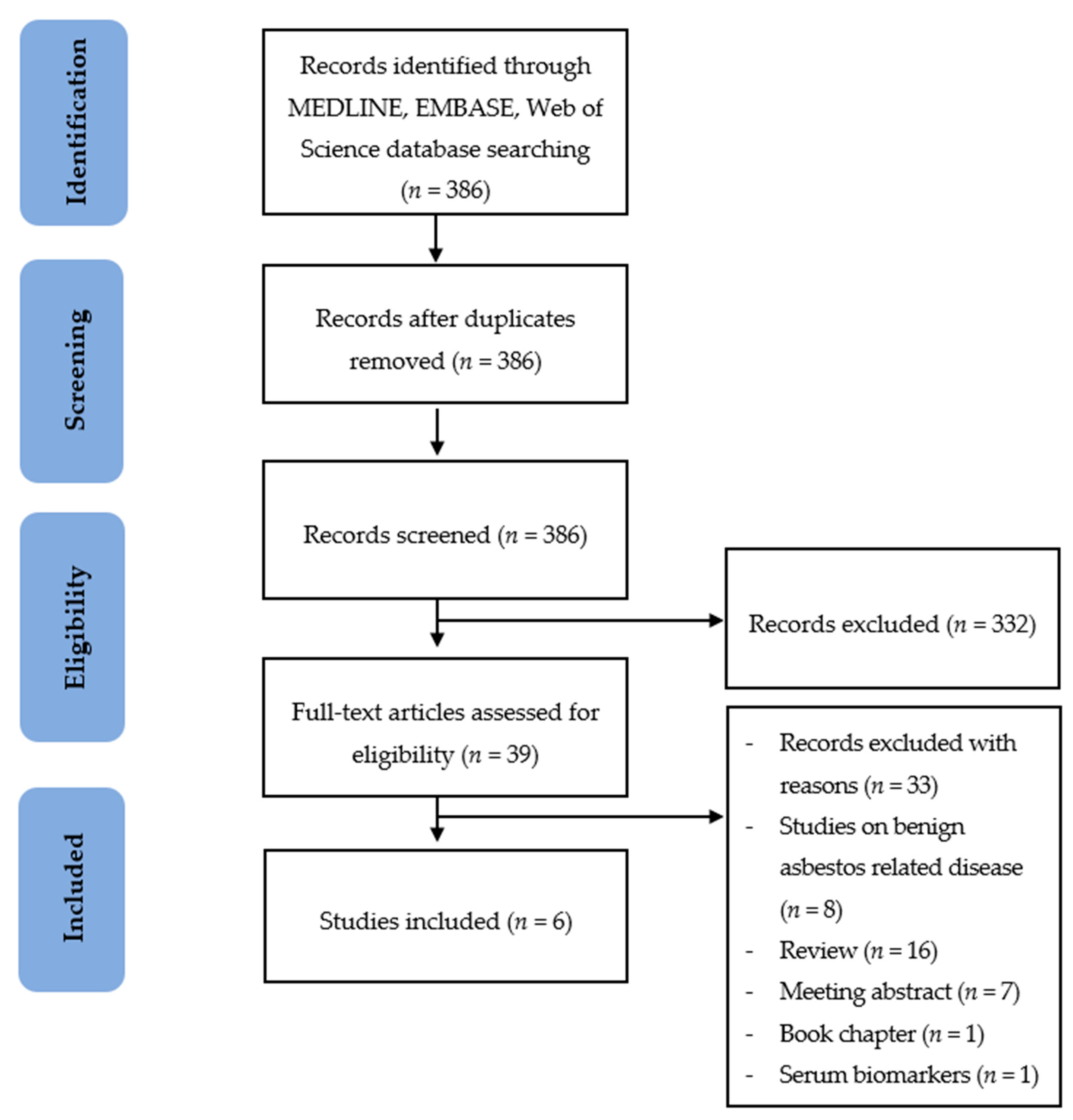
3.2. Study Selection
- Studies in English
- Studies on human samples
- Studies that included pleura biopsy confirmed MPM patients
- Studies that assessed diagnostic accuracy of exhaled breath methods in diagnosis and/or prognosis of MPM. Studies were excluded if a diagnostic marker discovery was performed only in biofluids other than exhaled breath.
3.3. Data Extraction and Synthesis
3.4. Quality Assessment
4. Results
4.1. Quality Assessment of Studies
4.2. Study Characteristics
4.3. Exhaled Breath Collection and Analysis Methods
4.3.1. Gas Chromatography Coupled to Mass Spectrometry (GC–MS)
4.3.2. Ion Mobility Spectrometry Coupled to Multi-capillary Columns (IMS–MCC)
4.3.3. Sensor-Based Technologies (Electronic Nose)
4.4. Statistical Methods Used in Studies
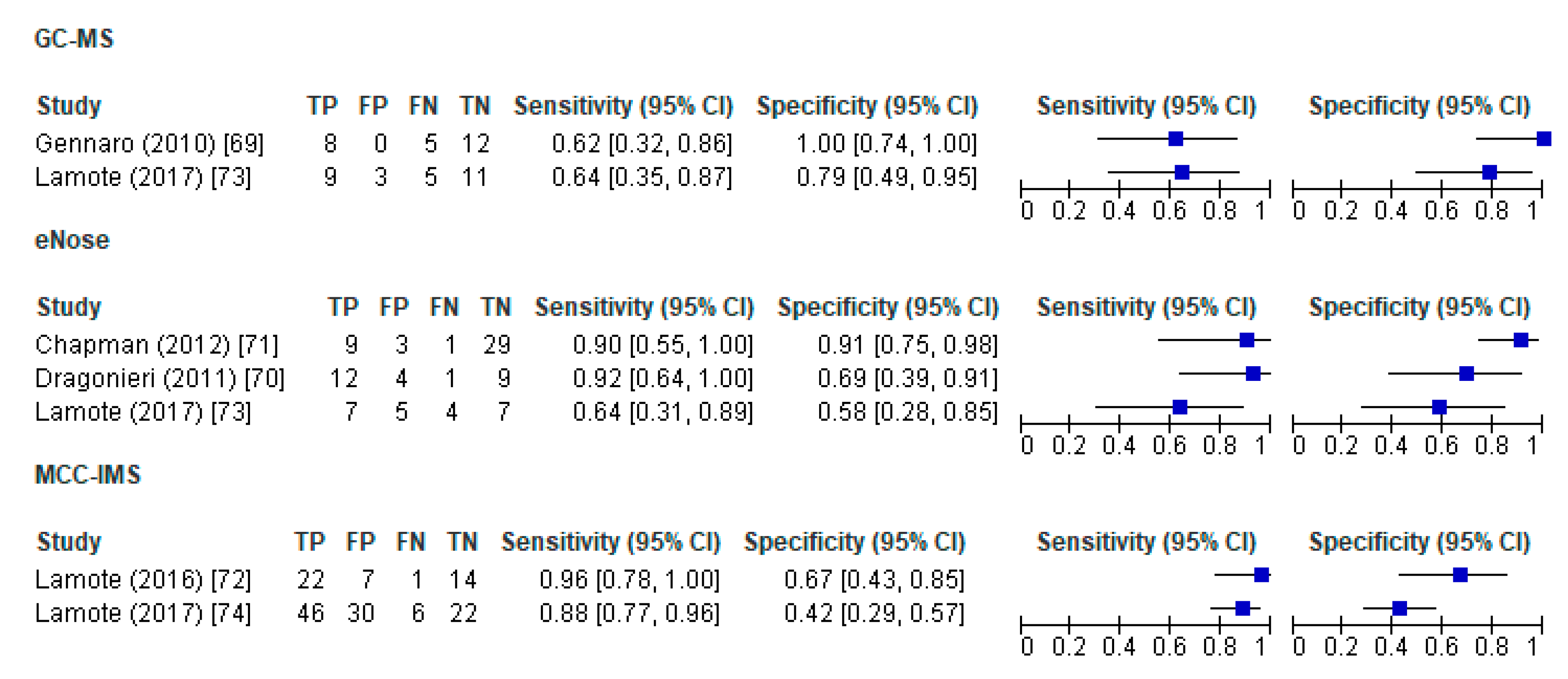
4.4.1. GC–MS Studies
4.4.2. IMS–MCC Studies
4.4.3. E-nose Studies
5. Discussion
6. Conclusions
Supplementary Materials
Funding
Acknowledgments
Conflicts of Interest
References
- Markowitz, S. Asbestos-related lung cancer and malignant mesothelioma of the pleura: Selected current issues. Semin. Respir. Crit. Care Med. 2015, 36, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazurek, J.M.; Syamlal, G.; Wood, J.M.; Hendricks, S.A.; Weston, A. Malignant Mesothelioma Mortality—United States, 1999–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Odgerel, C.-O.; Takahashi, K.; Sorahan, T.; Driscoll, T.; Fitzmaurice, C.; Yoko-O, M.; Sawanyawisuth, K.; Furuya, S.; Tanaka, F.; Horie, S.; et al. Estimation of the global burden of mesothelioma deaths from incomplete national mortality data. Occup. Environ. Med. 2017, 74, 851–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, J.C.; Sleggs, C.A.; Marchand, P. Diffuse pleural mesothelioma and asbestos exposure in the North Western Cape Province. Occup. Environ. Med. 1960, 17, 260–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doll, R. Mortality from lung cancer in asbestos workers 1955. Occup. Environ. Med. 1993, 50, 485–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, R.Y.; Sterman, D.H.; Haas, A.R. Malignant Mesothelioma: Has Anything Changed? Semin. Respir. Crit. Care Med. 2019, 40, 347–360. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risk to Humans. Arsenic, Metals, Fibres and Dusts. Lyon (FR): International Agency for Research on Cancer. (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 100C.) ERIONITE. 2012. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK304368/ (accessed on 25 October 2019).
- Metintas, M.; Hillerdal, G.; Metintas, S. Malignant mesothelioma due to environmental exposure to erionite: Follow-up of a Turkish emigrant cohort. Eur. Respir. J. 1999, 13, 523–526. [Google Scholar] [CrossRef] [Green Version]
- National Research Council (US) Committee on Nonoccupational Health Risks of Asbestiform Fibers. 2, Asbestiform Fibers: Historical Background, Terminology, and Physicochemical Properties. In Asbestiform Fibers: Nonoccupational Health Risks; National Academies Press: Washington, DC, USA, 1984. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK216753/ (accessed on 25 October 2019).
- Korchevskiy, A.; Rasmuson, J.O.; Rasmuson, E.J. Rasmuson. Empirical model of mesothelioma potency factors for different mineral fibers based on their chemical composition and dimensionality. Inhal. Toxicol. 2019, 31, 180–191. [Google Scholar] [CrossRef] [Green Version]
- Donaldson, K.; Murphy, F.A.; Duffin, R.; Poland, C. Asbestos, carbon nanotubes and the pleural mesothelium: A review of the hypothesis regarding the role of long fibre retention in the parietal pleura, inflammation and mesothelioma. Part Fibre Toxicol. 2010, 7. [Google Scholar] [CrossRef] [Green Version]
- Yap, T.A.; Aerts, J.G.; Popat, S.; Fennell, D.A. Novel insights into mesothelioma biology and implications for therapy. Nat. Rev. Cancer 2017, 17, 475–488. [Google Scholar] [CrossRef] [PubMed]
- Kehrer, J.P. The Haber—Weiss reaction and mechanisms of toxicity. Toxicology 2000, 149, 43–50. [Google Scholar] [CrossRef]
- Pelclová, D.; Fenclová, Z.; Kacer, P.; Kuzma, M.; Navrátil, T.; Lebedová, J. Increased 8-isoprostane, a marker of oxidative stress in exhaled breath condensate in subjects with asbestos exposure. Ind. Heal. 2008, 46, 484–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibby, A.C.; Tsim, S.; Kanellakis, N.; Ball, H.; Talbot, D.C.; Blyth, K.G.; Maskell, N.A.; Psallidas, I. Malignant pleural mesothelioma: an update on investigation, diagnosis and treatment. Eur. Respir. Rev. 2016, 25, 472–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ledda, C.; Senia, P.; Rapisarda, V. Biomarkers for Early Diagnosis and Prognosis of Malignant Pleural Mesothelioma: The Quest Goes on. Cancers 2018, 10, 203. [Google Scholar] [CrossRef] [Green Version]
- Baas, P.; Fennell, D.; Kerr, K.M.; Van Schil, P.E.; Haas, R.L.; Peters, S. Malignant pleural mesothelioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, v31–v39. [Google Scholar] [CrossRef]
- Porcel, J.M. Biomarkers in the diagnosis of pleural diseases: A 2018 update. Ther. Adv Respir. Dis. 2018, 12. [Google Scholar] [CrossRef]
- Foddis, R.; Bonotti, A.; Landi, S.; Fallahi, P.; Guglielmi, G.; Cristaudo, A. Biomarkers in the prevention and follow-up of workers exposed to asbestos. J. Thorac. Dis. 2018, 10, S360–S368. [Google Scholar] [CrossRef] [Green Version]
- Hooper, C.E.; Morley, A.J.; Virgo, P.; Harvey, J.E.; Kahan, B.; Maskell, N.A. A prospective trial evaluating the role of mesothelin in undiagnosed pleural effusions. Eur. Respir. J. 2013, 41, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Jakubec, P.; Pelclova, D.; Smolkova, P.; Kolek, V.; Nakladalova, M. Significance of serum mesothelin in an asbestos-exposed population in the Czech Republic. Biomed. Pap. 2015, 159, 472–479. [Google Scholar] [CrossRef] [Green Version]
- Cristaudo, A.; Foddis, R.; Vivaldi, A.; Guglielmi, G.; DiPalma, N.; Filiberti, R.; Neri, M.; Ceppi, M.; Paganuzzi, M.; Ivaldi, G.P.; et al. Clinical Significance of Serum Mesothelin in Patients with Mesothelioma and Lung Cancer. Clin. Cancer Res. 2007, 13, 5076–5081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristaduo, A.; Foddis, R.; Bonotti, A.; Simonini, S.; Vivaldi, A.; Guglielmi, G.; Bruno, R.; Gemignani, F.; Landi, S. Two novel polymorphisms in 5’flanking region of the mesothelin gene are associated with soluble mesothelin-related peptide (SMRP) levels. Int. J. Biol. Markers 2011, 26, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Cristaudo, A.; Foddis, R.; Bonotti, A.; Simonini, S.; Vivaldi, A.; Guglielmi, G.; Bruno, R.; Landi, D.; Gemignani, F.; Landi, S. Polymorphisms in the putative micro-RNA-binding sites of mesothelin gene are associated with serum levels of mesothelin-related protein. Occup. Environ. Med. 2010, 67, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Felten, M.K.; Khatab, K.; Knoll, L.; Schettgen, T.; Müller-Berndorff, H.; Kraus, T. Changes of mesothelin and osteopontin levels over time in formerly asbestos-exposed power industry workers. Int. Arch. Occup. Environ. Health 2014, 87, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.-D.; Liu, X.-F.; Liu, X.-C.; Ding, C.-M.; Hu, C.-J. Diagnostic accuracy of osteopontin for malignant pleural mesothelioma: A systematic review and meta-analysis. Clin. Chim. Acta 2014, 433, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Greillier, L.; Baas, P.; Welch, J.J.; Hasan, B.; Passioukov, A. Biomarkers for Malignant Pleural Mesothelioma. Mol. Diagn. Ther. 2008, 12, 375–390. [Google Scholar] [CrossRef] [PubMed]
- Cristaudo, A.; Bonotti, A.; Simonini, S.; Vivaldi, A.; Guglielmi, G.; Ambrosino, N.; Chella, A.; Lucchi, M.; Mussi, A.; Foddis, R. Combined Serum Mesothelin and Plasma Osteopontin Measurements in Malignant Pleural Mesothelioma. J. Thorac. Oncol. 2011, 6, 1587–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnen, G.; MoMar Study Group; Burek, K.; Raiko, I.; Wichert, K.; Pesch, B.; Weber, D.G.; Lehnert, M.; Casjens, S.; Hagemeyer, O.; et al. Prediagnostic detection of mesothelioma by circulating calretinin and mesothelin – a case-control comparison nested into a prospective cohort of asbestos-exposed workers. Sci. Rep. 2018, 8, 14321. [Google Scholar] [CrossRef]
- Jiménez-Ramírez, C.; Casjens, S.; Juárez-Pérez, C.A.; Raiko, I.; Del Razo, L.M.; Taeger, D.; Calderón-Aranda, E.S.; Rihs, H.-P.; Acosta-Saavedra, L.C.; Weber, D.G.; et al. Mesothelin, Calretinin, and Megakaryocyte Potentiating Factor as Biomarkers of Malignant Pleural Mesothelioma. Lung 2019, 197, 641–649. [Google Scholar] [CrossRef]
- Davis, M.D.; Fowler, S.J.; Montpetit, A.J. Montpetit. Exhaled breath testing—A tool for the clinician and researcher. Paediatr. Respir. Rev. 2019, 29, 37–41. [Google Scholar] [CrossRef]
- Davis, M.D.; Montpetit, A.; Hunt, J. Exhaled breath condensate: An overview. Immunol. Allergy Clin. N. Am. 2012, 32, 363–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haick, H.; Broza, Y.Y.; Mochalski, P.; Ruzsanyi, V.; Amann, A. Assessment, origin, and implementation of breath volatile cancer markers. Chem. Soc002E Rev. 2014, 43, 1423–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amann, A.; Miekisch, W.; Schubert, J.; Buszewski, B.; Ligor, T.; Jezierski, T.; Pleil, J.; Risby, T. Analysis of Exhaled Breath for Disease Detection. Annu. Rev. Anal. Chem. 2014, 7, 455–482. [Google Scholar] [CrossRef] [PubMed]
- Van Der Schee, M.P.; Paff, T.; Brinkman, P.; Van Aalderen, W.M.C.; Haarman, E.G.; Sterk, P.J. Breathomics in Lung Disease. Chest 2015, 147, 224–231. [Google Scholar] [CrossRef]
- Lee, C.W.; Mohr, S.N.; Weisel, C.P. Toxicokinetics of human exposure to methyl tertiary-butyl ether (MTBE) following short-term controlled exposures. J. Expo. Sci. Environ. Epidemiol. 2001, 11, 67–68. [Google Scholar] [CrossRef] [Green Version]
- Lavra, L.; Catini, A.; Ulivieri, A.; Capuano, R.; Salehi, L.B.; Sciacchitano, S.; Bartolazzi, A.; Nardis, S.; Paolesse, R.; Martinelli, E.; et al. Investigation of VOCs associated with different characteristics of breast cancer cells. Sci. Rep. 2015, 5, 13246. [Google Scholar] [CrossRef] [Green Version]
- Dutta, D.; Chong, N.S.; Lim, S.H. Endogenous volatile organic compounds in acute myeloid leukemia: Origins and potential clinical applications. J. Breath Res. 2018, 12, 034002. [Google Scholar] [CrossRef]
- Watanabe, M. Polymorphic CYP genes and disease predisposition—what have the studies shown so far? Toxicol. Lett. 1998, 102, 167–171. [Google Scholar] [CrossRef]
- Antoniou, S.X.; Gaude, E.; Ruparel, M.; Van Der Schee, M.P.; Janes, S.M.; Rintoul, R.C.; on behalf of LuCID research group. The potential of breath analysis to improve outcome for patients with lung cancer. J. Breath Res. 2019, 13, 034002. [Google Scholar] [CrossRef] [Green Version]
- Poli, D.; Carbognani, P.; Corradi, M.; Goldoni, M.; Acampa, O.; Balbi, B.; Bianchi, L.; Rusca, M.; Mutti, A. Exhaled volatile organic compounds in patients with non-small cell lung cancer: cross sectional and nested short-term follow-up study. Respir. Res. 2005, 6, 71. [Google Scholar] [CrossRef] [Green Version]
- Filipiak, W.; Filipiak, A.; Sponring, A.; Schmid, T.; Zelger, B.; Ager, C.; Klodzinska, E.; Denz, H.; Pizzini, A.; Lucciarini, P.; et al. Comparative analyses of volatile organic compounds (VOCs) from patients, tumors and transformed cell lines for the validation of lung cancer-derived breath markers. J. Breath Res. 2014, 8, 27111. [Google Scholar] [CrossRef] [PubMed]
- Marien, E.; Meister, M.; Muley, T.; Fieuws, S.; Bordel, S.; Derua, R.; Spraggins, J.; Van De Plas, R.; Dehairs, J.; Wouters, J.; et al. Non-small cell lung cancer is characterized by dramatic changes in phospholipid profiles. Int. J. Cancer 2015, 137, 1539–1548. [Google Scholar] [CrossRef] [PubMed]
- Chow, S.; Campbell, C.; Sandrini, A.; Thomas, P.S.; Johnson, A.R.; Yates, D.H. Exhaled breath condensate biomarkers in asbestos-related lung disorders. Respir. Med. 2009, 103, 1091–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandrini, A.; Johnson, A.R.; Thomas, P.S.; Yates, D.H. Fractional exhaled nitric oxide concentration is increased in asbestosis and pleural plaques. Respirol. 2006, 11, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Lehtonen, H.; Oksa, P.; Lehtimäki, L.; Sepponen, A.; Nieminen, R.; Kankaanranta, H.; Saarelainen, S.; Järvenpää, R.; Uitti, J.; Moilanen, E. Increased alveolar nitric oxide concentration and high levels of leukotriene B4 and 8-isoprostane in exhaled breath condensate in patients with asbestosis. Thorax 2007, 62, 602–607. [Google Scholar] [CrossRef] [Green Version]
- Ahmadzai, H.; Huang, S.; Hettiarachchi, R.; Lin, J.-L.; Thomas, P.S.; Zhang, Q. Exhaled breath condensate: A comprehensive update. Clin. Chem. Lab. Med. 2013, 51, 1343–1361. [Google Scholar] [CrossRef]
- Ng, A.W.; Bidani, A.; Thomas, A. Heming. Innate host defense of the lung: Effects of lung-lining fluid pH. Lung 2004, 182, 297–317. [Google Scholar] [CrossRef]
- Corradi, M.; Gergelova, P.; Mutti, A. Use of exhaled breath condensate to investigate occupational lung diseases. Curr. Opin. Allergy Clin. Immunol. 2010, 10, 93–98. [Google Scholar] [CrossRef]
- Milne, G.L.; Yin, H.; Hardy, K.D.; Davies, S.S.; Roberts, L.J., 2nd. Isoprostane generation and function. Chem. Rev. 2011, 111, 5973–5996. [Google Scholar] [CrossRef] [Green Version]
- Pelclova, D.; Fenclová, Z.; Vlcková, S.; Lebedová, J.; Syslová, K.; Pecha, O.; Belácek, J.; Navrátil, T.; Kuzma, M.; Kacer, P. Leukotrienes B4, C4, D4 and E4 in the exhaled breath condensate (EBC), blood and urine in patients with pneumoconiosis. Ind. Health 2012, 50, 299–306. [Google Scholar]
- Alonso, M.; Sanchez, J.M. Analytical challenges in breath analysis and its application to exposure monitoring. TrAC Trends Anal. Chem. 2013, 44, 78–89. [Google Scholar] [CrossRef] [Green Version]
- Wallace, M.A.G.; Pleil, J.D. Evolution of clinical and environmental health applications of exhaled breath research: Review of methods and instrumentation for gas-phase, condensate, and aerosols. Anal. Chim. Acta 2018, 1024, 18–38. [Google Scholar] [CrossRef]
- Horváth, I.; Barnes, P.J.; Loukides, S.; Sterk, P.J.; Högman, M.; Olin, A.-C.; Amann, A.; Antus, B.; Baraldi, E.; Bikov, A.; et al. A European Respiratory Society technical standard: exhaled biomarkers in lung disease. Eur. Respir. J. 2017, 49, 1600965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rattray, N.J.; Hamrang, Z.; Trivedi, D.K.; Goodacre, R.; Fowler, S.J. Taking your breath away: metabolomics breathes life in to personalized medicine. Trends Biotechnol. 2014, 32, 538–548. [Google Scholar] [CrossRef] [PubMed]
- Montuschi, P.; Santonico, M.; Mondino, C.; Pennazza, G.; Mantini, G.; Martinelli, E.; Capuano, R.; Ciabattoni, G.; Paolesse, R.; Di Natale, C.; et al. Diagnostic Performance of an Electronic Nose, Fractional Exhaled Nitric Oxide, and Lung Function Testing in Asthma. Chest 2010, 137, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Schubert, J.K.; Miekisch, W.; Geiger, K.; Nöldge–Schomburg, G.F. Breath analysis in critically ill patients: potential and limitations. Expert Rev. Mol. Diagn. 2004, 4, 619–629. [Google Scholar] [CrossRef]
- Cavaleiro Rufo, J.; Paciência, I.; Mendes, F.C.; Farraia, M.; Rodolfo, A.; Silva, D.; de Oliveira Fernandes, E.; Delgado, L.; Moreira, A. Exhaled breath condensate volatilome allows sensitive diagnosis of persistent asthma. Allergy 2019, 74, 527–534. [Google Scholar] [CrossRef]
- Baumbach, J.I. Ion mobility spectrometry coupled with multi-capillary columns for metabolic profiling of human breath. J. Breath Res. 2009, 3, 34001. [Google Scholar] [CrossRef]
- Tran, V.H.; Chan, H.P.; Thurston, M.; Jackson, P.; Lewis, C.; Yates, D.; Bell, G.; Thomas, P.S. Breath Analysis of Lung Cancer Patients Using an Electronic Nose Detection System. IEEE Sensors J. 2010, 10, 1514–1518. [Google Scholar] [CrossRef]
- Bikov, A.; Hernadi, M.; Korosi, B.Z.; Kunos, L.; Zsamboki, G.; Sutto, Z.; Tarnoki, A.D.; Tarnoki, D.L.; Losonczy, G.; Horváth, I. Expiratory flow rate, breath hold and anatomic dead space influence electronic nose ability to detect lung cancer. BMC Pulm. Med. 2014, 14, 202. [Google Scholar] [CrossRef] [Green Version]
- Gasparri, R.; Santonico, M.; Valentini, C.; Sedda, G.; Borri, A.; Petrella, F.; Maisonneuve, P.; Pennazza, G.; D’Amico, A.; Di Natale, C.; et al. Volatile signature for the early diagnosis of lung cancer. J. Breath Res. 2016, 10, 16007. [Google Scholar] [CrossRef] [PubMed]
- Dragonieri, S.; Annema, J.T.; Schot, R.; Van Der Schee, M.P.; Spanevello, A.; Carratu, P.; Resta, O.; Rabe, K.F.; Sterk, P.J. An electronic nose in the discrimination of patients with non-small cell lung cancer and COPD. Lung Cancer 2009, 64, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Review Manager (RevMan) [Computer Program]; Version 5.3; The Nordic Cochrane Centre; The Cochrane Collaboration: Copenhagen, Denmark, 2014.
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 23 September 2019).
- Thomson Reuters Endnote X9. Available online: https://endnote.com/product-details/ (accessed on 20 October 2019).
- De Gennaro, G.; Dragonieri, S.; Longobardi, F.; Musti, M.; Stallone, G.; Trizio, L.; Tutino, M. Chemical characterization of exhaled breath to differentiate between patients with malignant plueral mesothelioma from subjects with similar professional asbestos exposure. Anal. Bioanal. Chem. 2010, 398, 3043–3050. [Google Scholar] [CrossRef]
- Dragonieri, S.; Van Der Schee, M.P.; Massaro, T.; Schiavulli, N.; Brinkman, P.; Pinca, A.; Carratu, P.; Spanevello, A.; Resta, O.; Musti, M.; et al. An electronic nose distinguishes exhaled breath of patients with Malignant Pleural Mesothelioma from controls. Lung Cancer 2012, 75, 326–331. [Google Scholar] [CrossRef]
- Chapman, E.A.; Thomas, P.S.; Stone, E.; Lewis, C.; Yates, D.H. A breath test for malignant mesothelioma using an electronic nose. Eur. Respir. J. 2012, 40, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Lamote, K.; Vynck, M.; Van Cleemput, J.; Thas, O.; Nackaerts, K.; Van Meerbeeck, J.P. Detection of malignant pleural mesothelioma in exhaled breath by multicapillary column/ion mobility spectrometry (MCC/IMS). J. Breath Res. 2016, 10, 46001. [Google Scholar] [CrossRef]
- Lamote, K.; Brinkman, P.; Vandermeersch, L.; Vynck, M.; Sterk, P.J.; Van Langenhove, H.; Thas, O.; Van Cleemput, J.; Nackaerts, K.; Van Meerbeeck, J.P. Breath analysis by gas chromatography-mass spectrometry and electronic nose to screen for pleural mesothelioma: a cross-sectional case-control study. Oncotarget 2017, 8, 91593–91602. [Google Scholar] [CrossRef] [Green Version]
- Lamote, K.; Vynck, M.; Thas, O.; Van Cleemput, J.; Nackaerts, K.; Van Meerbeeck, J.P. Exhaled breath to screen for malignant pleural mesothelioma: a validation study. Eur. Respir. J. 2017, 50, 1700919. [Google Scholar] [CrossRef] [Green Version]
- Scherpereel, A.; Astoul, P.; Baas, P.; Berghmans, T.; Clayson, H.; de Vuyst, P.; Dienemann, H.; Galateau-Salle, F.; Hennequin, C.; Hillerdal, G.; et al. Guidelines of the European Respiratory Society and the European Society of Thoracic Surgeons for the management of malignant pleural mesothelioma. Eur. Respir. J. 2010, 35, 479–495. [Google Scholar] [CrossRef]
- Landi, M.T.; Consonni, D.; Rotunno, M.; Bergen, A.W.; Goldstein, A.M.; Lubin, J.H.; Goldin, L.; Alavanja, M.; Morgan, G.; Subar, A.F.; et al. Environment and Genetics in Lung cancer Etiology (EAGLE) study: An integrative population-based case-control study of lung cancer. BMC Public Heal. 2008, 8, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, P.; Zapp, J.A. Biologic activity of ε-caprolactam. CRC Crit. Rev. Toxicol. 1984, 13, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Altomare, D.F.; Di Lena, M.; Porcelli, F.; Trizio, L.; Travaglio, E.; Tutino, M.; Dragonieri, S.; Memeo, V.; de Gennaro, G. Exhaled volatile organic compounds identify patients with colorectal cancer. Br. J. Surg. 2013, 100, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Oguma, T.; Nagaoka, T.; Kurahashi, M.; Kobayashi, N.; Yamamori, S.; Tsuji, C.; Takiguchi, H.; Niimi, K.; Tomomatsu, H.; Tomomatsu, K.; et al. Clinical contributions of exhaled volatile organic compounds in the diagnosis of lung cancer. PLoS ONE 2017, 12, e0174802. [Google Scholar] [CrossRef] [PubMed]
- agniau, S.; Lamote, K.; Van Meerbeeck, J.P.; Vermaelen, K.Y. Biomarkers for early diagnosis of malignant mesothelioma: Do we need another moonshot? Oncotarget 2017, 8, 53751–53762. [Google Scholar]
- Dragonieri, S.; Quaranta, V.N.; Carratu, P.; Ranieri, T.; Resta, O. Influence of age and gender on the profile of exhaled volatile organic compounds analyzed by an electronic nose. J. Bras. de Pneumol. 2016, 42, 143–145. [Google Scholar] [CrossRef] [Green Version]
- Blanchet, L.; Smolinska, A.; Baranska, A.; Tigchelaar, E.; Swertz, M.; Zhernakova, A.; Dallinga, J.W.; Wijmenga, C.; Van Schooten, F.J. Factors that influence the volatile organic compound content in human breath. J. Breath Res. 2017, 11, 016013. [Google Scholar] [CrossRef]
- Capone, S.; Tufariello, M.; Forleo, A.; Longo, V.; Giampetruzzi, L.; Radogna, A.V.; Casino, F.; Siciliano, P. Chromatographic analysis of VOC patterns in exhaled breath from smokers and nonsmokers. Biomed. Chromatogr. 2018, 32. [Google Scholar] [CrossRef]
- LeBouf, R.F.; Virji, M.A.; Saito, R.; Henneberger, P.K.; Simcox, N.; Stefaniak, A.B. Exposure to volatile organic compounds in healthcare settings. Occup. Environ. Med. 2014, 71, 642–650. [Google Scholar] [CrossRef]
- Bessoneau, V.; Mosqueron, L.; Berrubé, A.; Mukensturm, G.; Buffet-Bataillon, S.; Gangneux, J.-P.; Thomas, O. VOC contamination in hospital from stationary sampling of a large panel of compounds, in view of healthcare workers and patients exposure assessment. PLoS ONE 2013, 8, e55535. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Malignant Pleural Mesothelioma Patients (MPM) |
|---|---|
| Exposure | Asbestos exposure |
| Comparison | MPM patients versus Asbestos exposed asymptomatic subjects (AEx) Subjects with benign asbestos related diseases (ARD) Healthy controls (HC) |
| Outcome | Exhaled breath profiles in MPM compared with that of (AEx, ARD, HC) |
| Study | Selection (/4) | Comparability (/2) | Exposure (/3) | Overall Score (/9) |
|---|---|---|---|---|
| Gennaro et al. (2010) [69] | 3 | 1 | 1 | 5 |
| Dragonieri et al. (2011) [70] | 3 | 1 | 1 | 5 |
| Chapman et al. (2012) [71] | 4 | 1 | 1 | 6 |
| Lamote et al. (2016) [72] | 3 | 1 | 1 | 5 |
| Lamote et al. (2017) [73] | 3 | 1 | 1 | 5 |
| Lamote et al. (2017) [74] | 3 | 0 | 1 | 4 |
| Study | Study Type | Population (n, Age) | Breath Collection Method | Alveolar/Total Breath | Adjustment for Ambient Air and Collector |
|---|---|---|---|---|---|
| Gennaro (2010) [69] | Cross-sectional, case-control | MPM (13, 60.9 ± 12.2 y) AEx (13, 67.2 ± 9.8 y) HC (13, 52.2 ± 16.2 y) | Tidal breathing (5 min) followed by VC maneuver Tedlar bag | Total breath | Inspiratory VOC filter, Background VOC concentration in a clean Tedlar bag |
| Dragonieri (2011) [70] | Cross-sectional, case-control | MPM (13, 61 ± 12 y) AEx (13, 67 ± 10 y) HC (13, 52 ± 16 y) | Tidal breathing (5 min) followed by VC maneuver10 L Tedlar bag | Total breath | Inspiratory VOC filter, Background VOC concentration in a clean Tedlar bag |
| Chapman (2012) [71] | Multicenter, cross-sectional, case-control | MPM (20, 69 ± 10 y) Asbestosis (5, 70 ± 10.5 y) BLD (13, 70.9 ± 8.2 y) HC (42, 66.5 ± 14 y) | Tidal breathing (5 min) followed by VC maneuver 2 L gas impermeable bag | Total breath | - |
| Lamote (2016) [72] | Multicenter, cross-sectional, case-control | MPM (23, 66(59–73) y) AEx (22,56(55–57) y) HC (21,56(40–58) y) | Tidal breathing (3 min) | Alveolar breath | 10 mL of ambient air sampled as background, alveolar gradients of VOCs were calculated |
| Lamote (2017) [73] | Multicenter, cross-sectional, case-control | MPM (14, 69(65–73) y) AEx (19,50(49–53) y) ARDs (15, 60(58–63) y) HC (16,56(52–59) y) | Tidal breathing (5 min) followed by VC maneuver 10 L Tedlar bag | Total breath | VOC filter Before sampling; Tenax tubes were being flushed with helium |
| Lamote (2017) [74] | Multicenter, cross-sectional, case-control | MPM (52, 67(62–72) y) AEx (59, 53(50–55) y) ARD (41, 58(55–62) y) BLD (70, 58(40–68) y) HC (52, 51(34–56) y) | Tidal breathing (3 min) | Alveolar breath | Disposable mouthpieces and filters Alveolar gradients of VOCs were calculated |
| Study | Breath Profile Detection Method | Pre-Treatment | Statistics | Results |
|---|---|---|---|---|
| Gennaro (2010) [69] | GC–MS | Adsorbtion on thermal desorption (TD) sorbent cartridge | Shapiro-Wilk tests, ANOVA, PCA, DFA, CP-ANN | Cyclohexane able to discriminate MPM from HC and AEx Cyclopentane able to discriminate AEx from MPM and HC |
| Dragonieri (2011) [70] | E-nose | - | PCA, CDA | (1) MPM vs HC Accuracy = 0.84; Cut-off probability of MPM; diagnosis = 0.31; Sensitivity = 0.92; Specificity = 0.69; AUC(ROC) = 0.893 (2) MPM vs AEx Accuracy = 0.80; Cut-off probability of MPM; diagnosis = 0.33; Sensitivity = 0.92; Specificity = 0.85; AUC(ROC) = 0.91 |
| Chapman (2012) [71] | E-nose | - | PCA, CDA, M-distance | (1) MPM vs HC Accuracy = 0.95; Sensitivity = 0.90; Specificity = 0.91 (2) MPM vs ARD Sensitivity = 0.90; Specificity = 0.83 (3) MPM vs ARD vs HC Sensitivity = 0.90; Specificity = 0.83 |
| Lamote (2016) [72] | MCC–IMS | - | Chi-square/ Fisher’s exact, Kolmogorov-Smirnov, T-test/ANOVA, Wilcoxon-Mann-Whitney/ Kruskal-Wallis, Logistic regression using the least absolute shrinkage and selection operator (lasso) | (1) MPM vs HC Accuracy = 0.82; Sensitivity = 0.96; Specificity = 0.67; AUC(ROC) = 0.74; Selected VOCs = P50, P84 (2) MPM vs AEx Accuracy = 0.87; Sensitivity = 0.87; Specificity = 0.86, AUC(ROC) = 0.86; Selected VOCs = P3, P5, P30, P50, P54, P71 (3) AEx vs HC Accuracy = 0.91; Sensitivity = 0.95; Specificity = 0.86; AUC(ROC) = 0.94; Selected VOCs = P5, P8, P13, P25 |
| Lamote (2017) [73] | GC–MS, E-nose | Adsorbtion onto Tenax GR sorbent tubes, Thermal desorption (TD) | Pearson’s Chi-square, Shapiro-Wilk, Lasso regression (applied to GC–MS data), PCA (applied to e-nose data) | GC–MS (1) MPM vs HC Accuracy = 0.71; Sensitivity = 0.64; Specificity = 0.79; AUC(ROC) = 0.77 (2) MPM vs AEx + ARD Accuracy = 0.94; Sensitivity = 1.0; Specificity = 0.91; AUC(ROC) = 0.94 (3) ARD vs AEx Accuracy = 0.5; Sensitivity = 0.60; Specificity = 0.42; AUC(ROC) = 0.36 Selected VOCs: diethyl ether, limonene, cyclohexane, nonanal, VOC IK 1287, isothiocyanatocyclohexane ENOSE (1) MPM vs HC Accuracy = 0.65; Sensitivity = 0.66; Specificity = 0.63; AUC(ROC) = 0.66 (2) MPM vs AEx + ARD Accuracy = 0.74; Sensitivity = 0.81; Specificity = 0.55; AUC(ROC) = 0.74 (3) ARD vs AEx Accuracy = 0.52; Sensitivity = 0.58; Specificity = 0.46; AUC(ROC) = 0.55 |
| Lamote (2017) [74] | MCC–IMS | - | Fisher’s exact, Kolmogorov-Smirnov, ANOVA, Kruskal-Wallis | (1) MPM vs HC Accuracy = 0.65; Sensitivity = 0.89; Specificity = 0.43; AUC(ROC) = 0.61 (2) MPM vs AEx + ARD Accuracy = 0.85; Sensitivity = 0.94; Specificity = 0.80; AUC(ROC) = 0.89 (3) MPM vs LC Accuracy = 0.72; Sensitivity = 0.73; Specificity = 0.71; AUC(ROC) = 0.77 (4) MPM vs BLD Accuracy = 0.80; Sensitivity = 0.71; Specificity = 0.87; AUC(ROC) = 0.83 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Töreyin, Z.N.; Ghosh, M.; Göksel, Ö.; Göksel, T.; Godderis, L. Exhaled Breath Analysis in Diagnosis of Malignant Pleural Mesothelioma: Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 1110. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031110
Töreyin ZN, Ghosh M, Göksel Ö, Göksel T, Godderis L. Exhaled Breath Analysis in Diagnosis of Malignant Pleural Mesothelioma: Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(3):1110. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031110
Chicago/Turabian StyleTöreyin, Zehra Nur, Manosij Ghosh, Özlem Göksel, Tuncay Göksel, and Lode Godderis. 2020. "Exhaled Breath Analysis in Diagnosis of Malignant Pleural Mesothelioma: Systematic Review" International Journal of Environmental Research and Public Health 17, no. 3: 1110. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031110