Examining Users’ Adoption of Precision Medicine: The Moderating Role of Medical Technical Knowledge


Abstract
:1. Introduction
2. Literature Review
2.1. User Acceptance and Adoption of Technology
2.2. Health Belief Theory
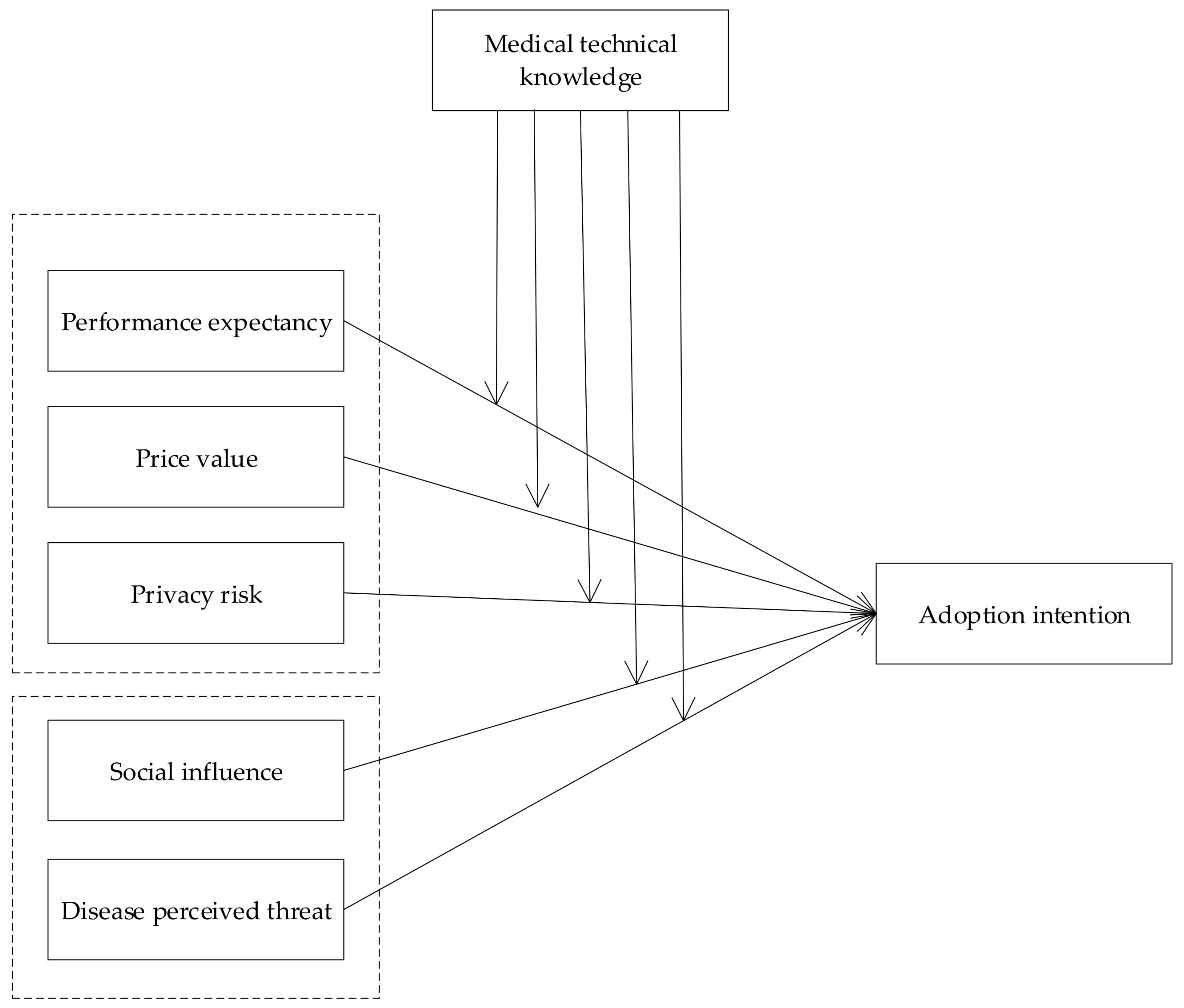
3. Theoretical Framework and Hypotheses Development
3.1. Technical Factors and PM Adoption Intention
3.2. External Stimuli and PM Adoption Intention
3.3. Moderating Effect of Medical Technical Knowledge
4. Research Methodology
4.1. Research Design
4.2. Measurement
5. Data Analysis and Results
5.1. Measurement Model
5.2. Correlation Analysis
5.3. Results
6. General Discussion
6.1. Principal Results
6.2. Implications
6.3. Limitations and Further Research
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Collins, F.S.; Varmus, H. A new initiative on precision medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hult, K.J. Measuring the Potential Health Impact of Personalized Medicine: Evidence from MS Treatments; National Bureau of Economic Research: Cambridge, MA, USA, 2017. [Google Scholar]
- Graner, M.; Tikkanen, E.; Rimpilä, O.; Tikkanen, H.; Ripatti, S.; Lokki, M.-L.; Nieminen, M.S.; Taskinen, M.-R.; Sinisalo, J. Diagnostic efficacy of myeloperoxidase to identify acute coronary syndrome in subjects with chest pain. Ann. Med. 2013, 45, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Zhao, W.; Yang, X.; Wang, Z.; Hao, M. miR-375 affects the proliferation, invasion, and apoptosis of HPV16-positive human cervical cancer cells by targeting IGF-1R. Int. J. Gynecol. Cancer 2016, 26, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Luo, M.; Nie, R.; Zhang, Y. Technical attributes, health attribute, consumer attributes and their roles in adoption intention of healthcare wearable technology. Int. J. Med Inform. 2017, 108, 97–109. [Google Scholar] [CrossRef]
- Kichko, K.; Marschall, P.; Flessa, S. Personalized medicine in the US and Germany: Awareness, acceptance, use and preconditions for the wide implementation into the medical standard. J. Pers. Med. 2016, 6, 15. [Google Scholar] [CrossRef]
- Dwivedi, Y.K.; Shareef, M.A.; Simintiras, A.C.; Lal, B.; Weerakkody, V. A generalised adoption model for services: A cross-country comparison of mobile health (m-health). Gov. Inf. Q. 2016, 33, 174–187. [Google Scholar] [CrossRef] [Green Version]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inform. 2017, 101, 75–84. [Google Scholar] [CrossRef]
- Nisha, N.; Iqbal, M.; Rifat, A. The Changing Paradigm of Health and Mobile Phones: An Innovation in the Health Care System. J. Glob. Inf. Manag. JGIM 2019, 27, 19–46. [Google Scholar] [CrossRef]
- De Veer, A.J.E.; Peeters, J.M.; Brabers, A.E.M.; Schellevis, F.G.; Rademakers, J.J.D.J.M.; Francke, A.L. Determinants of the intention to use e-Health by community dwelling older people. BMC Health Serv. Res. 2015, 15, 103. [Google Scholar] [CrossRef] [Green Version]
- Boontarig, W.; Chutimaskul, W.; Chongsuphajaisiddhi, V.; Papasratorn, B. Factors influencing the Thai elderly intention to use smartphone for e-Health services. In Proceedings of the 2012 IEEE Symposium on Humanities, Science and Engineering Research, Kuala Lumpur, Malaysia, 24–27 June 2012; pp. 479–483. [Google Scholar]
- Moon, Y.-J.; Hwang, Y.-H. A study of effects of UTAUT-based factors on acceptance of smart health care services. In Advanced Multimedia and Ubiquitous Engineering; Springer: Berlin/Heidelberg, Germany, 2016; pp. 317–324. [Google Scholar]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Rese, A.; Baier, D.; Geyer-Schulz, A.; Schreiber, S. How augmented reality apps are accepted by consumers: A comparative analysis using scales and opinions. Technol. Forecast. Soc. Chang. 2017, 124, 306–319. [Google Scholar] [CrossRef]
- San-Martín, S.; López-Catalán, B.; Ramón-Jerónimo, M.A. Mobile shoppers: Types, drivers, and impediments. J. Organ. Comput. Electron. Commer. 2013, 23, 350–371. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Bala, H. Technology acceptance model 3 and a research agenda on interventions. Decis. Sci. 2008, 39, 273–315. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Thong, J.Y.L.; Xu, X. Consumer acceptance and use of information technology: Extending the unified theory of acceptance and use of technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef] [Green Version]
- Lian, J.-W.; Yen, D.C. Online shopping drivers and barriers for older adults: Age and gender differences. Comput. Hum. Behav. 2014, 37, 133–143. [Google Scholar] [CrossRef]
- Oliveira, T.; Thomas, M.; Espadanal, M. Assessing the determinants of cloud computing adoption: An analysis of the manufacturing and services sectors. Inf. Manag. 2014, 51, 497–510. [Google Scholar] [CrossRef]
- McLean, G.; Osei-Frimpong, K. Hey Alexa… examine the variables influencing the use of artificial intelligent in-home voice assistants. Comput. Hum. Behav. 2019, 99, 28–37. [Google Scholar] [CrossRef]
- Workman, M. New media and the changing face of information technology use: The importance of task pursuit, social influence, and experience. Comput. Hum. Behav. 2014, 31, 111–117. [Google Scholar] [CrossRef]
- Hsieh, H.-L.; Kuo, Y.-M.; Wang, S.-R.; Chuang, B.-K.; Tsai, C.-H. A study of personal health record user’s behavioral model based on the PMT and UTAUT integrative perspective. Int. J. Environ. Res. Public Health 2016, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- Becker, M.H. The health belief model and sick role behavior. Health Educ. Monogr. 1974, 2, 409–419. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social learning theory and the health belief model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Painter, J.E.; Borba, C.P.C.; Hynes, M.; Mays, D.; Glanz, K. The use of theory in health behavior research from 2000 to 2005: A systematic review. Ann. Behav. Med. 2008, 35, 358–362. [Google Scholar] [CrossRef]
- Kim, H.-S.; Ahn, J.; No, J.-K. Applying the Health Belief Model to college students’ health behavior. Nutr. Res. Pract. 2012, 6, 551–558. [Google Scholar] [CrossRef] [Green Version]
- Rollins, L.; Sy, A.; Crowell, N.; Rivers, D.; Miller, A.; Cooper, P.; Teague, D.; Jackson, C.; Henry Akintobi, T.; Ofili, E. Learning and action in community health: Using the health belief model to assess and educate African American Community residents about participation in clinical research. Int. J. Environ. Res. Public Health 2018, 15, 1862. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [Green Version]
- Ahadzadeh, A.S.; Sharif, S.P.; Ong, F.S.; Khong, K.W. Integrating health belief model and technology acceptance model: An investigation of health-related internet use. J. Med Internet Res. 2015, 17, 45. [Google Scholar] [CrossRef]
- Tsai, C.-H. The adoption of a Telehealth system: The integration of extended technology acceptance model and health belief model. J. Med. Imaging Health Inform. 2014, 4, 448–455. [Google Scholar] [CrossRef]
- Ashley, E.A. The precision medicine initiative: A new national effort. JAMA 2015, 313, 2119–2120. [Google Scholar] [CrossRef]
- Jameson, J.L.; Longo, D.L. Precision medicine—Personalized, problematic, and promising. Obstet. Gynecol. Surv. 2015, 70, 612–614. [Google Scholar] [CrossRef]
- Macedo, I.M. Predicting the acceptance and use of information and communication technology by older adults: An empirical examination of the revised UTAUT2. Comput. Hum. Behav. 2017, 75, 935–948. [Google Scholar] [CrossRef]
- Okazaki, S.; Blas, S.S.; Castañeda, J.A. Physicians’adoption of mobile health monitoring systems in spain: Competing models and impact of prior experience. J. Electron. Commer. Res. 2015, 16, 194. [Google Scholar]
- Chang, T.-Z.; Wildt, A.R. Price, product information, and purchase intention: An empirical study. J. Acad. Mark. Sci. 1994, 22, 16–27. [Google Scholar] [CrossRef]
- Cropanzano, R.; Anthony, E.L.; Daniels, S.R.; Hall, A.V. Social exchange theory: A critical review with theoretical remedies. Acad. Manag. Ann. 2017, 11, 479–516. [Google Scholar] [CrossRef] [Green Version]
- Bauer, R.A. Consumer Behavior as Risk Taking. In Dynamic Marketing for a Changing World; Hancock, R.S., Ed.; American Marketing Association: Chicago, IL, USA, 1960; pp. 384–398. [Google Scholar]
- Martins, C.; Oliveira, T.; Popovič, A. Understanding the Internet banking adoption: A unified theory of acceptance and use of technology and perceived risk application. Int. J. Inf. Manag. 2014, 34, 1–13. [Google Scholar] [CrossRef]
- Akturan, U.; Tezcan, N. Mobile banking adoption of the youth market: Perceptions and intentions. Mark. Intell. Plan. 2012, 30, 444–459. [Google Scholar] [CrossRef]
- Milne, G.R.; Culnan, M.J. Strategies for reducing online privacy risks: Why consumers read (or don’t read) online privacy notices. J. Interact. Mark. 2004, 18, 15–29. [Google Scholar] [CrossRef]
- Frizzo-Barker, J.; Chow-White, P.A.; Charters, A.; Ha, D. Genomic big data and privacy: Challenges and opportunities for precision medicine. Comput. Supported Coop. Work CSCW 2016, 25, 115–136. [Google Scholar] [CrossRef]
- Wei, S. Charles Ornstein. Over 1100 Health Data Breaches, but Few Fines. Available online: https://projects.propublica.org/graphics/healthcare-data-breaches (accessed on 7 March 2015).
- Li, H.; Wu, J.; Gao, Y.; Shi, Y. Examining individuals’ adoption of healthcare wearable devices: An empirical study from privacy calculus perspective. Int. J. Med Inform. 2016, 88, 8–17. [Google Scholar] [CrossRef]
- Wang, X.; White, L.; Chen, X.; Gao, Y.; Li, H.; Luo, Y. An empirical study of wearable technology acceptance in healthcare. Ind. Manag. Data Syst. 2015, 115, 1704–1723. [Google Scholar]
- Cheung, M.L.; Chau, K.Y.; Lam, M.H.S.; Tse, G.; Ho, K.Y.; Flint, S.W.; Broom, D.R.; Tso, E.K.H.; Lee, K.Y. Examining Consumers’ Adoption of Wearable Healthcare Technology: The Role of Health Attributes. Int. J. Environ. Res. Public Health 2019, 16, 2257. [Google Scholar] [CrossRef] [Green Version]
- Hossain, N.; Yokota, F.; Sultana, N.; Ahmed, A. Factors influencing rural end-users’ acceptance of e-health in developing countries: A study on portable health clinic in bangladesh. Telemed. E-Health 2019, 25, 221–229. [Google Scholar] [CrossRef]
- Cimperman, M.; Brenčič, M.M.; Trkman, P. Analyzing older users’ home telehealth services acceptance behavior—Applying an Extended UTAUT model. Int. J. Med Inform. 2016, 90, 22–31. [Google Scholar] [CrossRef]
- Mazur, D.J.; Hickam, D.H.; Mazur, M.D.; Mazur, M.D. The role of doctor’s opinion in shared decision making: What does shared decision making really mean when considering invasive medical procedures? Health Expect. 2005, 8, 97–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.W.; Lessig, V.P. Students and housewives: Differences in susceptibility to reference group influence. J. Consum. Res. 1977, 4, 102–110. [Google Scholar] [CrossRef]
- Deutsch, M.; Gerard, H.B. A study of normative and informational social influences upon individual judgment. J. Abnorm. Soc. Psychol. 1955, 51, 629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaussabel, D.; Pulendran, B. A vision and a prescription for big data-enabled medicine. Nat. Immunol. 2015, 16, 435. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA A Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef]
- Mitchell, A.A.; Dacin, P.A. The assessment of alternative measures of consumer expertise. J. Consum. Res. 1996, 23, 219–239. [Google Scholar] [CrossRef]
- Khatwani, G.; Srivastava, P.R. Employing group decision support system for the selection of internet information search channels for consumers. Int. J. Strateg. Decis. Sci. IJSDS 2015, 6, 72–93. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.K.; Lee, W.-N. Country-of-origin effects on consumer product evaluation and purchase intention: The role of objective versus subjective knowledge. J. Int. Consum. Mark. 2009, 21, 137–151. [Google Scholar] [CrossRef]
- Park, C.W.; Mothersbaugh, D.L.; Feick, L. Consumer knowledge assessment. J. Consum. Res. 1994, 21, 71–82. [Google Scholar] [CrossRef]
- Brucks, M. The effects of product class knowledge on information search behavior. J. Consum. Res. 1985, 12, 1–16. [Google Scholar] [CrossRef]
- Philipson, T.J. The Economic Value and Pricing of Personalized Medicine; National Bureau of Economic Research: Cambridge, MA, USA, 2017; pp. 1–18. [Google Scholar]
- Huang, H.-T.; Kuo, Y.-M.; Wang, S.-R.; Wang, C.-F.; Tsai, C.-H. Structural factors affecting health examination behavioral intention. Int. J. Environ. Res. Public Health 2016, 13, 395. [Google Scholar] [CrossRef] [Green Version]
- Roscoe, J.T. Fundamental Research Statistics for the Behavioral Sciences; Holt Rinehart & Winston: New York, NY, USA, 1975. [Google Scholar]
- Duarte, P.; Pinho, J.C. A mixed methods UTAUT2-based approach to assess mobile health adoption. J. Bus. Res. 2019, 102, 140–150. [Google Scholar] [CrossRef]
- Ghosh, A.K.; Swaminatha, T.M. Software security and privacy risks in mobile e-commerce. Commun. ACM 2001, 44, 51–57. [Google Scholar] [CrossRef]
- Kahsay, Z.H.; Hiluf, M.K.; Shamie, R.; Tadesse, Y.; Bazzano, A.N. Pregnant Women’s Intentions to Deliver at a Health Facility in the Pastoralist Communities of Afar, Ethiopia: An Application of the Health Belief Model. Int. J. Environ. Res. Public Health 2019, 16, 888. [Google Scholar] [CrossRef] [Green Version]
- Restivo, V.; Costantino, C.; Marras, A.; Napoli, G.; Scelfo, S.; Scuderi, T.; Casuccio, A.; Cernigliaro, A.; Giusti, A.; Spila Alegiani, S. Pap testing in a high-income country with suboptimal compliance levels: A survey on acceptance factors among Sicilian women. Int. J. Environ. Res. Public Health 2018, 15, 1804. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Daugherty, T.; Biocca, F. Impact of 3-D advertising on product knowledge, brand attitude, and purchase intention: The mediating role of presence. J. Advert. 2002, 31, 43–57. [Google Scholar] [CrossRef]
- Chou, L.F.; Chu, C.C.; Yeh, H.C.; Chen, J. Work stress and employee well-being: The critical role of Zhong-Yong. Asian J. Soc. Psychol. 2014, 17, 115–127. [Google Scholar] [CrossRef]
- Wu, Y.; Lau, T.; Atkin, D.J.; Lin, C.A. A comparative study of online privacy regulations in the US and China. Telecommun. Policy 2011, 35, 603–616. [Google Scholar] [CrossRef]
- Lin, W.; Liu, G.G.; Chen, G. The urban resident basic medical insurance: A landmark reform towards universal coverage in China. Health Econ. 2009, 18, S83–S96. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Category | Factor | Consumer Quotes |
|---|---|---|
| Technical factors | Performance expectancy | For me, the main question is whether PM has a good effect and whether it can cure the disease. (interviewee 5) It is mainly to see whether PM has better therapeutic effect than traditional medicine. (Interviewee 7) Whether PM has a better therapeutic effect and whether it can better treat diseases is my most concern. (Interviewee 14) … |
| Price value | The cost of PM will affect whether I use it or not. (Interviewee 10) I focus on the price of PM. (Interviewee 19) Whether precision medicine is included in Chinese Urban Resident Basic Medical Insurance (URBMI) is the factor that affects whether I accept PM, because the general price of PM is relatively high. (Interviewee 25) … | |
| Privacy risk | I don’t use PM. I’m afraid my privacy will be compromised. (Interviewee 4) I’m not going to adopt PM. As in the novel, the relationship between genetic information and wealth, status, health, and even life, the adoption of PM may lead to higher insurance costs, borrowing risks, targeted marketing, and genetic discrimination. (Interviewee 6) There are mainly the following points: 1. How to protect the privacy of patients, and will the medical results cause discrimination by insurance companies or employers? … (Interviewee 17) … | |
| External stimuli | Social influence | The recommendations of doctors and relatives are also more critical. My father has advanced lung cancer. Now doctors recommend chemotherapy or genetic testing to take targeted medicines. With my support, my father chose genetic testing to take targeted medicines. (Interviewee 8) I will only consider using PM when I see real cases of successful use of PM around me. (Interviewee 9) When choosing between traditional treatment and PM, I tend to consider my family’s suggestions. (Interviewee 16) … |
| Perceived threat of disease | The worry about diseases is the main reason why I choose PM. Because my family has a genetic history, I want to know the probability of the disease in the next generation through the test. (Interviewee 2) For general diseases, I will definitely not choose PM. When I am faced with cancer, I will choose PM. At this time, I will not consider the price. (Interviewee 3) When this disease seriously threatens my life, I will choose PM. (Interviewee 11) … |
| Demographic Variable | Number | Percentage (%) | |
|---|---|---|---|
| Gender | Male | 194 | 46.747 |
| Female | 221 | 53.253 | |
| Age | 31 or less | 26 | 6.265 |
| 31–40 | 41 | 9.880 | |
| 41–50 | 54 | 13.012 | |
| 51–60 | 164 | 39.518 | |
| 61–70 | 121 | 29.157 | |
| 71 or more | 9 | 2.169 | |
| Occupation | Corporate white collar | 61 | 14.699 |
| Ordinary worker | 275 | 66.265 | |
| Civil servant | 30 | 7.229 | |
| Teacher | 33 | 7.952 | |
| Other | 16 | 3.855 | |
| Monthly income | 0–3000 yuan | 116 | 27.951 |
| 3000–5000 yuan | 147 | 35.422 | |
| 5000–8000 yuan | 59 | 14.217 | |
| 8000–10,000 yuan | 69 | 16.627 | |
| Over 10,000 yuan | 24 | 5.783 | |
| Variable | Measurement Index | Factor Loading | Cronbach α | CR | AVE |
|---|---|---|---|---|---|
| Performance expectancy (PE) | PE1 | 0.874 | 0.923 | 0.938 | 0.791 |
| PE2 | 0.902 | ||||
| PE3 | 0.891 | ||||
| PE4 | 0.891 | ||||
| Price value (PV) | PV1 | 0.880 | 0.877 | 0.920 | 0.793 |
| PV2 | 0.907 | ||||
| PV3 | 0.885 | ||||
| Privacy risk (PR) | PR1 | 0.891 | 0.900 | 0.931 | 0.818 |
| PR2 | 0.930 | ||||
| PR3 | 0.891 | ||||
| Social influence (SI) | SI1 | 0.879 | 0.921 | 0.934 | 0.780 |
| SI2 | 0.877 | ||||
| SI3 | 0.896 | ||||
| SI4 | 0.880 | ||||
| Perceived threat (PT) | PT1 | 0.884 | 0.896 | 0.915 | 0.782 |
| PT2 | 0.905 | ||||
| PT3 | 0.864 | ||||
| Medical technical knowledge (MTK) | MTK1 | 0.908 | 0.900 | 0.937 | 0.831 |
| MTK2 | 0.929 | ||||
| MTK3 | 0.898 | ||||
| Adoption intention (AI) | AI1 | 0.741 | 0.909 | 0.848 | 0.585 |
| AI2 | 0.630 | ||||
| AI3 | 0.789 | ||||
| AI4 | 0.878 |
| Title | Mean | SD | PE | PV | PR | SI | PT | MTK | AI |
|---|---|---|---|---|---|---|---|---|---|
| PE | 4.545 | 1.654 | 1 | ||||||
| PV | 4.678 | 1.611 | –0.078 | 1 | |||||
| PR | 4.551 | 1.700 | 0.009 | 0.007 | 1 | ||||
| SI | 4.682 | 1.605 | –0.034 | –0.051 | 0.085 | 1 | |||
| PT | 4.591 | 1.684 | –0.079 | 0.107 * | 0.077 | 0.039 | 1 | ||
| MTK | 4.347 | 1.759 | –0.023 | 0.055 | 0.004 | –0.017 | –0.058 | 1 | |
| AI | 4.658 | 1.527 | 0.336 ** | 0.142 ** | –0.216 ** | 0.407 ** | 0.425 ** | –0.036 | 1 |
| Variable Types | Model 1 | Model 2 | Model 3 | Model 4 | |
|---|---|---|---|---|---|
| Control variables | Gender | 0.012 | –0.006 | –0.006 | –0.011 |
| Age | 0.042 | 0.016 | 0.016 | 0.006 | |
| Occupation | –0.025 | –0.037 | –0.038 | –0.022 | |
| Monthly income | 0.021 | 0.011 | 0.011 | –0.022 | |
| Independent variables | Performance expectancy | 0.397 *** | 0.397 *** | 0.427 *** | |
| Price value | 0.148 *** | 0.148 *** | 0.161 *** | ||
| Privacy risk | –0.295 *** | –0.295 *** | –0.292 *** | ||
| Social influence | 0.436 *** | 0.436 *** | 0.431 *** | ||
| Perceived threat | 0.448 *** | 0.448*** | 0.468 *** | ||
| Moderator variable | Medical technical knowledge | –0.002 | –0.040 | ||
| Interaction items | Performance expectancy * Medical technical knowledge | 0.088 ** | |||
| Price value * Medical technical knowledge | 0.148 *** | ||||
| Privacy risk * Medical technical knowledge | 0.163 *** | ||||
| Social influence * Medical technical knowledge | 0.084 ** | ||||
| Perceived threat * Medical technical knowledge | 0.263 *** | ||||
| Statistics | R2 | 0.003 | 0.588 | 0.588 | 0.730 |
| Adjusted R2 | –0.006 | 0.579 | 0.578 | 0.720 | |
| F | 0.333 | 64.196 *** | 57.635 *** | 72.021 *** | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Liu, Y.; Liu, H. Examining Users’ Adoption of Precision Medicine: The Moderating Role of Medical Technical Knowledge. Int. J. Environ. Res. Public Health 2020, 17, 1113. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031113
Wang X, Liu Y, Liu H. Examining Users’ Adoption of Precision Medicine: The Moderating Role of Medical Technical Knowledge. International Journal of Environmental Research and Public Health. 2020; 17(3):1113. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031113
Chicago/Turabian StyleWang, Xingyuan, Yun Liu, and Hongchen Liu. 2020. "Examining Users’ Adoption of Precision Medicine: The Moderating Role of Medical Technical Knowledge" International Journal of Environmental Research and Public Health 17, no. 3: 1113. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17031113