Development of a Tool to Increase Physical Activity among People at Risk for Diabetes in Low-Resourced Communities in Cape Town

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Step 1: A Descriptive Analysis of Existing SA-DPP Pilot-Phase Baseline Screening Data Was Done. The Main Objective Was to Identify the Socio-Demographic Profile as Well as Health-Risk Profiles of People at Risk of Developing Diabetes
2.2. Step 2: Focus Group Discussions (FGDs) Were Conducted to Identify the Barriers and Facilitators to PA That Participants Experienced
2.3. Step 3: Comprised a Review of the Literature
2.4. Step 4: Comprised Expert Consultations (PA Experts with Experience in Working with Low-Income/Resourced Communities) and Engagement with the SA-DPP Project Team. Discussions Focused on Appropriate Tools, Exercises and Appropriate Intervention/Educational Content
3. Results
3.1. Socio-Demographic and Health Profile of the Study Population
3.2. Self-Reported Physical Activity Practices
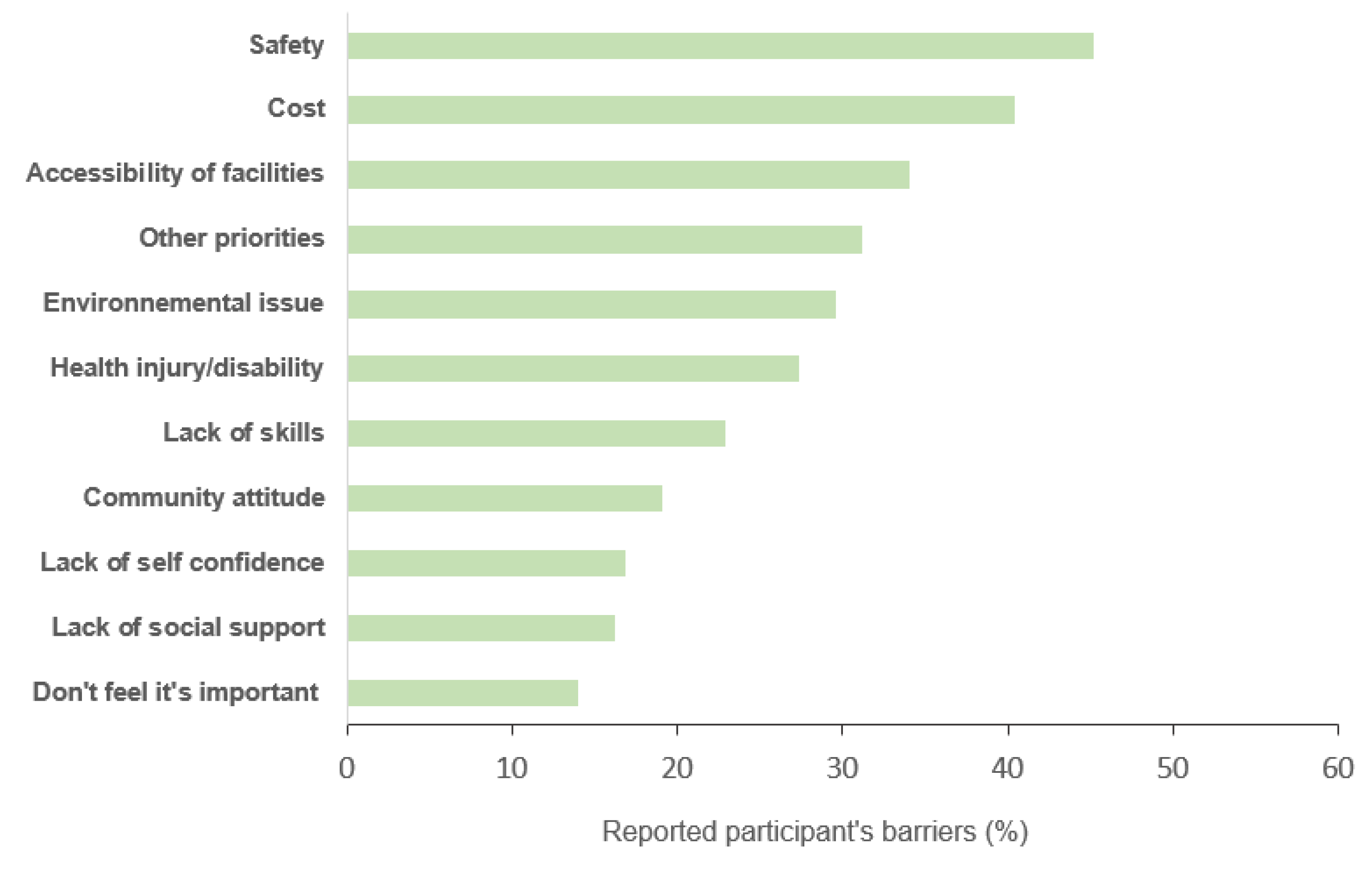
3.3. Self-Reported PA Aptitude and Barriers
3.4. Perceived Neighbourhood and Environment (NEWS Africa Questionnaire)
3.5. Qualitative (FGD) Data
3.5.1. Types of Activities Engaged in by Participants
My activity is cleaning the house. Up and down the stairs with the washing because I live in a flat. And walking to Athlone when I go shopping, but I come back with a taxi because of the stuff.[Area D, participant 7]
Monday to Friday I walk to school to sell snacks to the school children every day so, I do walking.[Area B, participant 6]
For us it is more like walking because we don’t go to the gym and pick up weights and stuff. We just do the walking in the morning or in the afternoon or wherever we go. We don’t actually take a car or a bus, we try to actually walk to try and get to that place.[Area D, participant 2]
My stomach used to be big and I do sit-ups so I see that my stomach becoming flatter.[Area B, participant 1]
3.5.2. Facilitators to PA
PA impacts your health. It gives good results meaning that when you do exercise you don’t get sick. To do exercise it means taking the stairs, try to do running or walking and jumping like you see people.[Area H, participant 4]
When you start seeing results with diet and exercise you will get confidence to exercise. I have a large tummy but if I exercise I know it will become flatter. So, if you exercise your weight will go down and you can start wearing the clothes sitting in the wardrobe because you gained weight.[Area H, participant 4]
I and other people decided as a group to walk twice a day. We walk early in the morning and we also walk in the afternoon. […] We see changes in the body, some of us in our walking group have lost weight and we can move faster and are more flexible.[Area B, participant 4]
No, but I am a neighbourhood watch with participant no. 3. We do exercise because we walk around the community all the time, we are always running after these bad guys stealing people’s cell phones.[Area H, participant 7]
I am very fit. I wake up at 4 o’clock in the morning to do my work as a neighbourhood watch.[Area H, participant 3]
“My family would be supportive. Everybody in my household likes exercising and going to the gym. The kids they do their chores and go to the gym afterwards.”[Area B, participant 3]
“They will support me.”[Area G, participant 7]
No, I think they will join, they will enjoy it and we do it together, yes.[Area D, participant 5]
My family and friends would be supportive because even my kids gym.[Area G, participant 3]
Like me and Carol, we like to do exercise and my children love it because I do dancing, I do things, they think I am the grandest granny.[Area G, participant 1]
3.5.3. Barriers to PA
There are no barriers we need to be disciplined, we are just lazy to exercise we sit the whole day.[Area H, participant 4]
“Yes, there is a park. In the park there is three or four stuff to help you to do some exercise, it is there and the community is safe to do it in. You can walk in your community, no one will disturb you.”[Area D, participant 2]
I don’t have any barriers because I work in the hall where people come to exercise so I can exercise at the community hall because the facilities are there and I can also work in my garden.[Area B, participant 1]
There are no places to exercise, no parks.[Area B, participant 2]
Even though there is a park close to my community to exercise it is not safe. There are robbers waiting to rob you when you are done.[Area B, participant 3]
3.5.4. Tools and Resources Currently Used to Support PA
TV is a tool I use. At 6 o’clock every morning there is a programme with a lady and two guys exercising. Me [sic.] and my daughter watch and follow the exercise with them. I exercise every day using the TV programme before going to work.[Area H, participant 7]
“Seeing exercise on TV also motivates me because when you are at home you can copy what you see if you can’t join the community groups.”[Area H, participant 4]
I need ideas on the types of exercise. At the old age home, they have a book in the library that shows different exercises. It would be nice if someone can do the exercises practically and teach me more exercise. [...] I want to do more exercising. I want to learn about different types of exercises I can do to my body [...]. If you can give us some pamphlet or booklet in English or isiXhosa to assist us to exercise at home.[Area H, participant 5]
3.5.5. Considerations from the Literature for Inclusions in a PA Tool
4. Discussion
4.1. Compiling the PA Tool
4.2. Overcoming the Barriers to PA
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B
Appendix C
References
- International Diabetes Federation. IDF Diabetes Atlas Eighth Edition; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Erasmus, R.T.; Soita, D.J.; Hassan, M.S.; Blanco-Blanco, E.; Vergotine, Z.; Kengne, A.P.; Matsha, T.E. High prevalence of diabetes mellitus and metabolic syndrome in a South African coloured population: Baseline data of a study in Bellville, Cape Town. S. Afr. Med. J. 2012, 102, 841–844. [Google Scholar] [CrossRef] [Green Version]
- Peer, N.; Steyn, K.; Lombard, C.; Lambert, E.V.; Vythilingum, B.; Levitt, N.S. Rising Diabetes Prevalence among Urban-Dwelling Black South Africans. PLoS ONE 2012, 7, e43336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruger, H.S.; Puoane, T.; Senekal, M.; Van der Merwe, M.T. Obesity in South Africa: Challenges for government and health professionals. Public Health Nutr. 2005, 8, 491–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jefferis, B.J.; Whincup, P.H.; Lennon, L.; Wannamethee, S.G. Longitudinal Associations Between Changes in Physical Activity and Onset of Type 2 Diabetes in Older British Men. Diabetes Care. 2012, 35, 1876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyle, T.; Keegel, T.; Bull, F.; Heyworth, J.; Fritschi, L. Physical activity and risks of proximal and distal colon cancers: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2012, 104, 1548–1561. [Google Scholar] [CrossRef]
- Sattelmair, J.; Pertman, J.; Ding, E.L.; Kohl, H.W.; Haskell, W.; Lee, I.M. Dose response between physical activity and risk of coronary heart disease: A meta-analysis. Circulation 2011, 124, 789–795. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.D.; Folsom, A.R.; Blair, S.N. Physical activity and stroke risk: A meta-analysis. Stroke 2003, 34, 2475–2481. [Google Scholar] [CrossRef] [Green Version]
- Tanasescu, M.; Leitzmann, M.F.; Rimm, E.B.; Willett, W.C.; Stampfer, M.J.; Hu, F.B. Exercise type and intensity in relation to coronary heart disease in men. JAMA 2002, 288, 1994–2000. [Google Scholar] [CrossRef]
- Lindstrom, J.; Louheranta, A.; Mannelin, M.; Rastas, M.; Salminen, V.; Eriksson, J.; Uusitupa, M.; Tuomilehto, J.; Finnish Diabetes Prevention Study Group. The Finnish Diabetes Prevention Study (DPS): Lifestyle intervention and 3-year results on diet and physical activity. Diabetes Care 2003, 26, 3230–3236. [Google Scholar] [CrossRef] [Green Version]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Absetz, P.; Valve, R.; Oldenburg, B.; Heinonen, H.; Nissinen, A.; Fogelholm, M.; Ilvesmäki, V.; Talja, M.; Uutela, A. Type 2 diabetes prevention in the “real world”: One-year results of the GOAL Implementation Trial. Diabetes Care. 2007, 30, 2465–2470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bromberger, J.T.; Matthews, K.A. A longitudinal study of the effects of pessimism, trait anxiety, and life stress on depressive symptoms in middle-aged women. Psychol. Aging 1996, 11, 207–213. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Physical Activity Questionnaire (GPAQ); World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Booth, M.L.; Bauman, A.; Owen, N.; Gore, C.J. Physical activity preferences, preferred sources of assistance, and perceived barriers to increased activity among physically inactive Australians. Prev. Med. 1997, 26, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Jerusalem, M. Generalized Self-Efficacy scale. In Measures in Health Psychology: A User’s Portfolio Causal and Control Beliefs Windsor; Weinman, J., Johnston, M., Eds.; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Oyeyemi, A.L.; Kasoma, S.S.; Onywera, V.O.; Assah, F.; Adedoyin, R.A.; Conway, T.L.; Moss, S.J.; Ocansey, R.; Kolbe-Alexander, T.L.; Akinroye, K.K.; et al. NEWS for Africa: Adaptation and reliability of a built environment questionnaire for physical activity in seven African countries. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 33. [Google Scholar] [CrossRef] [Green Version]
- Jepson, R.; Harris, F.M.; Bowes, A.; Robertson, R.; Avan, G.; Sheikh, A. Physical activity in South Asians: An in-depth qualitative study to explore motivations and facilitators. PLoS ONE 2012, 7, e45333. [Google Scholar] [CrossRef] [Green Version]
- Miller, S.T.; Marolen, K. Physical activity-related experiences, counseling expectations, personal responsibility, and altruism among urban African American women with type 2 diabetes. Diabetes Educ. 2012, 38, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Pope, C.; Ziebland, S.; Mays, N. Qualitative research in health care. Analysing qualitative data. Br. Med J. 2000, 320, 114–116. [Google Scholar] [CrossRef]
- Babbie, E.R.; Mouton, J. The Practice of Social Research; Oxford University Press: Cape Town, South Africa, 2001. [Google Scholar]
- Zlatkovic, M.; Zlatkovic, S.; Sullivan, T.; Bjornstad, J.; Kiavash, F.S.S. Assessment of effects of street connectivity on traffic performance and sustainability within communities and neighborhoods through traffic simulation. Sustain. Cities Soc. 2019, 46, 101409. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B.; American College of Sports Medicine; et al. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef] [Green Version]
- Irvine, C.; Taylor, N.F. Progressive resistance exercise improves glycaemic control in people with type 2 diabetes mellitus: A systematic review. Aust. J. Physiother. 2009, 55, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Holten, M.K.; Zacho, M.; Gaster, M.; Juel, C.; Wojtaszewski, J.F.; Dela, F. Strength training increases insulin-mediated glucose uptake, GLUT4 content, and insulin signaling in skeletal muscle in patients with type 2 diabetes. Diabetes 2004, 53, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Sigal, R.J.; Kenny, G.P.; Wasserman, D.H.; Castaneda-Sceppa, C.; White, R.D. Physical activity/exercise and type 2 diabetes: A consensus statement from the American Diabetes Association. Diabetes Care 2006, 29, 1433–1438. [Google Scholar] [CrossRef] [Green Version]
- Lesinski, M.; Hortobagyi, T.; Muehlbauer, T.; Gollhofer, A.; Granacher, U. Effects of Balance Training on Balance Performance in Healthy Older Adults: A Systematic Review and Meta-analysis. Sports Med. 2015, 45, 1721–1738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westcott, W.L. Resistance training is medicine: Effects of strength training on health. Curr. Sports Med. Rep. 2012, 11, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Shaw, B.S.; Shaw, I.; Brown, G.A. Resistance exercise is medicine: Strength training in health promotion and rehabilitation. Int. J. Ther. Rehabil. 2015, 22, 385–389. [Google Scholar] [CrossRef]
- Onagbiye, S.O.; Moss, S.J.; Cameron, M. Managing Noncommunicable Diseases in an African Community: Effects, Compliance, and Barriers to Participation in a 4-Week Exercise Intervention. Int. Q. Community Health Educ. 2016, 36, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Mathunjwa, M.L.; Semple, S.J.; du Preez, C. A 10-week aerobic exercise program reduces cardiometabolic disease risk in overweight/obese female African university students. Ethn. Dis. 2013, 23, 143–148. [Google Scholar]
- Jemmott, J.B.; Jemmott, L.S.; Ngwane, Z.; Zhang, J.; Heeren, G.A.; Icard, L.D.; O’Leary, A.; Mtose, X.; Teitelman, A.; Carty, C. Theory-based behavioral intervention increases self-reported physical activity in South African men: A cluster-randomized controlled trial. Prev. Med. 2014, 64, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Roos, R.; Myezwa, H.; Van Aswegen, H. “Not easy at all but I am trying”: Barriers and facilitators to physical activity in a South African cohort of people living with HIV participating in a home-based pedometer walking programme. AIDS Care. 2015, 27, 235–239. [Google Scholar] [CrossRef]
- Chetty, L.; Ramklass, S.S.; McKUNE, A.J. The Effects of a Structured Group Exercise Programme on Functional Fitness of Older Persons Living in Old-Age Homes. Master’s Thesis, University of KwaZulu-Natal, KwaZulu-Natal, South Africa, 2014. [Google Scholar]
- Pillay, J.D.; Van der Ploeg, H.P.; Kolbe-Alexander, T.L.; Proper, K.I.; Van Stralen, M.; Tomaz, S.A.; van Mechelen, W.; Lambert, E.V. The association between daily steps and health, and the mediating role of body composition: A pedometer-based, cross-sectional study in an employed South African population. BMC Public Health 2015, 15, 174. [Google Scholar] [CrossRef] [Green Version]
- Ley, C.; Leach, L.; Barrio, M.R.; Bassett, S. Effects of an exercise programme with people living with HIV: Research in a disadvantaged setting. Afr. J. AIDS Res. AJAR 2014, 13, 313–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, D.W.; Salmon, J.; Healy, G.N.; Shaw, J.E.; Jolley, D.; Zimmet, P.Z.; Owen, N.; On behalf of the AusDiab Steering Committee. Association of television viewing with fasting and 2-h postchallenge plasma glucose levels in adults without diagnosed diabetes. Diabetes Care 2007, 30, 516–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Z.; Scott, C.A.; Mao, C.; Tang, J.; Farmer, A.J. Resistance exercise versus aerobic exercise for type 2 diabetes: A systematic review and meta-analysis. Sports Med. 2014, 44, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Jorge, M.L.; De Oliveira, V.N.; Resende, N.M.; Paraiso, L.F.; Calixto, A.; Diniz, A.L.; Resende, E.S.; Ropelle, E.R.; Carvalheira, J.B.; Espindola, F.S.; et al. The effects of aerobic, resistance, and combined exercise on metabolic control, inflammatory markers, adipocytokines, and muscle insulin signaling in patients with type 2 diabetes mellitus. Metab. Clin. Exp. 2011, 60, 1244–1252. [Google Scholar] [CrossRef] [PubMed]
- Wallberg-Henriksson, H.; Rincon, J.; Zierath, J.R. Exercise in the management of non-insulin-dependent diabetes mellitus. Sports Med. 1998, 25, 25–35. [Google Scholar] [CrossRef]
- Skaal, L.; Pengpid, S. The predictive validity and effects of using the transtheoretical model to increase the physical activity of healthcare workers in a public hospital in South Africa. Transl. Behav. Med. 2012, 2, 384–391. [Google Scholar] [CrossRef] [Green Version]
- Mash, B.; Levitt, N.; Steyn, K.; Zwarenstein, M.; Rollnick, S. Effectiveness of a group diabetes education programme in underserved communities in South Africa: Pragmatic cluster randomized control trial. BMC Fam. Pract. 2012, 13, 126. [Google Scholar] [CrossRef] [Green Version]
- Van der Does, A.M.; Mash, R. Evaluation of the “Take Five School”: An education programme for people with Type 2 Diabetes in the Western Cape, South Africa. Prim. Care Diabetes 2013, 7, 289–295. [Google Scholar] [CrossRef]
- Plow, M.; Bethoux, F.; Mai, K.; Marcus, B. A formative evaluation of customized pamphlets to promote physical activity and symptom self-management in women with multiple sclerosis. Health Educ. Res. 2014, 29, 883–896. [Google Scholar] [CrossRef] [Green Version]
- Patel, D.; Lambert, E.V.; Da Silva, R.; Greyling, M.; Kolbe-Alexander, T.; Noach, A.; Conradie, J.; Nossel, C.; Borresen, J.; Gaziano, T. Participation in fitness-related activities of an incentive-based health promotion program and hospital costs: A retrospective longitudinal study. Am. J. Health Promot. 2011, 25, 341–348. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Component | Measurements Tools/Questions |
|---|---|---|
| Socio-demographic measures | Age, gender, area, community, current marital status, education level, occupation, income | |
| Behavioural measures | Tobacco use | WHO STEPS questionnaire [14] |
| Alcohol use | WHO STEPS questionnaire [14] | |
| Sedentary behaviour | Time spent in front of a screen | |
| Sleep | Time, quality | |
| Psychological measures | Chronic stress | Chronic stress scale [13] |
| Physical activity measures | Physical activity pattern | WHO STEPS questionnaire: global physical activity questionnaire (GPAQ) [14] |
| Barriers to physical activity | Scale adapted from the one designed by Booth et al. [15] | |
| Self-efficacy | Scale adapted from the exercise self-efficacy scale (ESES) designed by Schwarzer and Jerusalem [16] | |
| Medical history | Family history of diabetes | |
| Clinical measures | Waist circumference | Measured between the lower border of the lowest rib and upper border of the iliac crest/pelvic bone to the nearest 0.1 cm. |
| Weight | Weight measurement with minimal clothing on a digital (SECA) scale, recorded to the nearest 0.1 kg | |
| Height | Standing height, minimal clothing, aligning head in a standard anatomical position using a SECA stadiometer | |
| SBP | Electronic M6 COMFORT OMRON device with an integrated cuff | |
| DBP HbA1c | Electronic M6 COMFORT OMRON device with an integrated cuff HbA1c measured using fasting blood and HPLC | |
| Neighbourhood indicators | Stores and facilities, Access to services and places, Roads and walking paths, places for walking/cycling/playing, Surroundings, Safety from crime and traffic, Personal safety, Stranger danger | Neighbourhood Environment Walkability Scale (NEWS) Africa Questionnaire [17] |
| Socio-Demographic Characteristics (N = 316) | ||
|---|---|---|
| N | % | |
| Age, median (25th–75th percentiles) | 53.00 [46.00–59.00] | |
| 25–45 years | 57 | 18.0 |
| 45–65 years | 256 | 81.0 |
| Not Assigned | 3 | 1.0 |
| Gender | ||
| Male | 60 | 19.0 |
| Female | 253 | 80.1 |
| NA | 3 | 0.9 |
| Community | ||
| Black | 172 | 54.4 |
| Mixed-ancestry | 141 | 44.6 |
| Not Assigned | 3 | 1.0 |
| Education | ||
| Never went to school | 2 | 0.6 |
| Primary school (Grades 1–7) | 76 | 24.1 |
| High school (Grades 8–12) | 136 | 43.0 |
| Less than Grade 12 + FET */Certificate/Diploma | 11 | 3.5 |
| Grade 12 and higher (Tertiary/Diploma/Degree) | 86 | 27.2 |
| NA | 5 | 1.6 |
| Occupation | ||
| Employed (full- or part-time/self-employed/ | 92 | 29.1 |
| Unemployed | 123 | 38.9 |
| Full-time homemaker | 21 | 6.6 |
| Pensioner | 58 | 18.4 |
| On a disability grant | 13 | 4.1 |
| Child grant | 4 | 1.3 |
| Not Assigned | 5 | 1.6 |
| Income | ||
| No income | 32 | 10.1 |
| R1–R800 | 39 | 12.3 |
| R801–R1,600 | 42 | 23.4 |
| R1601–R3200 | 94 | 29.8 |
| R3201–R6400 | 74 | 13.3 |
| R6401–R12,800 | 19 | 6.0 |
| R12,801–R51,200 | 11 | 3.5 |
| Not Assigned | 5 | 1.6 |
| Risks Factors (N = 316) | ||
|---|---|---|
| N | % | |
| Waist circumference (cm), median (25th–75th percentiles) (NA = 4) | 102.00 [95.08–111.11] | |
| Body mass index (BMI, kg/m2), median (25th–75th percentiles) | 34.85 [29.93–40.74] | |
| BMI | ||
| Underweight (<18.5) | 0 | 0.0 |
| Normal weight (18.5–24.9) | 12 | 3.8 |
| Overweight (25.0 to 29.9) | 67 | 21.2 |
| Obese | 233 | 73.7 |
| Class 1 (30.0 to 34.9) | 80 | 34.3 |
| Class 2 (35.0 to 39.9) | 62 | 26.6 |
| Class 3 (≥40) | 91 | 39.1 |
| Not documented | 4 | 1.3 |
| Family medical history | ||
| Having at least one known diabetic close relative | 141 | 44.6 |
| Do not have one known diabetic close relative | 57 | 18.0 |
| Do not know | 114 | 36.1 |
| Not documented | 4 | 1.3 |
| Blood pressure | ||
| Optimal/normal (<120/120–129 mmHg/<80/80–84 mmHg) | 129 | 40.8 |
| High normal (130–139 mmHg/85–89 mmHg) | 71 | 22.5 |
| Hypertension (≥140 mmHg/90 mmHg) | 93 | 29.4 |
| Isolated systolic hypertension (≥140 mmHg/<90 mmHg) | 19 | 6.0 |
| Not documented | 4 | 1.3 |
| Glycated haemoglobin (HbA1c) | ||
| <5.7 mmol/L | 99 | 31.3 |
| ≥5.7 mmol/L | 206 | 65.2 |
| Not documented | 11 | 3.5 |
| Alcohol consumption | ||
| Abstainer | 174 | 55.1 |
| Less than once a month | 51 | 16.1 |
| 1–3 days per month | 45 | 14.2 |
| Several times per week | 42 | 13.3 |
| Not documented | 4 | 1.3 |
| Tobacco status | ||
| Non-smoker (never smoked tobacco) | 190 | 60.1 |
| Current Smoker (daily or occasionally) | 83 | 26.3 |
| Ex-smoker | 40 | 12.7 |
| Not documented | 3 | 0.9 |
| Stress | ||
| Having an ongoing problem/stressor | 154 | 48.7 |
| Having no chronic difficulties | 157 | 49.7 |
| Not documented | 5 | 1.6 |
| Physical Activity Patterns | Median | 25th–75th Percentiles |
|---|---|---|
| Total time spending doing PA (minutes/week) | 720.00 | [240.00–1710.00] |
| At work | 360.00 | [0.00–1050.00] |
| For transport | 180.00 | [60.00–360.00] |
| For leisure | 30.00 | [0.00–180.00] |
| Sedentary (minutes/week) | 1260.00 | [630.00–1680.00] |
| N | % | |
| Practice of PA | ||
| In general | ||
| Yes | 290 | 95.1 |
| No | 15 | 4.9 |
| At work | ||
| Yes | 221 | 72.5 |
| No | 84 | 27.5 |
| For transport | ||
| Yes | 265 | 86.9 |
| No | 40 | 13.1 |
| For leisure | ||
| Yes | 157 | 51.5 |
| No | 148 | 48.5 |
| Vigorous-intensity | ||
| Yes | 39 | 12.8 |
| No | 266 | 87.2 |
| WHO recommendations * | ||
| Does not meet recommendations | 40 | 13.1 |
| Meets recommendations | 265 | 86.9 |
| Short Form-36—Physical Functioning Subscale | ||
|---|---|---|
| N | % | |
| Poor health limits the following activities: | ||
| Vigorous activities | 202 | 64.3 |
| Moderate activities | 101 | 32.2 |
| Lift/carry groceries | 62 | 19.7 |
| Climb several flights of stairs | 104 | 33.1 |
| Climb one flight of stairs | 74 | 23.6 |
| Bending/kneeling/stooping | 99 | 31.5 |
| Walk more than one kilometre | 75 | 23.9 |
| Walk several hundreds of meters | 82 | 26.1 |
| Walk one hundred meters | 73 | 23.2 |
| Bath and dress oneself | 23 | 7.3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hill, J.; Lavigne Delville, C.; Auorousseau, A.-M.; Jonathan, D.; Peer, N.; Oldenburg, B.; Kengne, A.-P. Development of a Tool to Increase Physical Activity among People at Risk for Diabetes in Low-Resourced Communities in Cape Town. Int. J. Environ. Res. Public Health 2020, 17, 865. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030865
Hill J, Lavigne Delville C, Auorousseau A-M, Jonathan D, Peer N, Oldenburg B, Kengne A-P. Development of a Tool to Increase Physical Activity among People at Risk for Diabetes in Low-Resourced Communities in Cape Town. International Journal of Environmental Research and Public Health. 2020; 17(3):865. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030865
Chicago/Turabian StyleHill, Jillian, Camille Lavigne Delville, Anne-Marie Auorousseau, Deborah Jonathan, Nasheeta Peer, Brian Oldenburg, and Andre-Pascal Kengne. 2020. "Development of a Tool to Increase Physical Activity among People at Risk for Diabetes in Low-Resourced Communities in Cape Town" International Journal of Environmental Research and Public Health 17, no. 3: 865. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030865