Endoscopic Treatment and Pulmonary Rehabilitation for Management of Lung Abscess in Elderly Lymphoma Patients

 , , , and
, , , and
Abstract
:1. Introduction
2. Materialsand Methods
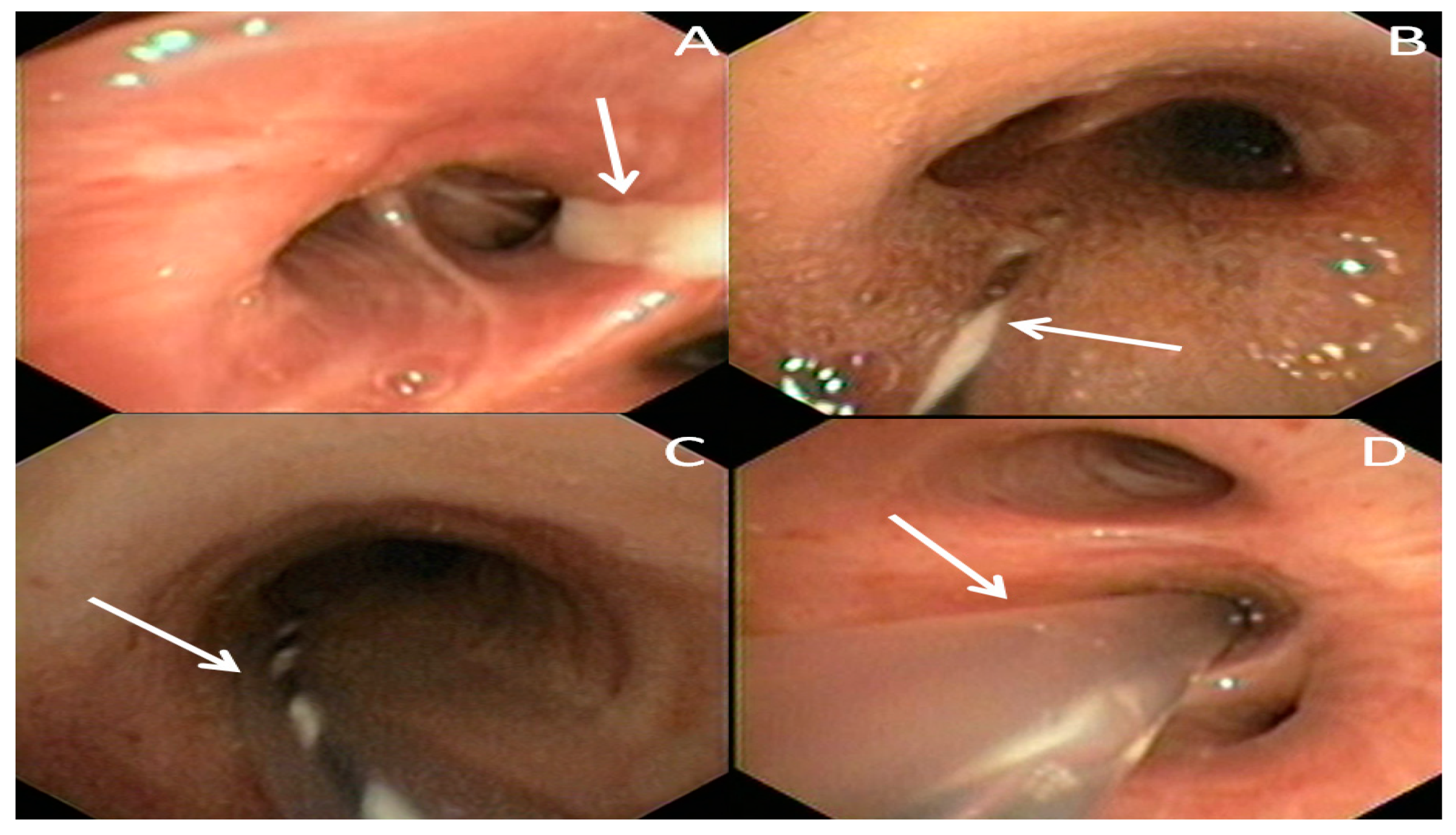
2.1. Endoscopic Procedure
2.2. Respiratory RehabilitationProgram
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kuhajda, I.; Zarogoulidis, K.; Tsirgogianni, K.; Tsavlis, D.; Kioumis, I.; Kosmidis, C.; Tsakiridis, K.; Mpakas, A.; Zarogoulidis, P.; Zissimopoulos, A.; et al. Lung abscess-etiology, diagnostic and treatment options. Ann. Transl. Med. 2015, 3, 183. [Google Scholar] [PubMed]
- Loukeri, A.A.; Kampolis, C.F.; Tomos, P.; Papapetrou, D.; Pantazopoulos, I.; Tzagkaraki, A.; Veldekis, D.; Lolis, N. Diagnosis, treatment and prognosis of lung abscess. Pneumon 2015, 28, 54–60. [Google Scholar]
- Herth, F.; Ernst, A.; Becker, H.D. Endoscopic Drainage of Lung Abscesses. Chest 2005, 127, 1378. [Google Scholar] [PubMed]
- Sica, A.; Vitiello, P.; Papa, A.; Calogero, A.; Sagnelli, C.; Casale, D.; Mottola, M.; Svanera, G.; Dodaro, C.A.; Martinelli, E.; et al. Use of rituximab in NHL malt type pregnant in I° trimester for two times. Open Med. 2019, 14, 757–760. [Google Scholar] [CrossRef]
- Reginelli, A.; Belfiore, M.P.; Russo, A.; Turriziani, F.; Moscarella, E.; Troiani, T.; Brancaccio, G.; Ronchi, A.; Giunta, E.; Sica, A.; et al. A preliminary study for quantitative assessment with HFUS (High Frequency ultrasound) of nodular skin melanoma Breslow thickness in adults before surgery: Interdisciplinary team experience. Curr. Radiopharm. 2019, 12, 1. [Google Scholar] [CrossRef]
- Unterman, A.; Fruchter, O.; Rosengarten, D.; Izhakian, S.; Abdel-Rahman, N.; Kramer, M.R. Bronchoscopic Drainage of Lung Abscesses Using a Pigtail Catheter. Respiration 2017, 93, 99–105. [Google Scholar] [CrossRef]
- Sica, A.; Vitiello, P.; Sorriento, A.; Ronchi, A.; Calogero, A.; Sagnelli, C.; Troiani, T.; Fasano, M.; Dodaro, C.A.; Franco, R.; et al. Lymphomatoid papulosis: Overview. Minerva Med. 2020. [Google Scholar] [CrossRef]
- Merli, M.; Frigeni, M.; Alric, L.; Visco, C.; Besson, C.; Mannelli, L.; Di Rocco, A.; Ferrari, A.; Farina, L.; Pirisi, M.; et al. Direct-Acting Antivirals in Hepatitis C Virus-Associated Diffuse Large B-cell Lymphomas. Oncology 2018, 24, e720–e729. [Google Scholar] [CrossRef] [Green Version]
- Coppola, N.; Pisaturo, M.; Guastafierro, S.; Tonziello, G.; Sica, A.; Iodice, V.; Sagnelli, C.; Ferrara, M.G.; Sagnelli, E. Increased hepatitis C viral load and reactivation of liver disease in HCV RNA-positive patients with onco-haematological disease undergoing chemotherapy. Dig. Liver Dis. 2012, 44, 49–54. [Google Scholar] [CrossRef]
- Pisaturo, M.; Guastafierro, S.; Filippini, P.; Tonziello, G.; Sica, A.; Di Martino, F.; Sagnelli, C.; Ferrara, M.G.; Martini, S.; Cozzolino, D.; et al. Absence of occult HCV infection in patients experiencing an immunodepression condition. Infez. Med. 2013, 21, 296–301. [Google Scholar]
- Coppola, N.; Pisaturo, M.; Guastafierro, S.; Tonziello, G.; Sica, A.; Sagnelli, C.; Ferrara, M.G.; Sagnelli, E. Absence of occult hepatitis C virus infection in patients under immunosupressive therapy for oncohematological diseases. Hepatology 2011, 54, 1487–1489. [Google Scholar] [CrossRef]
- Tonziello, G.; Pisaturo, M.; Sica, A.; Ferrara, M.G.; Sagnelli, C.; Pasquale, G.; Sagnelli, E.; Guastafierro, S.; Coppola, N. Transient reactivation of occult hepatitis B virus infection despite lamivudine prophylaxis in a patient treated for non-Hodgkin lymphoma. Infection 2013, 41, 225–229. [Google Scholar] [CrossRef]
- Fiorelli, A.; Vicidomini, G.; Mazzella, A.; Messina, G.; Milione, R.; Di Crescenzo, V.G.; Santini, M. The Influence of Body Mass Index and Weight Loss on Outcome of Elderly Patients Undergoing Lung Cancer Resection. Thorac. Cardiovasc. Surg. 2014, 62, 578–587. [Google Scholar] [CrossRef]
- Caccavale, S.; Vitiello, P.; Franco, R.; Panarese, I.; Ronchi, A.; Sica, A.; Toncic, R.J.; Alfano, R.; Argenziano, G. Dermoscopic characterization of folliculotropic mycosis fungoides selectively localized on trunk and limbs. Int. J. Dermatol. 2019, 58, e187–e189. [Google Scholar] [CrossRef]
- Neuthof, H.; Touroff, A.S.W. Acute putrid abscess of the lung. Hyperacute variety. J. Thorac. Surg. 1942, 12, 98–106. [Google Scholar]
- Monaldi, V. Endocavitary Aspiration in the Treatment of Lung Abscess. Dis. Chest 1956, 29, 193–201. [Google Scholar] [CrossRef]
- Sica, A.; Casale, B.; Di Dato, M.T.; Calogero, A.; Spada, A.; Sagnelli, C.; Santagata, M.; Buonavolontà, P.; Fiorelli, A.; Salzano, A.; et al. Cancer and not cancer related chronic pain: From the physiopathological bases to the management. Open Med. 2019, 14, 761–766. [Google Scholar] [CrossRef]
- Sica, A.; Casale, B.; Spada, A.; Di Dato, M.T.; Sagnelli, C.; Calogero, A.; Buonavolontà, P.; Salzano, A.; Martinelli, E.; Saracco, E.; et al. Differential diagnosis: Retroperitoneal fibrosis and oncological diseases. Open Med. 2019, 15, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.-J.; Wu, H.-B.; Zhang, Y.; Zhou, W.-L.; Wang, Q.-S. A Rare Case of Neutrophil-Rich, ALK-Negative Anaplastic Large Cell Lymphoma in the Lung Mimicking a Pulmonary Abscess on 18F-FDG PET/CT. Clin. Nucl. Med. 2019, 44, 234–237. [Google Scholar] [CrossRef]
- Foderaro, A.E.; Reagan, J.L. Hodgkin lymphoma mimicking lung abscess. Blood 2016, 128, 3011. [Google Scholar] [CrossRef] [Green Version]
- Viscardi, G.; Zanaletti, N.; Ferrara, M.G.; Sica, A.; Falcone, U.; Guastafierro, S.; Bracale, U.; Ribero, D.; Fasano, M.; Napolitano, S.; et al. Atypical haemolytic-uraemic syndrome in patient with metastatic colorectal cancer treated with fluorouracil and oxaliplatin: A case report and a review of literature. ESMO Open 2019, 4, e000551. [Google Scholar] [CrossRef] [Green Version]
- Calogero, A.; Sagnelli, C.; Carlomagno, N.; Tammaro, V.; Candida, M.; Vernillo, A.; Peluso, G.; Minieri, G.; Sica, A.; Ciccozzi, M.; et al. Familial polyposis coli: The management of desmoid tumor bleeding. Open Med. 2019, 14, 572–576. [Google Scholar] [CrossRef]
- Fiorelli, A.; Izzo, A.C.; Frongillo, E.M.; Del Prete, A.; Liguori, G.; Di Costanzo, E.; Vicidomini, G.; Santini, M. Efficacy of wound analgesia for controlling post-thoracotomy pain: A randomized double-blind study. Eur. J. Cardiothorac. Surg. 2016, 49, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Yuba, T.; Hatsuse, M.; Kodama, M.; Uda, S.; Yoshimura, A.; Kurisu, N. Reactivation of Tuberculosis Presenting With Empyema Due to Anticancer Chemotherapy for Diffuse Large B Cell Lymphoma. Kekkaku [Tuberculosis] 2016, 91, 475–479. [Google Scholar]
- Chae, J.; Kern, R.; Nelson, D.; Mullon, J. Diffuse large B cell lymphoma with superimposed lung abscess: Potential role for intracavitaryfibrinolytic therapy through a percutaneous drain to facilitate lung abscess drainage. BMJ Case Rep. 2018, 11. [Google Scholar] [CrossRef]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Naidu, B. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery after Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardiothorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef]
- Qiu, Z.; He, M.; Yu, S.; Wang, L.; Lv, H. Efficiency and Safety of Pulmonary Rehabilitation in Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Med. Sci. Monit. 2015, 21, 806–812. [Google Scholar] [CrossRef] [Green Version]
- Katajisto, M.; Laitinen, T. Estimating the effectiveness of pulmonary rehabilitation for COPD exacerbations: Reduction of hospital inpatient days during the following year. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 2763–2769. [Google Scholar] [CrossRef] [Green Version]
- Vincent, E.; Chaplin, E.J.; Williams, J.E.; Harvey-Dunstan, T.; Greening, N.J.; Steiner, M.C.; Morgan, M.D.; Singh, S.J. Experiences of patients undergoing pulmonary rehabilitation during an exacerbation of chronic respiratory disease. Chronic Respir. Dis. 2017, 14, 298–308. [Google Scholar] [CrossRef] [Green Version]
- Wada, J.T.; Borges-Santos, E.; Porras, D.C.; Paisani, D.M.; Cukier, A.; Lunardi, A.C.; Carvalho, C.R. Effects of aerobic training combined with respiratory muscle stretching on the functional exercise capacity and thoracoabdominal kinematics in patients with COPD: A randomized and controlled trial. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2691–2700. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patient No. | Lymphoproliferative Disease | Sex | Age, Years | Catheter, Days | Cultural Test | Discharge, Days |
|---|---|---|---|---|---|---|
| 1 | Hodgkinlymphoma | M | 54 | 3 | Staphylococcus aureus | 7 |
| 2 | Large B-cell lymphoma | M | 67 | 4 | Enterobacter sp. | 12 |
| 3 | Follicular lymphoma | F | 49 | 4 | negative | 6 |
| 4 | Hodgkin lymphoma | M | 72 | 3 | Pseudomonas sp. | 8 |
| 5 | Large B-cell lymphoma | F | 70 | 5 | Staphylococcus aureus | 8 |
| 6 | Hodgkin lymphoma | M | 64 | 4 | Negative | 10 |
| 7 | Mycosisfungoides | F | 55 | 3 | Klebsiella sp. | 9 |
| 8 | Large B-cell lymphoma | F | 58 | 4 | Enterobacter sp. | 7 |
| 9 | Hodgkin lymphoma | M | 61 | 4 | negative | 8 |
| 10 | Hodgkin lymphoma | M | 45 | 5 | Klebsiella sp. | 13 |
| 11 | MALT lymphoma | M | 53 | 4 | negative | 15 |
| 12 | Large B-cell lymphoma | F | 72 | 5 | Enterobacter sp. | 9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cascone, R.; Sica, A.; Sagnelli, C.; Carlucci, A.; Calogero, A.; Santini, M.; Fiorelli, A. Endoscopic Treatment and Pulmonary Rehabilitation for Management of Lung Abscess in Elderly Lymphoma Patients. Int. J. Environ. Res. Public Health 2020, 17, 997. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030997
Cascone R, Sica A, Sagnelli C, Carlucci A, Calogero A, Santini M, Fiorelli A. Endoscopic Treatment and Pulmonary Rehabilitation for Management of Lung Abscess in Elderly Lymphoma Patients. International Journal of Environmental Research and Public Health. 2020; 17(3):997. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030997
Chicago/Turabian StyleCascone, Roberto, Antonello Sica, Caterina Sagnelli, Annalisa Carlucci, Armando Calogero, Mario Santini, and Alfonso Fiorelli. 2020. "Endoscopic Treatment and Pulmonary Rehabilitation for Management of Lung Abscess in Elderly Lymphoma Patients" International Journal of Environmental Research and Public Health 17, no. 3: 997. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030997