The Unique Extended Selection Cohorts Design for the Evaluation of the School-Based Jump-In Intervention on Dietary Habits: A Study Protocol


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
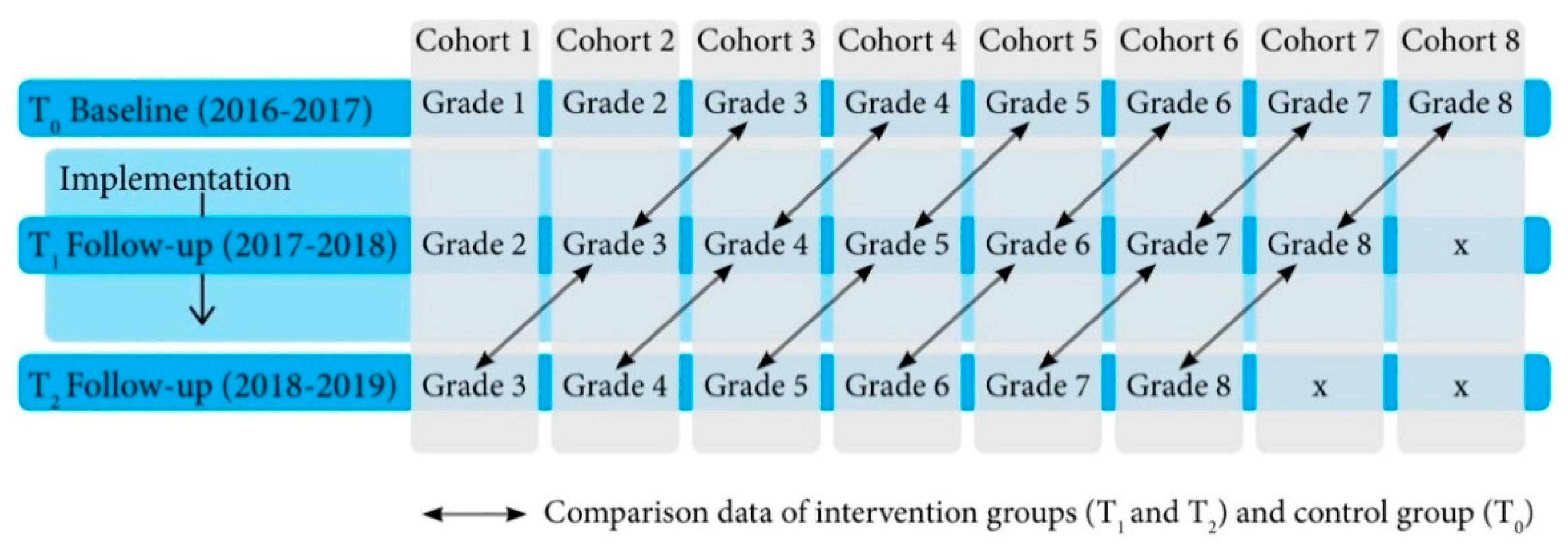
2.1. Study Design
2.1.1. Mixed Methods Design
2.1.2. Effect Evaluation
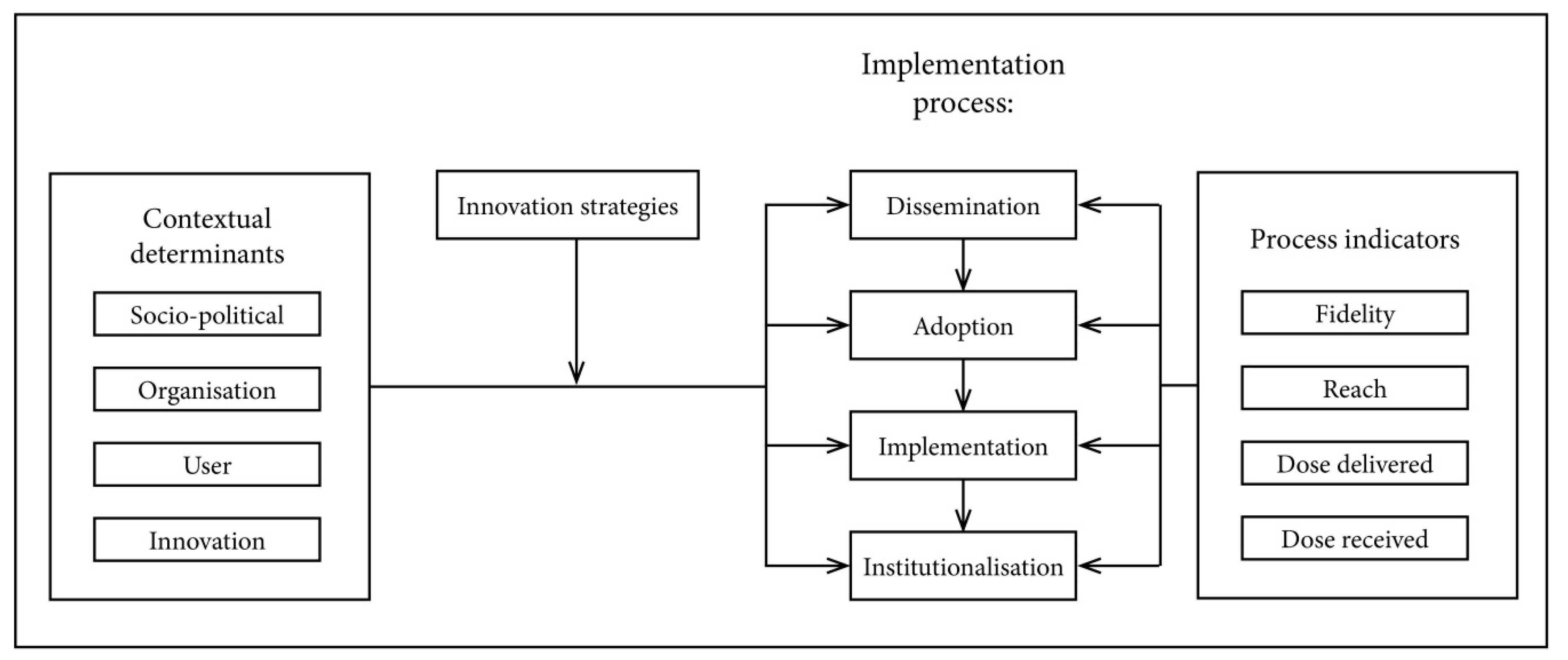
2.1.3. Process Evaluation
2.1.4. Quantitative Implementation Measures
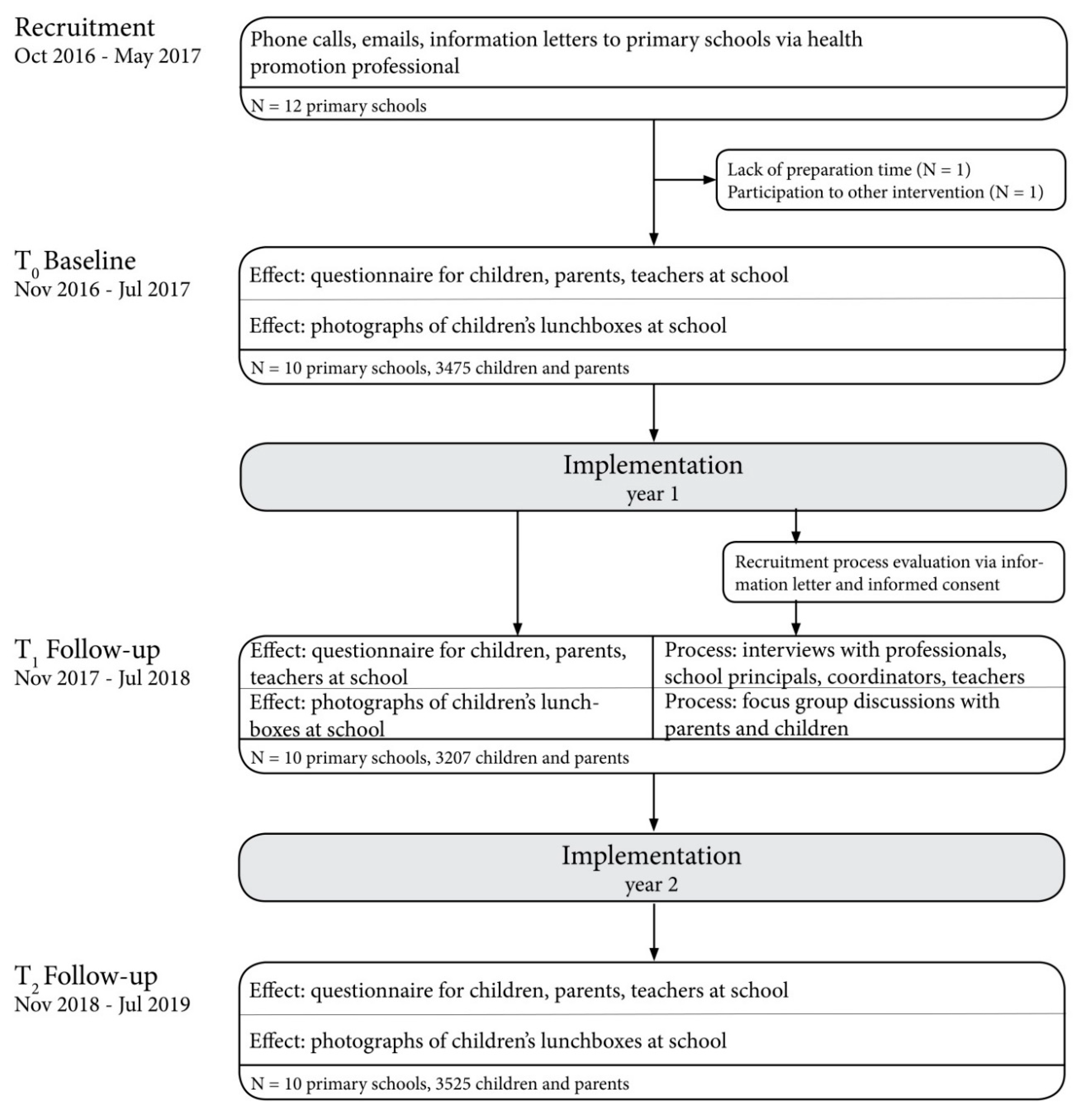
2.2. Procedures
2.2.1. Recruitment of Primary Schools
2.2.2. Consent
2.3. Outcome Measures
2.3.1. Effect Measures
2.3.2. Process Measures
2.4. Analyses
2.4.1. Quantitative Analysis
2.4.2. Qualitative Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNICEF; WHO; World Bank Group. Levels and Trends in Child Malnutrition: UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates, Key Findings of the 2017 Edition; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- NCD-RisC. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Bouthoorn, S.H.; Wijtzes, A.I.; Jaddoe, V.W.; Hofman, A.; Raat, H.; van Lenthe, F.J. Development of socioeconomic inequalities in obesity among Dutch pre-school and school-aged children. Obesity 2014, 22, 2230–2237. [Google Scholar] [CrossRef]
- van Dommelen, P.; Schonbeck, Y.; HiraSing, R.A.; van Buuren, S. Call for early prevention: Prevalence rates of overweight among Turkish and Moroccan children in The Netherlands. Eur. J. Public Health 2015, 25, 828–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Export Consultation; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- Singh, A.S.; Mulder, C.; Twisk, J.W.; van Mechelen, W.; Chinapaw, M.J. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef]
- CBS; RIVM; Voedingscentrum. Kinderen eten te Weinig Fruit, Groente en Vis. Available online: https://www.cbs.nl/nl-nl/nieuws/2017/46/kinderen-eten-te-weinig-fruit-groente-en-vis (accessed on 2 February 2020).
- WHO. Guideline: Sugars Intake for Adults and Children; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- RIVM. Resultaten van de VCP 2012–2016. Available online: https://www.wateetnederland.nl/onderwerpen/suiker (accessed on 26 November 2019).
- Sluik, D.; Engelen, A.; Feskens, E.J.M. Suikerconsumptie in Nederland: Resultaten uit de Nederlandse Voedselconsumptiepeiling 2007–2010; Wageningen University and Research Centre: Wageningen, The Netherlands, 2013. [Google Scholar]
- Langford, R.; Bonell, C.P.; Jones, H.E.; Pouliou, T.; Murphy, S.M.; Waters, E.; Komro, K.A.; Gibbs, L.F.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst. Rev. 2014, CD008958. [Google Scholar] [CrossRef] [PubMed]
- Nathan, N.; Janssen, L.; Sutherland, R.; Hodder, R.K.; Evans, C.E.L.; Booth, D.; Yoong, S.L.; Reilly, K.; Finch, M.; Wolfenden, L. The effectiveness of lunchbox interventions on improving the foods and beverages packed and consumed by children at centre-based care or school: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 38. [Google Scholar] [CrossRef] [Green Version]
- Brug, J.; van Stralen, M.M.; Chinapaw, M.J.; De Bourdeaudhuij, I.; Lien, N.; Bere, E.; Singh, A.S.; Maes, L.; Moreno, L.; Jan, N.; et al. Differences in weight status and energy-balance related behaviours according to ethnic background among adolescents in seven countries in Europe: The ENERGY-project. Pediatric Obes. 2012, 7, 399–411. [Google Scholar] [CrossRef]
- Mackenbach, J.D.; Nelissen, K.G.M.; Dijkstra, S.C.; Poelman, M.P.; Daams, J.G.; Leijssen, J.B.; Nicolaou, M. A Systematic Review on Socioeconomic Differences in the Association between the Food Environment and Dietary Behaviors. Nutrients 2019, 11, 2215. [Google Scholar] [CrossRef] [Green Version]
- van Sluijs, E.M.; McMinn, A.M.; Griffin, S.J. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. BMJ 2007, 335, 703. [Google Scholar] [CrossRef] [Green Version]
- Busch, V.; van Opdorp, P.A.J.; Broek, J.; Harmsen, I.A. Bright spots, physical activity investments that work: JUMP-in: Promoting physical activity and healthy nutrition at primary schools in Amsterdam. Br. J. Sports Med. 2018, 52, 1299–1301. [Google Scholar] [CrossRef] [PubMed]
- De Meij, J.S.; Chinapaw, M.J.; Kremers, S.P.; Van der Wal, M.F.; Jurg, M.E.; Van Mechelen, W. Promoting physical activity in children: The stepwise development of the primary school-based JUMP-in intervention applying the RE-AIM evaluation framework. Br. J. Sports Med. 2010, 44, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Amsterdam Healthy Weight Programme. Factsheet Gewicht en Leefstijl van Kinderen in Amsterdam; July 2019; AHWP: Amsterdam, The Netherlands, 2019. [Google Scholar]
- de Meij, J.S.; Chinapaw, M.J.; van Stralen, M.M.; van der Wal, M.F.; van Dieren, L.; van Mechelen, W. Effectiveness of JUMP-in, a Dutch primary school-based community intervention aimed at the promotion of physical activity. Br. J. Sports Med. 2011, 45, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- de Meij, J.S.; van der Wal, M.F.; van Mechelen, W.; Chinapaw, M.J. A mixed methods process evaluation of the implementation of JUMP-in, a multilevel school-based intervention aimed at physical activity promotion. Health Promot. Pract. 2013, 14, 777–790. [Google Scholar] [CrossRef]
- Janssen, M.; Twisk, J.W.; Toussaint, H.M.; van Mechelen, W.; Verhagen, E.A. Effectiveness of the PLAYgrounds programme on PA levels during recess in 6-year-old to 12-year-old children. Br. J. Sports Med. 2015, 49, 259–264. [Google Scholar] [CrossRef]
- City of Amsterdam. Summary Amsterdam Healthy Weight Programme 2018–2021: Amsterdam Will Become the Healthiest City for Children; City of Amsterdam: Amsterdam, The Netherlands, 2017.
- WHO. International Panel of Experts on Sustainable Food Systems 2017; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Karna, A.; Voeten, M.; Little, T.D.; Poskiparta, E.; Alanen, E.; Salmivalli, C. Going to scale: A nonrandomized nationwide trial of the KiVa antibullying program for grades 1–9. J. Consult. Clin. Psychol. 2011, 79, 796–805. [Google Scholar] [CrossRef]
- Olweus, D. A useful evaluation design, and effects of the Olweus Bullying Prevention Program. Psychol. Crime Law 2005, 11, 389–402. [Google Scholar] [CrossRef]
- Oakley, A.; Strange, V.; Bonell, C.; Allen, E.; Stephenson, J.; Team, R.S. Process evaluation in randomised controlled trials of complex interventions. BMJ 2006, 332, 413–416. [Google Scholar] [CrossRef] [Green Version]
- Boeije, H.R.; Drabble, S.J.; O’Cathain, A. Methodological challenges of mixed methods intervention evaluations. Methodology 2015, 11, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Fleuren, M.; Wiefferink, K.; Paulussen, T. Determinants of innovation within health care organizations: Literature review and Delphi study. Int. J. Qual. Health Care 2004, 16, 107–123. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Cooper, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; et al. Process evaluation in complex public health intervention studies: The need for guidance. J. Epidemiol. Community Health 2014, 68, 101–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, R.P.; Evans, M.H.; Joshi, P. Developing a process-evaluation plan for assessing health promotion program implementation: A how-to guide. Health Promot. Pract. 2005, 6, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linnan, L.; Steckler, A.B. Process Evaluation for Public Health Interventions and Research; Jossey-Bass: San Francisco, CA, USA, 2002. [Google Scholar]
- NEVO-Online Versie 2019/6.0. Available online: https://nevo-online.rivm.nl/Default.aspx (accessed on 19 December 2019).
- Guinard, J.-X. Sensory and consumer testing with children. Trends Food Sci. Technol. 2000, 11, 273–283. [Google Scholar] [CrossRef]
- Hall, L.; Hume, C.; Tazzyman, S. Five Degrees of Happiness: Effective Smiley Face Likert Scales for Evaluating with Children. In Proceedings of the 15th International Conference on Interaction Design and Children, Manchester, UK, 21–24 June 2016; pp. 311–321. [Google Scholar]
- de Hoog, M.L.; van Eijsden, M.; Stronks, K.; Gemke, R.J.; Vrijkotte, T.G. Ethnic differences in cardiometabolic risk profile at age 5–6 years: The ABCD study. PLoS ONE 2012, 7, e43667. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.S.; Chinapaw, M.J.; Uijtdewilligen, L.; Vik, F.N.; van Lippevelde, W.; Fernandez-Alvira, J.M.; Stomfai, S.; Manios, Y.; van der Sluijs, M.; Terwee, C.; et al. Test-retest reliability and construct validity of the ENERGY-parent questionnaire on parenting practices, energy balance-related behaviours and their potential behavioural determinants: The ENERGY-project. BMC Res. Notes 2012, 5, 434. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.S.; Vik, F.N.; Chinapaw, M.J.; Uijtdewilligen, L.; Verloigne, M.; Fernandez-Alvira, J.M.; Stomfai, S.; Manios, Y.; Martens, M.; Brug, J. Test-retest reliability and construct validity of the ENERGY-child questionnaire on energy balance-related behaviours and their potential determinants: The ENERGY-project. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 136. [Google Scholar] [CrossRef] [Green Version]
- De Bourdeaudhuij, I.; Klepp, K.I.; Due, P.; Rodrigo, C.P.; de Almeida, M.; Wind, M.; Krolner, R.; Sandvik, C.; Brug, J. Reliability and validity of a questionnaire to measure personal, social and environmental correlates of fruit and vegetable intake in 10-11-year-old children in five European countries. Public Health Nutr. 2005, 8, 189–200. [Google Scholar] [CrossRef] [Green Version]
- Haraldsdóttir, J.; Thórsdóttir, I.; de Almeida, M.; Maes, L.; Pérez Rodrigo, C.; Elmadfa, I.; Andersen, F. Validity and Reproducibility of a Precoded Questionnaire to Assess Fruit and Vegetable Intake in European 11- to 12-Year-Old Schoolchildren. Ann. Nutr. Metab. 2005, 49, 221–227. [Google Scholar] [CrossRef]
- de Jong, E. Parenting and Home Environment as Targets in Childhood Overweight Prevention: Results from the ChecKid Study. Ph.D. Thesis, Vrije Universiteit Amsterdam, Amsterdam, Netherlands, 2013. [Google Scholar]
- van Nassau, F.; Singh, A.S.; Broekhuizen, D.; van Mechelen, W.; Brug, J.; Chinapaw, M.J. Barriers and facilitators to the nationwide dissemination of the Dutch school-based obesity prevention programme DOiT. Eur. J. Public Health 2016, 26, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Scherbaum, C.; Ferreter, J. Estimating Statistical Power and Required Sample Sizes for Organizational Research Using Multilevel Modeling. SAGE Publ. 2009, 12, 347–367. [Google Scholar] [CrossRef]
- Cornelisse-Vermaat, J.R.; van den Brink, H.M. Ethnic differences in lifestyle and overweight in The Netherlands. Obesity 2007, 15, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Hebert, J.R.; Clemow, L.; Pbert, L.; Ockene, I.S.; Ockene, J.K. Social desirability bias in dietary self-report may compromise the validity of dietary intake measures. Int. J. Epidemiol. 1995, 24, 389–398. [Google Scholar] [CrossRef]
- Klesges, L.M.; Baranowski, T.; Beech, B.; Cullen, K.; Murray, D.M.; Rochon, J.; Pratt, C. Social desirability bias in self-reported dietary, physical activity and weight concerns measures in 8- to 10-year-old African-American girls: Results from the Girls Health Enrichment Multisite Studies (GEMS). Prev. Med. 2004, 38, 78–87. [Google Scholar] [CrossRef] [PubMed]
- McMurray, R.G.; Ring, K.B.; Treuth, M.S.; Welk, G.J.; Pate, R.R.; Schmitz, K.H.; Pickrel, J.L.; Gonzalez, V.; Almedia, M.J.; Young, D.R.; et al. Comparison of two approaches to structured physical activity surveys for adolescents. Med. Sci. Sports Exerc. 2004, 36, 2135–2143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, T.M.; Abdel-Maksoud, M.F.; Crane, L.A.; Marcus, A.C.; Byers, T.E. Effects of social approval bias on self-reported fruit and vegetable consumption: A randomized controlled trial. Nutr. J. 2008, 7, 18. [Google Scholar] [CrossRef] [Green Version]
- Livingstone, M.B.; Robson, P.J.; Wallace, J.M. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92 (Suppl. S2), S213–S222. [Google Scholar] [CrossRef]
- Tak, N.I.; te Velde, S.J.; de Vries, J.H.; Brug, J. Parent and child reports of fruit and vegetable intakes and related family environmental factors show low levels of agreement. J. Hum. Nutr. Diet 2006, 19, 275–285. [Google Scholar] [CrossRef]
- Taylor, J.C.; Yon, B.A.; Johnson, R.K. Reliability and validity of digital imaging as a measure of schoolchildren’s fruit and vegetable consumption. J. Acad Nutr. Diet 2014, 114, 1359–1366. [Google Scholar] [CrossRef]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takens, F.E.; Busch, V.; Ujčič-Voortman, J.K.; van Eijsden, M.; Chinapaw, M.J.M. The Unique Extended Selection Cohorts Design for the Evaluation of the School-Based Jump-In Intervention on Dietary Habits: A Study Protocol. Int. J. Environ. Res. Public Health 2020, 17, 1145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041145
Takens FE, Busch V, Ujčič-Voortman JK, van Eijsden M, Chinapaw MJM. The Unique Extended Selection Cohorts Design for the Evaluation of the School-Based Jump-In Intervention on Dietary Habits: A Study Protocol. International Journal of Environmental Research and Public Health. 2020; 17(4):1145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041145
Chicago/Turabian StyleTakens, Froukje E., Vincent Busch, Joanne K. Ujčič-Voortman, Manon van Eijsden, and Mai J. M. Chinapaw. 2020. "The Unique Extended Selection Cohorts Design for the Evaluation of the School-Based Jump-In Intervention on Dietary Habits: A Study Protocol" International Journal of Environmental Research and Public Health 17, no. 4: 1145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041145