Relationship between Cortisol Changes during the Night and Subjective and Objective Sleep Quality in Healthy Older People

 ,
,
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Procedure
2.3. Cortisol Measurements.
2.4. Measurements of Subjective Sleep and Stress Perception at Home
2.5. Objective Sleep Measurements
2.6. Statistical Analysis and Data Management
3. Results
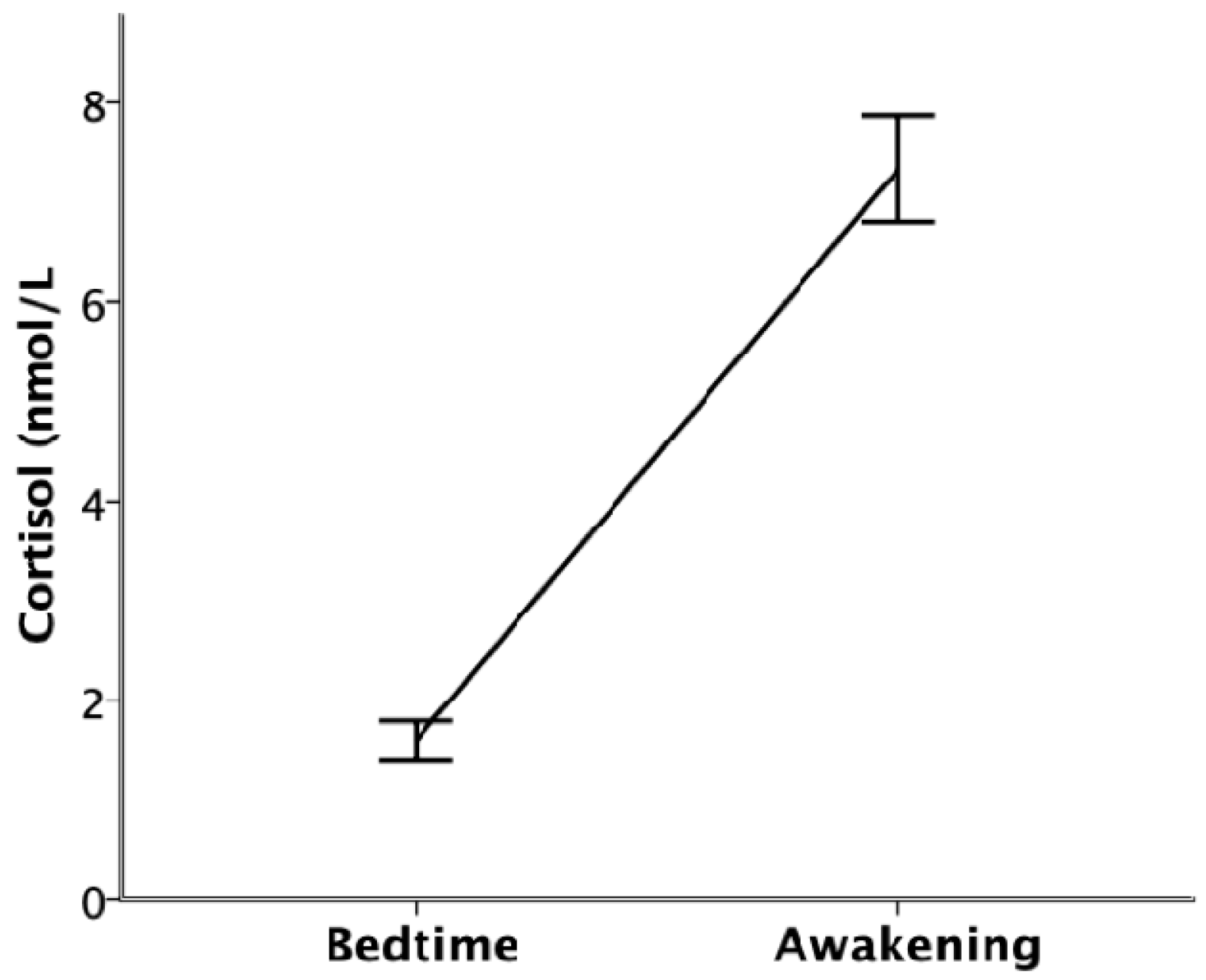
3.1. Cortisol Levels
3.2. Relationship between Sleep Parameters and Cortisol
3.2.1. Relationship with Subjective and Objective Sleep Quality
3.2.2. Relationship with the Discrepancy between Subjective and Objective Sleep Quality
3.2.3. Analyses Excluding Participants Suspected of Nonadherence to the Protocol
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mander, B.A.; Winer, J.R.; Walker, M.P. Sleep and Human Aging. Neuron 2017, 94, 19–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruno, R.M.; Palagini, L.; Gemignani, A.; Virdis, A.; Giulio, A.D.; Ghiadoni, L.; Riemann, D.; Taddei, S. Poor sleep quality and resistant hypertension. Sleep Med. 2013, 14, 1157–1163. [Google Scholar] [CrossRef] [PubMed]
- De Gennaro, L.D.; Martina, M.; Curcio, G.; Ferrara, M. The relationship between alexithymia, depression, and sleep complaints. Psychiatry Res. 2004, 128, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.S.P.; Kowgier, M.; Yu, L.; Buchman, A.S.; Bennett, D.A. Sleep Fragmentation and the Risk of Incident Alzheimer’s Disease and Cognitive Decline in Older Persons. Sleep 2013, 36, 1027–1032. [Google Scholar] [CrossRef] [Green Version]
- Landry, G.J.; Best, J.R.; Liu-Ambrose, T. Measuring sleep quality in older adults: A comparison using subjective and objective methods. Fron Aging Neurosci. 2015, 7, 166. [Google Scholar] [CrossRef] [Green Version]
- Ohayon, M.; Wickwire, E.M.; Hirshkowitz, M.; Albert, S.M.; Avidan, A.; Daly, F.J.; Dauvilliers, Y.; Ferri, R.; Fung, C.; Gozal, D.; et al. National Sleep Foundation’s sleep quality recommendations: First report. Sleep Health 2017, 3, 6–19. [Google Scholar] [CrossRef] [Green Version]
- Van der Berg, J.F.; Miedema, H.M.; Tulen, J.H.; Hofman, A.; Neven, A.K.; Tiemeier, H. Sex Differences in Subjective and Actigraphic Sleep Measures: A Population-Based Study of Elderly Persons. Sleep 2009, 32, 1367–1375. [Google Scholar] [CrossRef]
- Unruh, M.; Redline, S.; An, M.-W.; Buysse, D.J.; Nieto, F.J.; Yeh, J.-L.; Newman, A.B. Subjective and Objective Sleep Quality and Aging in the Sleep Heart Health Study. J. Am. Geriatr. Soc. 2008, 56, 1218–1227. [Google Scholar] [CrossRef]
- Jackowska, M.; Dockray, S.; Hendrickx, H.; Steptoe, A. Psychosocial Factors and Sleep Efficiency. Psychosom. Med. 2011, 73, 810–816. [Google Scholar] [CrossRef]
- Jackowska, M.; Ronaldson, A.; Brown, J.; Steptoe, A. Biological and psychological correlates of self-reported and objective sleep measures. J. Psychosom. Res. 2016, 84, 52–55. [Google Scholar] [CrossRef]
- Ren, R.; Covassin, N.; Yang, L.; Li, Y.; Zhang, Y.; Zhou, J.; Tan, L.; Li, T.; Li, X.; Wang, Y.; et al. Objective but Not Subjective Short Sleep Duration Is Associated with Hypertension in Obstructive Sleep Apnea. Hypertension 2018, 72, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Zilli, I.; Ficca, G.; Salzarulo, P. Factors involved in sleep satisfaction in the elderly. Sleep Med. 2009, 10, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Buckley, T.M.; Schatzberg, A.F. On the Interactions of the Hypothalamic-Pituitary-Adrenal (HPA) Axis and Sleep: Normal HPA Axis Activity and Circadian Rhythm, Exemplary Sleep Disorders. J. Clin. Endocrin. Met. 2005, 90, 3106–3114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elder, G.J.; Wetherell, M.A.; Barclay, N.L.; Ellis, J.G. The cortisol awakening response—Applications and implications for sleep medicine. Sleep Med. Rev. 2014, 18, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, J.; Junghanns, K.; Hohagen, F. Sleep disturbances are correlated with decreased morning awakening salivary cortisol. Psychoneuroendocrinology 2004, 29, 1184–1191. [Google Scholar] [CrossRef]
- Castro-Diehl, C.; Diez Roux, A.V.; Redline, S.; Seeman, T.; Shrager, S.E.; Shea, S. Association of sleep duration and quality with alterations in the hypothalamic-pituitary adrenocortical axis: The multi-ethnic study of atherosclerosis (MESA). J. Clin. Endocrin. Met. 2015, 100, 3149–3158. [Google Scholar] [CrossRef]
- Van Lenten, S.A.V.; Doane, L.D. Examining multiple sleep behaviors and diurnal salivary cortisol and alpha-amylase: Within- and between-person associations. Psychoneuroendocrinology 2016, 68, 100–110. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Ma, R.C.; Kong, A.P.; So, W.Y.; Li, A.M.; Lam, S.P.; Li, S.X.; Yu, M.W.; Ho, C.S.; Chan, M.H.; et al. Relationship of Sleep Quantity and Quality with 24-Hour Urinary Catecholamines and Salivary Awakening Cortisol in Healthy Middle-Aged Adults. Sleep 2011, 34, 225–233. [Google Scholar] [CrossRef] [Green Version]
- Nader, N.; Chrousos, G.P.; Kino, T. Interactions of the circadian CLOCK system and the HPA axis. Trends Endocrin. Met. 2010, 21, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Rosmond, R.; Dallman, M.F.; Björntorp, P. Stress-Related Cortisol Secretion in Men: Relationships with Abdominal Obesity and Endocrine, Metabolic and Hemodynamic Abnormalities. J. Clin. Endocrin. Met. 1998, 83, 1853–1859. [Google Scholar] [CrossRef]
- Adam, E.K.; Quinn, M.E.; Tavernier, R.; McQuillan, M.T.; Dahlke, K.A.; Gilbert, K.E. Diurnal cortisol slopes and mental and physical health outcomes: A systematic review and meta-analysis. Psychoneuroendocrinology 2017, 83, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Pulopulos, M.M.; Hidalgo, V.; Puig-Perez, S.; Salvador, A. Cortisol awakening response and cognitive performance in hypertensive and normotensive older people. Horm. Behav. 2016, 83, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Sapolsky, R.M.; Romero, L.M.; Munck, A.U. How Do Glucocorticoids Influence Stress Responses? Integrating Permissive, Suppressive, Stimulatory, and Preparative Actions∗. Endocrin. Rev. 2000, 21, 55–89. [Google Scholar]
- Rodenbeck, A.; Huether, G.; Rüther, E.; Hajak, G. Interactions between evening and nocturnal cortisol secretion and sleep parameters in patients with severe chronic primary insomnia. Neurosc. Let. 2002, 324, 159–163. [Google Scholar] [CrossRef]
- Born, J.; Schenk, U.; Späth-Schwalbe, E.; Fehm, H. Influences of partial REM sleep deprivation and awakenings on nocturnal cortisol release. Biol. Psychiat. 1988, 24, 801–811. [Google Scholar] [CrossRef]
- Riemann, D.; Klein, T.; Rodenbeck, A.; Feige, B.; Horny, A.; Hummel, R.; Weske, G.; Al-Shajlawi, A.; Voderholzer, U. Nocturnal cortisol and melatonin secretion in primary insomnia. Psychiat Res. 2002, 113, 17–27. [Google Scholar] [CrossRef]
- Tasali, E.; Leproult, R.; Ehrmann, D.A.; Cauter, E.V. Slow-wave sleep and the risk of type 2 diabetes in humans. Proc. Nat. Acad. Sci. USA 2008, 105, 1044–1049. [Google Scholar] [CrossRef] [Green Version]
- Lobo, A.; Saz, P.; Marcos, G.; Día, J.L.; de la Cámara, C.; Ventura, T.; Morales Asín, F.; Fernando Pascu-al, L.; Montañés, J.A.; Aznar, S. Revalidación y normalización del Mini-Examen Cognoscitivo (primera versión en castellano del Mini-Mental Status Examination) en la población general geriátrica (Re-validation of the Mini-Examen Cognoscitivo (first Spanish version of the Mini-Mental Status Examination) and population-based norms in the elderly community). Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Beck, A.; Steer, R.; Brown, G. Beck Depression Inventory-II. San Antonio 1996, 78, 490–498. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385. [Google Scholar] [CrossRef]
- Hita-Yañez, E.; Atienza, M.; Cantero, J.L. Polysomnographic and Subjective Sleep Markers of Mild Cognitive Impairment. Sleep 2013, 36, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Adler, N.E.; Epel, E.S.; Castellazzo, G.; Ickovics, J.R. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, White women. Health Psychol. 2000, 19, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Stalder, T.; Kirschbaum, C.; Kudielka, B.M.; Adam, E.K.; Pruessner, J.C.; Wüst, S.; Dockray, S.; Smyth, N.; Evans, P.; Hellhammer, D.H.; et al. Assessment of the cortisol awakening response: Expert consensus guidelines. Psychoneuroendocrinology 2016, 63, 414–432. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, V.; Almela, M.; Pulopulos, M.M.; Salvador, A. Memory performance is related to the cortisol awakening response in older people, but not to the diurnal cortisol slope. Psychoneuroendocrinology 2016, 71, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Pulopulos, M.M.; Hidalgo, V.; Almela, M.; Puig-Perez, S.; Villada, C.; Salvador, A. Hair cortisol and cognitive performance in healthy older people. Psychoneuroendocrinology 2014, 44, 100–111. [Google Scholar] [CrossRef]
- Wirtz, P.H.; Känel, R.; Emini, L.; Ruedisueli, K.; Groessbauer, S.; Maercker, A.; Ehlert, U. Evidence for altered hypothalamus–pituitary–adrenal axis functioning in systemic hypertension: Blunted cortisol response to awakening and lower negative feedback sensitivity. Psychoneuroendocrinology 2007, 32, 430–436. [Google Scholar] [CrossRef]
- Pulpulos, M.M.; Hidalgo, V.; Puig-Perez, S.; Salvador, A. Psychophysiological response to social stressors: Relevance of sex and age. Psicothema 2018, 30, 171–176. [Google Scholar]
- Van de Water, A.T.M.; Holmes, A.; Hurley, D.A. Objective measurements of sleep for non-laboratory settings as alternatives to polysomnography—A systematic review. J. Sleep Res. 2011, 20, 183–200. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Carskadon, M.A.; Guilleminault, C.; Vitiello, M.V. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: Developing normative sleep values across the human lifespan. Sleep 2004, 27, 1255–1273. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Mean | SD |
|---|---|---|
| Age (years) | 63.89 | 4.06 |
| SES | 5.62 | 1.27 |
| Physical activity | 1.78 | 0.77 |
| Education | 3.76 | 1.30 |
| PSS | 18.60 | 5.77 |
| BDI | 5.04 | 4.46 |
| Objective sleep time (min) | 333.44 | 57.48 |
| Subjective sleep time (min) | 400.53 | 63.03 |
| Objective sleep quality (Efficiency) | 81.19 | 10.13 |
| Subjective sleep quality | 3.53 | 0.92 |
| Perceived stress day before | 2.05 | 0.92 |
| Stress expected coming day | 2.17 | 0.82 |
| Cortisolchange (nmol/L) | 1.63 | 0.72 |
| Variables | β | p | 95% Confidence Interval | |
|---|---|---|---|---|
| DV: Subjective Sleep Quality | ||||
| Cortisolchange (nmol/L) | 0.263 | 0.029 | [0.028, 0.499] | |
| Objective sleep time (min) | 0.169 | 0.155 | [−0.066, 0.404] | |
| Age (years) | −0.097 | 0.435 | [−0.342, 0.149] | |
| SES | −0.058 | 0.627 | [−0.293, 0.178] | |
| Physical activity | 0.068 | 0.561 | [−0.164, 0.300] | |
| Sex | −0.127 | 0.329 | [−0.386, 0.132] | |
| Perceived stress day before | −0.191 | 0.132 | [−0.441, 0.059] | |
| Stress expected coming day | 0.162 | 0.209 | [−0.093, 0.416] | |
| PSS | 0.122 | 0.337 | [−0.130, 0.375] | |
| BDI | −0.124 | 0.385 | [−0.406, 0.159] | |
| DV: Objective sleep quality | ||||
| Cortisolchange (nmol/L) | 0.029 | 0.728 | [−0.137, 0.195] | |
| Objective sleep time (min) | −0.138 | 0.141 | [−0.323, 0.047] | |
| Age (years) | 0.586 | 0.000 | [0.401, 0.771] | |
| SES | 0.166 | 0.090 | [−0.027, 0.359] | |
| Physical activity | −0.119 | 0.204 | [−0.304, 0.066] | |
| Sex | 0.134 | 0.147 | [−0.048, 0.317] | |
| Perceived stress day before | 0.153 | 0.139 | [−0.051, 0.356] | |
| Stress expected coming day | −0.229 | 0.023 | [−0.426, −0.032] | |
| PSS | 0.200 | 0.050 | [0.000, 0.401] | |
| BDI | −0.078 | 0.433 | [−0.276, 0.120] | |
| Variables | β | p | 95% Confidence Interval | |
|---|---|---|---|---|
| DV: Discrepancy in sleep quality | ||||
| Cortisolchange (nmol/L) | 0.290 | 0.010 | [0.072, 0.507] | |
| Objective sleep time (min) | −0.301 | 0.007 | [−0.518, −0.084] | |
| Age (years) | −0.190 | 0.099 | [−0.416, 0.037] | |
| SES | 0.044 | 0.686 | [−0.173, 0.262] | |
| Physical activity | −0.048 | 0.657 | [−0.263, 0.167] | |
| Sex | −0.202 | 0.097 | [−0.441, 0.037] | |
| Perceived stress day before | 0.027 | 0.814 | [−0.204, 0.258] | |
| Stress expected coming day | −0.028 | 0.814 | [−0.263, 0.207] | |
| PSS | 0.144 | 0.219 | [−0.088, 0.377] | |
| BDI | −0.024 | 0.854 | [−0.285, 0.237] | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pulopulos, M.M.; Hidalgo, V.; Puig-Perez, S.; Montoliu, T.; Salvador, A. Relationship between Cortisol Changes during the Night and Subjective and Objective Sleep Quality in Healthy Older People. Int. J. Environ. Res. Public Health 2020, 17, 1264. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041264
Pulopulos MM, Hidalgo V, Puig-Perez S, Montoliu T, Salvador A. Relationship between Cortisol Changes during the Night and Subjective and Objective Sleep Quality in Healthy Older People. International Journal of Environmental Research and Public Health. 2020; 17(4):1264. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041264
Chicago/Turabian StylePulopulos, Matias M., Vanesa Hidalgo, Sara Puig-Perez, Teresa Montoliu, and Alicia Salvador. 2020. "Relationship between Cortisol Changes during the Night and Subjective and Objective Sleep Quality in Healthy Older People" International Journal of Environmental Research and Public Health 17, no. 4: 1264. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041264