A Scoping Review of the Health of Conflict-Induced Internally Displaced Women in Africa



Abstract
:1. Introduction
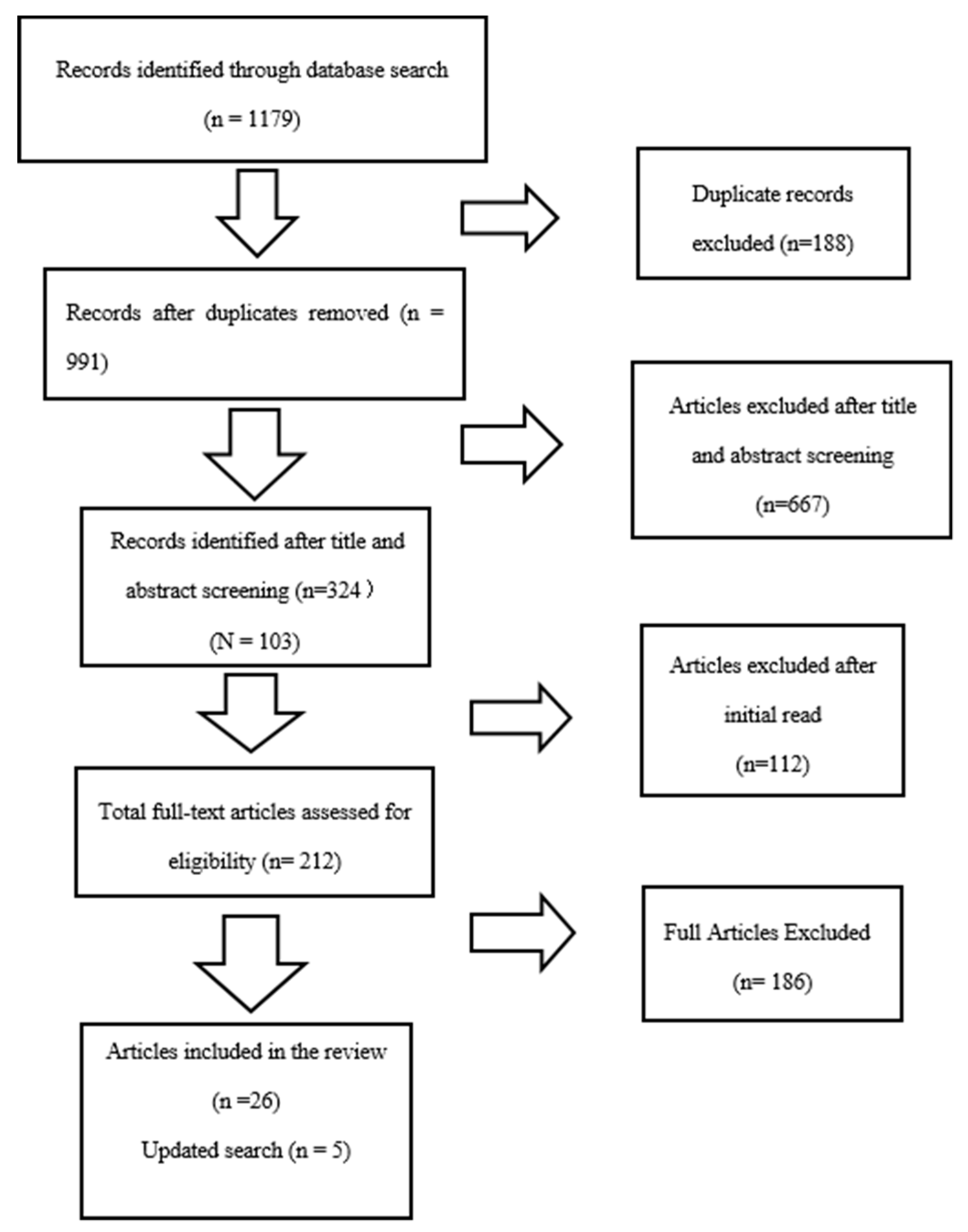
2. Materials and Methods
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)
- A focus on women who migrated outside of their country’s borders, who were displaced by a natural disaster, or who are economic migrants;
- A focus on instrument testing or the piloting of questionnaires;
- Lacking a methodology;
- Merely literature reviews or discussion papers;
- Grey literature, reports, websites, and graduate theses;
- Published in a language other than English.
3. Results
3.1. Violence
3.2. Mental Health
3.3. Sexual and Reproductive Health
3.4. Malaria
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Internal Displacement Monitoring Center. Global Report on Internal Displacement. Available online: http://www.internal-displacement.org/sites/default/files/publications/documents/2019-IDMC-GRID.pdf (accessed on 10 July 2019).
- WHO. Inter-Agency Field Manual on Reproductive Health in Humanitarian Settings. Available online: https://www.who.int/reproductivehealth/publications/emergencies/field_manual/en/ (accessed on 5 August 2010).
- Brookings Institution. Improving the Protection of Internally Displaced Women: Assessing Progress and Challenges. Available online: https://www.brookings.edu/ (accessed on 11 March 2014).
- Mulugeta, A.A. The African Union Convention on internally displaced persons: Its codification background, scope, and enforcement challenges. Refug. Surv. Q. 2010, 29, 28–57. [Google Scholar] [CrossRef]
- WHO Draft Global Action Plan ‘Promoting the health of refugees and migrants’ (2019–2023). Available online: https://www.who.int/migrants/en/ (accessed on 25 January 2020).
- Matlin, S.A.; Depoux, A.; Schütte, S.; Flahault, A.; Saso, L. Migrants’ and Refugees’ Health: Towards an Agenda of Solutions. Public Health Rev. 2018, 39, 27. [Google Scholar] [CrossRef] [Green Version]
- UNHCR. Internally Displaced People. 2020. Available online: https://www.unhcr.org/internally-displaced-people.html (accessed on 22 January 2020).
- UNHCR. Global Trends Forced Displacement in 2017. 2017. Available online: https://www.unhcr.org/globaltrends2017/ (accessed on 26 January 2020).
- United Nations. Security Council Considers Boost in UN Peacekeepers Numbers in Central African Republic. UN News. Available online: https://goo.gl/mXYo8x (accessed on 6 November 2017).
- United Nations. Central African Republic: UN Mission Mandate Extended, Additional ‘Blue Helmets’ Authorized. UN News. Available online: https://goo.gl/oh9MJA (accessed on 15 November 2017).
- United Nations. ‘Leave No Stone Unturned’ to Secure Aid Funding for Central African Republic, Senior UN Official Urges. UN News. Available online: https://goo.gl/cDQxMP (accessed on 25 January 2020).
- UN News. UN Highlights Need to Solve Growing Burden of Forcibly Displaced Africans. 2019. Available online: https://news.un.org/en/story/2019/05/1038911 (accessed on 24 January 2020).
- UNFPA. Five Reasons Migration Is a Feminist Issue. 2018. Available online: https://www.unfpa.org/news/five-reasons-migration-feminist-issue (accessed on 21 January 2020).
- UNHCR. Women. 2020. Available online: https://www.unhcr.org/women.html (accessed on 18 January 2020).
- IOM. International Women’s Day 2014 Women Migrants Must Not Be Left Behind. 2014. Available online: https://www.iom.int/ (accessed on 19 January 2020).
- Jesuthasan, J.; Witte, Z.; Oertelt-Prigione, S. Health-related needs and barriers for forcibly displaced women: A systematic review. Gender Genome 2019, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Oloka-Onyango, J. The plight of the larger half: Human rights, gender violence and the legal status of refugee and internally displaced women in Africa. Denv. J. Int. L. Pol. 1995, 24, 349. [Google Scholar]
- Olu, O.; Usman, A.; Woldetsadik, S.; Chamla, D.; Walker, O. Lessons learnt from coordinating emergency health response during humanitarian crises: A case study of implementation of the health cluster in northern Uganda. Conflict Health 2015, 9, 1. [Google Scholar] [CrossRef] [Green Version]
- WHO. Displaced or Refugee Women Are at Increased Risk of Violence. What Can WHO Do? 2018. Available online: https://www.who.int/reproductivehealth/displaced-refugee-women-violence-risk/en/ (accessed on 18 January 2020).
- UN Report of the Secretary-General on Conflict-Related Sexual Violence. Available online: https://www.un.org/en/events/elimination-of-sexual-violence-in-conflict/pdf/1494280398.pdf (accessed on 19 January 2020).
- Yacob-Haliso, O. Intersectionality and Durable Solutions for Refugee Women in Africa. J. Peacebuilding Dev. 2016, 11, 53–67. [Google Scholar] [CrossRef]
- UN. Sustainable Development Goals International Organization for Migration (IOM). 2020. Available online: https://sustainabledevelopment.un.org/index.php?page=view&type=30022&nr=869&menu=3170 (accessed on 19 January 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA group preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 151, 264–269. [Google Scholar]
- Ager, A.; Bancroft, C.; Berger, E.; Stark, L. Local constructions of gender-based violence amongst IDPs in northern Uganda: Analysis of archival data collected using a gender-and age-segmented participatory ranking methodology. Conflict Health 2018, 12, 10. [Google Scholar] [CrossRef] [Green Version]
- Stark, L.; Roberts, L.; Wheaton, W.; Acham, A.; Boothby, N.; Ager, A. Measuring violence against women amidst war and displacement in northern Uganda using the “neighbourhood method”. J. Epidemiol. Community Health 2010, 64, 1056–1061. [Google Scholar] [CrossRef]
- Stark, L.; Sommer, M.; Davis, K.; Asghar, K.; Baysa, A.A.; Abdela, G.; Tanner, S.; Falb, K. Disclosure bias for group versus individual reporting of violence amongst conflict-affected adolescent girls in DRC and Ethiopia. PLoS ONE 2017, 12, e0174741. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, L.; Gupta, J.F.; Shuman, S.; Cole, H.; Kpebo, D.; Falb, K.L. What factors contribute to intimate partner violence against women in urban, conflict-affected settings? Qualitative findings from Abidjan, Cote d’Ivoire. J. Urban Health 2016, 93, 364–378. [Google Scholar]
- Aham-Chiabuotu, C.B.; Abel, G.; Thompson, L. ‘Men don’t have patience’: Sexuality, pleasure and danger in displacement settings in Northcentral Nigeria. Global Public Health 2019, 20, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Logie, C.H.; Okumu, M.; Mwima, S.; Hakiza, R.; Irungi, K.P.; Kyambadde, P.; Kironde, E.; Narasimhan, M. Social ecological factors associated with experiencing violence among urban refugee and displaced adolescent girls and young women in informal settlements in Kampala, Uganda: A cross-sectional study. Conflict Health 2019, 13, 60. [Google Scholar] [CrossRef] [PubMed]
- Oladeji, O.; Oladeji, B.; Chamla, D.; Safiyanu, G.; Mele, S.; Mshelia, H.; Agbor, J. Sexual violence–related pregnancy among internally displaced women in an internally displaced persons camp in northeast Nigeria. J. Interpers. Violence 2018. [Google Scholar] [CrossRef]
- Almedom, A.; Tesfamichael, B.; Mohammed, Z.; Mascie-Taylor, N.; Muller, J.; Alemu, Z. Prolonged displacement may compromise resilience in Eritrean mothers. Afr. Health Sci. 2005, 5, 310–314. [Google Scholar]
- Almedom, A.M.; Tesfamichael, B.; Mohammed, Z.S.; Mascie-Taylor, C.G.N.; Alemu, Z. Use of ‘Sense of Coherence (SOC)’ scale to measure resilience in Eritrea: Interrogating both the data and the scale. J. Biosoc. Sci. 2007, 39, 91–107. [Google Scholar] [CrossRef]
- Hamid, A.A.; Musa, S.A. Mental health problems among internally displaced persons in Darfur. Int. J. Psychol. 2010, 45, 278–285. [Google Scholar] [CrossRef]
- Kinyanda, E.; Musisi, S.; Biryabarema, C.; Ezati, I.; Oboke, H.; Ojiambo-Ochieng, R.; Were-Oguttu, J.; Levin, J.; Walugembe, J. War-related sexual violence and its medical and psychological consequences as seen in Kitgum, Northern Uganda: A cross-sectional study. BMC Int. Health Hum. Rights 2010, 10, 28. [Google Scholar] [CrossRef] [Green Version]
- Olanrewaju, F.O.; Omotoso, F.; Alabi, J.O. Datasets on the challenges of forced displacement and coping strategies among displaced women in selected internally displaced persons ׳(IDPs) camps in Nigeria. Data Brief 2018, 1, 152–158. [Google Scholar] [CrossRef]
- Corbin, J.N.; Hall, J.C. Resettlement post conflict: Risk and protective factors and resilience among women in northern Uganda. Int. Soc. Work 2019, 62, 918–932. [Google Scholar] [CrossRef]
- Kim, G.; Torbay, R.; Lawry, L. Basic health, women’s health, and mental health among internally displaced persons in Nyala Province, South Darfur, Sudan. Am. J. Public Health 2007, 97, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Kizza, D.; Hjelmeland, H.; Kinyanda, E.; Knizek, B.L. Alcohol and suicide in post-conflict northern Uganda. Crisis Hogrefe Publ. 2012, 33, 95–105. [Google Scholar]
- Kizza, D.; Knizek, B.L.; Kinyanda, E.; Hjelmeland, H. Men in despair: A qualitative psychological autopsy study of suicide in Northern Uganda. Transcult. Psychiatry 2012, 49, 696–717. [Google Scholar] [CrossRef] [PubMed]
- Roberts, B.; Ocaka, K.F.; Browne, J.; Oyok, T.; Sondorp, E. Factors associated with post-traumatic stress disorder and depression amongst internally displaced persons in northern Uganda. BMC Psychiatry 2008, 8, 38. [Google Scholar] [CrossRef] [Green Version]
- Kisindja, R.M.; Kimona, C.; Etoy, M.; Dorme, F.; Benfield, N. Family planning knowledge and use among women in camps for internally displaced people in the Democratic Republic of the Congo. Int. J. Gyn. Obs. 2017, 138, 256–260. [Google Scholar] [CrossRef]
- Ali, A.A.A.; Okud, A. Factors affecting unmet need for family planning in Eastern Sudan. BMC Public Health 2013, 13, 102. [Google Scholar] [CrossRef] [Green Version]
- Decker, M.; Constantine, N.A. Factors associated with contraceptive use in Angola. Afr. J. Reprod. Health 2011, 15, 68–77. [Google Scholar]
- McGinn, T.; Austin, J.; Anfinson, K.; Amsalu, R.; Casey, S.E.; Fadulalmula, S.I.; Langston, A.; Lee-Jones, L.; Meyers, J.; Mubiru, F.K.; et al. Family planning in conflict: Results of cross-sectional baseline surveys in three African countries. Conflict Health 2011, 5, 11. [Google Scholar] [CrossRef] [Green Version]
- Orach, C.G.; Musoba, N.; Byamukama, N.; Mutambi, R.; Aporomon, J.F.; Luyombo, A.; Rostedt, A. Perceptions about human rights, sexual and reproductive health services by internally displaced persons in northern Uganda. Afr. Health Sci. 2009, 9, 72–80. [Google Scholar]
- Adam, I.F. The influence of maternal health education on the place of delivery in conflict settings of Darfur, Sudan. Conflict Health 2015, 9, 31. [Google Scholar] [CrossRef] [Green Version]
- Adam, I.F.; Nakamura, K.; Kizuki, M.; Al Rifai, R.; Vanching, U. Relationship between implementing interpersonal communication and mass education campaigns in emergency settings and use of reproductive healthcare services: Evidence from Darfur, Sudan. BMJ Open 2015, 5, e008285. [Google Scholar] [CrossRef] [Green Version]
- Chi, P.C.; Bulage, P.; Urdal, H.; Sundby, J. Perceptions of the effects of armed conflict on maternal and reproductive health services and outcomes in Burundi and Northern Uganda: A qualitative study. BMC Int. Health Hum. Rights 2015, 15, 7. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.A.; Malele, F.; Kaiser, R.; Mama, N.; Kinkela, T.; Mantshumba, J.C.; Hynes, M.; De Jesus, S.; Musema, G.; Kayembe, P.K.; et al. HIV infection among internally displaced women and women residing in river populations along the Congo River, Democratic Republic of Congo. AIDS Behav. 2009, 13, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Obol, J.; David Lagoro, K.; Christopher Garimoi, O. Knowledge and misconceptions about malaria among pregnant women in a post-conflict internally displaced persons’ camps in Gulu District, northern Uganda. Malar. Res. Treat. 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dræbel, T.; Kueil, B.G.; Meyrowitsch, D.W. Prevalence of malaria and use of malaria risk reduction measures among resettled pregnant women in South Sudan. Int. Health 2013, 5, 211–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dræbel, T.; Gueth Kueil, B. Lay perceptions of malaria and therapeutic itinerary of resettled pregnant women in South Sudan. Int. Health 2014, 6, 317–321. [Google Scholar] [CrossRef]
- Obol, J.H.; Ononge, S.; Orach, C.G. Utilisation of insecticide treated nets among pregnant women in Gulu: A post conflict district in northern Uganda. Afr. Health Sci. 2013; 13, 962–969. [Google Scholar]
- Brooks, H.M.; Paul, M.K.J.; Claude, K.M.; Mocanu, V.; Hawkes, M.T. Use and disuse of malaria bed nets in an internally displaced persons’ camp in the Democratic Republic of the Congo: A mixed-methods study. PLoS ONE 2017, 12, e0185290. [Google Scholar] [CrossRef] [Green Version]
- Idemudia, E.S.; William, J.K.; Boehnke, K.; Wyatt, G. Gender differences in trauma and posttraumatic stress symptoms among displaced Zimbabweans in South Africa. J. Trauma. Stress Disord. Treat. 2013, 2, 1340. [Google Scholar] [CrossRef]
- Morina, N.; Akhtar, A.; Barth, J.; Schnyder, U. Psychiatric disorders in refugees and internally displaced persons after forced displacement: A systematic review. Front. Psychiatry 2018, 9, 433. [Google Scholar] [CrossRef]
- Araya, M.; Chotai, J.; Komproe, I.H.; de Jong, J.T. Effect of trauma on quality of life as mediated by mental distress and moderated by coping and social support among post-conflict displaced Ethiopians. Q. Life Res. 2007, 16, 915–927. [Google Scholar] [CrossRef]
- Koegler, E.; Kennedy, C.E. A scoping review of the associations between mental health and factors related to HIV acquisition and disease progression in conflict-affected populations. Conflict Health 2018, 12, 20. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, O.; Rai, M.; Kemigisha, E. A systematic review of sexual and reproductive health knowledge, experiences and access to services among Refugee, migrant and displaced girls and young women in Africa. Int. J. Environ. Res. Public Health 2018, 15, 1583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations. The Sustainable Development Goals Report 2018. Available online: https://unstats.un.org/sdgs/files/report/2018/TheSustainableDevelopmentGoalsReport2018-EN.pdf (accessed on 6 September 2018).


{kind=link}
| Author | Purpose of Study | Design | Country/Setting of Research | Study Results |
|---|---|---|---|---|
| Ager et al. (2018) [24] | To elicit local descriptions of gender-based violence experienced by women in camp | Participatory ranking method | Northern Uganda |
|
| Stark et al. (2010) [25] | To establish incidence rates for gender-based violence in IDP camps in northern Uganda. | Interviews: a neighborhood methodology | Northern Uganda |
|
| Stark et al. (2017) [26] | To identify discrepancies in the conceptualization and reporting on inter- personal violence in humanitarian settings. | Mixed method | DRC and Sudan |
|
| Cardoso et al. (2016) [27] | To understand the factors in the urban environment contributing to intimate partner violence experiences of women | Focus group | Cote d’Ivoire |
|
| Aham-Chaibuotu et al. (2019) [28] | To examine the influence of conflict and displacement on gender relations, sexuality, and natality of internally displaced women in Nigeria | Focus group discussions and in-depth interviews | Northern Nigeria |
|
| Logie et al. (2019) [29] | To explore factors associated with intimate partner violence and young adulthood violence among forcibly displaced young women | Cross-sectional survey | Kampala, Uganda |
|
| Oladeji et al. (2018) [30] | To report the disclosure and outcomes of sexual violence-related pregnancies (SVRP) among rescued female victims of Boko Haram insurgencies | Clinic records review | Borno state, Nigeria |
|
| Almedom et al. (2005) [31] | To assess the impact of prolonged displacement on the resilience of Eritrean mothers | Mixed methods | Eritrea |
|
| Almedom et al. (2007) [32] | To identify the determinants of sense of coherence (resilience) in displaced Eritrean persons | Quantitative questionnaire approach: Sense of Coherence scale assessment | Eritrea: Northeast Africa |
|
| Hamid et al. (2010) [33] | To investigate the effects of the Darfur crisis on the mental health of internally displaced women | Mixed methods | Darfur, Sudan |
|
| Kinyanda et al. (2010) [34] | To examine the long-term health consequences of war-related sexual violence among rural women living in camps | Purposive cross-sectional study design: structured interview | Northern Uganda |
|
| Olanrewaju et al. (2018) [35] | To explain the challenges of displacement and the coping startegies of internally diaplaced women in Nigeria | Qualitative approach with a descriptive survey | Yola and Abuja, northern Nigeria |
|
| Corbin et al. (2018) [36] | To explore resilience among internally displaced women in norther Uganda | Qualitative study | Nwoya and Gulu district, northern Uganda |
|
| Kim et al. (2007) [37] | To assess basic health, women’s health, and mental health among Sudanese IDPs in South Darfur | Questionnaire survey | Nyala Province, South Darfur, Sudan |
|
| Kizza et al. (2012) [38] | To examine the role of alcohol in suicides | Qualitative psychological autopsy method | Northern Uganda |
|
| Kizza et al. (2012) [39] | To investigate suicide among women in a post-conflict context | Qualitative psychological autopsy interviews | Northern Uganda |
|
| Roberts et al. (2009) [40] | To measure the rates of post-traumatic stress disorder (PTSD) and depression among IDPs, and investigate associated demographic and trauma-exposure risk factors | Cross-sectional survey | Northern Uganda |
|
| Kisindja et al. (2017) [41] | To describe family planning awareness and needs among internally displaced women | Cross-sectional survey | DRC |
|
| Ali et al. (2013) [42] | To investigate the unmet need for family planning and associated factors, and total demand for family planning | Community-based cross-sectional household survey | Eastern Sudan |
|
| Decker et al. (2011) [43] | To assess the factors that influence the use of contraception among women in post-war Angola | Semi-structured interviews | Angola |
|
| McGinn et al. (2011) [44] | To document and disseminate data on family planning knowledge, attitudes, and practices among displaced women | Population-based household surveys and health facility assessments | Sudan, Uganda, and the DRC |
|
| Orach et al. (2009) [45] | To explore female and male IDPs’ perceptions of their access to information about rights, access to health services, and experiences of gender-based violence | Cross-sectional study | Northern Uganda |
|
| Adam (2015) [46] | To determine the association between the place of delivery for maternal health education and home visits, and women’s socio-demographic characteristics | Cross-sectional study | Darfur-Sudan |
|
| Adam et al. (2015) [47] | To examine women’s awareness and use of reproductive health care services in emergency settings | Cross-sectional surveys | Darfur-Sudan |
|
| Chi et al. (2015) [48] | To explore perceptions of the effects of armed conflict on maternal and reproductive health services (MRH) and outcomes | Descriptive qualitative study | Burundi and northern Uganda |
|
| Kim et al. (2009) [49] | To analyze HIV, STI, and sexual risk as part of a larger reproductive health assessment of females in IDP camps | Two-stage random sample household survey | DRC |
|
| Obol et al. (2011) [50] | To assess the level of knowledge and misconception about malaria among pregnant women in post-conflict IDP camps | Cross-sectional study using a semi-structured questionnaire | Northern Uganda |
|
| Dræbel et al. (2013) [51] | To assess aspects of malaria infection, prevention, and treatment in a population of resettled pregnant women. | Cross-sectional study | South Sudan |
|
| Draebel et al. (2014) [52] | To explore lay perceptions of malaria and therapeutic process among 30 resettled pregnant women | Semi-structured interviews | South Sudan |
|
| Obol et al. (2013) [53] | To establish the prevalence and factors associated with insecticide-treated net (ITN) use among pregnant women in IDP camps | Cross-sectional study | Northern Uganda |
|
| Brooks et al. (2017) [54] | To explore the factors influencing bednet ownership and use in an IDP camp with free bednet distribution | Mixed methods | Eastern Democratic Republic of Congo (DRC) |
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amodu, O.C.; Richter, M.S.; Salami, B.O. A Scoping Review of the Health of Conflict-Induced Internally Displaced Women in Africa. Int. J. Environ. Res. Public Health 2020, 17, 1280. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041280
Amodu OC, Richter MS, Salami BO. A Scoping Review of the Health of Conflict-Induced Internally Displaced Women in Africa. International Journal of Environmental Research and Public Health. 2020; 17(4):1280. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041280
Chicago/Turabian StyleAmodu, Oluwakemi C., Magdalena S. Richter, and Bukola O. Salami. 2020. "A Scoping Review of the Health of Conflict-Induced Internally Displaced Women in Africa" International Journal of Environmental Research and Public Health 17, no. 4: 1280. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041280