Migration, Stress and the Challenges of Accessing Food: An Exploratory Study of the Experience of Recent Afghan Women Refugees in Adelaide, Australia

 , , and
, , and 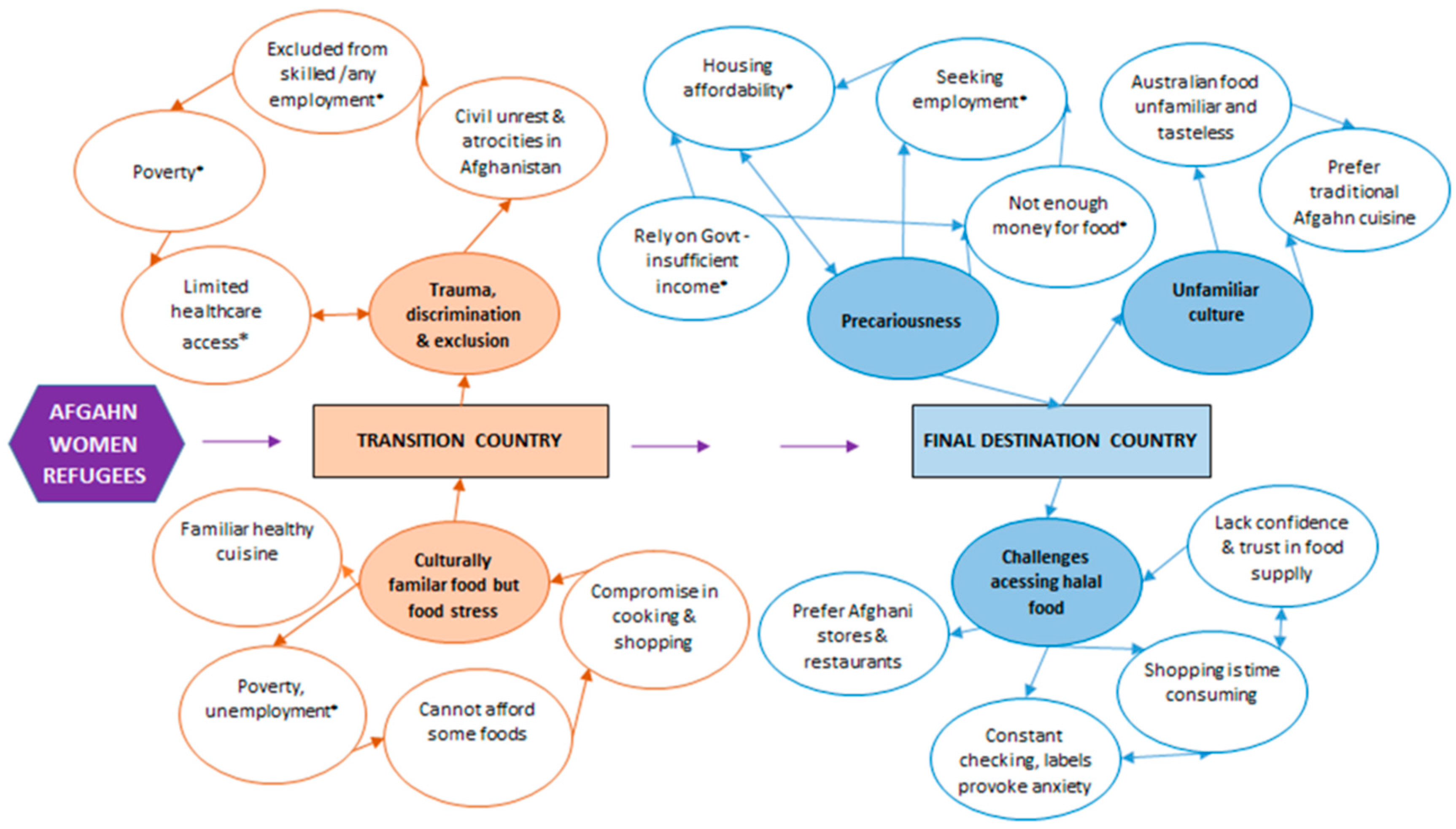{kind=link}
Abstract
:1. Introduction
2. Study Design
2.1. Recruitment
2.2. Data Collection
2.3. Ethics Approval
2.4. Data Analysis
3. Results
3.1. Trauma, Discrimination and Exclusion (in the Transition Country)
P5: We lived in rural area in Kabul and I was only able to do my education up to primary since I did not have any facilities with transportation to the school … Kabul was very unsafe place and always a war zone.
P7: … Our community get attacked by Pakistani people. I remember when I was 13 and we lived in a rural area and there was a blast and many people from my community got killed …
P4: Yeah, we lived in one of the dangerous areas of Pakistan which has been targeted for 15 years by the Taliban. We had a blast next to our land and it killed more than a hundred people at time. We had seen a lot of body parts and everything just came into our house. It was that close. So that why we thought that, no, we cannot live here anymore now, and we cannot go back to Afghanistan as well because the situation there is even worse, so we decided to move to Australia.
P8: The only employment was being a cheap labourer. Even with a university degree, employers were hesitant to employ us because of the high likelihood of being deported to Afghanistan if the rules changed.
P10: Because we were Afghani, we had less right than local people and for example for getting admission for schools there was heaps of bureaucracy work between different department … there was a big discrimination for you as an Afghani refugee. It was really hard to have any hope for your future. In schools there was a lot of discrimination and they did not want us to progress.
P10: In Iran we studied in a public school for a while then they had a rule and removed us from public school, and we had to go to private schooling which was very expensive.
P7: We did not have access to health services in our place and we had to travel to the next town and they would charge us more than the locals and we could not afford that.
3.2. Familiar Food Culture, but Food Stress (in the Transition Country)
P3: There was not much difference between Afghani and Iranian cuisine so my parents were able to adapt very easily.
P8: Food in Iran was healthy and had good quality. It was very similar to our own traditional foods.
P10: Food in Iran was really good since it was a halal food but the only problem was its price which was not affordable for families like us. Sometimes my dad did not get his salary on-time and my mother had to make a lot of compromises to her cooking ingredients. We could not afford red meat specially most of the times.
P4: We didn’t eat meat that much because meat was too expensive for us [in Pakistan]. Even the people used to say that lentil is the cheapest food that anyone can afford, but even the price of lentil have become so high that it was above the pay of a person … So, we never could not afford it.
3.3. Precariousness (in Australia)
P10: Finding an employment for us is also challenging considering we do not have local experiences and fluency in English.
P4: Still I don’t have a job. I am talking to the job seeker to try and get me a part time job, but because of my studies they are getting so much tougher and it is fulltime, so it was not possible and the job offering me was to do work in a pork factory, so we are not comfortable with it.
P4: I want to support my family. Now we are living in a rent house, so we need to buy house, that’s why I need to have a job for that.
P2: My husband and I could not survive on Centrelink money without the support of my father-in law and could not afford to rent a place to live.
P4: Over here most problems I have faced was driving. It was too difficult for me to get a driving license because we have to pay a lot for every license that we have to get. The driving test we must pay is too much, because I failed my first driving test, it was $250.
P1: In Australia we have difficulty finding a place to rent for several reasons. First, we are a big family and second, our family relies on Centrelink payment and landlords are not trusting us that we can afford their rent.
P10: In Iran if we can afford cheese or butter for our breakfast we felt that we eating like a rich people but in here we can afford to eat variety of things for example egg, jam, milk, walnut, honey all in one meal which is amazing.
P6: I live with my cousin and rely on government money to live. I can afford food shopping, but I cannot afford other shopping like clothes etc.
P1: Now that we are not living in governmental house, the rent and bills is taking up most of money and we need to watch how we spend leftover money on food and we will buy food in bulk to save some money or we will only shop at cheap markets such as Sunday market.
P7: Support for refugees to find good quality cheap food is really important as they might pay for their house, bills and education and or as an elder son they are supporting the whole family, this will leave small budget for the food.
P7: In Pakistan if we run out of a food, we will ask our neighbours because neighbours there are in relationship but here in Australia this is not possible. Here I made a lot of friends and I will ask them if I need.
3.4. An Unfamiliar Food Culture (in Australia)
P5: When I came to Australia two years ago, food was tasteless, and I even do not like the taste of water here but later on I got used to it.
P2: Chicken here is tasteless, and I don’t like that taste of dairy and egg either here and I would not eat them.
P10: I have not tasted Australian food … but my sister once has tried Sushi and she could not eat it as its odour is like a raw fish which is not pleasant for us. I do not know why this food is so popular here.
P9: We eat traditional food here in Australia. I think Australian foods are healthier, but I would prefer our own food as it is tastier.
P7: I do not know what the Australian food means, and I will eat traditional food most of times …
3.5. Challenges in Accessing Halal Food (in Australia)
P3: One of my biggest concern over coming to Australia was that I brought up in a very religious Muslim family and I am very strict about halal food and I had a big stress that how I am going to maintain it here in Australia.
P4: Even in the vegetables, they say ham flavour, so we have to check everything.
P10: We were lucky to live in a suburb (Prospect) close to Afghani shops and bakeries which have halal foods, but I have friends that they have to travel a long way from Salisbury or Elizabeth to come to shop at these places.
P9: In Australia we need to buy food that we can eat that is why we would only shop from Iranian or Afghani shops. We will eat out once a week only at Afghani restaurants.
P10: My friends from Afghanistan mainly and I have an App that you can upload your food and you can get ideas about which food you can make for your next meal.
P3: I always worry when I do not shop from Afghani supermarkets and I will check all the ingredients specially for gelatine and alcohol. I still cannot trust foods here that they are halal. I have heard that if they have a code it means that it is not halal.
P7: Whenever I go to a restaurant for example Chinese restaurant, I am not comfortable and if I ask about halal food, normally they have no idea and they will get really confused.
P1: We cannot eat in most restaurants as their food contains alcohol but in Iran, we had peace of mind when we shop or we eat outside.
4. Discussion
4.1. The Transition Country Experience
4.2. The Australian Experience
4.3. Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Australian Refugee Council. UNHCR Global Trends 2017—How Australia Compares with the World. 2018. Available online: https://www.refugeecouncil.org.au/global-trends-2017/ (accessed on 11 March 2019).
- United Nations High Commission for Refugees. Figures at a Glance. 2019. Available online: https://www.unhcr.org/en-au/figures-at-a-glance.html (accessed on 11 March 2019).
- United Nations High Commission for Refugees. UNHRC Statistics: The World Numbers 2017. 2019. Available online: http://popstats.unhcr.org/en/overview#_ga=2.62464292.908401948.1552272050-2146327032.1552272050 (accessed on 11 March 2019).
- Australian Government: Department of Immigration and Citizenship. Community Information Summary-Afghanistan-Born. 2014. Available online: https://www.dss.gov.au/sites/default/files/documents/02_2014/afghanistan.pdf (accessed on 11 March 2019).
- Australian Bureau of Statistics. Understanding Migrant Outcomes—Insights from the Australian Census and Migrants Integrated Dataset, Australia, 2016. 2018. Available online: https://www.abs.gov.au/ausstats/[email protected]/PrimaryMainFeatures/3417.0?OpenDocument (accessed on 18 July 2018).
- Koser, K.; Marsden, P. Migration and Displacement Impacts of Afghan Transitions in 2014: Implications for Australia; Migration Research Program Occasional Paper Series 03; Australian Capital Territory: Canberra, Australia; Department of Immigration and Border Protection: Belconnen, Australia, 2013. [Google Scholar]
- Southern Migrant and Refugee Centre. Afghani Community Profile—Older People. 2015. Available online: https://smrc.org.au/wp-content/uploads/2018/06/cultural-profile-for-afghani-seniors.pdf (accessed on 30 October 2019).
- UNHCR. Global Trends: Forced Displacement in 2016; UNHCR: Geneva, Switzerland, 2017.
- Australian Human Rights Commission. Questions and Answers about Australian Refugees and Asylum Seekers. 2019. Available online: www.humanrights.gov.au/publications/questions-and-answers-abuot-refugees-asylum-seekers#q9 (accessed on 29 October 2019).
- Australian Bureau of Statistics. Personal Income of Migrants, Australia 2013–2014. 2017. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3418.02013-14?OpenDocument (accessed on 4 November 2019).
- Hadgekiss, E.; Renzaho, A. The physical health status, service utilization and barriers to access care for asylum seekers residing in the community: A systematic review of the literature. Aust. Health Rev. 2014, 38, 142–159. [Google Scholar] [CrossRef]
- Popovic-Lipovac, A.; Strasser, B. A review on the changes in food habits among immigrant women and implications for health. J. Immigr. Minor. Health 2013, 17, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Hall, J. Food and dietary requirements for international students. J. Int. Educ. 1995, 6, 53–60. [Google Scholar]
- Satia-Abouta, J. Dietary Acculturation: Definition, process, assessmetn and implications. Int. J. Hum. Ecol. 2003, 4, 71–86. [Google Scholar]
- Thomson, L.; McFeeter, J. What’s for Dinner? An Exploration of Changes in Eating Habits and Dietary Acculturation among Migrants New to Australia; AMES Australia: Melbourne, Australia, 2019. [Google Scholar]
- Dovey, M.T.; Staples, P.A.; Gibson, E.E.; Halford, J.C.G. Food neophobia and picky/fussy eating in children: A review. Appetite 2008, 50, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Burns, C. Effect of migration on food habits of Somali women living as refugees in Australia. Ecol. Food Nutr. 2004, 2, 213–229. [Google Scholar] [CrossRef]
- Rabinowska, M. The ritualisation of food, home and national identity among Polish migrants in London. Soc. Identities 2010, 16, 377–398. [Google Scholar] [CrossRef] [Green Version]
- Southcomb, F. Feeding the Family in an Unfamiliar Environment: Food Security among Recently Resettled Refugees; New South Wales Refugee Service: Newtown, Australia, 2019. [Google Scholar]
- Bradby, H.; Humphries, R.; Newall, D.; Phillimore, J. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Refugees and Asylum Seekers in the European Region; Health Evidence Networks Synthesis Report 44; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Campbell, K.D.; Mann, K.D.; Moffatt, S.; Dave, M.S.; Pearce, S. Social determinants of emotional well-being in new refugees in the UK. Public Health 2018, 164, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Gallegos, D.; Ellies, P.; Wright, J. Still there’s no food! Food insecurity in a refugee population in Perth, Western Australia. Nutr. Diet. 2008, 65, 78–83. [Google Scholar] [CrossRef]
- McKay, F.; Dunn, M. Food security among asylum seekers in Melbourne. Aust. N. Z. J. Public Health 2015, 39, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Kocturk, T. Food habit changes in a group of immigrant women in Uppsala. Women Health Urban Life 2004, 3, 48–61. [Google Scholar]
- Wilkinson, R.; Marmot, M. Social Determinants of Health—The Solid Facts; World Health Organisation: Copenhagen, Denmark, 2003. [Google Scholar]
- Taylor, J.; Lamaro-Haintz, G. Influence of the social determinants of health on access to healthcare services among refugees in Australia. Aust. J. Prim. Health 2017, 24, 14–28. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.A.; Basten, A.; Frattini, C. Migration: A Social Determinant of the Health of Migrants—Background Paper. 2006. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.462.6286&rep=rep1&type=pdf (accessed on 29 October 2019).
- Sarantakos, S. Varieties of Social Research; Social Research: London, UK; Palgrave: London, UK, 1998. [Google Scholar]
- Liamputtong, P. Qualitative Research Methods; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Greig, A.; Taylor, M.; MacKay, T. Doing Research with Children; Sage: London, UK, 2007. [Google Scholar]
- Tami, S.; Reed, D.; Boylan, M.; Zvonkovic, A. Assessment of the effect of acculturation on dietary and physical activity behaviors of Arab mothers in Lubbock, Texas. Ethn. Dis. 2012, 22, 192–197. [Google Scholar] [PubMed]
- Ayoob, M.; Singh, T.; Jan, M. Length of stay, acculturative stress and health among Kashmiri students in Central India. Pak. J. Soc. Clin. Psychol. 2011, 9, 11–15. [Google Scholar]
- Khakpour, M.; Sadeghi, L.; Jenzer, H.; Martins, S.; Farag, M.; Koc, M.; Garcea, J.; Henry, C.; Engler-Stringer, R.; Vatanparast, H. The impact of soci-economic and cultural factors on refugee households’ food insecurity: A snapshot of the food security status of Afghan refugees in Switzerland. FASEB J. 2017, 31 (Suppl. 1), 791–813. [Google Scholar]
- Sadler, G.; Lee, H.; Seung-Hwan, R.L.; Fullerton, J. Recruitment of hard to reach population subgroups via adapatations of the snowball sampling strategy. Nurs. Health Sci. 2010, 12, 369–374. [Google Scholar] [CrossRef] [Green Version]
- Temple, B. Being bilingual: Issues for cross-language research. J. Res. Pract. 2006, 2, M2. [Google Scholar]
- Derrida, J.; Venuti, L. What is a relevant translation? Crit. Inq. 2001, 27, 174–200. [Google Scholar] [CrossRef]
- Guest, G.; Bruce, A.; Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Stud. 2006, 18, 59–82. [Google Scholar]
- Glaser, B.; Strauss, A. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine Publishing Company: New York, NY, USA, 1967. [Google Scholar]
- Strauss, A.; Corbin, J. Basics of Qualitative Grounded Research: Grounded Theory Procedures and Techniques; Sage: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- Strauss, A.L.; Corbin, J. Open Coding. Social Research Methods: A Reader; Seale, C., Ed.; Routledge: London, UK, 2004. [Google Scholar]
- Charmaz, K. Constructing Grounded Theory a Practical Guide Through Qualitative Analysis; Sage: Los Angeles, CA, USA, 2006. [Google Scholar]
- Pascoe, A.E.; Richman, L.S. Perceived discrimination and health: A meta-analytic review. Psychol. Bull. 2009, 135, 531–554. [Google Scholar] [CrossRef] [Green Version]
- WHO. Social Determinants of Health. 2018. Available online: http://www.who.int/topics/social_determinants/en (accessed on 22 July 2019).
- Kessler, R.C.; Mickelson, K.D.; Williams, D.R. The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. J. Health Soc. Behav. 1999, 40, 208–230. [Google Scholar] [CrossRef] [PubMed]
- Borrell, L.N.; Kiefe, C.I.; Williams, D.R.; Diez-Roux, A.V.; Gordon-Larsen, P. Self-reported health, perceived racial discrimination, and skin color in African Americans in the CARDIA study. Soc. Sci. Med. 2006, 63, 1415–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsen, S.; Nazroo, J.Y. Relation between racial discrimination, social class and health among ethnic minority groups. Am. J. Public Health 2002, 92, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.M.; Dhalimi, A.; Lumley, M.; Jamil, H.; Pole, N.; Arnetz, J.E.; Arnetz, B.B. Unemployment in Iraqi refugees: The interaction of pre and post-displacement trauma. Scand. J. Psychol. 2016, 57, 564–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibney, K.B.; Mihrshahi, S.; Torresi, J.; Marshall, C.; Leder, K.; Briggs, B.A. The profile of health problems in African immigrants attending an infectious disease unit in Melbourne, Australia. Am. J. Trop. Med. Hyg. 2009, 80, 805–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paxton, G.A.; Sangster, K.J.; Maxwell, E.L.; McBride, C.R.; Drewe, R.H. Post-arrival health screening in Karen refugees in Australia. PLoS ONE 2012, 7, e38194. [Google Scholar] [CrossRef]
- Sheikh, M.; Pal, A.; Wang, S.; MacIntyre, C.R.; Wood, N.J.; Isaacs, D.; Howell, A. The epidemiology of health conditions of newly arrived refugee children: A review of patients attending a specialist health clinic in Sydney. J. Pediatr. Child Health 2009, 45, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Ngo, C.; Maidment, C.; Atkins, L.; Eagar, S.; Smith, M.M. Blood screen findings in a 2 year cohort of newly arrived refugees to Sydney, Australia. Public Health Res. Pract. 2018, 28, e2811804. [Google Scholar] [CrossRef] [Green Version]
- Ward, P.R.; Verity, F.; Carter, P.; Tsourtos, G.; Coveney, J.; Wong, K.C. Food Stress in Adelaide: The relationship between low income and the affordability of healthy food. J. Environ. Public Health 2013, 2013, 968078. [Google Scholar] [CrossRef]
- Gallegos, D. Healthy Eating: A Right for All Australians; Diversit-e Health e-Magazine: Paramatta, NSW, Australia, 2010; Volume 3. [Google Scholar]
- Temple, J.; Booth, S.; Pollard, C.M. Social Assistance payments and food insecurity in Australia: Evidence from the Household Expenditure Survey. Int. J. Environ. Res. Public Health 2019, 16, 455. [Google Scholar] [CrossRef] [Green Version]
- Ziersch, A.; Walsh, M.; Due, C.; Dulvesteyn, E. Exploring the relationship between housing and health for refugees and asylum seekers in South Australia: A qualitative study. Int. J. Environ. Res. Public Health 2017, 14, 1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raphael, D. Social determinants of health: Present status, unanswered questions, and future directions’. Int. J. Health Serv. 2006, 36, 651–677. [Google Scholar] [CrossRef] [PubMed]
- Den Hartog, A.P. Nutrition and migration: Adaptation of food habits and its implications. Ernhrungs Umsch. 1995, 42, 61–66. [Google Scholar]
- Nath, J.; Henderson, J.; Coveney, J.; Ward, P.R. Consumer faith. Food Cult. Soc. 2013, 16, 421–436. [Google Scholar] [CrossRef]
- Mumuni, A.G.; Veeck, A.; Luqmani, M.; Quraeshi, Z.A. Religious identity, community and religious minorities’ search efforts for religiously sanctioned food: The case of halal food in non-Muslim majority markets. Int. J. Consum. Stud. 2018, 42, 586–598. [Google Scholar] [CrossRef]
- Ahmed, A. Marketing of halal meat in the United Kingdom: Supermarkets versus local shops. Br. Food J. 2008, 110, 655–670. [Google Scholar] [CrossRef]
- Bonne, K.; Verbeke, W. Muslim consumer trust in halal meat status and control in Belgium. Meat Sci. 2008, 79, 113–123. [Google Scholar] [CrossRef]
- Yahaya, C.K.H.C.K.; Kassim, M.; Bin Mazlan, M.H.; Bakar, Z.A. A framework on halal product recognition system through smartphone authentication. In Advances in Automation and Robotics, Lecture Notes in Electrical Engineering; Lee, G., Ed.; Springer: Berlin/Heidelberg, Germany, 2011; Volume 1. [Google Scholar]
- Special Broadcasting Service. New Halal Phone App is Helping Aussie Muslims Dine Out. 2019. Available online: https://www.sbs.com.au/yourlanguage/arabic/en/audiotrack/new-halal-phone-app-helping-aussie-muslims-dine-out (accessed on 8 May 2019).
- Vasileiou, K.; Barrett, J.; Thorpe, S.; Young, T. Characterising and justifying sample size sufficiency in interview-based studies: Systematic analysis of qualitative health research over a 15 year period. BMC Med Res. Methodol. 2018, 18, 148. [Google Scholar] [CrossRef] [Green Version]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kavian, F.; Mehta, K.; Willis, E.; Mwanri, L.; Ward, P.; Booth, S. Migration, Stress and the Challenges of Accessing Food: An Exploratory Study of the Experience of Recent Afghan Women Refugees in Adelaide, Australia. Int. J. Environ. Res. Public Health 2020, 17, 1379. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041379
Kavian F, Mehta K, Willis E, Mwanri L, Ward P, Booth S. Migration, Stress and the Challenges of Accessing Food: An Exploratory Study of the Experience of Recent Afghan Women Refugees in Adelaide, Australia. International Journal of Environmental Research and Public Health. 2020; 17(4):1379. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041379
Chicago/Turabian StyleKavian, Foorough, Kaye Mehta, Eileen Willis, Lillian Mwanri, Paul Ward, and Sue Booth. 2020. "Migration, Stress and the Challenges of Accessing Food: An Exploratory Study of the Experience of Recent Afghan Women Refugees in Adelaide, Australia" International Journal of Environmental Research and Public Health 17, no. 4: 1379. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041379