The Impact of Population Aging and Public Health Support on EU Labor Markets




Abstract
:1. Introduction
2. Theoretical Framework
2.1. Health and Aging
2.2. Health, Aging, and Welfare/Labor Market
2.3. Implications of the “Digital Era”
2.4. Policies and Strategies
3. Data and Methodology
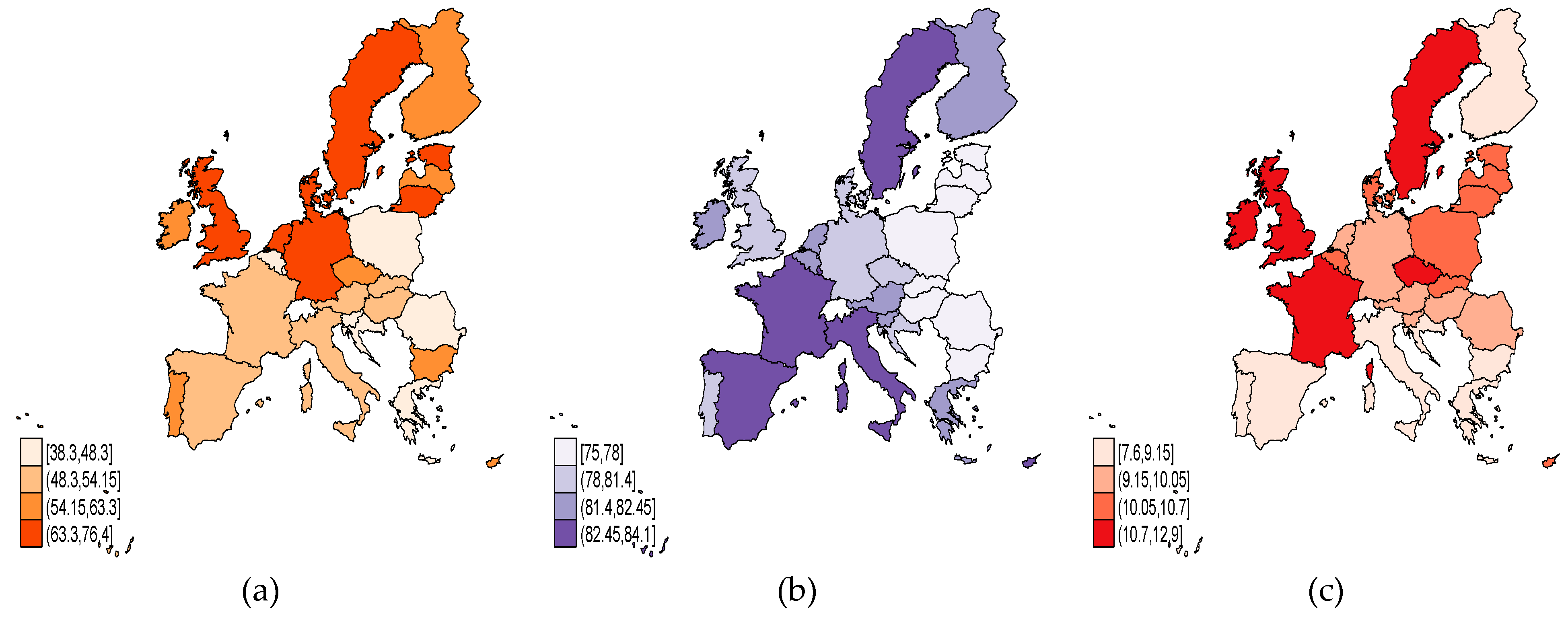
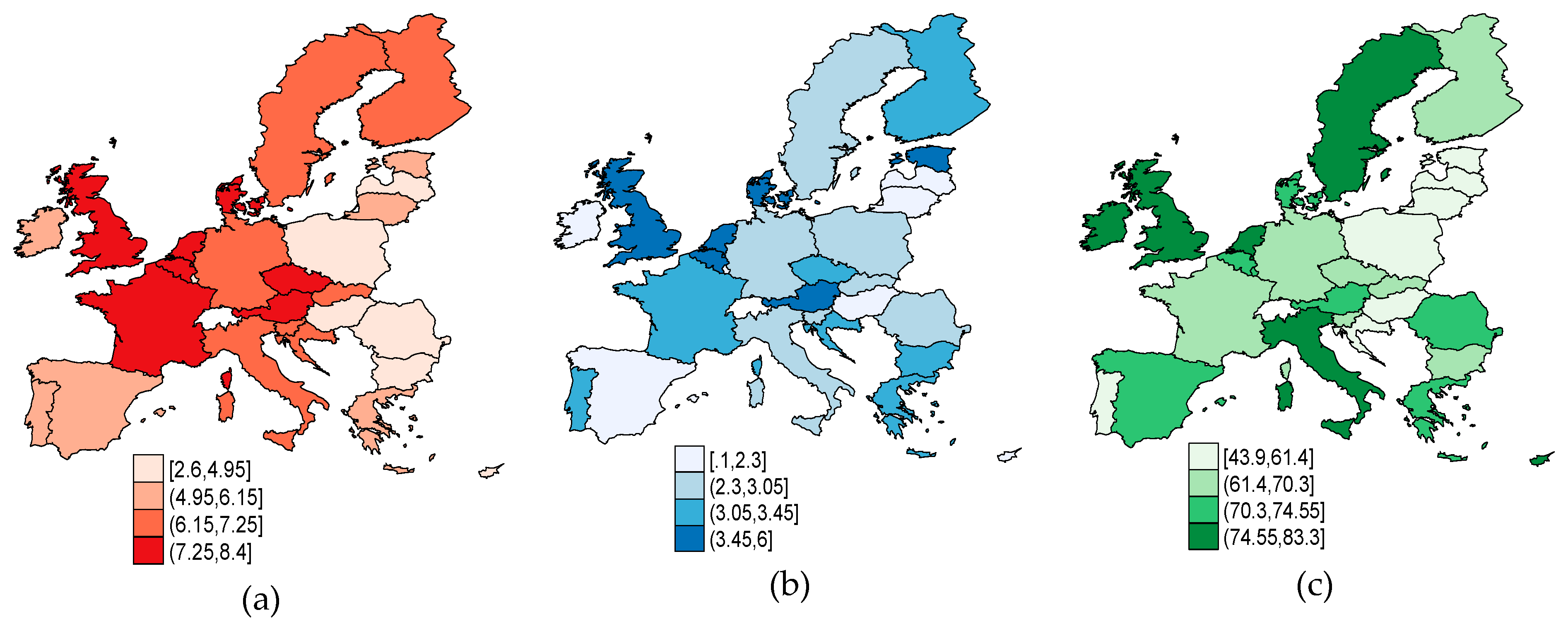
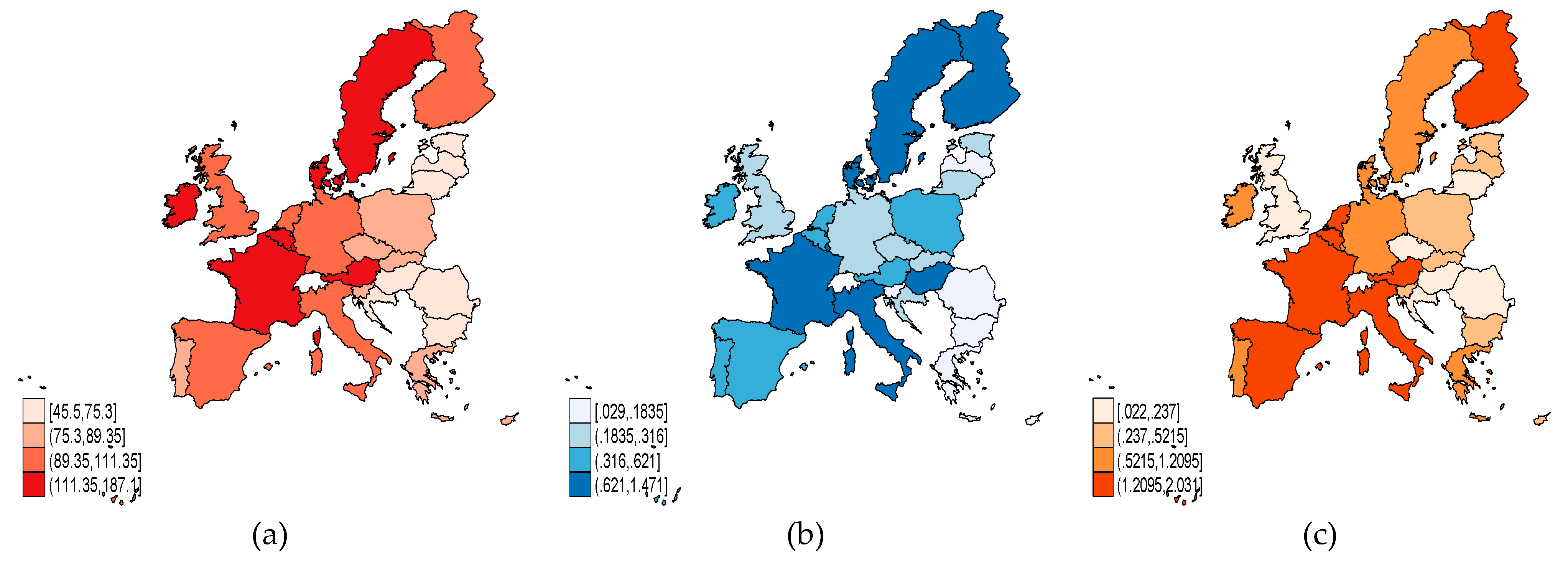
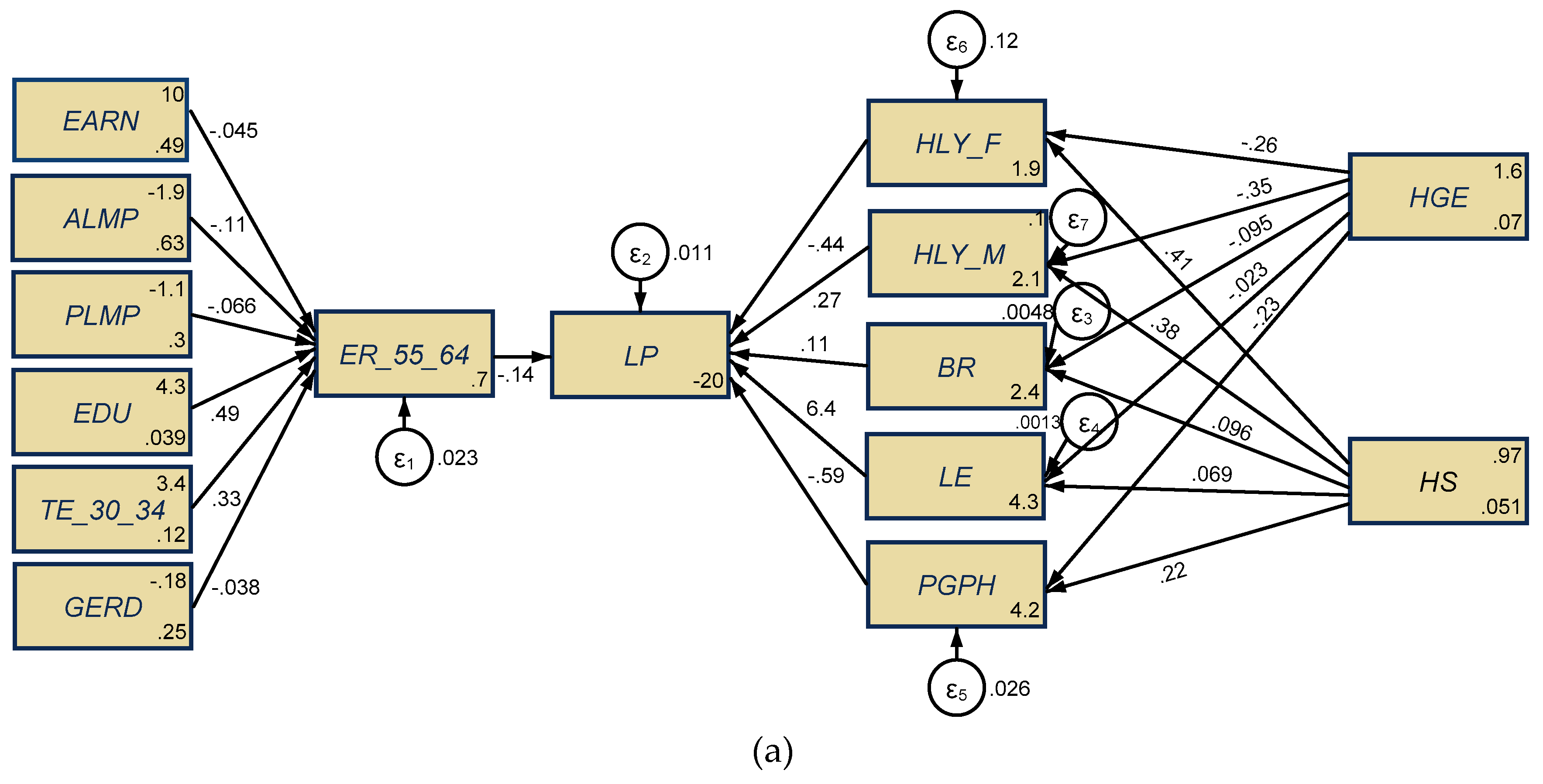
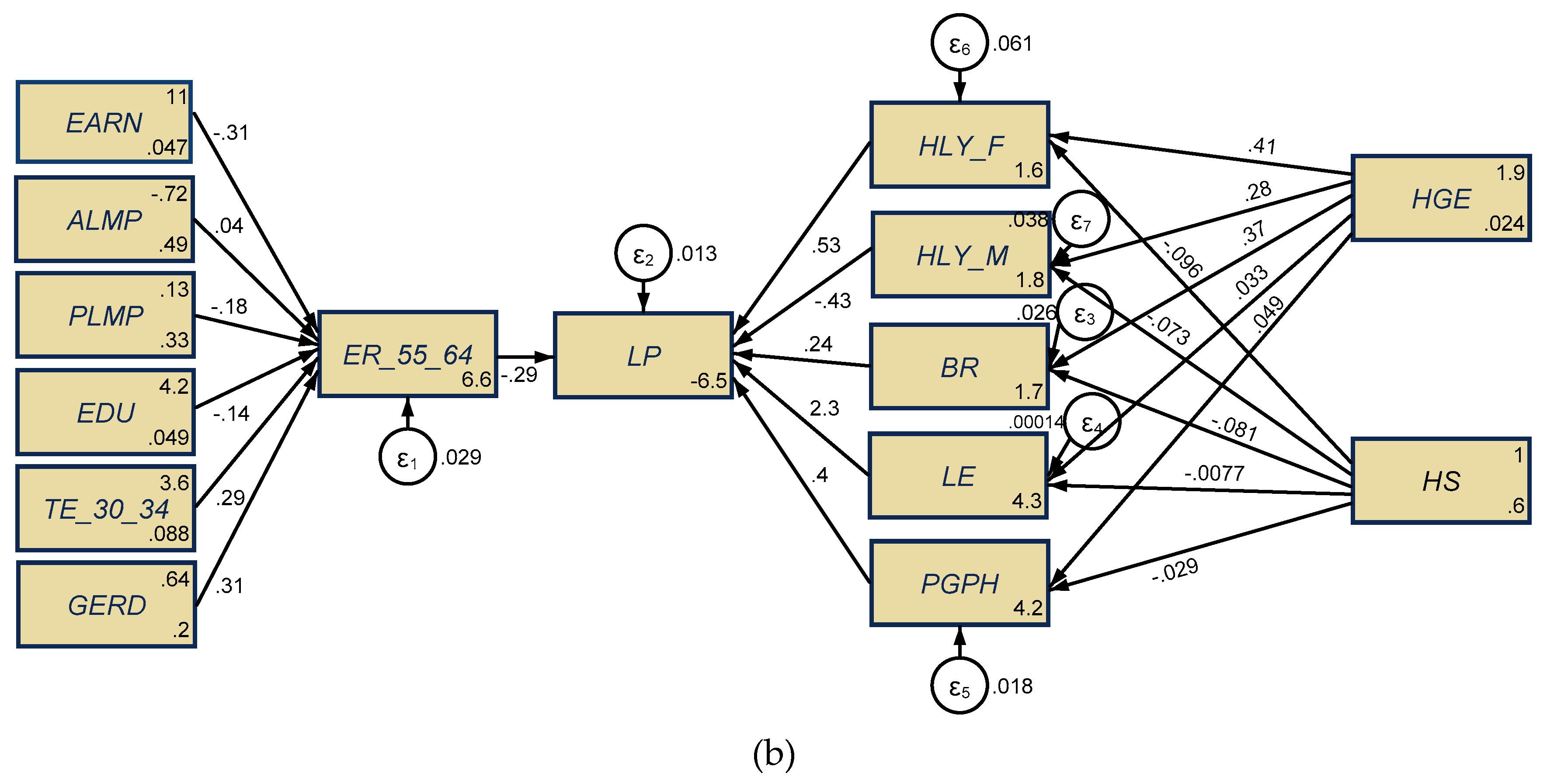
- Aging representative indicators: Employment rate, 55–64-year-old group (% of total population) (ER_55_64); life expectancy at birth, total population (years) (LE); crude birth rate (number of live births per 1000 people) (BR).
- Health indicators: Health government expenditure (% of GDP) (HGE); hospital services (% of GDP) (HS); healthy life years in absolute value at 65—females (years) (HLY_F); healthy life years in absolute value at 65—males (years) (HLY_M); share of people (aged 16+) with good or very good perceived health (%) (PGPH), as a targeted indicator of the Sustainable Development Goals (SDG), namely, SDG3 “Good health and wellbeing”, which “has been found to be a good predictor of people’s future health care use” [30].
- Labor market and other specific indicators: Labor productivity per person employed and hours worked (%, EU-28 = 100) (LP); active labor market policies (% of GDP) (ALMP); passive labor market policies (% of GDP) (PLMP); annual net earnings (purchasing power standard—PPS) (EARN); tertiary education level, 30–34-year old group (% of the population aged 30–34) (TE_30_34); population with secondary, upper, post-secondary, and tertiary education for 15–64-year-old group (levels 3–8) (% of 15–64 years) (EDU); total R&D expenditures (% of GDP) (GERD).
- H1: There are significant implications of the employment rate of the population aged 55–64 for labor productivity, more emphasized for developed countries (EU-15) than developing ones (EU-13);
- H2: There are significant implications of health expenditure (health government expenditure and hospital services) upon aging coordinates (birth rate and life expectancy) in both EU-15 and EU-13 panels, more prominent for developed countries (EU-15) than developing ones (EU-13);
- H3: There are substantial impacts of health expenditure (health government expenditure and hospital services) on older people’s health conditions and overall health perceptions, both for the EU-15 and EU-13 panels;
- H4: There are overall (direct, indirect, total) significant implications of health dimensions and aging upon labor productivity, both for the EU-15 and EU-13 panels.
4. Results and Discussion
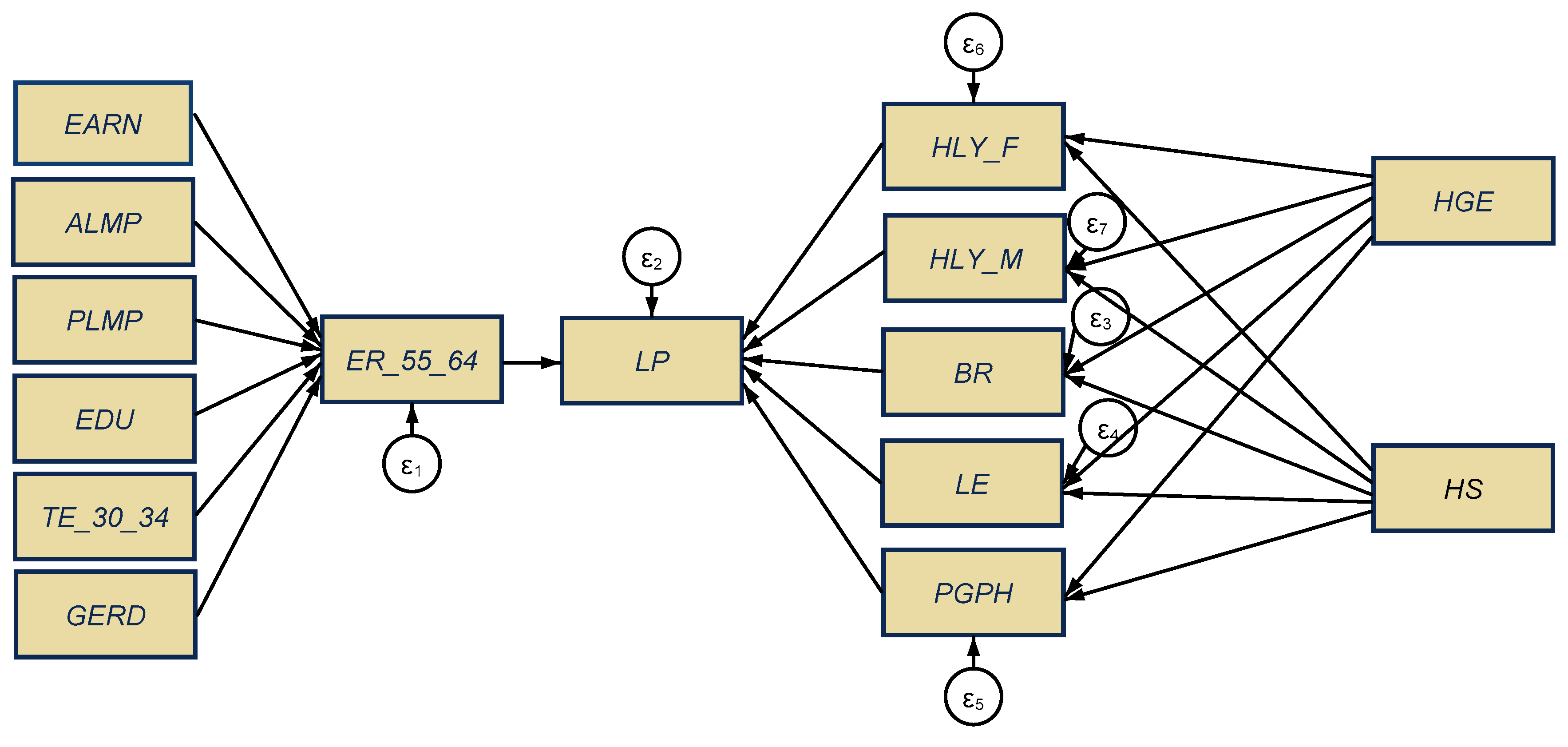
4.1. Results of the Structural Equation Model (SEM)
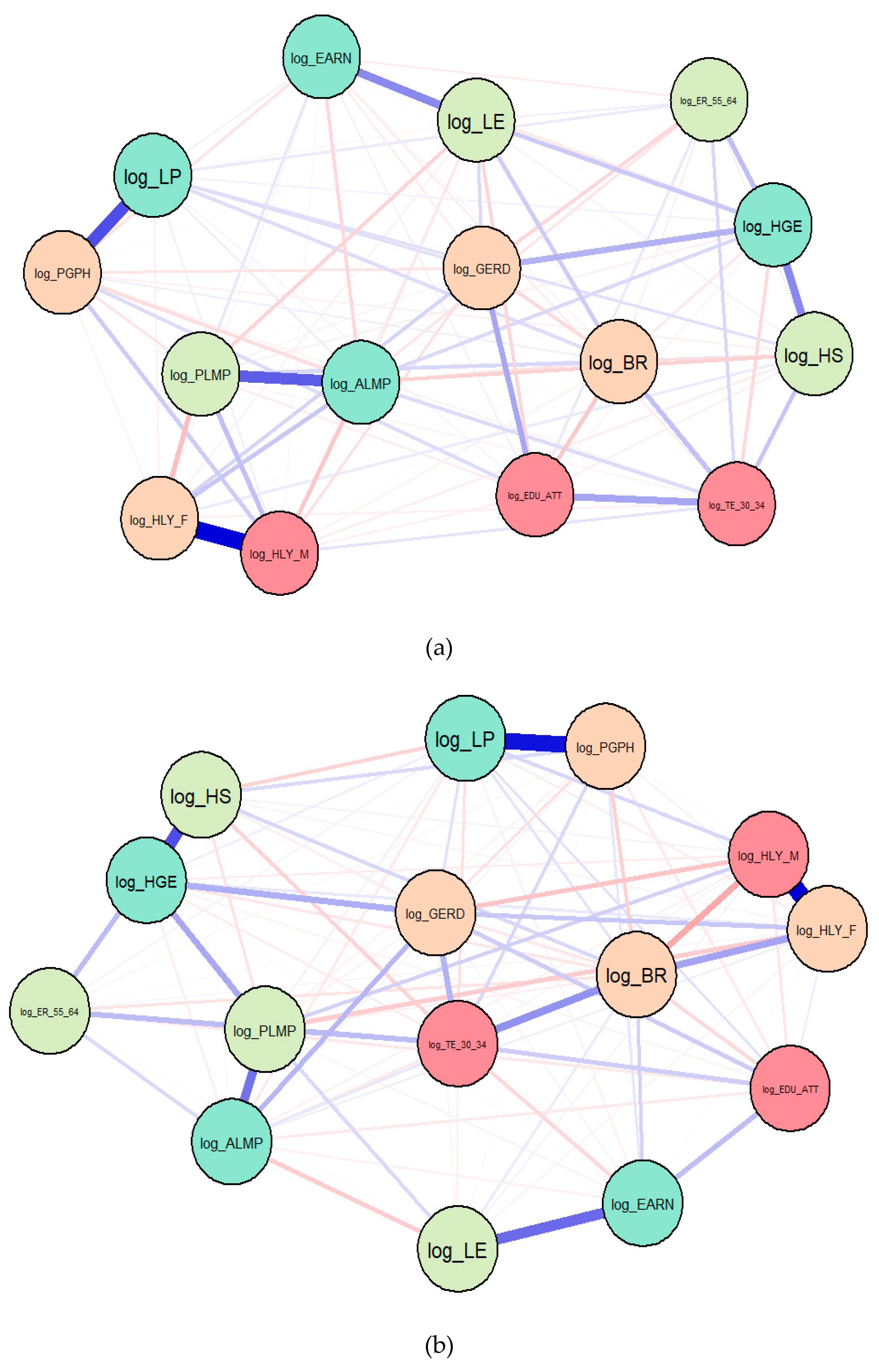
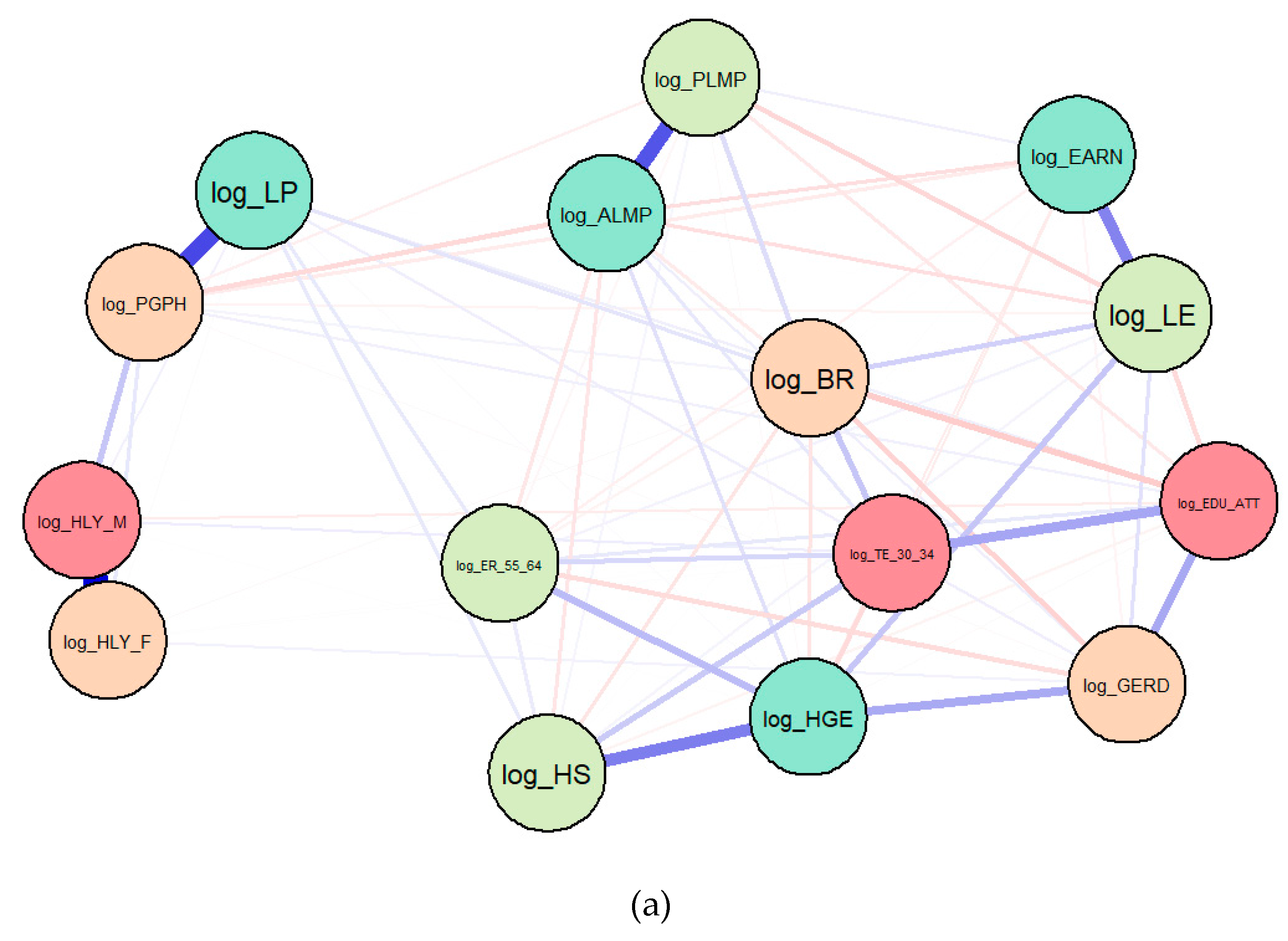
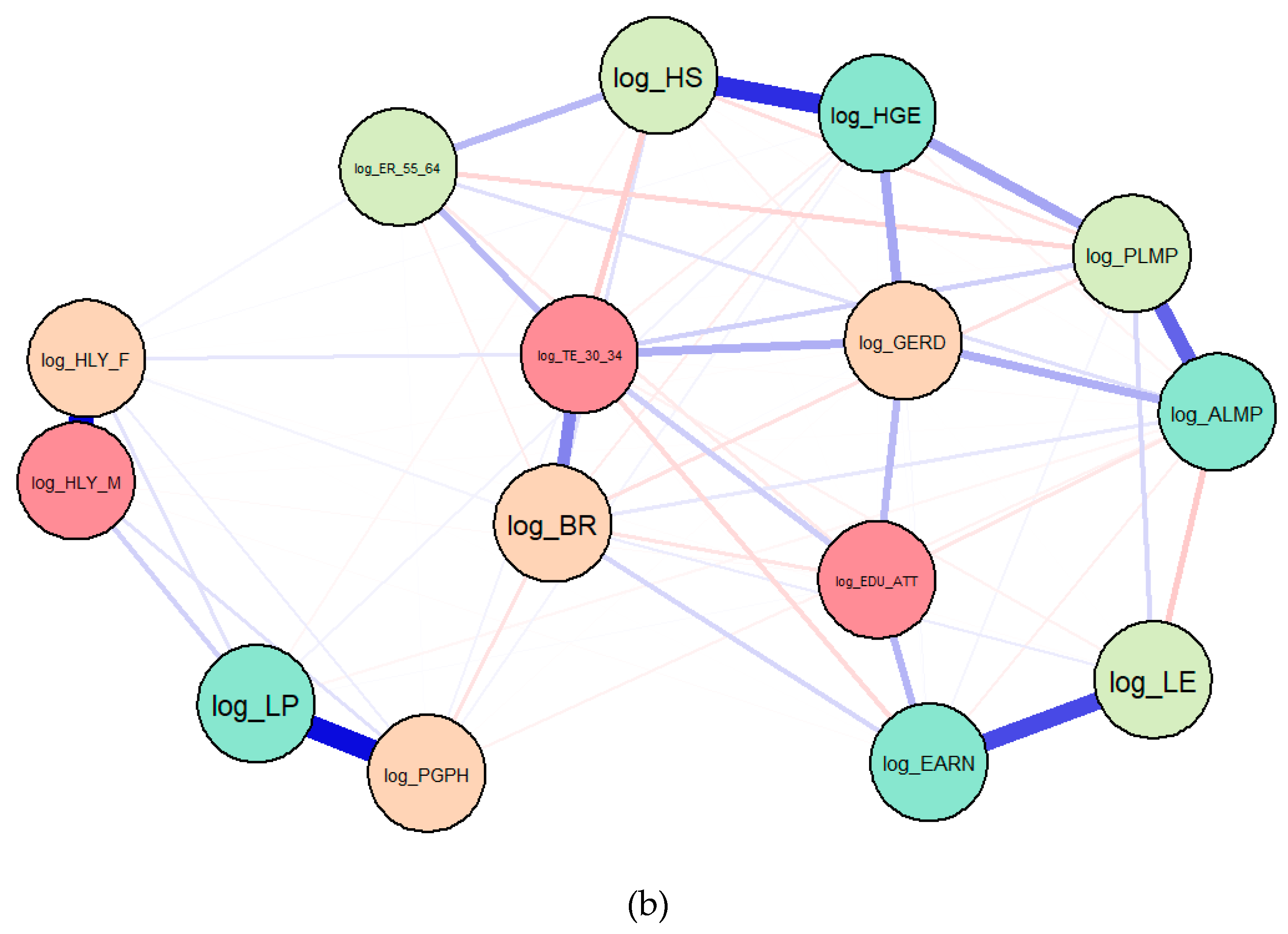
4.2. Results of the Gaussian Graphical Models (GGMs)
4.3. Results of Macroeconometric Models
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | Mean | Sd | Min | Max |
|---|---|---|---|---|---|
| EU-13 | |||||
| LP | 169 | 70.75858 | 14.42612 | 35.7 | 96.1 |
| ER_55_64 | 261 | 41.49157 | 11.0632 | 17.1 | 68.1 |
| GERD | 299 | 0.8074314 | 0.4609393 | 0.024 | 2.604 |
| EDU | 299 | 71.79532 | 14.59404 | 17.1 | 88 |
| EARN | 273 | 35414.8 | 43926.32 | 666.42 | 265212 |
| LE | 273 | 75.16593 | 3.220439 | 67.7 | 82.7 |
| BR | 299 | 10.07358 | 1.053504 | 7.6 | 15.2 |
| TE_30_34 | 299 | 26.13512 | 12.49351 | 1 | 58.7 |
| ALMP | 161 | 0.2024037 | 0.1598259 | 0.019 | 0.873 |
| PLMP | 162 | 0.3844074 | 0.2232345 | 0.065 | 1.365 |
| HLY_F | 161 | 7.165217 | 2.504128 | 2.7 | 14.2 |
| HLY_M | 161 | 7.017391 | 2.335047 | 3 | 13.5 |
| HGE | 289 | 4.975779 | 1.415306 | 1.8 | 7.9 |
| HS | 251 | 2.669323 | 0.6839117 | 0.8 | 5.1 |
| PGPH | 164 | 59.72256 | 9.925003 | 35 | 80.3 |
| N total | 131 | ||||
| EU-15 | |||||
| LP | 195 | 115.0303 | 21.86116 | 75.6 | 188.2 |
| ER_55_64 | 343 | 45.74577 | 12.38773 | 22.2 | 76.4 |
| GERD | 345 | 1.886067 | 0.8329314 | 0 | 3.914 |
| EDU | 341 | 63.13856 | 13.93617 | 19.3 | 82.3 |
| EARN | 317 | 46101.44 | 27095.49 | 1648.52 | 311052 |
| LE | 330 | 79.63242 | 1.790216 | 75.3 | 83.5 |
| BR | 345 | 11.01391 | 1.720831 | 7.6 | 16.7 |
| TE_30_34 | 345 | 33.01696 | 11.05093 | 8.6 | 54.6 |
| ALMP | 266 | 0.6394812 | 0.3517511 | 0.034 | 2.082 |
| PLMP | 278 | 1.362842 | 0.6684728 | 0.15 | 3.126 |
| HLY_F | 192 | 9.878646 | 2.337115 | 5.2 | 16.8 |
| HLY_M | 192 | 9.684375 | 1.839294 | 6.2 | 15.7 |
| HGE | 345 | 6.488696 | 1.085938 | 3.7 | 8.9 |
| HS | 304 | 3.065461 | 1.436566 | 0 | 6.3 |
| PGPH | 196 | 70.79031 | 8.242352 | 45.9 | 84.5 |
| N total | 146 | ||||
| Variables | EU-13 | EU-15 | ||||
|---|---|---|---|---|---|---|
| Coef. | Std. err. | p-Value | Coef. | Std. err | p-Value | |
| Log_ER_55_64 <- | ||||||
| Log_EARN | −0.044 | 0.020 | 0.025 | −0.308 | 0.099 | 0.002 |
| Log_ALMP | −0.106 | 0.019 | −0.000 | 0.040 | 0.033 | 0.237 |
| Log_PLMP | −0.066 | 0.259 | 0.011 | −0.181 | 0.036 | 0.000 |
| Log_EDU_ATT | 0.493 | 0.079 | 0.000 | −0.135 | 0.104 | 0.195 |
| Log_TE_30_34 | 0.328 | 0.040 | 0.000 | 0.293 | 0.060 | 0.000 |
| Log_GERD | −0.037 | 0.285 | 0.184 | 0.314 | 0.046 | 0.000 |
| Log_LP <- | ||||||
| Log_ER_55_64 | −0.144 | 0.050 | 0.004 | −0.292 | 0.046 | 0.000 |
| Log_BR | 0.105 | 0.152 | 0.488 | 0.239 | 0.079 | 0.003 |
| Log_LE | 6.366 | 0.351 | 0.000 | 2.251 | 0.803 | 0.005 |
| Log_PGPH | −0.585 | 0.088 | 0.000 | 0.404 | 0.106 | 0.000 |
| Log_HLY_F | −0.440 | 0.109 | 0.000 | 0.527 | 0.140 | 0.000 |
| Log_HLY_M | 0.266 | 0.131 | 0.043 | −0.434 | 0.155 | 0.005 |
| Log_EARN | 0.006 | 0.003 | 0.078 | 0.090 | 0.032 | 0.005 |
| Log_ALMP | 0.015 | 0.006 | 0.012 | −0.011 | 0.010 | 0.245 |
| Log_PLMP | 0.009 | 0.005 | 0.057 | 0.053 | 0.013 | 0.000 |
| Log_DU_ATT | −0.071 | 0.027 | 0.010 | 0.039 | 0.031 | 0.204 |
| Log_TE_30_34 | −0.047 | 0.017 | 0.007 | −0.085 | 0.022 | 0.000 |
| Log_GERD | 0.005 | 0.004 | 0.228 | −0.091 | 0.019 | 0.000 |
| Log_HS | 0.247 | 0.140 | 0.078 | −0.067 | 0.029 | 0.021 |
| Log_HGE | −0.001 | 0.119 | 0.989 | 0.277 | 0.145 | 0.056 |
| Log_BR <- | ||||||
| Log_HS | 0.096 | 0.031 | 0.002 | −0.081 | 0.026 | 0.002 |
| Log_HGE | −0.095 | 0.027 | 0.000 | 0.371 | 0.130 | 0.004 |
| Log_LE <- | ||||||
| Log_HS | 0.069 | 0.016 | 0.000 | −0.007 | 0.001 | 0.000 |
| Log_HGE | −0.023 | 0.014 | 0.097 | 0.033 | 0.009 | 0.001 |
| Log_PGPH <- | ||||||
| Log_HS | 0.215 | 0.073 | 0.003 | −0.028 | 0.021 | 0.190 |
| Log_HGE | −0.230 | 0.062 | 0.000 | 0.048 | 0.108 | 0.655 |
| Log_HLY_F <- | ||||||
| Log_HS | 0.405 | 0.158 | 0.011 | −0.095 | 0.040 | 0.017 |
| Log_HGE | −0.264 | 0.135 | 0.050 | 0.406 | 0.200 | 0.043 |
| Log_HLY_M <- | ||||||
| Log_HS | 0.384 | −0.146 | 0.009 | −0.072 | 0.031 | 0.021 |
| Log_HGE | −0.354 | 0.124 | 0.004 | 0.277 | 0.158 | 0.080 |
| Test Scale = Mean (Standardized Items) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Average | EU-13 | EU-15 | ||||||
| Item | Obs | Sign | Interitem Correlation | Alpha | Obs | Sign | Interitem Correlation | Alpha |
| Log_ER_55_64 | 261 | − | 0.0782 | 0.5428 | 343 | + | 0.1895 | 0.7660 |
| Log_LP | 169 | + | 0.0577 | 0.4615 | 195 | + | 0.1632 | 0.7319 |
| Log_BR | 299 | − | 0.0963 | 0.5988 | 345 | + | 0.1848 | 0.7604 |
| Log_LE | 273 | + | 0.0478 | 0.4129 | 330 | + | 0.1948 | 0.7720 |
| Log_PGPH | 164 | + | 0.0534 | 0.4413 | 196 | + | 0.1657 | 0.7355 |
| Log_HLY_F | 161 | + | 0.0502 | 0.4250 | 192 | + | 0.1597 | 0.7269 |
| Log_HLY_M | 161 | + | 0.0460 | 0.4029 | 192 | + | 0.1642 | 0.7334 |
| Log_EARN | 273 | + | 0.0614 | 0.4779 | 317 | + | 0.1774 | 0.7512 |
| Log_ALMP | 161 | − | 0.0812 | 0.5530 | 266 | + | 0.1856 | 0.7613 |
| Log_PLMP | 162 | + | 0.0726 | 0.5230 | 278 | + | 0.20006 | 0.7784 |
| Log_EDU_ATT | 299 | − | 0.0694 | 0.5106 | 341 | + | 0.1616 | 0.7296 |
| Log_TE_30_34 | 299 | + | 0.0901 | 0.5808 | 345 | + | 0.1502 | 0.7121 |
| Log_GERD | 299 | + | 0.0873 | 0.5725 | 344 | + | 0.1724 | 0.7447 |
| Log_HS | 251 | + | 0.0709 | 0.5163 | 287 | − | 0.1985 | 0.7762 |
| Log_HGE | 289 | − | 0.1089 | 0.6310 | 345 | − | 0.2389 | 0.8146 |
| Total scale | 0.6346 | 0.7674 | ||||||
| Variables | EU-13 | EU-15 | ||||
|---|---|---|---|---|---|---|
| Chi2 | df | p-Value | Chi2 | df | p-Value | |
| Log_ER_55_64 | 140.69 | 6 | 0.0000 | 108.28 | 6 | 0.0000 |
| Log_LP | 456.36 | 6 | 0.0000 | 207.21 | 6 | 0.0000 |
| Log_BR | 14.34 | 2 | 0.0008 | 10.34 | 2 | 0.0057 |
| Log_LE | 17.92 | 2 | 0.0001 | 16.34 | 2 | 0.0003 |
| Log_PGPH | 14.97 | 2 | 0.0006 | 2.37 | 2 | 0.3057 |
| Log_HLY_F | 7.06 | 2 | 0.0293 | 5.86 | 2 | 0.0535 |
| Log_HLY_M | 9.84 | 2 | 0.0073 | 5.33 | 2 | 0.0695 |
| EU-13 | ||
| Likelihood ratio | ||
| chi2_ms(55) | 905.818 | model vs. saturated |
| p > chi2 | 0.000 | |
| chi2_bs(77) | 1258.973 | baseline vs. saturated |
| p > chi2 | 0.000 | |
| Information criteria | ||
| AIC | −266.492 | Akaike’s information criterion |
| BIC | −162.984 | Bayesian information criterion |
| Baseline comparison | ||
| CFI | 0.280 | Comparative fit index |
| TLI | −0.008 | Tucker-Lewis index |
| Size of residuals | ||
| SRMR | 0.070 | Standardized root mean squared residual |
| CD | 0.681 | Coefficient of determination |
| EU-15 | ||
| Likelihood ratio | ||
| chi2_ms(26) | 1217.706 | model vs. saturated |
| p > chi2 | 0.000 | |
| chi2_bs(38) | 1466.510 | baseline vs. saturated |
| p > chi2 | 0.000 | |
| Information criteria | ||
| AIC | −1259.765 | Akaike’s information criterion |
| BIC | −1152.355 | Bayesian information criterion |
| Baseline comparison | ||
| CFI | 0.163 | Comparative fit index |
| TLI | −0.171 | Tucker-Lewis index |
| Size of residuals | ||
| SRMR | 0.040 | Standardized root mean squared residual |
| CD | 0.550 | Coefficient of determination |


| EU-13 | EU-15 | |||
|---|---|---|---|---|
| (1) | (2) | (1) | (2) | |
| RREG log_LP | PCSE log_LP | RREG log_LP | PCSE log_LP | |
| log_ER_55_64 | −0.107 (0.0698) | −0.0918 * (0.0470) | −0.0770 * (0.0365) | −0.127 *** (0.0264) |
| _cons | 4.680 *** (0.265) | 4.583 *** (0.175) | 5.026 *** (0.142) | 5.224 *** (0.103) |
| N | 169 | 169 | 195 | 195 |
| (a) | |||||
| EU-13 | (1) | (2) | (3) | (4) | (5) |
| log_HLY_F | log_HLY_M | log_BR | log_LE | log_PGPH | |
| log_HGE | −0.219 (0.128) | −0.400 ** (0.121) | −0.126 *** (0.0229) | −0.0182 (0.0107) | −0.279 *** (0.0603) |
| log_HS | 0.491 ** (0.150) | 0.466 ** (0.142) | 0.0952 *** (0.0258) | 0.0697 *** (0.0119) | 0.235 ** (0.0708) |
| _cons | 1.802 *** (0.179) | 2.101 *** (0.169) | 2.407 *** (0.0297) | 4.286 *** (0.0139) | 4.312 *** (0.0826) |
| N | 161 | 161 | 251 | 237 | 164 |
| EU-15 | (1) | (2) | (3) | (4) | (5) |
| log_HLY_F | log_HLY_M | log_BR | log_LE | log_PGPH | |
| log_HGE | 0.377 * (0.182) | 0.245 (0.143) | −0.219 ** (0.0702) | 0.102 *** (0.00822) | −0.195 *** (0.0527) |
| log_HS | −0.0648 (0.0356) | −0.0536 (0.0280) | 0.0108 (0.0170) | −0.0172 *** (0.00202) | 0.0256 * (0.0103) |
| _cons | 1.606 *** (0.326) | 1.832 *** (0.256) | 2.805 *** (0.121) | 4.204 *** (0.0141) | 4.638 *** (0.0944) |
| N | 179 | 179 | 287 | 273 | 182 |
| (b) | |||||
| EU-13 | (1) | (2) | (3) | (4) | (5) |
| log_HLY_F | log_HLY_M | log_BR | log_LE | log_PGPH | |
| log_HGE | −0.301 *** (0.0430) | −0.391 *** (0.0285) | −0.143 *** (0.0137) | −0.0195 *** (0.00538) | −0.255 *** (0.0123) |
| log_HS | 0.493 *** (0.0702) | 0.451 *** (0.0605) | 0.112 *** (0.0185) | 0.0602 *** (0.00682) | 0.234 *** (0.0303) |
| _cons | 1.914 *** (0.0563) | 2.088 *** (0.0498) | 2.422 *** (0.0184) | 4.298 *** (0.00787) | 4.261 *** (0.0257) |
| N | 161 | 161 | 251 | 237 | 164 |
| EU-15 | (1) | (2) | (3) | (4) | (5) |
| log_HLY_F | log_HLY_M | log_BR | log_LE | log_PGPH | |
| log_HGE | 0.378 ** (0.142) | 0.239 * (0.0949) | −0.219 ** (0.0702) | 0.102 *** (0.00822) | 0.0219 (0.0598) |
| log_HS | −0.0690 ** (0.0257) | −0.0547 ** (0.0177) | 0.0108 (0.0170) | −0.0172 *** (0.00202) | −0.0194 * (0.00795) |
| _cons | 1.604 *** (0.253) | 1.843 *** (0.167) | 2.805 *** (0.121) | 4.204 *** (0.0141) | 4.230 *** (0.108) |
| N | 179 | 179 | 287 | 273 | 182 |
| EU-13 | EU-15 | |||
|---|---|---|---|---|
| (1) RREG | (2) PCSE | (3) RREG | (4) PCSE | |
| log_LP | log_LP | log_LP | log_LP | |
| log_HGE | 0.195 *** (0.0460) | 0.174 *** (0.0232) | 0.554 *** (0.0684) | 0.371 *** (0.0966) |
| log_HS | −0.178 *** (0.0525) | −0.134 *** (0.0354) | −0.218 *** (0.0135) | −0.189 *** (0.0177) |
| log_HLY_F | −0.361 ** (0.111) | −0.376 *** (0.0860) | 0.357 *** (0.0939) | 0.395 *** (0.0821) |
| log_HLY_M | 0.213 (0.135) | 0.227 * (0.106) | −0.414 *** (0.107) | −0.443 *** (0.0829) |
| log_BR | 0.205 (0.142) | 0.120 (0.158) | 0.0462 (0.0563) | 0.144 (0.0795) |
| log_LE | 6.112 *** (0.378) | 6.113 *** (0.319) | −0.833 (0.577) | 0.0420 (0.352) |
| log_PGPH | −0.417 *** (0.0847) | −0.407 *** (0.0603) | 0.564 *** (0.0726) | 0.511 *** (0.0576) |
| _cons | –20.90 *** (1.459) | −20.75 *** (1.078) | 5.162 * (2.482) | 1.621 (1.436) |
| N | 148 | 148 | 165 | 165 |
| R2 | 0.759 | 0.771 | 0.797 | 0.771 |
References
- Börsch-Supan, A.; Chiappori, P.A. Aging population: Problems and policy options in the US and Germany. Econ. Policy 1991, 6, 104–139. [Google Scholar] [CrossRef]
- Coleman, D. Population ageing: An unavoidable future. In The Welfare State Reader, 2nd ed.; Pierson, C., Castles, F.G., Eds.; Polity Press: Cambridge, UK; Malden, MA, USA, 2006; pp. 298–308. [Google Scholar]
- Káčerová, M.; Mladek, J. Population ageing as generation substitutions: Economic and social aspects. Ekon. Cas. 2012, 60, 259–276. [Google Scholar]
- Cristea, M.; Mitrica, A. Global ageing: Do privately managed pension funds represent a long term alternative for the Romanian Pension system? Empirical research. Rom. J. Polit. Sci. 2016, 16, 63–106. [Google Scholar]
- Song, J.; Ryu, D. Aging effects on consumption risk-sharing channels in European countries. Zb. Rad. Ekon. Fak. U Rijeci Časopis Za Ekon. Teor. Praksu 2018, 36, 585–617. [Google Scholar]
- Andor, L. Employment Trends and Policies for Older Workers in the Recession. European Foundation for the Improvement of Living and Working Conditions. 2012, pp. 1–12. Available online: https://www.eurofound.europa.eu/sites/default/files/ef_publication/field_ef_document/ef1235en.pdf (accessed on 2 October 2019).
- Bengtsson, T.; Qi, H. Ageing workforce, social cohesion and sustainable development: Political challenges within the Baltic Sea region: Sweden. In Ageing Workforce, Social Cohesion and Sustainable Development: Political Challenges within The Baltic Sea Region; Becker, P., Schütz, J., Zimmermann, A., Eds.; Max Planck Society/Population Europe: Berlin, Germany, 2018; pp. 55–59. [Google Scholar]
- European Commission. The 2018 Ageing Report: Underlying Assumptions and Projection Methodologies; Publications Office of the European Union: Luxembourg, 2017; pp. 1–240. [Google Scholar]
- European Commission. Ready for the Demographic Revolution? Measuring Active Ageing. 2016. Available online: https://ec.europa.eu/social/main.jsp?langId=en&catId=752&furtherNews=yes&newsId=2430 (accessed on 1 October 2019).
- OECD/EU. Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2018. [Google Scholar]
- OECD. Working Better with Age; Ageing and Employment Policies; OECD Publishing: Paris, France, 2019. [Google Scholar]
- World Health Organization (WHO). Global Strategy and Action Plan. on Ageing and Health; World Health Organization: Geneva, Switzerland, 2017; pp. 1–46. [Google Scholar]
- Taylor, P. Ageing Labour Forces: Promises and Prospects; Edward Elgar Publishing: Cheltenham, UK; Northampton, MA, USA, 2008. [Google Scholar]
- Gusmano, M.K.; Okma, K.G.H. Population aging and the sustainability of the welfare state. Hastings Cent. Rep. 2018, 48, S57–S61. [Google Scholar] [CrossRef] [Green Version]
- Jensen, S.E.H.; Bo Nielsen, S. Population ageing, public debt and sustainable fiscal policy. Fisc. Stud. 1995, 16, 1–20. [Google Scholar] [CrossRef]
- Zokalj, M. The impact of population aging on public finance in the European Union. Financial Theory and Practice 2016, 40, 383–412. [Google Scholar] [CrossRef]
- European Commission. The 2018 Ageing Report: Economic and Budgetary Projections for the 28 EU Member States (2016-2070); Publications Office of the European Union: Luxembourg, 2018; pp. 1–383. [Google Scholar]
- Breyer, F.; Costa-Font, J.; Felder, S. Ageing, health, and health care. Oxf. Rev. Econ. Policy 2010, 26, 674–690. [Google Scholar] [CrossRef] [Green Version]
- Cohen, N. The Silver Economy: Healthier and Wealthier. Available online: https://www.ft.com/content/08bff556-52c7-11e4-a236-00144feab7de (accessed on 12 October 2019).
- Bosch-Farré, C.; Garre-Olmo, J.; Bonmatí-Tomàs, A.; Malagón-Aguilera, M.C.; Gelabert-Vilella, S.; Fuentes-Pumarola, C.; Juvinyà-Canal, D. Prevalence and related factors of active and healthy ageing in Europe according to two models: Results from the Survey of Health, Ageing and Retirement in Europe (SHARE). PLoS ONE 2018, 13, 1–19. [Google Scholar] [CrossRef]
- Griffiths, A. Ageing, health and productivity: A challenge for the new millennium. Work Stress 1997, 11, 197–214. [Google Scholar] [CrossRef]
- Garibaldi, P.; Oliveira Martins, J.; van Ours, J. Ageing, Health, and Productivity: The Economics of Increased Life Expectancy; Oxford University Press: Oxford, UK, 2010; pp. 1–288. [Google Scholar]
- Sharpe, A. Is ageing a drag on productivity growth? A review article on Ageing, Health and Productivity: The Economics of Increased Life Expectancy. Int. Prod. Monit. 2011, 21, 82–94. [Google Scholar]
- UNECE/European Commission. Active Ageing Index 2014 Analytical Report; Report prepared by Asghar Zaidi and David Stanton, Geneva, Italy. 2015. Available online: https://ec.europa.eu/eip/ageing/library/2014-active-ageing-index-aai-analytical-report_en (accessed on 11 September 2019).
- Gray, A. Population Ageing and Health Care Expenditure. In Oxford Institute of Ageing, Ageing Horizons; Available online: https://www.ageing.ox.ac.uk/download/15 (accessed on 19 September 2019).
- Bussolo, M.; Koettl, J.; Sinnott, E. Golden Aging: Prospects for Healthy, Active, and Prosperous Aging in Europe and Central Asia; Europe and Central Asia Studies; The World Bank: Washington, DC, USA, 2015; pp. 1–330. [Google Scholar]
- Bremer, D.; Lüdecke, D.; von dem Knesebeck, O. Social relationships, age and the use of preventive health services: Findings from the German Ageing Survey. Int. J. Environ. Res. Public Health 2019, 16, 4272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltrán-Sánchez, H.; Soneji, S.; Crimmins, E.M. Past, present, and future of healthy life expectancy. Cold Spring Harb. Perspect. Med. 2015, 5, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klenk, J.; Keil, U.; Jaensch, A.; Christiansen, M.C.; Nagel, G. Changes in life expectancy 1950–2010: Contributions from age- and disease-specific mortality in selected countries. Popul. Health Metr. 2016, 14, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. Eurostat Database. 2019. Available online: https://ec.europa.eu/eurostat/data/database (accessed on 2 September 2019).
- Yang, L.; Zhao, K.; Fan, Z. Exploring determinants of population ageing in Northeast China: From a socio-economic perspective. Int. J. Environ. Res. Public Health 2019, 16, 4265. [Google Scholar] [CrossRef] [Green Version]
- Taylor, P. European Foundation for the Improvement of Living and Working Conditions. In Employment Initiatives for an Ageing Workforce in the EU15; Office for Official Publications of the European Communities: Luxembourg, 2006; pp. 1–95. [Google Scholar]
- European Commission. Growing The European Silver Economy. 2015. Available online: http://ec.europa.eu/research/innovation-union/pdf/active-healthy-ageing/silvereco.pdf (accessed on 2 September 2019).
- Barkovic Bojanic, I.; Erceg, A. Silver Economy: Demographic Change and Economic Opportunity. Interdisciplinary Management Research XIII. 2017, pp. 1005–1020. Available online: https://bib.irb.hr/datoteka/879480.349724720-Interdisciplinary-Management-Research-XIII.pdf#page=1006 (accessed on 4 September 2019).
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S. Data resource profile: The survey of health, ageing and retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef]
- Mahlberg, B.; Freund, I.; Crespo Cuaresma, J.; Prskawetz, A. Ageing, productivity and wages in Austria. Labour Econ. 2013, 22, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Myck, M. Living longer, working longer: The need for a comprehensive approach to labour market reform in response to demographic changes. Eur. J. Ageing 2015, 12, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Akanni, M.T.; Čepar, Ž. Impact of population ageing on unemployment and entrepreneurial activity: The case of Slovenia. Organizacija 2015, 48, 232–245. [Google Scholar] [CrossRef] [Green Version]
- Hsu, Y.H. Population Aging, Labor Force Participation, and Economic Growth. Available online: http://jbepnet.com/journals/Vol_4_No_1_March_2017/13.pdf (accessed on 12 September 2019).
- Börsch-Supan, A. Population Aging, Social Security Design, and Early Retirement. Available online: https://0-www-jstor-org.brum.beds.ac.uk/stable/40751550 (accessed on 14 September 2019).
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The triple aim: Care, health, and cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). World Report On Ageing and Health; World Health Organization: Geneva, Switzerland, 2015; pp. 1–247. Available online: https://apps.who.int/iris/bitstream/handle/10665/186463/9789240694811_eng.pdf?sequence=1 (accessed on 14 September 2019).
- Dormont, B.; Martins, J.O.; Pelgrin, F.; Suhrcke, M. Health expenditures, longevity and growth. In Ageing, Health, and Productivity: The Economics of Increased Life Expectancy; Garibaldi, P., Oliveira Martins, J., van Ours, J., Eds.; Oxford University Press: New York, NY, USA, 2010; pp. 5–113. [Google Scholar]
- Mannheim, I.; Schwartz, E.; Xi, W.; Buttigieg, S.C.; McDonnell-Naughton, M.; Wouters, E.J.M.; van Zaalen, Y. Inclusion of older adults in the research and design of digital technology. Int. J. Environ. Res. Public. Health 2019, 16, 3718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koc, E.; Bozkurt, G.A. Hospitality employees’ future expectations: Dissatisfaction, stress, and burnout. Int. J. Hosp. Tour. Adm. 2017, 18, 459–473. [Google Scholar] [CrossRef]
- Gong, L.; Li, H.; Wang, D. Health investment, physical capital accumulation, and economic growth. China Econ. Rev. 2012, 23, 1104–1119. [Google Scholar] [CrossRef]
- Hansen, C.W. Life expectancy and human capital: Evidence from the international epidemiological transition. J. Health Econ. 2013, 32, 1142–1152. [Google Scholar] [CrossRef]
- Gulavani, S.S.; Kulkarni, R.V. Role of Information Technology in Health Care. In Proceedings of the 4th National Conference INDIA-Com 2010, New Delhi, India, 25–26 February 2010. [Google Scholar]
- Thimbleby, H. Technology and the future of healthcare. J. Pub. Health Res. 2013, 2, e28. [Google Scholar] [CrossRef] [Green Version]
- Bianco, A. Active Labour Market. Policies for Digital Economy: Skills Development and Workforce Preparation; Working Papers. ASTRIL—Associazione Studi e Ricerche Interdisciplinari sul Lavoro, 2018. Available online: http://host.uniroma3.it/associazioni/astril/db/434116a6-9952-477f-9fff-98da58bb36a7.pdf (accessed on 16 September 2019).
- Taylor, P.; Jorgensen, B.; Watson-Lynn, E. Population ageing in a globalizing labour market: Implications for older workers. China J. Soc. Work 2010, 3, 259–272. [Google Scholar] [CrossRef]
- European Union. The European Year for Active Ageing and Solidarity between Generations (2012); The European Parliament and the Council of the European Union: Brussels, Belgium, 2012. [Google Scholar]
- Álvarez-García, J.; Durán-Sánchez, A.; Del Río-Rama, M.D.; García-Vélez, D.F. Active ageing: Mapping of Scientific Coverage. Int. J. Environ. Res. Public. Health 2018, 15, 2727. [Google Scholar] [CrossRef] [Green Version]
- European Commission. Active Ageing Index at the Local Level. Peer Review in Social Protection and Social Inclusion 2015–2016; Directorate-General for Employment, Social Affairs and Inclusion, Population Unit of the UNECE and the European Centre for Social Welfare Policy and Research in Vienna: Berlin, Germany, 2016. [Google Scholar]
- Zaidi, A.; Gasior, K.; Zolyomi, E.; Schmidt, A.; Rodrigues, R.; Marin, B. Measuring active and healthy ageing in Europe. J. Eur. Soc. Policy 2017, 27, 138–157. [Google Scholar] [CrossRef]
- Cylus, J.; Figueras, J.; Normand, C. Will population ageing spell the end of the welfare state? A review of evidence and policy options. In The Economics of Healthy and Active Ageing Series; Sagan, A., Richardson, E., Eds.; European Observatory on Health Systems and Policies; WHO Regional Office for Europe: Copenhagen, Denmark, 2018; pp. 1–43. [Google Scholar]
- Börsch-Supan, A. The Impact of Global Ageing on Labor, Product and Capital Markets. 2005, pp. 1–32. Available online: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.569.1414&rep=rep1&type=pdf (accessed on 25 October 2019).
- Aiyar, S.S.; Ebeke, C.; Shao, X. The Impact of Workforce Aging on European Productivity. IMF Working Paper 2016, 16/238, 1-30. Available online: https://ssrn.com/abstract=2924323 (accessed on 2 September 2019).
- Lloyd-Sherlock, P. Population ageing in developed and developing regions: Implications for health policy. Soc. Sci. Med. 2000, 51, 887–895. [Google Scholar] [CrossRef]
- European Commission. Directorate-General for Employment, Social Affairs & Inclusion. Statistical Data. 2019. Available online: https://ec.europa.eu/social/main.jsp?catId=1249&langId=en (accessed on 2 September 2019).
- Cristea, M.; Noja, G.G. European agriculture under immigration effects: New empirical evidence. Agric. Econ. 2019, 65, 112–122. [Google Scholar] [CrossRef] [Green Version]
- Fisman, R.; Luca, M. How Amazon’s Higher Wages Could Increase Productivity. Harvard Business Review Digital Article. 2018. Available online: https://hbsp.harvard.edu.product.H04LEC-PDF-ENG (accessed on 19 December 2019).
- Foygel, R.; Drton, M. Extended Bayesian information criteria for Gaussian Graphical Models. Adv. Neural. Inf. Process. Syst. 2010, 23, 2020–2028. [Google Scholar]
- Börsch-Supan, A.; Weiss, M. Productivity and age: Evidence from work teams at the assembly line. J. Econ. Ageing 2016, 7, 30–42. [Google Scholar] [CrossRef] [Green Version]
- Feyrer, J. Aggregate evidence on the link between age structure and productivity. Popul. Dev. Rev. 2008, 34, 78–99. [Google Scholar]
- Guest, R.; Shacklock, K. The impending shift to an older mix of workers: Perspectives from the management and economics literatures. Int. J. Organ. Behav. 2005, 10, 713–728. [Google Scholar]
- Bersin, J.; Chamorro-Premuzic, T. The Case for Hiring Older Workers. Harvard Business Review. 2019. Available online: https://hbr.org/2019/09/the-case-for-hiring-older-workers (accessed on 22 January 2020).
- OECD. Ageing and Employment Policies: Denmark 2015: Working Better with Age; Ageing and Employment Policies; Policies, OECD Publishing: Paris, France, 2015; pp. 1–160. [Google Scholar]
- Noja, G.G.; Cristea, M. Working conditions and flexicurity measures as key drivers of economic growth: Empirical evidence for Europe. Ekon. Cas. 2018, 66, 719–749. [Google Scholar]
- Smith, A.D. Memory. In Handbook of the Psychology of Ageing, 4th ed.; Birren, J.E., Ed.; Academic Press: New York, NY, USA, 1996; pp. 236–247. [Google Scholar]
- Verhaeghen, P.; Salthouse, T.A. Meta-analyses of age-cognition relations in adulthood: Estimates of linear and nonlinear age effects and structural models. Psychol. Bull. 1997, 122, 231–249. [Google Scholar] [CrossRef] [PubMed]
- Dufek, J.; Minarik, B. Age of population and the development of population ageing in the regions of the Czech Republic. Agric. Econ. 2009, 55, 259–270. [Google Scholar] [CrossRef] [Green Version]
- Noja, G.; Cristea, S.; Yüksel, A.; Pânzaru, C.; Drăcea, R. Migrants’ role in enhancing the economic development of host countries: Empirical evidence from Europe. Sustainability 2018, 10, 894. [Google Scholar] [CrossRef] [Green Version]
- Thalassinos, E.; Cristea, M.; Noja, G.G. Measuring active ageing within the European Union: implications on economic development. Equilibrium 2019, 14, 591–609. [Google Scholar] [CrossRef]
- Pirtea, M.; Botoc, C.; Jurcut, C. Risk and return analysis: evidence from emerging markets. Transform. Bus. Econ. 2014, 13, 637–647. [Google Scholar]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristea, M.; Noja, G.G.; Stefea, P.; Sala, A.L. The Impact of Population Aging and Public Health Support on EU Labor Markets. Int. J. Environ. Res. Public Health 2020, 17, 1439. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041439
Cristea M, Noja GG, Stefea P, Sala AL. The Impact of Population Aging and Public Health Support on EU Labor Markets. International Journal of Environmental Research and Public Health. 2020; 17(4):1439. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041439
Chicago/Turabian StyleCristea, Mirela, Gratiela Georgiana Noja, Petru Stefea, and Adrian Lucian Sala. 2020. "The Impact of Population Aging and Public Health Support on EU Labor Markets" International Journal of Environmental Research and Public Health 17, no. 4: 1439. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041439