The Impact of Acute Kidney Injury in the Perioperative Period on the Incidence of Postoperative Delirium in Patients Undergoing Coronary Artery Bypass Grafting—Observational Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
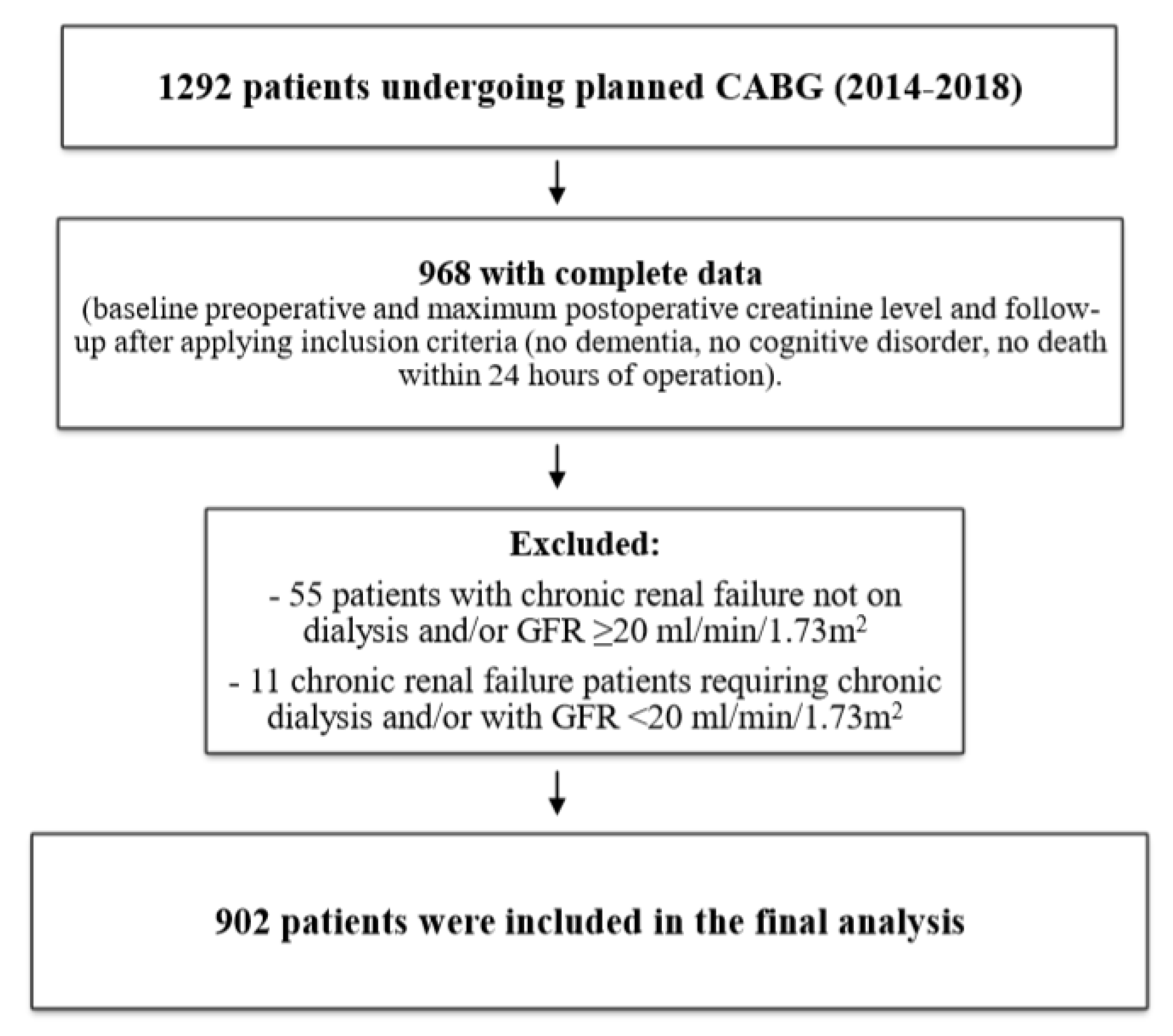
2.1. Study Group and Data Collection
2.2. Delirium Diagnosis
2.3. Acute Kidney Injury Diagnosis
2.4. Ethical Issues
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Data Availability
References
- Yap, S.C.; Lee, H.T. Acute Kidney Injury and Extrarenal Organ Dysfunction: New Concepts and Experimental Evidence. Anesthesiology 2012, 116, 1139–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, R.Y.Y.; Ostermann, M. Acute Kidney Injury and Delirium: Kidney–Brain Crosstalk. In Annual Update in Intensive Care and Emergency Medicine 2019; Vincent, J.L., Ed.; Annual Update in Intensive Care and Emergency Medicine; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Liu, M.; Liang, Y.; Chigurupati, S.; Lathia, J.D.; Pletnikov, M.; Sun, Z.; Crow, M.; Ross, C.A.; Mattson, M.P.; Rabb, H. Acute kidney injury leads to inflammation and functional changes in the brain. J. Am. Soc. Nephrol. 2008, 19, 1360–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burkhart, C.S.; Dell-Kuster, S.; Gamberini, M.; Moeckli, A.; Grapow, M.; Filipovic, M.; Seeberger, M.D.; Monsch, A.U.; Strebel, S.P.; Steiner, L.A. Modifiable and nonmodifiable risk factors for postoperative delirium after cardiac surgery with cardiopulmonary bypass. J. Cardiothorac. Vasc. Anesth. 2010, 24, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Kotfis, K.; Marra, A.; Ely, E.W. ICU delirium—A diagnostic and therapeutic challenge in the intensive care unit. Anaesthesiol. Intensive Ther. 2018, 50, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Marra, A.; Kotfis, K.; Hosie, A.; MacLullich, A.M.J.; Pandharipande, P.P.; Ely, E.W.; Pun, B.T. Delirium Monitoring: Yes or No? That Is the Question. Am. J. Crit. Care 2019, 28, 127–135. [Google Scholar] [CrossRef]
- Kotfis, K.; Zegan-Barańska, M.; Żukowski, M.; Kusza, K.; Kaczmarczyk, M.; Ely, E.W. Multicenter assessment of sedation and delirium practices in the intensive care units in Poland—Is this common practice in Eastern Europe? BMC Anesthesiol. 2017, 17, 120. [Google Scholar] [CrossRef]
- Siew, E.D.; Fissell, W.H.; Tripp, C.M.; Blume, J.D.; Wilson, M.D.; Clark, A.J.; Vincz, A.J.; Ely, E.W.; Pandharipande, P.P.; Girard, T.D. Acute Kidney Injury as a Risk Factor for Delirium and Coma during Critical Illness. Am. J. Respir. Crit. Care Med. 2017, 195, 1597–1607. [Google Scholar] [CrossRef]
- Pisani, M.A.; Murphy, T.E.; Van Ness, P.H.; Araujo, K.L.; Inouye, S.K. Characteristics associated with delirium in older patients in a medical intensive care unit. Arch. Intern. Med. 2007, 167, 1629–1634. [Google Scholar] [CrossRef] [Green Version]
- Kotfis, K.; Szylińska, A.; Listewnik, M.; Strzelbicka, M.; Brykczyński, M.; Rotter, I.; Żukowski, M. Early delirium after cardiac surgery: an analysis of incidence and risk factors in elderly (≥65 years) and very elderly (≥80 years) patients. Clin. Interv. Aging 2018, 13, 1061–1070. [Google Scholar] [CrossRef] [Green Version]
- Grigoryev, D.N.; Liu, M.; Hassoun, H.T.; Cheadle, C.; Barnes, K.C.; Rabb, J. The local and systemic inflammatory transcriptome after acute kidney injury. J. Am. Soc. Nephrol. 2008, 19, 547–558. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Kieman, M.C.; Murray, A.; Rosner, M.H.; Ronco, C. Kidney-brain crosstalk in the acute and chronic setting. Nat. Rev. Nephrol. 2015, 11, 707–719. [Google Scholar] [CrossRef] [PubMed]
- Schopka, S.; Diez, C.; Camboni, D.; Floerchinger, B.; Schmid, C.; Hilker, M. Impact of cardiopulmonary bypass on acute kidney injury following coronary artery bypass grafting: A matched pair analysis. J. Cardiothorac. Surg. 2014, 9, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolpin, D.A.; Collard, C.D.; Lee, V.V.; Virani, S.S.; Allison, P.M.; Elayda, M.A.; Pan, W. Subclinical changes in serum creatinine and mortality after coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 2012, 143, 682–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Kellum, J.A.; Lameire, N.; KDIGO AKI Guideline Work Group. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lassnigg, A.; Schmidlin, D.; Mouhieddine, M.; Bachmann, L.M.; Druml, W.; Bauer, P.; Hiesmay, M. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: A prospective cohort study. J. Am. Soc. Nephrol. 2004, 15, 1597–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acosta-Ochoa, I.; Bustamante-Munguira, J.; Mendiluce-Herrero, A.; Bustamante-Bustamante, J.; Coca-Rojo, A. Impact on Outcomes across KDIGO-2012 AKI Criteria According to Baseline Renal Function. J. Clin. Med. 2019, 8, 1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nongnuch, A.; Panorchan, K.; Davenport, A. Brain–kidney crosstalk. Crit. Care 2014, 18, 225. [Google Scholar] [CrossRef] [Green Version]
- Palkovits, M.; Sebekova, K.; Gallatz, K.; Boor, P.; Sebekova, K., Jr.; Klassen, A.; Bahner, U.; Heidland, A. Neuronal activation in the CNS during different forms of acute renal failure in rats. Neuroscience 2009, 159, 862–882. [Google Scholar] [CrossRef]
- Kelly, K.J. Acute renal failure: much more than a kidney disease. Semin. Nephrol. 2006, 26, 105–113. [Google Scholar] [CrossRef]
- Ratliff, B.B.; Rabadi, M.M.; Vasko, R.; Yasuda, K.; Goligorsky, M.S. Messengers without borders: Mediators of systemic inflammatory response in AKI. J. Am. Soc. Nephrol. 2013, 24, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Biernawska, J.; Bober, J.; Kotfis, K.; Bogacka, A.; Barnik, E.; Żukowski, M. Cardiac surgery related cardio-renal syndrome assessed by conventional and novel biomarkers—Under or overestimated diagnosis? Arch. Med. Sci. 2017, 13, 1111–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Study Group (n = 902) |
|---|---|
| Age (years), mean ± SD | 65.95 ± 8.01 |
| Sex, male, n (%) | 693 (76.83) |
| BMI (kg/m2), mean ± SD | 28.97 ± 4.24 |
| Ejection fraction, mean ± SD | 47.57 ± 9.71 |
| EuroScore Logistic 2 (%), mean ± SD | 1.82 ± 1.57 |
| Concomitant diseases | |
| Current smoking, n (%) | 133 (14.75) |
| Arterial hypertension, n (%) | 680 (75.39) |
| Myocardial infarction, n (%) | 467 (51.77) |
| Heart failure (NYHA III or IV), n (%) | 73 (8.09) |
| Atrial Fibrillation, n (%) | 91 (10.09) |
| Diabetes [insulin], n (%) | 97 (10.75) |
| Diabetes [oral medications/diet], n (%) | 324 (35.92) |
| Impaired glucose tolerance, n (%) | 31 (3.44) |
| Previous stroke, n (%) | 40 (4.43) |
| Transient Ischemic Attack, n (%) | 8 (0.89) |
| Internal Carotid Artery stenosis, n (%) | 66 (7.32) |
| Extracardiac atherosclerosis, n (%) | 156 (17.29) |
| Chronic Obstructive Pulmonary Disease, n (%) | 41 (4.54) |
| Perioperative data | |
| Number of anastomoses, mean ± SD | 3.07 ± 0.76 |
| Crystalloid cardioplegia, n (%) | 886 (98.23) |
| Perfusion time (min), mean ± SD | 49.52 ± 13.51 |
| Cross-clamping time (min), mean ± SD | 29.89 ± 8.94 |
| Intraoperative hemofiltration, n (%) | 141 (15.63) |
| Intra-Aortic Balloon Pump, n (%) | 1 (0.11) |
| Postoperative drainage, mean ± SD | 486.99 ± 395.48 |
| Reoperation (early), n (%) | 32 (3.55) |
| Postoperative outcome | |
| Intubation time (min), mean ± SD | 742.66 ± 858.44 |
| Postoperative delirium, n (%) | 115 (12.75) |
| Hospital LOS (days), mean ± SD | 8.34 ± 6.29 |
| ICU LOS (days), mean ± SD | 2.43 ± 2.92 |
| Mortality until 30 days, n (%) | 9 (0.99) |
| Mortality above 30 days, n (%) | 33 (3.66) |
| Perioperative Laboratory Data | Study Group (n = 902) |
|---|---|
| Baseline CKMB, mean ± SD | 25.86 ± 28.63 |
| Maximum postop CKMB, mean ± SD | 58.24 ± 64.62 |
| Baseline serum creatinine, mean ± SD | 0.91 ± 0.21 |
| Maximum postop serum creatinine, mean ± SD | 1.13 ± 0.49 |
| Baseline GFR (mL/min/1.73 m2), mean ± SD | 82.32 ± 16.02 |
| Minimal postop GFR (mL/min/1.73 m2), mean ± SD | 70.81 ± 22.39 |
| No AKI according to KDIGO, n (%) | 702 (77.83) |
| Any AKI according to KDIGO, n (%) | 200 (22.17) |
| KDIGO Stage 1, n (%) | 159 (17.63) |
| KDIGO Stage 2, n (%) | 30 (3.33) |
| KDIGO Stage 3, n (%) | 11 (1.22) |
| Postoperative CRRT, n (%) | 11 (1.22) |
| Delirium | ||||
|---|---|---|---|---|
| p-Value | OR | CI OR −95% | CI OR +95% | |
| Age | <0.001 | 1.108 | 1.078 | 1.139 |
| BMI | 0.383 | 0.979 | 0.935 | 1.026 |
| Ejection Fraction | 0.372 | 0.991 | 0.971 | 1.011 |
| EuroScore Logistic 2 (%) | <0.001 | 1.303 | 1.180 | 1.440 |
| Number of anastomoses | 0.435 | 1.108 | 0.857 | 1.432 |
| Perfusion time | 0.082 | 1.012 | 0.998 | 1.026 |
| Cross-clamping time | 0.041 | 1.022 | 1.001 | 1.044 |
| Intubation time | 0.638 | 1.000 | 1.000 | 1.000 |
| Baseline CKMB | 0.018 | 1.006 | 1.001 | 1.011 |
| Maximum postop CKMB | 0.079 | 1.002 | 1.000 | 1.004 |
| Postoperative Drainage | 0.240 | 1.000 | 1.000 | 1.001 |
| Hospital LOS | <0.001 | 1.069 | 1.036 | 1.104 |
| ICU LOS | 0.215 | 1.031 | 0.983 | 1.081 |
| Glycated hemoglobin HbA1c | 0.001 | 1.306 | 1.108 | 1.538 |
| Baseline creatinine | 0.003 | 3.362 | 1.502 | 7.527 |
| Baseline GFR (mL/min/1.73 m2) | <0.001 | 0.969 | 0.958 | 0.980 |
| Maximum postop creatinine | <0.001 | 2.907 | 2.087 | 4.049 |
| Minimal postop GFR (mL/min/1.73 m2) | <0.001 | 0.967 | 0.959 | 0.976 |
| Sex, female | 0.015 | 1.696 | 1.108 | 2.598 |
| Current smoking | 0.166 | 0.641 | 0.342 | 1.202 |
| Heart failure NYHA III and IV | 0.006 | 2.264 | 1.265 | 4.053 |
| Previous stroke | 0.360 | 1.481 | 0.639 | 3.431 |
| Transient Ischemic Attack | 0.310 | 2.304 | 0.459 | 11.554 |
| Impaired glucose tolerance | 0.296 | 0.463 | 0.109 | 1.965 |
| Diabetes (oral medications/diet) | 0.072 | 1.440 | 0.969 | 2.142 |
| Diabetes (insulin) | 0.244 | 1.409 | 0.792 | 2.506 |
| Arterial hypertension | 0.018 | 1.886 | 1.112 | 3.196 |
| Myocardial infarction | 0.060 | 1.466 | 0.984 | 2.184 |
| Atrial fibrillation | 0.428 | 1.278 | 0.697 | 2.344 |
| Internal Carotid Artery stenosis | <0.001 | 2.857 | 1.597 | 5.111 |
| Chronic Obstructive Pulmonary Disease | 0.026 | 2.323 | 1.107 | 4.875 |
| Extracardiac atherosclerosis | <0.001 | 2.173 | 1.389 | 3.399 |
| Intraoperative hemofiltration | <0.001 | 2.530 | 1.610 | 3.977 |
| Reoperation (early) | 0.522 | 0.700 | 0.210 | 2.336 |
| KDIGO Stage 1 | <0.001 | 3.300 | 2.106 | 5.172 |
| KDIGO Stage 2 | <0.001 | 5.254 | 2.353 | 11.731 |
| KDIGO Stage 3 | <0.001 | 12.610 | 3.739 | 42.522 |
| p-Value | OR | CI OR −95% | CI OR +95% | |
|---|---|---|---|---|
| Age | <0.001 | 1.078 | 1.046 | 1.111 |
| Internal Carotid Artery stenosis | 0.123 | 1.835 | 0.848 | 3.972 |
| Extracardiac atherosclerosis | 0.303 | 1.369 | 0.753 | 2.486 |
| EuroScore Logistic 2 (%) | 0.060 | 1.118 | 0.995 | 1.255 |
| Intraoperative hemofiltration | 0.047 | 1.683 | 1.008 | 2.810 |
| KDIGO Stage 1 | 0.002 | 2.165 | 1.329 | 3.526 |
| KDIGO Stage 2 | 0.033 | 2.619 | 1.079 | 6.356 |
| KDIGO Stage 3 | 0.003 | 7.241 | 1.960 | 26.758 |
| Hospital LOS | 0.021 | 1.037 | 1.006 | 1.070 |
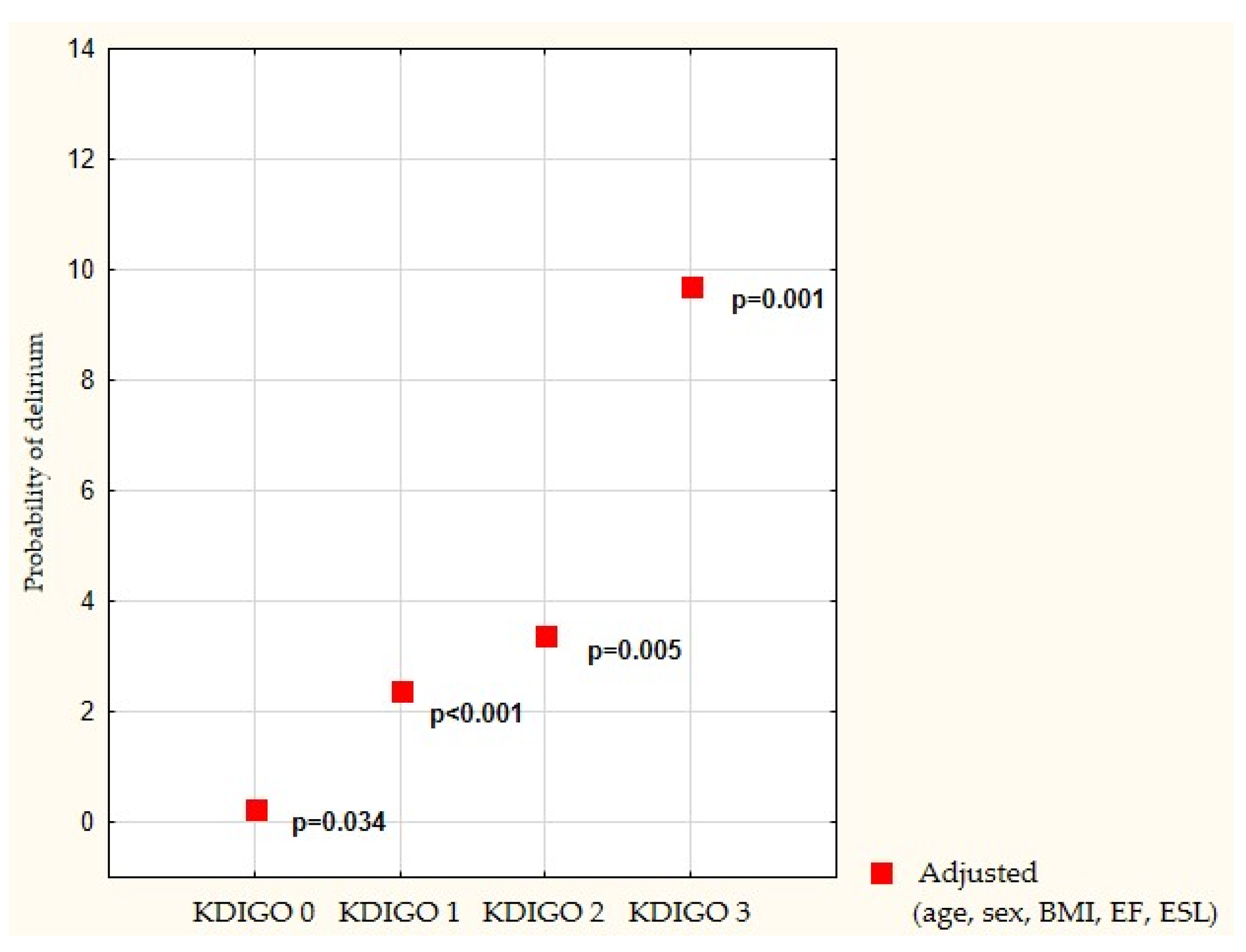
| Delirium Unadjusted | Delirium Adjusted (Age, Sex, BMI, EF, and ESL) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| p-Value | OR | CI OR −95% | CI OR 95% | p-Value | OR | CI OR −95% | CI OR 95% | ||
| KDIGO | Stage 1 | <0.001 | 3.300 | 2.106 | 5.172 | <0.001 | 2.401 | 1.484 | 3.884 |
| Stage 2 | <0.001 | 5.254 | 2.353 | 11.731 | 0.005 | 3.387 | 1.459 | 7.866 | |
| Stage 3 | <0.001 | 12.610 | 3.739 | 42.522 | 0.001 | 9.729 | 2.675 | 35.382 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotfis, K.; Ślozowska, J.; Listewnik, M.; Szylińska, A.; Rotter, I. The Impact of Acute Kidney Injury in the Perioperative Period on the Incidence of Postoperative Delirium in Patients Undergoing Coronary Artery Bypass Grafting—Observational Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 1440. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041440
Kotfis K, Ślozowska J, Listewnik M, Szylińska A, Rotter I. The Impact of Acute Kidney Injury in the Perioperative Period on the Incidence of Postoperative Delirium in Patients Undergoing Coronary Artery Bypass Grafting—Observational Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(4):1440. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041440
Chicago/Turabian StyleKotfis, Katarzyna, Justyna Ślozowska, Mariusz Listewnik, Aleksandra Szylińska, and Iwona Rotter. 2020. "The Impact of Acute Kidney Injury in the Perioperative Period on the Incidence of Postoperative Delirium in Patients Undergoing Coronary Artery Bypass Grafting—Observational Cohort Study" International Journal of Environmental Research and Public Health 17, no. 4: 1440. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041440