Validation of the Portuguese Version of the Healthy Lifestyle Questionnaire

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Participants
2.3. Instruments
2.4. Procedures
2.5. Data Analysis
3. Results
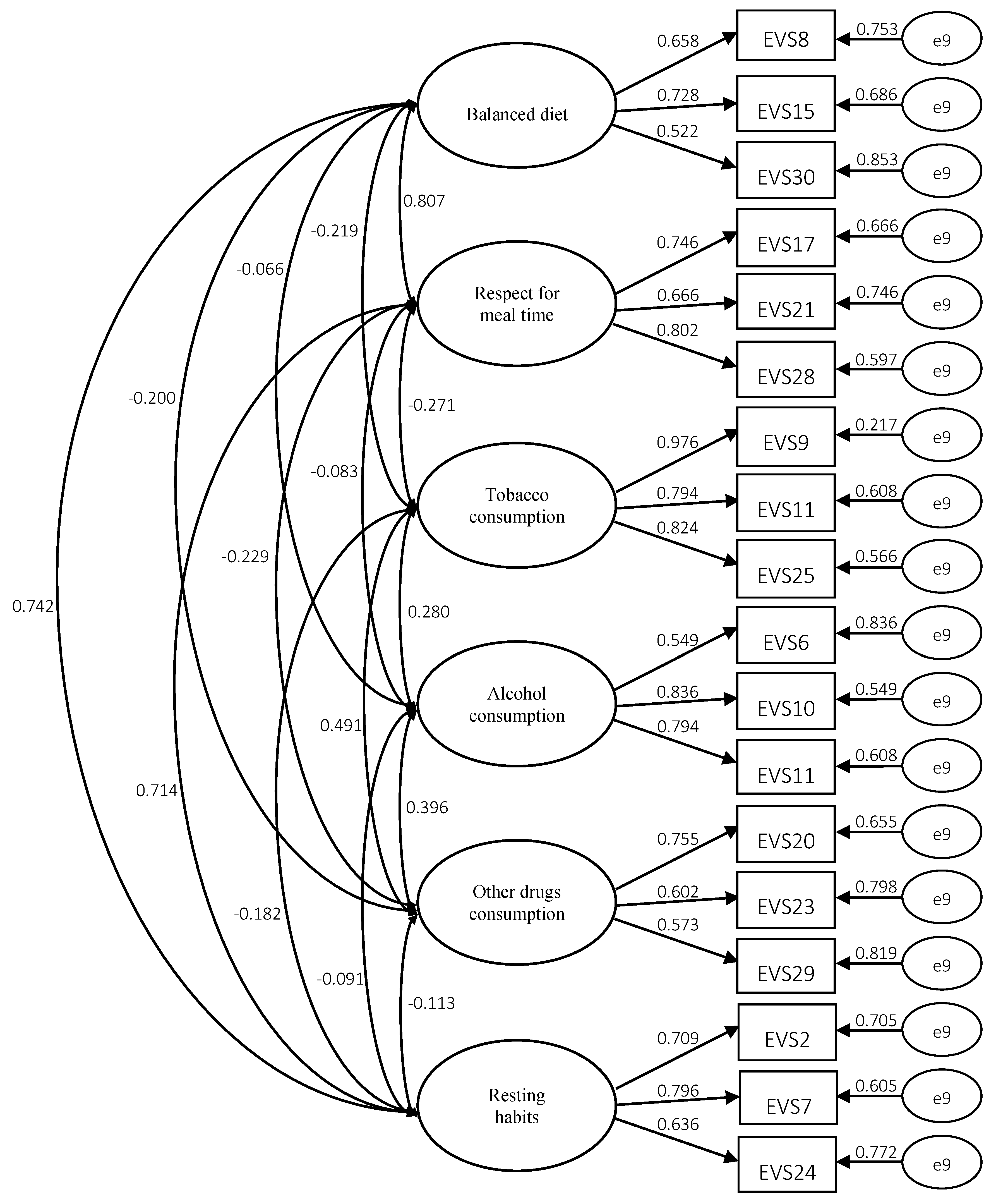
3.1. Confirmatory Factor Analysis
3.2. Analysis of Internal Consistency and Convergent Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Leyton, M.; Batista, M.; Jiménez-Castuera, R. Modelo de predicción de los estilos de vida saludables a través de la teoría de la autodeterminación de estudiantes de educación física. Rev. Psicodidáct. 2020, 25, 68–75. [Google Scholar] [CrossRef]
- Leyton, M.; Lobato, S.; Batista, M.; Aspano, M.; Jiménez-Castuera, R. Validation of the healthy lifestyle questionnaire (EVS) in a Spanish population. Rev. Iberoam. Psicol. Deporte 2018, 1, 23–31. [Google Scholar]
- Pastor, Y.; Balaguer, I.; García-Merita, M.L. Dimensions of health-related lifestyle in adolescence: A review. Rev. Psicol. Gen. Apl. 1998, 51, 469–483. [Google Scholar]
- Olson, D.; McCubbin, H.; Barnes, H.; Larsen, A.; Muxen, M.; Wilson, M. Families Inventories: Inventories used in a National Survey of Families Across the Family Life-Cycle, 2nd ed.; University of Minnesota: St. Paul, MN, USA, 1982. [Google Scholar]
- Diener, E.; Emmons, R.; Larsen, R.; Griffin, S. The Satisfaction with Life Scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Wold, B. Health-Behaviour in Schoolchildren: A WHO Cross-National Survey; Resource Package Questions 1993-4; University of Bergen: Bergen, Norway, 1995. [Google Scholar]
- Jiménez-Castuera, R. Motivación, trato de igualdad, comportamientos de disciplina y estilos de vida saludables en estudiantes de educación física en secundaria. Ph.D. Tesis, Universidad de Extremadura, Extremadura, Cáceres, 2004. [Google Scholar]
- Apostolidou, M. Teachers and health education in Cyprus schools: Historical context, current concerns and perceptions na future development. PhD Thesis, University of Wales, Cardiff, UK, 1999. [Google Scholar]
- Rodríguez, A.; Lemos, S.; Canga, A. Relationship between personality variables. Attitudes toward health and lifestyle. Rev. De Psicol. Gen. Y Apl. 2001, 54, 659–670. [Google Scholar]
- Salazar, I.; Arrivillaga, M. Consumption of alcohol, tobacco, and other drugs as part of the college youth lifestyle. Rev. Colomb. De Psicol. 2004, 13, 74–89. [Google Scholar]
- Grimaldo, M. Manual técnico de la escala de calidad de vida de Barnes y Olson; Universidad de San Martín de Porres: Lima, Peru, 2003. [Google Scholar]
- Ramírez-Vélez, R.; Agredo, R. Fiabilidad y validez del instrumento" Fantástico" para medir el estilo de vida en adultos colombianos. Rev. De Salud Pública 2012, 14, 226–237. [Google Scholar]
- Bennasar, M. Estilos de vida y salud en estudiantes universitarios: La universidad como entorno promotor de la salud. Ph.D. Tesis, Universitat de les Illes Balears, Mallorca, Spain, 2012. [Google Scholar]
- Jiménez-Castuera, R.; Cervelló-Gimeno, E.; García-Calvo, T.; Santos-Rosa, F.; Iglesias-Gallego, D. Estudio de las relaciones entre motivación, práctica deportiva extraescolar y hábitos alimenticios y de descanso en estudiantes de Educación Física. Int. J. Clin. Health Psychol. 2007, 7, 385–401. [Google Scholar]
- Moreno, J.; Moreno, R.; Cervelló, E. El autoconcepto físico como predictor de la intención de ser físicamente activo. Psicol. Y Salud 2007, 17, 261–267. [Google Scholar]
- DeFreese, J.; Smith, A. Teammate social support, burnout, and self-determined motivation in collegiate athletes. Psychol. Sport Exerc. 2013, 14, 258–265. [Google Scholar] [CrossRef]
- Deci, E.; Ryan, R. Self-determination theory. In Handbook of theories social psychology; Kruglanski, A., Van Lange, P., Higgins, E., Eds.; SAGE: London, UK, 2012; pp. 416–437. [Google Scholar] [CrossRef]
- Hagger, M.; Hardcastle, S.; Chater, A.; Mallett, C.; Pal, S.; Chatzisarantis, N. Autonomous and controlled motivational regulations for multiple health-related behaviors: Between- and within-participants analyses. Health Psychol. Behav. Med. 2014, 2, 565–601. [Google Scholar] [CrossRef] [PubMed]
- Leyton, M.; García, M.; Fuentes, G.; Jiménez, C. Analysis of motivational variables and healthy lifestyles in sports center practitioners by gender. Retos 2018, 34, 166–171. [Google Scholar]
- Ruiz-Juan, F.; Isorna, M.; Ruiz-Risueño, J.; Vaquero-Cristóbal, R. Consumo y ingesta de alcohol en españoles mayores de 16 años y su relación con la actividad físico-deportiva, la familia y el consumo de tabaco. Rev. Iberoam. De Psicol. Del Ejerc. Y El Deporte 2014, 9, 339–372. [Google Scholar]
- Aspano, M. Predicción de estilos de vida saludables a través de la teoría de la autodeterminación en adolescentes portugueses. Master’s Thesis, Universidad de Extremadura, Cáceres, Spain, 2015. [Google Scholar]
- Batista, M.; Jiménez, R.; Leyton, M.; Lobato, S.; Aspano, M. Adaptation and validation of the portuguese version of the healthy lifestyles questionnaire. Ponte–Int. Sci. Res. J. 2016, 72, 145–158. [Google Scholar] [CrossRef] [Green Version]
- Montero, I.; León, O.G. A guide for naming research studies in psychology. Int. J. Clin. Health Psychol. 2007, 7, 847–862. [Google Scholar]
- Lonsdale, C.; Hodge, K.; Rose, E. The Behavioral Regulation in Sport Questionnaire (BRSQ): Instrument Development and Initial Validity Evidence. J. Sport Exerc. Psychol. 2008, 30, 323–355. [Google Scholar] [CrossRef]
- Monteiro, D.; Moutão, J.; Cid, L. Validation of the Behavioral Regulation Sport Questionnaire in Portuguese athletes. Rev. De Psicol. Del Deporte 2018, 27, 145–150. [Google Scholar]
- Cubo-Delgado, S.; Martín-Marin, B.; Ramos-Sanchez, J.L. Métodos de Investigación y Análisis de Datos en Ciências Sociales y de la Salud; Madrid Pirâmide: Madrid, Spain, 2011. [Google Scholar]
- Pestana, M.; Gageiro, J. Análise de dados para ciéncias sociais - A complementaridade do SPSS; Edições Silabo: Lisboa, Portugal, 2005. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods Psychol. Res. Online 2003, 8, 23–74. [Google Scholar]
- Satorra, A.; Bentler, P. A scaled difference chi-square test statistic for moment structure analysis. Psychometrika 2001, 66, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Gignac, G.E.; Kretzschmar, A. Evaluating dimensional distinctness with correlated-factor models: Limitations and suggestions. Intelligence 2017, 62, 138–147. [Google Scholar] [CrossRef]
- Revelle, W. Psych: Procedures for Psychological, Psychometric, and Personality Research; Evanston: Illinois, USA, 2014. [Google Scholar]
- Hu, L.; Bentler, P. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Schumacker, R.; Lomax, R. A Beginner’s Guide to Structural Equation Modeling, 3rd ed.; Routledge: New York, NY, USA, 2010. [Google Scholar]
- Ng, J.; Ntoumanis, N.; Thøgersen-Ntoumani, C.; Deci, E.; Ryan, R.; Duda, J.; Williams, G. Self-determination theory applied to health contexts: A meta-analysis. Perspect. Psychol. Sci. 2012, 7, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Leyton, M.; Batista, M.; Lobato, S.; Aspano, M.; Jiménez, R. Application of two intervention programs in order to optimize motivation and to improve eating habits in adult and elderly women. J. Hum. Kinet. 2017, 59, 131–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Item | FL | CF | Ω | MVE | CR | OHS |
|---|---|---|---|---|---|---|---|
| Balanced diet | EVS 8 | 0.741 | 0.837 * | 0.81 | 0.82 | 0.53 | 0.27 |
| EVS 15 | 0.707 | 0.658 * | |||||
| EVS 19 | 0.582 | 0.530 * | |||||
| EVS 26 | 0.639 | 0.630 * | |||||
| EVS 30 | 0.708 | 0.762 * | |||||
| Respect for mealtime | EVS 4 | 0.699 | 0.682 * | 0.90 | 0.91 | 0.71 | 0.36 |
| EVS 17 | 0.787 | 0.852 * | |||||
| EVS 21 | 0.718 | 0.761 * | |||||
| EVS 27 | 0.728 | 0.754 * | |||||
| EVS 28 | 0.851 | 0.975 * | |||||
| Tobacco consumption | EVS 1 | 0.847 | 0.899 * | 0.96 | 0.96 | 0.85 | 0.49 |
| EVS 9 | 0.944 | 0.986 * | |||||
| EVS 14 | 0.865 | 0.848 * | |||||
| EVS 25 | 0.903 | 0.980 * | |||||
| Alcohol consumption | EVS 6 | 0.700 | 0.539 * | 0.76 | 0.79 | 0.51 | 0.35 |
| EVS 10 | 0.827 | 0.940 * | |||||
| EVS 11 | 0.825 | 0.847 * | |||||
| Other drugs consumption | EVS 18 | 0.681 | 0.618 * | 0.78 | 0.78 | 0.51 | 0.27 |
| EVS 20 | 0.776 | 0.742 * | |||||
| EVS 23 | 0.762 | 0.767 * | |||||
| EVS 29 | 0.685 | 0.625 * | |||||
| Resting habits | EVS 2 | 0.828 | 0.823 * | 0.74 | 0.77 | 0.54 | 0.34 |
| EVS 7 | 0.875 | 0.982 * | |||||
| EVS 24 | 0.732 | 0.560 * |
| Variable | Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Balanced diet | 3.63 | 0.80 | - | 0.61 ** | −0.21 ** | −0.49 | −0.13 * | 0.53 ** | 0.14 * | −0.28 ** | −0.34 ** |
| 2. Respect for mealtime | 3.64 | 0.89 | - | −0.27 ** | −0.17 ** | −0.23 ** | 0.61 ** | 0.45 ** | −0.22 ** | −0.09 | |
| 3.Tobacco consumption | 1.57 | 1.02 | - | 0.33 ** | 0.42 ** | −0.17 ** | −0.14 * | 0.20 ** | 0.13 * | ||
| 4.Alcohol consumption | 1.52 | 0.68 | - | 0.41 ** | −0.08 | -0.11 * | 0.11 * | 0.05 | |||
| 5.Other drugs consumption | 1.55 | 0.74 | - | −0.12 * | −0.01 | 0.18 ** | 0.11 * | ||||
| 6.Resting habits | 3.40 | 0.93 | - | 0.10 * | −0.11 * | −0.11 * | |||||
| 7. Autonomous motivation | 5.43 | 0.89 | - | −0.21 ** | −0.31 ** | ||||||
| 8. Controlled motivation | 1.99 | 1.07 | - | 0.76 ** | |||||||
| 9.Amotivation | 2.02 | 1.20 | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batista, M.; Leyton-Román, M.; Honório, S.; Santos, J.; Jiménez-Castuera, R. Validation of the Portuguese Version of the Healthy Lifestyle Questionnaire. Int. J. Environ. Res. Public Health 2020, 17, 1458. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041458
Batista M, Leyton-Román M, Honório S, Santos J, Jiménez-Castuera R. Validation of the Portuguese Version of the Healthy Lifestyle Questionnaire. International Journal of Environmental Research and Public Health. 2020; 17(4):1458. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041458
Chicago/Turabian StyleBatista, Marco, Marta Leyton-Román, Samuel Honório, Jorge Santos, and Ruth Jiménez-Castuera. 2020. "Validation of the Portuguese Version of the Healthy Lifestyle Questionnaire" International Journal of Environmental Research and Public Health 17, no. 4: 1458. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041458