Psychometric Analysis and Effectiveness of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire on Injured Soccer Players

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrument
2.3. Measurement Properties
2.4. Procedure
2.5. Data Analysis
2.5.1. Psychometric Properties
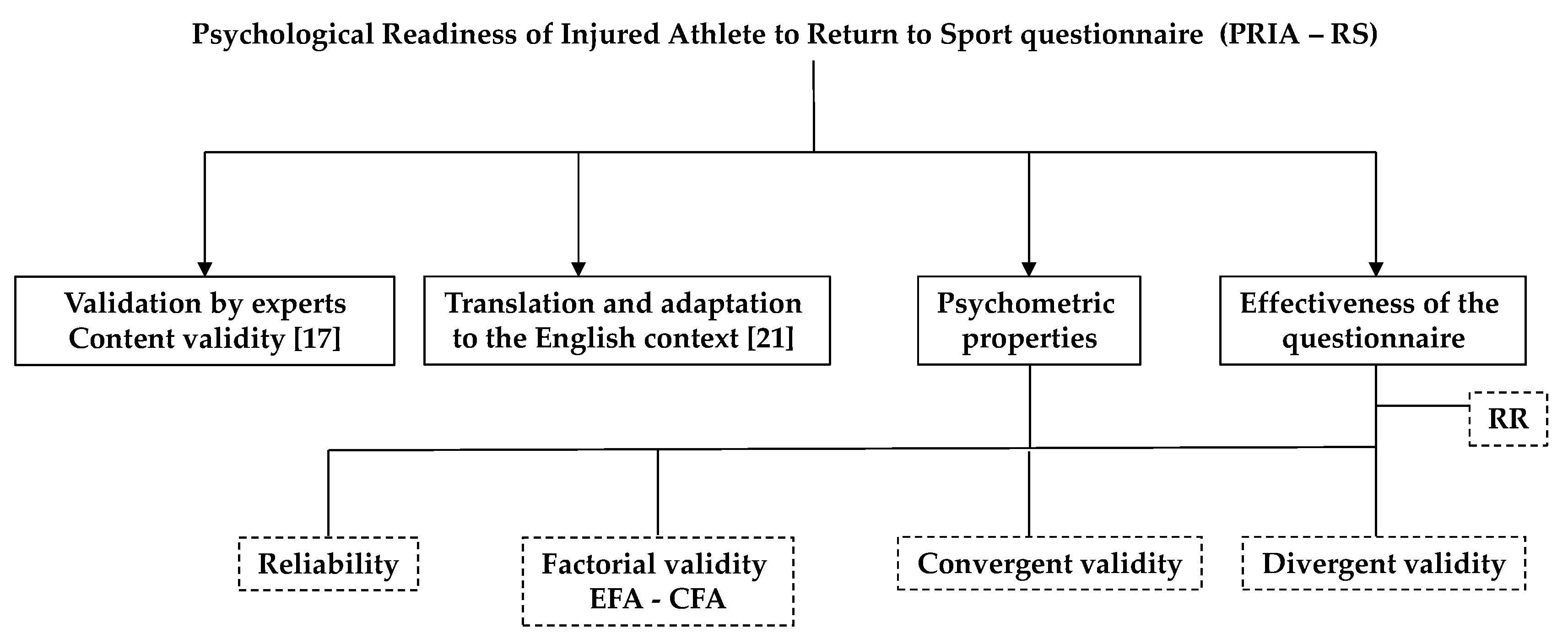
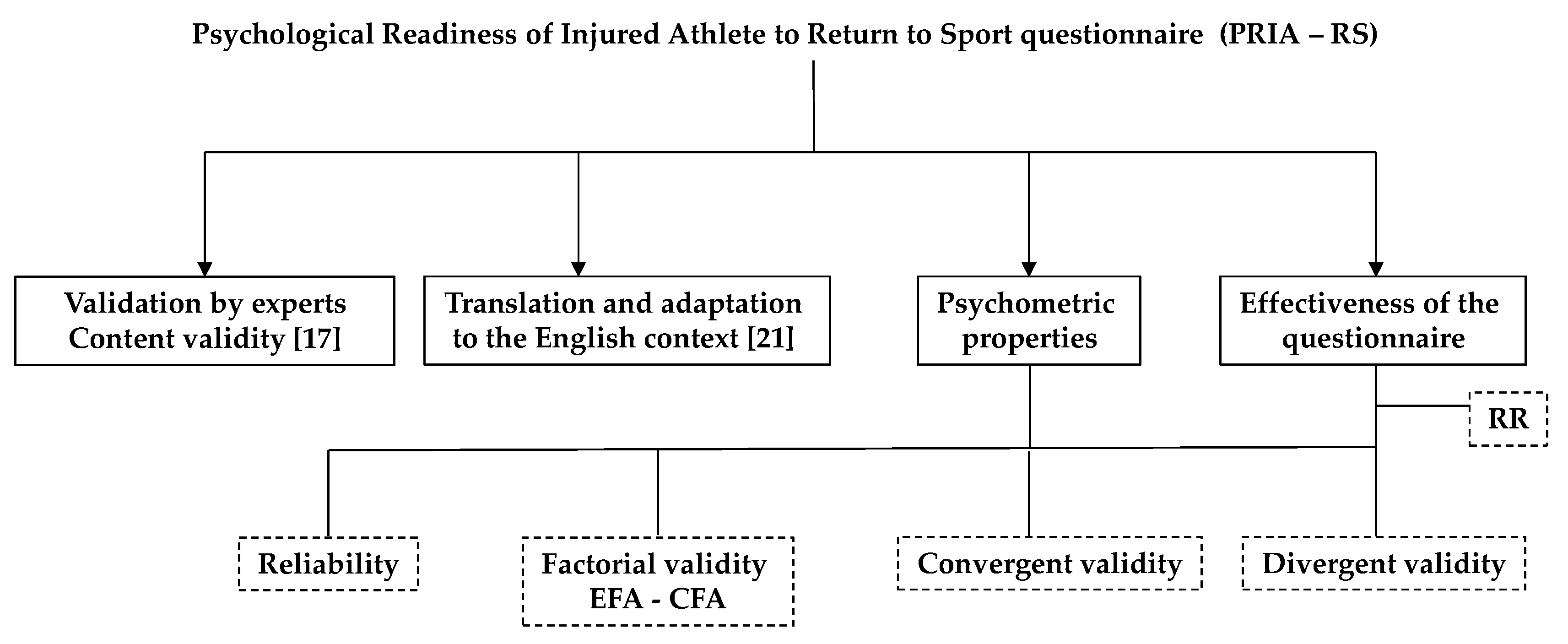
2.5.2. Validity and Effectiveness
2.5.3. Reliability
3. Results
3.1. Convergent Validity
3.2. Divergent Validity
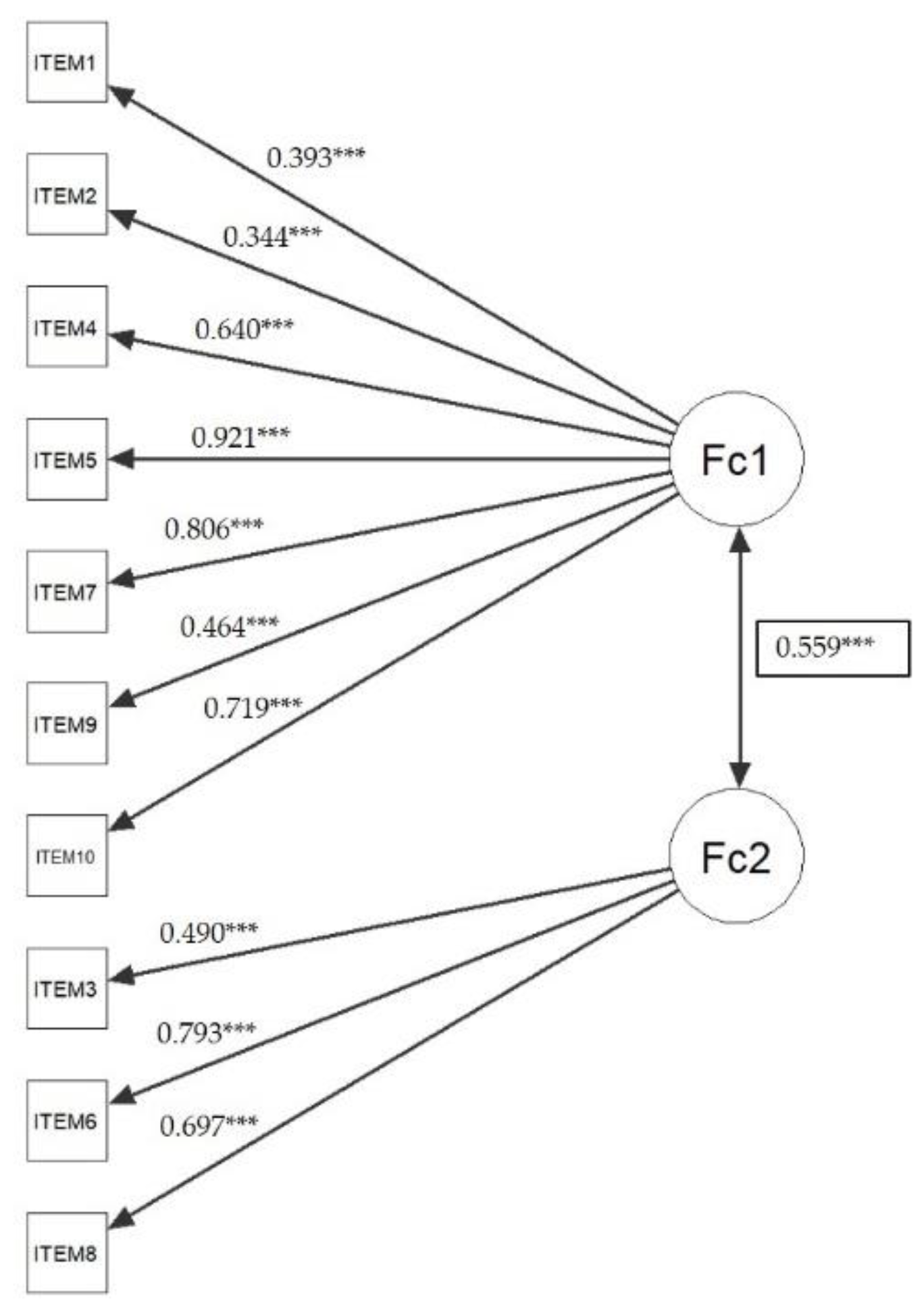
3.3. Structural Validity
3.4. Internal Consistency
3.5. External Psychometric Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Åman, M.; Forssblad, M.; Henriksson-Larsén, K. Incidence and severity of reported acute sports injuries in 35 sports using insurance registry data. Scand. J. Med. Sci. Sports 2016, 26, 451–462. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gómez, A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Injury incidence and distribution in elite football—A prospective study of the Danish and the Swedish top divisions. Scand. J. Med. Sci. Sports 2005, 15, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stubbe, J.H.; van Beijsterveldt, A.M.M.; van der Knaap, S.; Stege, J.; Verhagen, E.A.; Van Mechelen, W.; Backx, F.J. Injuries in professional male soccer players in the Netherlands: A prospective cohort study. J. Athl. Train. 2015, 50, 211–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fear of re-injury in people who have returned to sport following anterior cruciate ligament reconstruction surgery. J. Sci. Med. Sport 2012, 15, 488–495. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. A systematic review of the psychological factors associated with returning to sport following injury. Br. J. Sports Med. 2013, 47, 1120–1126. [Google Scholar] [CrossRef]
- Forsdyke, D.; Smith, A.; Jones, M.; Gledhill, A. Psychosocial factors associated with outcomes of sports injury rehabilitation in competitive athletes: A mixed studies systematic review. Br. J. Sports Med. 2016, 50, 537–544. [Google Scholar] [CrossRef]
- Hsu, C.-J.; Meierbachtol, A.; George, S.Z.; Chmielewski, T.L. Fear of reinjury in athletes. Sports Health 2017, 9, 162–167. [Google Scholar] [CrossRef] [Green Version]
- Sonesson, S.; Kvist, J.; Ardern, C.; Österberg, A.; Silbernagel, K.G. Psychological factors are important to return to pre-injury sport activity after anterior cruciate ligament reconstruction: Expect and motivate to satisfy. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1375–1384. [Google Scholar] [CrossRef]
- Wiese-Bjornstal, D.M.; Smith, A.M.; Shaffer, S.M.; Morrey, M.A. An integrated model of response to sport injury: Psychological and sociological dynamics. J. Appl. Sport Psychol. 1998, 10, 46–69. [Google Scholar] [CrossRef] [Green Version]
- Morrey, M.A.; Stuart, M.J.; Smith, A.M.; Wiese-Bjornstal, D.M. A longitudinal examination of athletes’ emotional and cognitive responses to anterior cruciate ligament injury. Clin. J. Sport Med. 1999, 9, 63–69. [Google Scholar] [CrossRef]
- Clement, D.; Arvinen-Barrow, M.; Fetty, T. Psychosocial responses during different phases of sport-injury rehabilitation: A qualitative study. J. Athl. Train. 2015, 50, 95–104. [Google Scholar] [CrossRef]
- Podlog, L.; Wadey, R.; Stark, A.; Lochbaum, M.; Hannon, J.; Newton, M. An adolescent perspective on injury recovery and the return to sport. Psychol. Sport Exerc. 2013, 14, 437–446. [Google Scholar] [CrossRef]
- McPherson, A.L.; Feller, J.A.; Hewett, T.E.; Webster, K.E. Smaller change in psychological readiness to return to sport is associated with second anterior cruciate ligament injury among younger patients. Am. J. Sports Med. 2019, 47, 1209–1215. [Google Scholar] [CrossRef]
- Ardern, C.L.; Glasgow, P.; Schneiders, A.; Witvrouw, E.; Clarsen, B.; Cools, A.; Bizzini, M. Consensus statement on return to sport from the First World Congress in Sports Physical. Br. J. Sports Med. 2016, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Dijkstra, H.P.; Pollock, N.; Chakraverty, R.; Ardern, C.L. Return to play in elite sport: A shared decision-making process. Br. J. Sports Med. 2017, 51, 853–864. [Google Scholar] [CrossRef]
- Gómez-Piqueras, P.; Sainz de Baranda, P.; Ortega, E.; Contreras, O.; Olmedilla, A. Design and validation of a questionnaire on the perception of the athlete regarding his return to training after injury. Rev. Psicol. Deporte 2014, 23, 479–487. [Google Scholar]
- Glazer, D. Development and preliminary validation of the injury-psychological readiness to return to sport (I-PRRS) scale. J. Athl. Train. 2009, 44, 185–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, N.; Thatcher, J.; Lavallee, D. A preliminary development of the Re-Injury Anxiety Inventory (RIAI). Phys. Ther. Sport 2010, 11, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Feller, J.A.; Lambros, C. Development and preliminary validation of a scale to measure the psychological impact of returning to sport following anterior cruciate ligament reconstruction surgery. Phys. Ther. Sport 2008, 9, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Piqueras, P.; Ruiz-Barquín, R.; Olmedilla, A. Translation and adaptation to English of a questionnaire to determine the Psychological readiness of the injured football player. Rev. Psicol. Deporte 2019, 29, 39–48. [Google Scholar]
- Faulkner, J. Physiology of Swimming and Diving; Academic Press: Baltimore, MD, USA, 1968. [Google Scholar]
- Calvert, M.; Brundage, M.; Jacobsen, P.B.; Schünemann, H.J.; Efficace, F. The CONSORT Patient-Reported Outcome (PRO) extension: Implications for clinical trials and practice. Health Qual. Life Outcomes 2013, 11, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valderas, J.M.; Ferrer, M.; Mendívil, J.; Garin, O.; Rajmil, L.; Herdman, M. Scientific Committee on “patient-reported outcomes” of the Iryss network. development of empro: A tool for the standardized assessment of patient-reported outcome measures. Value Health 2008, 11, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand. J. Med. Sci. Sports 2006, 16, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Maratia, S.; Cedillo, S.; Rejas, J. Assessing health-related quality of life in patients with breast cancer: A systematic and standardized comparison of available instruments using the EMPRO tool. Qual. Life Res. 2016, 25, 2467–2480. [Google Scholar] [CrossRef]
- Schmidt, S.; Ferrer, M.; González, M.; González, N.; Valderas, J.M.; Alonso, J. EMPRO Group. Evaluation of shoulder-specific patient-reported outcome measures: A systematic and standardized comparison of available evidence. J. Shoulder Elbow Surg. 2014, 23, 434–444. [Google Scholar] [CrossRef]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar] [CrossRef]
- Batterham, A.M.; Hopkins, W.G. Making meaningful inferences about magnitudes. Int. J. Sports Physiol. Perform. 2006, 1, 50–57. [Google Scholar] [CrossRef]
- Villa Rodríguez, J.A. IBM SPSS: Análisis Estadístico; CreateSpace Independent Publishing Platform: Seattle, WA, USA, 2014. [Google Scholar]
- Aedo, S.; Pavlov, S.; Clavero, F. Riesgo relativo y Odds ratio ¿Qué son y cómo se interpretan? Rev. Obs. Ginecol. 2010, 5, 51–54. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K.A., Long, J.S., Eds.; Sage: Newbury Park, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis, 6th ed.; Pearson-Prentice Hall: Upper Saddle River, NJ, USA, 2006. [Google Scholar]
- Jöreskog, K. Statistical analysis of sets of congeneric test. Psychometrika 1971, 36, 109–133. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D. Structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Johnston, L.H.; Carroll, D. The context of emotional responses to athletic injury: A qualitative analysis. J. Sport Rehabil. 1998, 7, 206–220. [Google Scholar] [CrossRef]
- Bekker, S.; Clark, A. Bringing complexity to sports injury prevention research: From simplification to explanation. Br. J. Sports Med. 2016, 50, 1489–1490. [Google Scholar] [CrossRef]
- Bittencourt, N.; Meeuwssie, W.; Mendonca, L.; Netter-Aguirre, A.; Ocarino, J.; Fonseca, S. Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition—Narrative review and new concept. Br. J. Sports Med. 2016, 50, 1309–1314. [Google Scholar] [CrossRef] [Green Version]
- Garin, O.; Herdman, M.; Vilagut, G.; Ferrer, M.; Ribera, A.; Rajmil, L.; Alonso, J. Assessing health-related quality of life in patients with heart failure: A systematic, standardized comparison of available measures. Heart Fail. Rev. 2014, 19, 359–367. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; de Vet, H.C.W. The cosmin checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danner, D.; Aichholzer, J.; Rammstedt, B. Acquiescence in personality questionnaires: Relevance, domain specificity, and stability. J. Res. Pers. 2015, 57, 119–130. [Google Scholar] [CrossRef]
- Ferrando, P.J.; Morales-Vives, F.; Lorenzo-Seva, U. Assessing and controlling acquiescent responding when acquiescence and content are related: A comprehensive factor-analytic approach. Struct. Equ. Model. 2016, 23, 713–725. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- Bauman, J. Returning to play: The mind does matter. Clin. J. Sport Med. 2005, 15, 432–435. [Google Scholar] [CrossRef] [PubMed]
- Everhart, J.S.; Best, T.M.; Flanigan, D.C. Psychological predictors of anterior cruciate ligament reconstruction outcomes: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 752–762. [Google Scholar] [CrossRef]
- Van der Horst, N.; Backx, F.; Goedhart, E.A.; Huisstede, B.M. Return to play after hamstring injuries in football (soccer): A worldwide Delphi procedure regarding definition, medical criteria and decision-making. Br. J. Sports Med. 2017, 51, 1583–1591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zambaldi, M.; Beasley, I.; Rushton, A. Return to play criteria after hamstring muscle injury in professional football: A Delphi consensus study. Br. J. Sports Med. 2017, 51, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R. Why screening tests to predict injury do not work—And probably never will: A critical review. Br. J. Sports Med. 2016, 50, 776–780. [Google Scholar] [CrossRef] [Green Version]
- Olmedilla, A.; Rubio, V.J.; Ortega, E.; García-Mas, A. Effectiveness of a stress management pilot program aimed at reducing the incidence of sports injuries in young football (soccer) players. Phys. Ther. Sport 2017, 24, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García, J.A.; Landa, V.; Trigueros, M.C.; Gaminde, I. Texas revised inventory of grief: Adaptation to spanish, reliability and validity. Rev. Col. Psiquiatr. 2005, 35, 353–358. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Re-Injury (n = 23) | Non Re-Injury (n = 88) | p | ES | |
|---|---|---|---|---|
| Absence days 2 | 28.09 ± 28.32 | 24.82 ± 24.71 | 0.58 | 0.13 |
| Age 1 | 24.83 ± 3.15 | 25.23 ± 3.36 | 0.60 | 0.12 |
| Height (m) 1 | 1.76 ± 0.06 | 1.77 ± 0.05 | 0.24 | 0.18 |
| Weight (kg) 2 | 74.30 ± 4.17 | 74.58 ± 3.67 | 0.91 | 0.07 |
| Years of experience 1 | 17.78 ± 3.10 | 18.06 ± 3.33 | 0.72 | 0.08 |
| Offensive players * Defensive players * | 11 | 37 | 0.61 | chi-square |
| 12 | 51 | |||
| Joint/ligament injury Muscle/tendon injury | 7 | 41 | 0.16 | chi-square |
| 16 | 47 |
| Question | M | SD | |
|---|---|---|---|
| 1 | How do you evaluate the progression you have experienced during the rehabilitation/sport functional recovery period since your injury? | 4.59 | 0.52 |
| 2 | How is your mood? | 4.75 | 0.43 |
| 3 | What is your physical state in view of a potential return to the team? | 4.33 | 0.66 |
| 4 | How do you evaluate the functional status of your damaged area? | 4.38 | 0.66 |
| 5 | Do you feel any discomfort or limitations that prevent you from training as normal? | 4.24 | 1.26 |
| 6 | Are you feeling nervous about returning to regular training with the team? | 4.82 | 0.63 |
| 7 | How secure do you feel when performing physical actions or movements in the injured area? | 4.40 | 0.75 |
| 8 | Give an estimated percentage of how likely you are to experience a recurrence of the injury soon | 4.95 | 0.22 |
| 9 | What level of pressure do you feel in your surroundings to return to training with the team? | 4.92 | 0.27 |
| 10 | How would you evaluate your overall condition in view of a potential return to full training? | 4.73 | 0.48 |
| Total Score | ||
|---|---|---|
| Coef. | Sig. | |
| Question 1 | 0.47 | 0.00 |
| Question 2 | 0.40 | 0.00 |
| Question 3 | 0.51 | 0.00 |
| Question 4 | 0.73 | 0.00 |
| Question 5 | 0.87 | 0.00 |
| Question 6 | 0.61 | 0.00 |
| Question 7 | 0.80 | 0.00 |
| Question 8 | 0.45 | 0.00 |
| Question 9 | 0.46 | 0.00 |
| Question 10 | 0.73 | 0.00 |
| Self-Perception Return to Sport | ||||
|---|---|---|---|---|
| Re-Injury n = 23 | Non Re-Injury n = 88 | p | ES | |
| Question 1 | 4.17 ± 0.57 | 4.70 ± 0.45 | 0.00 | 1.03 |
| Question 2 | 4.35 ± 0.48 | 4.85 ± 0.35 | 0.00 | 1.19 |
| Question 3 | 4.09 ± 0.73 | 4.40 ± 0.63 | 0.04 | 0.45 |
| Question 4 | 3.61 ± 0.58 | 4.58 ± 0.51 | 0.00 | 1.77 |
| Question 5 | 2.22 ± 0.99 | 4.77 ± 0.63 | 0.00 | 3.07 |
| Question 6 | 4.30 ± 1.14 | 4.95 ± 0.30 | 0.00 | 0.77 |
| Question 7 | 3.39 ± 0.58 | 4.66 ± 0.54 | 0.00 | 2.26 |
| Question 8 | 4.91 ± 0.28 | 4.95 ± 0.20 | 0.43 | 0.16 |
| Question 9 | 4.70 ± 0.47 | 4.98 ± 0.15 | 0.00 | 0.80 |
| Question 10 | 4.13 ± 0.54 | 4.89 ± 0.31 | 0.00 | 1.72 |
| TOTAL SCORE | 39.78 ± 2.31 | 47.74 ± 2.33 | 0.00 | 3.43 |
| Ranks | Re-Injury n = 23 | Non Re-Injury n = 88 | Chi-Square x2 | RR (CI) | |
|---|---|---|---|---|---|
| Question 1 | ≤3 | 2 | 0 | 0.00 * | - |
| >3 | 21 | 88 | |||
| Question 2 | ≤3 | 0 | 0 | - | - |
| >3 | 23 | 88 | |||
| Question 3 | ≤3 | 5 | 7 | 0.058 | 3.21 (0.9–11.2) |
| >3 | 18 | 81 | |||
| Question 4 | ≤3 | 10 | 1 | 0.00 * | 66.92 (7.9–566.9) ** |
| >3 | 13 | 87 | |||
| Question 5 | ≤3 | 23 | 10 | 0.00* | - |
| >3 | 0 | 78 | |||
| Question 6 | ≤3 | 7 | 2 | 0.00 * | 18.8 (3.5–98.9) ** |
| >3 | 16 | 86 | |||
| Question 7 | ≤3 | 15 | 3 | 0.00 * | 53.12 (12.6–223.3) ** |
| >3 | 8 | 85 | |||
| Question 8 | >60% | 0 | 0 | - | - |
| ≤60% | 23 | 88 | |||
| Question 9 | ≤3 | 0 | 0 | - | - |
| >3 | 23 | 88 | |||
| Question 10 | ≤3 | 1 | 0 | 0.04 * | - |
| >3 | 22 | 88 | |||
| Total score | ≤40 | 12 | 2 | 0.00 * | 46.90 (9.2–237.7) ** |
| >40 | 11 | 86 |
| Question | Factor 1 | Factor 2 |
|---|---|---|
| Question 1 | 0.41 | |
| Question 2 | 0.44 | |
| Question 3 | 0.46 | |
| Question 4 | 0.55 | |
| Question 5 | 0.91 | |
| Question 6 | 0.61 | |
| Question 7 | 0.67 | |
| Question 8 | 0.81 | |
| Question 9 | 0.34 | |
| Question 10 | 0.67 |
| Question | M | Sd | Item–Rest Correlation | If Item Dropped Cronbach’s α |
|---|---|---|---|---|
| Question 1 | 3.41 | 0.529 | 0.374 | 0.801 |
| Question 2 | 4.25 | 0.436 | 0.296 | 0.807 |
| Question 3 | 3.67 | 0.665 | 0.378 | 0.802 |
| Question 4 | 3.62 | 0.661 | 0.641 | 0.772 |
| Question 5 | 1.76 | 1.266 | 0.755 | 0.770 |
| Question 6 | 1.18 | 0.635 | 0.508 | 0.788 |
| Question 7 | 3.60 | 0.754 | 0.719 | 0.759 |
| Question 8 | 4.05 | 0.227 | 0.414 | 0.805 |
| Question 9 | 4.08 | 0.274 | 0.412 | 0.803 |
| Question 10 | 3.27 | 0.485 | 0.670 | 0.777 |
| Question | Variance Extracted | Composite Reliability |
|---|---|---|
| Factor 1 | 0.401 | 0.810 |
| Factor 2 | 0.609 | 0.647 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Piqueras, P.; Ardern, C.; Prieto-Ayuso, A.; Robles-Palazón, F.J.; Cejudo, A.; Sainz de Baranda, P.; Olmedilla, A. Psychometric Analysis and Effectiveness of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire on Injured Soccer Players. Int. J. Environ. Res. Public Health 2020, 17, 1536. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051536
Gómez-Piqueras P, Ardern C, Prieto-Ayuso A, Robles-Palazón FJ, Cejudo A, Sainz de Baranda P, Olmedilla A. Psychometric Analysis and Effectiveness of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire on Injured Soccer Players. International Journal of Environmental Research and Public Health. 2020; 17(5):1536. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051536
Chicago/Turabian StyleGómez-Piqueras, Pedro, Clare Ardern, Alejandro Prieto-Ayuso, Francisco Javier Robles-Palazón, Antonio Cejudo, Pilar Sainz de Baranda, and Aurelio Olmedilla. 2020. "Psychometric Analysis and Effectiveness of the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) Questionnaire on Injured Soccer Players" International Journal of Environmental Research and Public Health 17, no. 5: 1536. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051536