A Linked Community and Health Facility Intervention to Improve Newborn Health in Cambodia: The NICCI Stepped-Wedge Cluster-Randomized Controlled Trial

 ,
,
Abstract
:1. Background
2. Methods
2.1. Objectives
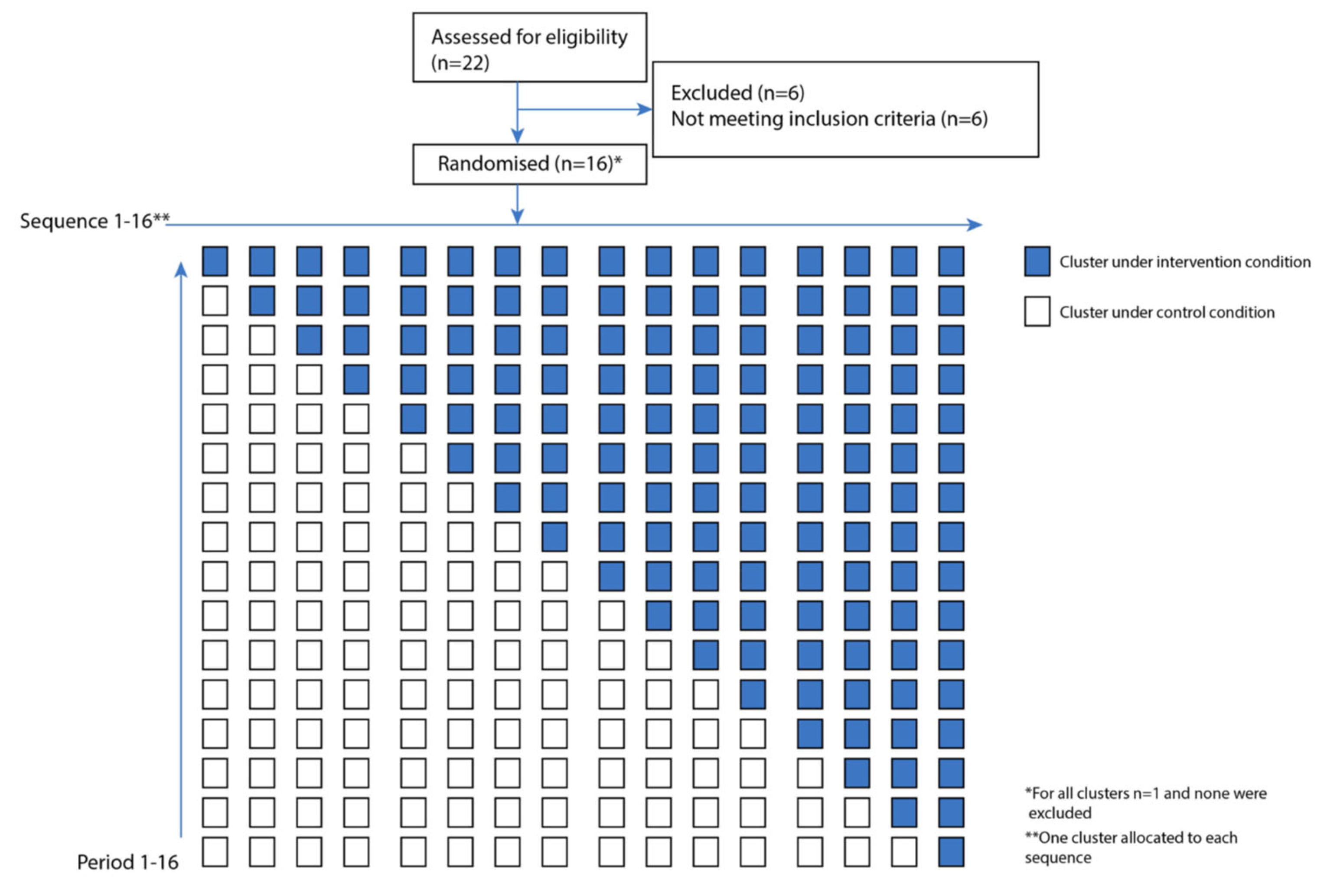
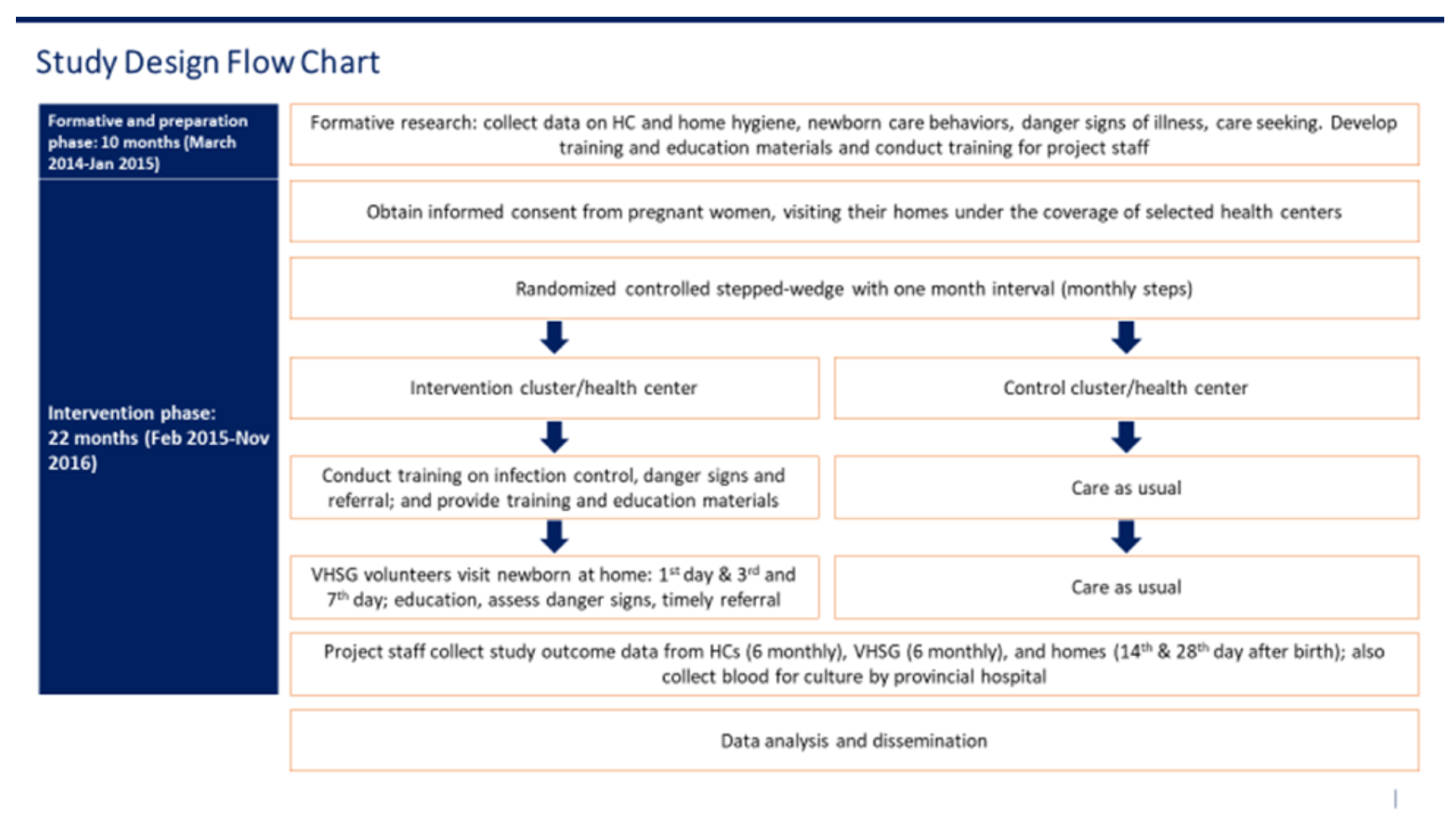
2.2. Trial Design
- % of mothers/caregivers who know at least three danger signs of newborn illness
- % VHSG who know six danger signs of newborn illness
- % of caregivers who seek care from an appropriate facility
- Time between onset of suspected danger signs and referral to appropriate facility
- Improved infection control behavior among HC staff
- % of newborns visited by VHSG within the first day of life
- % of newborns visited by VHSG after the first day of life
- % VHSG who can deliver hygiene messages
- % of mothers who received messages on hygiene from HC staff
- % of mothers who received messages on hygiene from VHSG
- % of mothers who received messages on care-seeking from VHSG
- % HC staff who know six danger signs of newborn illness
- % HC staff who recall hygiene messages
2.3. Sample Size
2.4. Participants
2.5. Randomization
2.6. Implementation, Care Coordination and Data Collection
2.7. Statistical Methods and Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lawn, J.E.; Kerber, K.; Enweronu-Laryea, C.; Cousens, S. 3.6 Million Neonatal Deaths—What Is Progressing and What Is not? In Seminars in Perinatology; WB Saunders: Philadelphia, PA, USA, 2010; Volume 34, pp. 371–386. [Google Scholar]
- Lawn, J.E.; Bahl, R.; Bergström, S.; Bhutta, Z.A.; Darmstadt, G.L.; Ellis, M.; English, M.; Kurinczuk, J.J.; Lee, A.C.C.; Merialdi, M.; et al. Setting Research Priorities to Reduce Almost One Million Deaths from Birth Asphyxia by 2015. PLoS Med. 2011, 8, e1000389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawn, J.E.; Cousens, S.; Zupan, J. 4 million neonatal deaths: When? Where? Why? Lancet 2005, 365, 891–900. [Google Scholar] [CrossRef]
- E Black, R.; Cousens, S.; Johnson, H.L.; E Lawn, J.; Rudan, I.; Bassani, D.G.; Jha, P.; Campbell, H.; Walker, C.F.; Cibulskis, R.; et al. Global, regional, and national causes of child mortality in 2008: A systematic analysis. Lancet 2010, 375, 1969–1987. [Google Scholar] [CrossRef]
- National Institute of Statistics, Derectorate General for Health, and ICF International. National Insititute of Statistics, Derectorate General for Health, and ICF International Cambodia Demographic Health Survey 2014; National Institute of Statistics, Derectorate General for Health, and ICF International: Phnom Penh, Cambodia; Rockville, MD, USA, 2015.
- Patel, A.; Khatib, M.N.; Kurhe, K.; Bhargava, S.; Bang, A. Impact of neonatal resuscitation trainings on neonatal and perinatal mortality: A systematic review and meta-analysis. BMJ Paediatr. Open 2017, 1, e000183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hibberd, P.L.; Hansen, N.I.; Wang, M.E.; Goudar, S.S.; Pasha, O.; Esamai, F.; Chomba, E.; Garces, A.; Althabe, F.; Derman, R.J.; et al. Trends in the incidence of possible severe bacterial infection and case fatality rates in rural communities in Sub-Saharan Africa, South Asia and Latin America, 2010–2013: A multicenter prospective cohort study. Reprod. Health 2016, 13, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Maternal Child Health Center. Verbal Autopsy Study Svay Rieng; Ministry of Health: Phnom Penh, Cambodia, 2009.
- Bazzano, A.N.; Taub, L.; Oberhelman, R.A.; Var, C. Newborn Care in the Home and Health Facility: Formative Findings for Intervention Research in Cambodia. In Healthcare; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2016; Volume 4, p. 94. [Google Scholar]
- National Institute of Statistics, Directorate General for Health, and ICF Macro. National Institute of Statistics, Directorate General for Health and ICF Macro, 2011, Cambodia Demographic and Health Survey; National Institute of Statistics, Directorate General for Health, and ICF Macro: Phnom Penh, Cambodia; Calverton, MD, USA, 2010.
- Fast Track Initiative Road Map for Reducing Maternal and Newborn Mortality 2010–2015; Ministry of Health: Phnom Penh, Cambodia, 2010.
- Ministry of Health. Five Year Action Plan for Newborn Care in Cambodia 2016–2020; Ministry of Health: Phnom Penh, Cambodia, 2015.
- National Maternal and Child Health Center. National Strategy for Reproductive and Sexual Health in Cambodia, National Reproductive Health Center; Ministy of Health: Phnom Penh, Cambodia, 2017.
- Bang, A.T.; A Bang, R.; Reddy, H.M.; Deshmukh, M.D.; Baitule, S.B. Reduced Incidence of Neonatal Morbidities: Effect of Home-Based Neonatal Care in Rural Gadchiroli, India. J. Perinatol. 2005, 25, S51–S61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baqui, A.H.; Williams, E.; El-Arifeen, S.; Applegate, J.A.; Mannan, I.; Begum, N.; Rahman, S.M.; Ahmed, S.; Black, R.E.; Darmstadt, G.L. Effect of community-based newborn care on cause-specific neonatal mortality in Sylhet district, Bangladesh: Findings of a cluster-randomized controlled trial. J. Perinatol. 2016, 36, 71–76. [Google Scholar] [CrossRef]
- Darmstadt, G.L.; Choi, Y.; Arifeen, S.E.; Bari, S.; Rahman, S.M.; Mannan, I.; Seraji, H.R.; Winch, P.J.; Saha, S.K.; Ahmed, A.S.M.N.U.; et al. Evaluation of a Cluster-Randomized Controlled Trial of a Package of Community-Based Maternal and Newborn Interventions in Mirzapur, Bangladesh. PLoS ONE 2010, 5, e9696. [Google Scholar] [CrossRef]
- Waiswa, P.; Pariyo, G.; Källander, K.; Akuze, J.; Namazzi, G.; Ekirapa-Kiracho, E.; Kerber, K.; Sengendo, H.; Aliganyira, P.; Lawn, J.E.; et al. Effect of the Uganda Newborn Study on care-seeking and care practices: A cluster-randomised controlled trial. Glob. Health Action 2015, 8, 24584. [Google Scholar] [CrossRef] [Green Version]
- Daviaud, E.; Owen, H.; Pitt, C.; Kerber, K.; Jassir, F.B.; Barger, D.; Manzi, F.; Ekipara-Kiracho, E.; Greco, G.; Waiswa, P.; et al. Overview, methods and results of multi-country community-based maternal and newborn care economic analysis. Health Policy Plan. 2017, 32, i6–i20. [Google Scholar] [CrossRef] [Green Version]
- Borghi, J.; Thapa, B.; Osrin, D.; Jan, S.; Morrison, J.; Tamang, S.; Shrestha, B.P.; Wade, A.; Manandhar, D.S.; Costello, A.M.D.L. Economic assessment of a women’s group intervention to improve birth outcomes in rural Nepal. Lancet 2005, 366, 1882–1884. [Google Scholar] [CrossRef]
- Ekirapa-Kiracho, E.; Barger, D.; Mayora, C.; Waiswa, P.; E Lawn, J.; Kalungi, J.; Namazzi, G.; Kerber, K.; Owen, H.; Daviaud, E. Uganda Newborn Study (UNEST) trial: Community-based maternal and newborn care economic analysis. Health Policy Plan. 2017, 32, i42–i52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Guidelines Approved by the Guidelines Review Committee. In Home Visits for the Newborn Child: A Strategy to Improve Survival; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Var, C.; Bazzano, A.N.; Srivastav, S.K.; Welty, J.C.; Ek, N.I.; A Oberhelman, R. Newborn Infection Control and Care Initiative for health facilities to accelerate reduction of newborn mortality (NICCI): Study protocol for a randomized controlled trial. Trials 2015, 16, 257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemming, K.; Taljaard, M.; Grimshaw, J. Introducing the new CONSORT extension for stepped-wedge cluster randomised trials. Trials 2019, 20, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardin, J.; Hilbe, J. Generalized Estimating Equations; Chapman and Hall/CRC: London, UK, 2003. [Google Scholar]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Liang, K.; Zeger, S. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Bogale, T.N.; Worku, A.G.; Bikis, G.A.; Kebede, Z.T. Why gone too soon? Examining social determinants of neonatal deaths in northwest Ethiopia using the three delay model approach. BMC Pediatr. 2017, 17, 216. [Google Scholar] [CrossRef] [Green Version]
- Velleman, Y.; Mason, E.; Graham, W.; Benova, L.; Chopra, M.; Campbell, O.M.R.; Gordon, B.; Wijesekera, S.; Hounton, S.; Mills, J.E.; et al. From Joint Thinking to Joint Action: A Call to Action on Improving Water, Sanitation, and Hygiene for Maternal and Newborn Health. PLoS Med. 2014, 11, e1001771. [Google Scholar] [CrossRef] [Green Version]
- Blencowe, H.; Cousens, S.; Mullany, L.C.; Lee, A.C.; Kerber, K.; Wall, S.; Darmstadt, G.L.; E Lawn, J. Clean birth and postnatal care practices to reduce neonatal deaths from sepsis and tetanus: A systematic review and Delphi estimation of mortality effect. BMC Public Health 2011, 11, S11. [Google Scholar] [CrossRef] [Green Version]
- Rhee, V.; Mullany, L.C.; Khatry, S.K.; Katz, J.; LeClerq, S.C.; Darmstadt, G.L.; Tielsch, J.M. Maternal and Birth Attendant Hand Washing and Neonatal Mortality in Southern Nepal. Arch. Pediatr. Adolesc. Med. 2008, 162, 603–608. [Google Scholar] [CrossRef] [Green Version]
- Cross, S.; Afsana, K.; Banu, M.; Mavalankar, D.; Morrison, E.; Rahman, A.; Roy, T.; Saxena, D.; Vora, K.; Graham, W.J. Hygiene on maternity units: Lessons from a needs assessment in Bangladesh and India. Glob. Health Action 2016, 9, 32541. [Google Scholar] [CrossRef] [PubMed]
- Cronk, R.; Bartram, J. Environmental conditions in health care facilities in low- and middle-income countries: Coverage and inequalities. Int. J. Hyg. Environ. Health 2018, 221, 409–422. [Google Scholar] [CrossRef] [PubMed]
- Hodgins, S.; McPherson, R. Reducing Sepsis Deaths in Newborns through Home Visitation and Active Case Detection: Is it Realistic? Glob. Health Sci. Pract. 2017, 5, 177–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gon, G.; Ali, S.M.; Towriss, C.; Kahabuka, C.; O Ali, A.; Cavill, S.; Dahoma, M.; Faulkner, S.; Haji, H.S.; Kabole, I.; et al. Unpacking the enabling factors for hand, cord and birth-surface hygiene in Zanzibar maternity units. Health Policy Plan. 2017, 32, 1220–1228. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Health Center Level: Staff |
|
| Community Level: VHSG |
|
| Household: Mothers/caregivers |
|
| Visits: Within 24 h of birth |
|
| Visits: Day 3 |
|
| Visits: Day 7 |
|
| Characteristics of Interest | Control | Intervention |
|---|---|---|
| N = 803 | N = 1691 | |
| Demographic characteristics | ||
| • Age, mean (IQR) | 26.7 (23.0–30.0) | 26.7 (23.0–30.0) |
| • No previous pregnancies, N(%) | 314 (39.1) | 655 (38.7) |
| • Previous pregnancies, N(%) | ||
| ▪ Three or more previous | 36 (7.4) | 78 (7.5) |
| • Education, N(%) | ||
| ▪ No schooling | 47 (5.9) | 82 (4.9) |
| ▪ Primary | 325 (40.5) | 667 (39.5) |
| ▪ Lower and upper | 427 (53.1) | 894 (53.0) |
| ▪ Higher than upper | 4 (0.5) | 47 (2.8) |
| • Assets, household ownership, N(%) | ||
| ▪ Car | 20 (2.5) | 41 (2.4) |
| ▪ Motorcycle | 661 (82.3) | 1441 (83.4) |
| • Housing, N(%) | ||
| ▪ Sole owner | 334 (41.6) | 726 (42.9) |
| ▪ Living at relative's house | 458 (57.0) | 939 (55.5) |
| ▪ Other (joint homeowner, renting, other) | 11 (1.5) | 26 (1.5) |
| • Farm land property, N(%) | ||
| ▪ Own farm land | 477 (59.4) | 1020 (60.4) |
| ▪ Other (parent's land, rented land, no farm land) | 326 (40.7) | 670 (39.6) |
| • Occupation, N(%) | ||
| ▪ Farmer | 316 (39.4) | 419 (24.8) |
| ▪ Factory worker | 183 (22.8) | 684 (40.5) |
| ▪ Housewife | 208 (26.0) | 354 (20.9) |
| ▪ Other (vendor/seller, civil servant, business woman, other) | 96 (12.0) | 234 (13.9) |
| Other characteristics | ||
| • Household with electricity, N(%) | 694 (86.4) | 1340 (79.2) |
| • Latrine, N(%) | ||
| ▪ Any latrine | 536 (66.8) | 1187 (70.2) |
| ▪ No latrine | 267 (33.3) | 504 (29.8) |
| • Water for drinking boiled, N (%) | 595 (74.1) | 1298 (76.8) |
| • Handwashing practice | ||
| ▪ Not wash hands | 2 (0.3) | 3 (0.2) |
| ▪ Water only | 44 (5.5) | 121 (7.2) |
| ▪ Water with soap | 590 (73.5) | 989 (58.5) |
| ▪ Other (water with detergent, ash, other) | 311 (38.8) | 1123 (66.4) |
| • Family has a “PoorID card” | 174 (21.7) | 356 (21.1) |
| Outcome | Results | OR (CI) | p-Value | |
|---|---|---|---|---|
| Intervention | Control | |||
| Infection prevention and control behavior among HC staff (measured by proportion of appropriate handwashing with soap or disinfectant at key points in provision of care to mothers and newborns) | 52.88% | 6.71% | 15.60 (7.73–31.47) | <0.0001 |
| HC staff knowledge of danger signs (measured by % of HC staff who know at least six danger signs) | 98.45% | 14.77% | 35.91 (19.31–66.78) | <0.0001 |
| HC staff ability to recall hygiene messages (as measured by % of HC staff who recall at least three hygiene messages) | 95.29% | 54.36% | 16.98 | <0.0001 |
| Outcome | Results | OR (CI) | p-value | |
|---|---|---|---|---|
| Intervention | Control | |||
| VHSG knowledge of danger signs (as measured by % of VHSG who know six danger signs) | 60.58% | 2.11% | 71.44 (41.55–122.87) | <0.0001 |
| Percent of newborns visited at least once by VHSG on or before day 7 of life | 24.25% | 15.94% | 1.69 | <0.001 |
| Percent of newborns visited at least twice by VHSG on or before day 7 of life | 24.24% | 16.04% | 1.77 | <0.001 |
| VHSG knowledge of hygiene (as measured by % of VHSG who can deliver hygiene messages) | 67.75% | 18.10% | 9.51 | <0.0001 |
| Outcome | Results | OR (CI) | p-Value | |
|---|---|---|---|---|
| Intervention | Control | |||
| Mothers’ knowledge of danger signs (% of mothers who know at least three danger signs) | 54.9% | 30.5% | 2.35 (1.22–4.52) | 0.0104 |
| Care-seeking (% of families who sought care from appropriate facility) | 80.20% (Frequency only) | 81.82% (Frequency only) | * | * |
| Referral (time between onset of suspected danger signs and referral to appropriate facility: <6 h) | 17.28% | 36.84% | 0.45 (0.19–1.06) | 0.0688 |
| Infection prevention (as measured by proportion of mothers’ reporting handwashing with soap at key events) | 57.78% | 37.36% | 1.62 (0.81–3.22) | 0.1697 |
| Counseling by VHSG (% of mothers who reported receipt of messages on the following topics): Essential newborn care Handwashing Care-seeking | 36.15% 11.1.% 35.01% | 5.53% 15.1% 5.35% | 10.66 0.70 9.52 | 0.0005 0.5342 <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Var, C.; Oberhelman, R.A.; Shu, T.; Leang, S.; Duggal, R.; Le, J.; Bazzano, A.N. A Linked Community and Health Facility Intervention to Improve Newborn Health in Cambodia: The NICCI Stepped-Wedge Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 1559. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051559
Var C, Oberhelman RA, Shu T, Leang S, Duggal R, Le J, Bazzano AN. A Linked Community and Health Facility Intervention to Improve Newborn Health in Cambodia: The NICCI Stepped-Wedge Cluster-Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(5):1559. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051559
Chicago/Turabian StyleVar, Chivorn, Richard A. Oberhelman, Tian Shu, Supheap Leang, Ryan Duggal, Jennifer Le, and Alessandra N. Bazzano. 2020. "A Linked Community and Health Facility Intervention to Improve Newborn Health in Cambodia: The NICCI Stepped-Wedge Cluster-Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 5: 1559. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051559