Development and Psychometric Properties of MisoQuest—A New Self-Report Questionnaire for Misophonia



Abstract
:1. Introduction
- An individual experiences a strong, immediate somatic reaction that begins with irritation or disgust which quickly turns into anger in the presence of or in the expectation of aversive sounds. The anger makes a person feel out of control, sometimes leading to aggressive behavior;
- The person assesses these reactions as disproportionate to the situation;
- Due to the consequences of unpleasant experiences caused by certain sounds, the person, if possible, avoids situations in which the trigger is expected or struggles with high discomfort in its presence. Therefore, the condition has a significant, negative impact on the person’s life;
- The avoidance and emotional reaction to certain triggers cannot be better explained by other disorders, such as post-traumatic stress disorder or obsessive-compulsive disorder.
2. Materials and Methods
2.1. Ethical Approval
2.2. Questionnaire Construction
2.3. Participants
2.4. Data Management and Analytic Strategy
3. Results
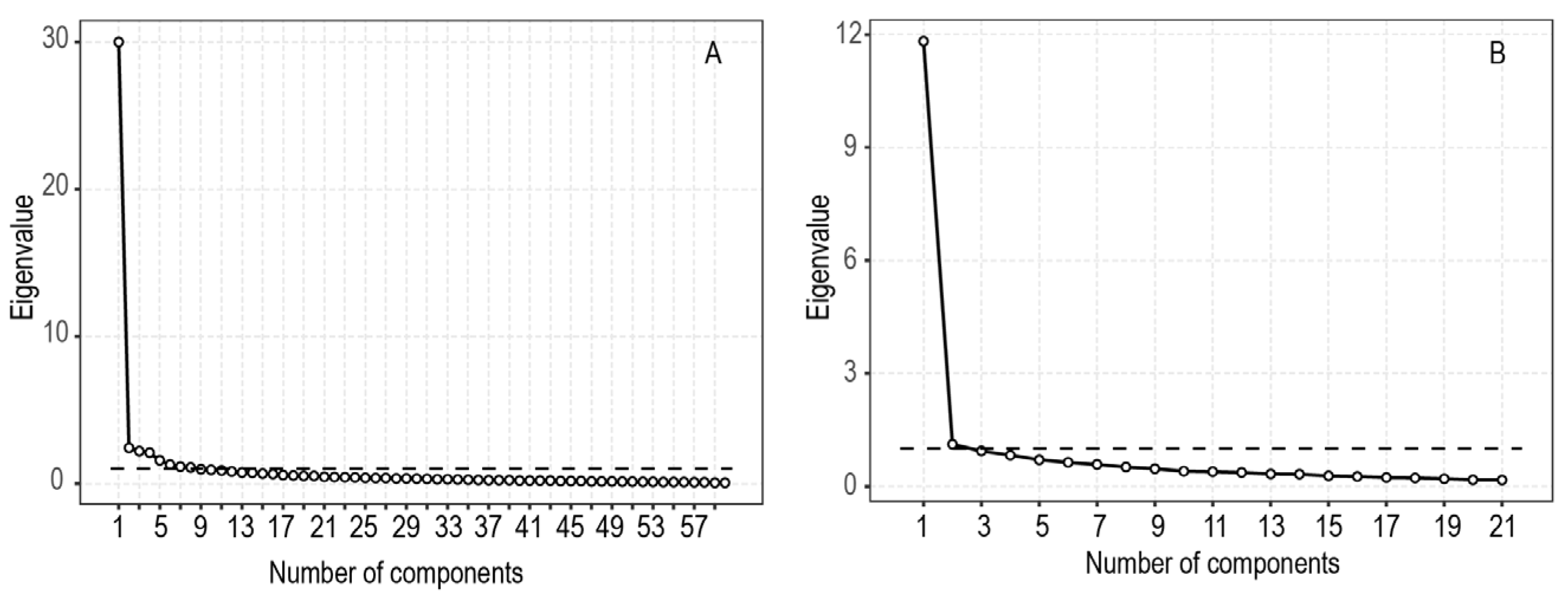
3.1. Psychometric Validation: Construct Validity
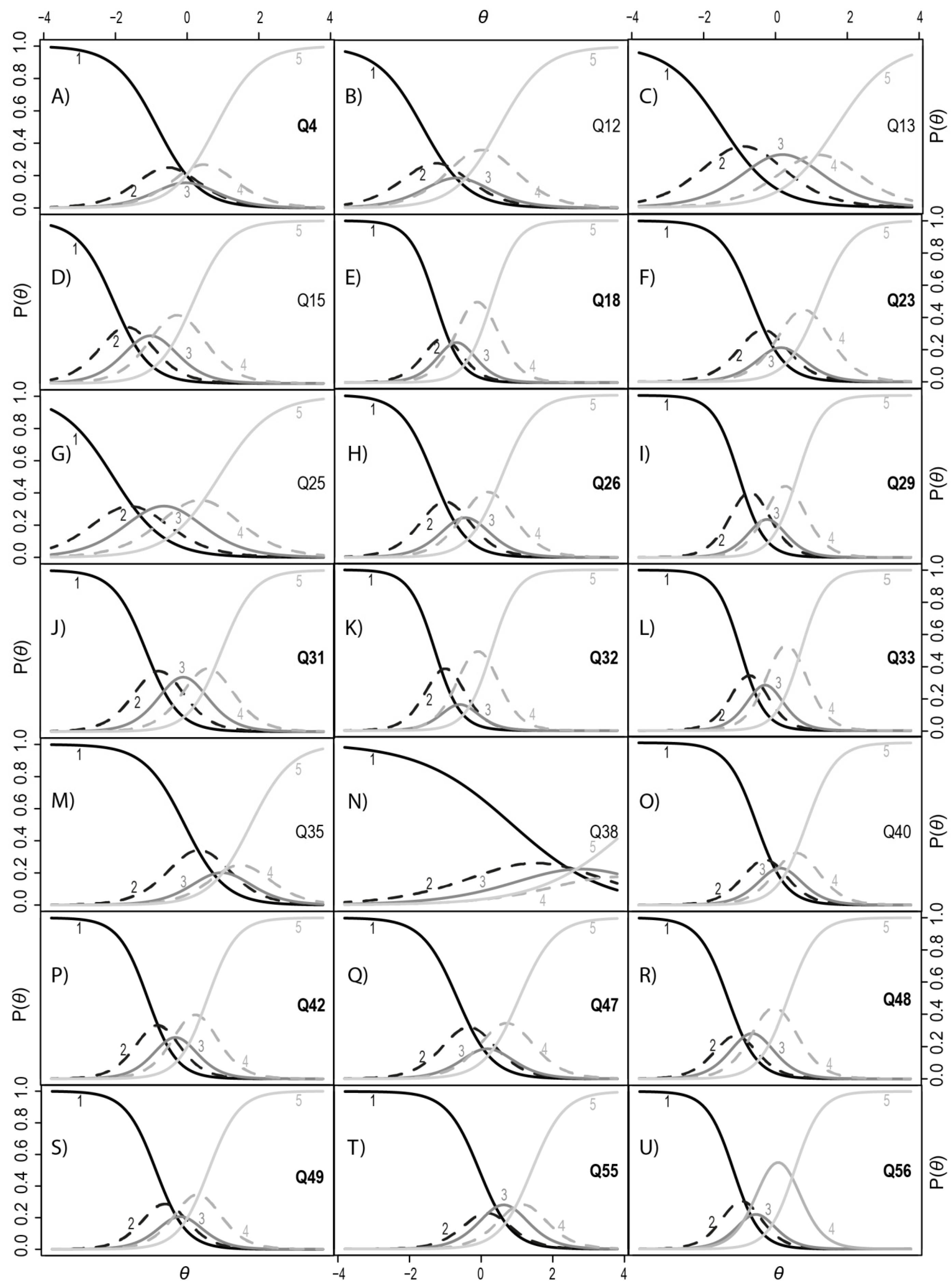
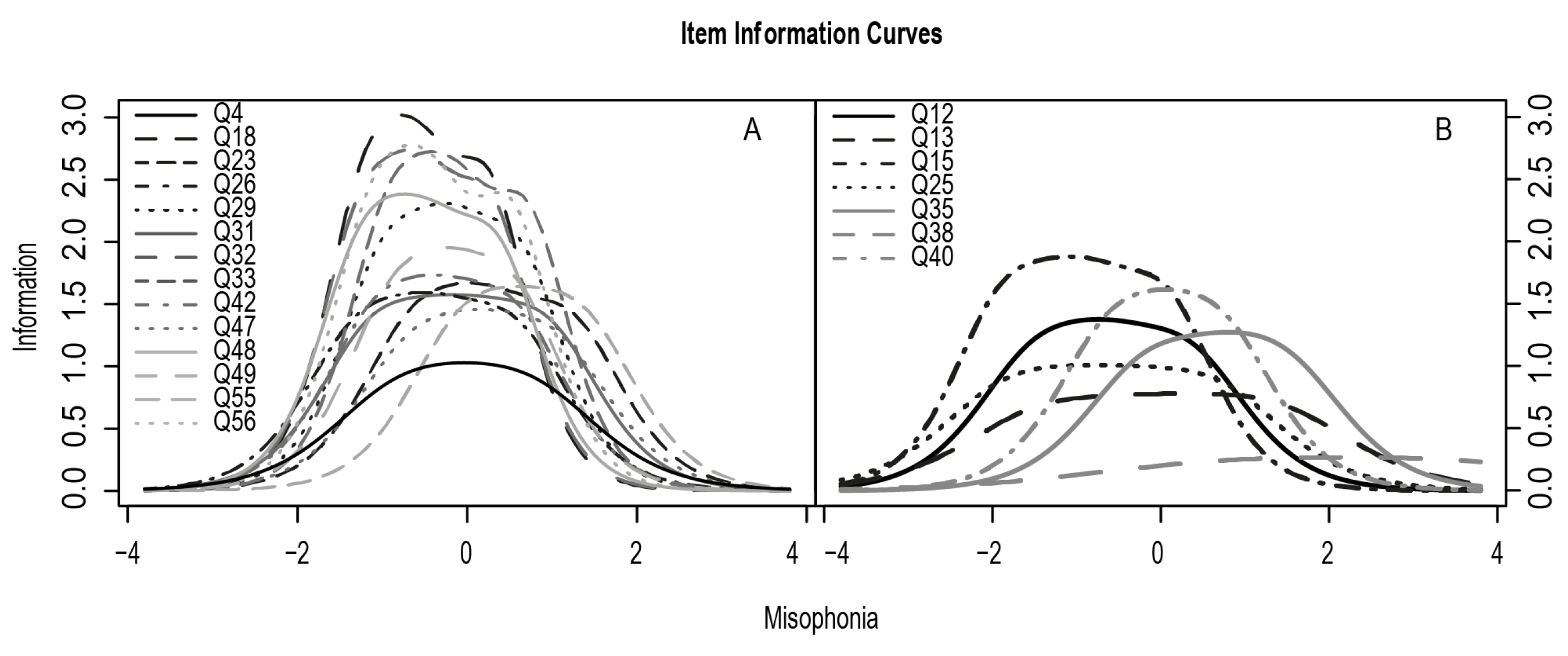
3.2. Item Response Theory Analysis
3.3. Reliability Analysis
3.4. Criterion-Related Validity
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jastreboff, M.M.; Jastreboff, P.J. Decreased sound tolerance and tinnitus retraining therapy (TRT). Aust. N. Z. J. Audiol. 2002, 24, 74–84. [Google Scholar] [CrossRef]
- Jastreboff, P.J.; Jastreboff, M.M. Treatments for decreased sound tolerance (hyperacusis and misophonia). Semin. Hear. 2014, 35, 105–120. [Google Scholar] [CrossRef] [Green Version]
- Brout, J.J.; Edelstein, M.; Erfanian, M.; Mannino, M.; Miller, L.J.; Rouw, R.; Kumar, S.; Rosenthal, M.Z. Investigating misophonia: A review of the empirical literature, clinical implications, and a research agenda. Front. Neurosci. 2018, 12, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jastreboff, M.M.; Jastreboff, P.J. Components of decreased sound tolerance: Hyperacusis, misophonia, phonophobia. ITHS News Lett. 2001, 2, 5–7. [Google Scholar]
- Edelstein, M.; Brang, D.; Rouw, R.; Ramachandran, V.S. Misophonia: Physiological investigations and case descriptions. Front. Hum. Neurosci. 2013, 7, 296. [Google Scholar] [CrossRef] [Green Version]
- Quek, T.; Ho, C.; Choo, C.; Nguyen, L.; Tran, B.; Ho, R.; Quek, T.C.; Ho, C.S.; Choo, C.C.; Nguyen, L.H.; et al. Misophonia in Singaporean psychiatric patients: A cross-sectional study. Int. J. Environ. Res. Public Health 2018, 15, 1410. [Google Scholar] [CrossRef] [Green Version]
- Asha’Ari, Z.A.; Mat Zain, N.; Razali, A. Phonophobia and hyperacusis: Practical points from a case report. Malays. J. Med. Sci. 2010, 17, 49–51. [Google Scholar]
- Schröder, A.; Vulink, N.; Denys, D. Misophonia: Diagnostic criteria for a new psychiatric disorder. PLoS ONE 2013, 8, e54706. [Google Scholar] [CrossRef]
- Schröder, A.; van Wingen, G.; Eijsker, N.; San Giorgi, R.; Vulink, N.C.; Turbyne, C.; Denys, D. Misophonia is associated with altered brain activity in the auditory cortex and salience network. Sci. Rep. 2019, 9, 7542. [Google Scholar] [CrossRef]
- Kumar, S.; Tansley-Hancock, O.; Sedley, W.; Winston, J.S.; Callaghan, M.F.; Allen, M.; Cope, T.E.; Gander, P.E.; Bamiou, D.E.; Griffiths, T.D. The brain basis for misophonia. Curr. Biol. 2017, 27, 527–533. [Google Scholar] [CrossRef] [Green Version]
- Rouw, R.; Erfanian, M. A large-scale study of misophonia. J. Clin. Psychol. 2018, 74, 453–479. [Google Scholar] [CrossRef] [PubMed]
- Mckay, D.; Kim, S.-K.; Mancusi, L.; Storch, E.A.; Spankovich, C. Profile analysis of psychological symptoms associated with misophonia: A community sample. Behav. Ther. 2018, 49, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Dozier, T. Phenomenology of misophonia: Initial physical and emotional responses misophonia initial physical reflex measurement view project misophonia research view project. Am. J. Psychol. 2017, 130, 431–438. [Google Scholar] [CrossRef]
- Wu, M.S.; Lewin, A.B.; Murphy, T.K.; Storch, E.A. Misophonia: Incidence, phenomenology, and clinical correlates in an undergraduate student sample. J. Clin. Psychol. 2014, 70, 994–1007. [Google Scholar] [CrossRef]
- Zhou, X.; Wu, M.S.; Storch, E.A. Misophonia symptoms among Chinese university students: Incidence, associated impairment, and clinical correlates. J. Obsessive Compuls. Relat. Disord. 2017, 14, 7–12. [Google Scholar] [CrossRef]
- Cusack, S.E.; Cash, T.V.; Vrana, S.R. An examination of the relationship between misophonia, anxiety sensitivity, and obsessive-compulsive symptoms. J. Obsessive Compuls. Relat. Disord. 2018, 18, 67–72. [Google Scholar] [CrossRef]
- McErlean, A.B.J.; Banissy, M.J. Increased misophonia in self-reported Autonomous Sensory Meridian Response. PeerJ 2018, 6, e5351. [Google Scholar] [CrossRef] [Green Version]
- Misophonia Assessment Questionaire (MAQ). Available online: https://misophoniatreatment.com/wp-content/uploads/2014/06/MAQ-2.pdf (accessed on 26 February 2020).
- Misophonia Physiological Response Scale (MPRS). Available online: https://misophoniatreatment.com/wp-content/uploads/2014/06/MPRS.pdf (accessed on 26 February 2020).
- The Misophonia Activation Scale. Available online: http://www.misophonia-uk.org/the-misophonia-activation-scale.html (accessed on 26 February 2020).
- Schröder, A.; van Wingen, G.; Vulink, N.C.; Denys, D. Commentary: The brain basis for misophonia. Front. Behav. Neurosci. 2017, 11, 111. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Griffiths, T.D. Response: Commentary: The brain basis for misophonia. Front. Behav. Neurosci. 2017, 11, 127. [Google Scholar] [CrossRef] [Green Version]
- Kliuchko, M.; Heinonen-Guzejev, M.; Monacis, L.; Gold, B.P.; Heikkilä, K.V.; Spinosa, V.; Tervaniemi, M.; Brattico, E. The association of noise sensitivity with music listening, training, and aptitude. Noise Health 2015, 17, 350–357. [Google Scholar] [CrossRef]
- Franek, M. Is Noise Sensitivity Influenced by Musical Factors? In Recent Advances in Acoustics and Music: Theory and Applications, Proceedings of the 10th WSEAS International Conference on Acoustics & Music: Theory & Applications, Prague, Czech Republic, 23–25 March 2009; Mastorakis, N.E., Croitoru, A., Balas, V.E., Son, E., Mladenov, V., Eds.; World Scientific and Engineering Academy and Society WSEAS: Stevens Point, WI, USA, 2009; pp. 19–22. [Google Scholar]
- Jansen, E.J.M.; Helleman, H.W.; Dreschler, W.A.; Laat, J.A.P.M. Noise induced hearing loss and other hearing complaints among musicians of symphony orchestras. Int. Arch. Occup. Environ. Health 2009, 82, 153–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, K.K.; Lai, C.M.; Ko, C.H.; Chou, C.; Kim, D.I.; Watanabe, H.; Ho, R.C.M. Psychometric properties of the Revised Chen Internet Addiction Scale (CIAS-R) in Chinese adolescents. J. Abnorm. Child Psychol. 2014, 42, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Brzezińska, J. A polytomous item response theory models using R/Politomiczne modele teorii odpowiedzi na pozycje testowe w programie R. Ekonometria 2016, 2, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Rizopoulos, D. Itm: An R package for latent variable modeling and item response theory analyses. J. Stat. Softw. 2006, 17, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Schivinski, B.; Brzozowska-Woś, M.; Buchanan, E.M.; Griffiths, M.D.; Pontes, H.M. Psychometric assessment of the internet gaming disorder diagnostic criteria: An item response theory study. Addict. Behav. Rep. 2018, 8, 176–184. [Google Scholar] [CrossRef]
- Akaike, H. A new look at the statistical model identification. IEEE Trans. Autom. Control 1974, 19, 716–723. [Google Scholar] [CrossRef]
- Schwarz, G. Estimating the dimension of a model. Ann. Stat. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- RStudio: Integrated Development for R. Available online: http://www.rstudio.com (accessed on 28 November 2019).
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Dozier, T.H.; Lopez, M.; Pearson, C. Proposed diagnostic criteria for misophonia: A multisensory conditioned aversive reflex disorder. Front. Psychol. 2017, 8, 1975. [Google Scholar] [CrossRef] [Green Version]
- Samejima, F. Acceleration model in the heterogeneous case of the general graded response model. Psychometrika 1995, 60, 549–572. [Google Scholar] [CrossRef]
- Burnham, K.P.; Anderson, D.R. Model Selection and Multimodel Inference: A Practical Information; Springer: New York, NY, USA, 2002. [Google Scholar]
- Webber, T.A.; Johnson, P.L.; Storch, E.A. Pediatric misophonia with comorbid obsessive-compulsive spectrum disorders. Gen. Hosp. Psychiatry 2014, 36, 231. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.L.; Webber, T.A.; Wu, M.S.; Lewin, A.B.; Murphy, T.K.; Storch, E.A. When selective audiovisual stimuli become unbearable: A case series on pediatric misophonia. Neuropsychiatry 2013, 3, 6. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Phase 1 | Phase 2 | |||||
|---|---|---|---|---|---|---|
| Domain of the Diagnostic Criteria | MisoQuest items (numbers of items from the I version_II version) | Factor loadings | Factor loadings | Item-scale correlations | Test-retest reliability (ICC) | IRT unconstrained model Discrimination |
| Reaction to Specific Sound | Q4_16 “I find some sounds made by the human body unbearable.” | 0.698 | 0.718 | 0.69 | 0.77 | 1.685 |
| Q12_1 “I find some quiet sounds unbearable.” | 0.703 | 0.701 | 0.67 | 0.57 | 1.592 | |
| Q13_6 “I find sounds made by things/items unbearable.” | 0.355 | 0.652 | 0.62 | 0.54 | 1.343 | |
| Occurrence of Reaction | Q15_2 “When I hear some sounds, I am immediately overcome by unpleasant emotions.” | 0.827 | 0.725 | 0.69 | 0.57 | 2.010 |
| Q18_19 “Some unpleasant sounds make me instantly angry.” | 0.834 | 0.805 | 0.78 | 0.67 | 2.763 | |
| Emotional Reactions | Q23_12 “I start feeling anger the moment I see a thing/animal/person that might make an unpleasant sound at any time.” | 0.825 | 0.778 | 0.75 | 0.70 | 2.202 |
| Q25_3 “When I hear an unpleasant sound, my heart starts beating faster.” | 0.757 | 0.646 | 0.61 | 0.69 | 1.397 | |
| Q26_9 “When I hear unpleasant sounds, I start sensing emotions in my body (e.g., I sweat, feel pain, feel pressure, my muscles tense).” | 0.646 | 0.769 | 0.74 | 0.73 | 2.165 | |
| Q29_5 “Unpleasant sounds make me feel overwhelmed.” | 0.818 | 0.841 | 0.82 | 0.68 | 2.794 | |
| Q31_7 “I become anxious at the mere thought of an unpleasant sound.” | 0.862 | 0.773 | 0.74 | 0.67 | 2.201 | |
| Control of Emotional Reactions | Q32_8 “Some sounds bother me so much that I have difficulty controlling my emotions.” | 0.857 | 0.818 | 0.79 | 0.59 | 2.806 |
| Q33_14 “I put a lot of effort into controlling emotions when I hear an unpleasant sound.” | 0.834 | 0.856 | 0.83 | 0.66 | 2.943 | |
| Q35_10 “When I hear unpleasant sounds, my eyes start filling with tears.” | 0.832 | 0.664 | 0.64 | 0.71 | 1.764 | |
| Q38_11 “As a child I would hit people who made unpleasant sounds.” | 0.851 | 0.402 | 0.37 | 0.62 | 0.779 | |
| Attitude to Own Reactions | Q40_13 “I think that something is wrong with me because I react too strongly to certain sounds.” | 0.844 | 0.797 | 0.77 | 0.71 | 2.435 |
| Q42_4 “I believe that my reactions to sounds are exaggerated but I can’t get rid of them.” | 0.828 | 0.807 | 0.79 | 0.77 | 2.450 | |
| Avoidance | Q47_15 “If I can, I avoid meeting with certain people because of the sounds they make.” | 0.812 | 0.760 | 0.73 | 0.69 | 2.041 |
| Q48_17 “I feel that my mental state worsens if I cannot leave a place where there’s an unpleasant sound.” | 0.786 | 0.789 | 0.76 | 0.71 | 2.460 | |
| Q49_18 “I often think about how to drown out unpleasant sounds.” | 0.736 | 0.781 | 0.76 | 0.72 | 2.344 | |
| Daily Functioning | Q55_20 “I am scared that unpleasant sounds may impact my future.” | 0.846 | 0.739 | 0.71 | 0.78 | 2.210 |
| Q56_21 “When meeting with other people, I am sometimes irritated because of unpleasant sounds that are present.” | 0.804 | 0.805 | 0.78 | 0.69 | 2.699 | |
| Variable | Phase 1 (N = 383) | Phase 2 (N = 322) |
|---|---|---|
| Age, Mean ± Standard Deviation (years) | 31.7 ± 9.22 | 31.7 ± 8.83 |
| Gender, | ||
| Male, No. (%) | 53 (13.8%) | 65 (20.2%) |
| Female, No. (%) | 330 (86.2%) | 257 (79.8%) |
| Educational Attainment | ||
| Lower Secondary Education | - | 5 (1.6%) |
| High School Education | - | 81 (25.2%) |
| Non-tertiary Education | - | 1 (0.3%) |
| Higher Education | - | 232 (72%) |
| Place of Residence | ||
| Village | - | 28 (8.7%) |
| Small City (less than 500k residents) | - | 88 (27.3%) |
| Large City (more than 500k residents) | - | 206 (64%) |
| Marital Status | ||
| Single, Never Married | - | 88 (27.3%) |
| Cohabiting with Partner | - | 110 (34.2%) |
| Married | - | 105 (32.6%) |
| Divorced | - | 9 (2.8%) |
| Diagnosis, No. (%) | ||
| Misophonia | 68 (17.8%) | 63 (19.6%) |
| Hyperacusis | - | 11 (3.4%) |
| Autism/Asperger Syndrome | - | 33 (10.2%) |
| Affective Disorders | - | 16 (5%) |
| Anxiety Disorders | - | 4 (1.2%) |
| Personality Disorders | - | 12 (3.7%) |
| Neurological Disorders | - | 5 (1.5%) |
| Musician, No. (%) | - | 96 (29.8%) |
| Group (n) | MisoQuest M(SD) | t Test (df) | p-Value Cohen’s d |
|---|---|---|---|
| With Misophonia (n = 61) | 65.72 (4.3) | t = 21.65 (308.85) | p < 0.001 d = 2.13 |
| Without Misophonia (n = 254) | 41.77 (15.3) | ||
| Without Diagnosis (n = 253) | 44.83 (17.1) | T = 3.9 (111.322) | p < 0.001 d = 0.52 |
| With Diagnosis (n = 62) | 52.87 (13.84) | ||
| -ASD (n = 31) | 53.39 (12.49) | ||
| -Hyperacusis (Without Misophonia) (n = 8) | 52.87 (15.35) | ||
| -Psychiatric Diagnosis (n = 23) | 52.17 (15.58) | ||
| Musician (n = 95) | 43.55 (13.9) | t = 2.51 (225.67) | p < 0.05 d = 0.29 |
| Non-Musician (n = 220) | 47.64 (17.78) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siepsiak, M.; Śliwerski, A.; Łukasz Dragan, W. Development and Psychometric Properties of MisoQuest—A New Self-Report Questionnaire for Misophonia. Int. J. Environ. Res. Public Health 2020, 17, 1797. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051797
Siepsiak M, Śliwerski A, Łukasz Dragan W. Development and Psychometric Properties of MisoQuest—A New Self-Report Questionnaire for Misophonia. International Journal of Environmental Research and Public Health. 2020; 17(5):1797. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051797
Chicago/Turabian StyleSiepsiak, Marta, Andrzej Śliwerski, and Wojciech Łukasz Dragan. 2020. "Development and Psychometric Properties of MisoQuest—A New Self-Report Questionnaire for Misophonia" International Journal of Environmental Research and Public Health 17, no. 5: 1797. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17051797