Association of Arch Stiffness with Plantar Impulse Distribution during Walking, Running, and Gait Termination




Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
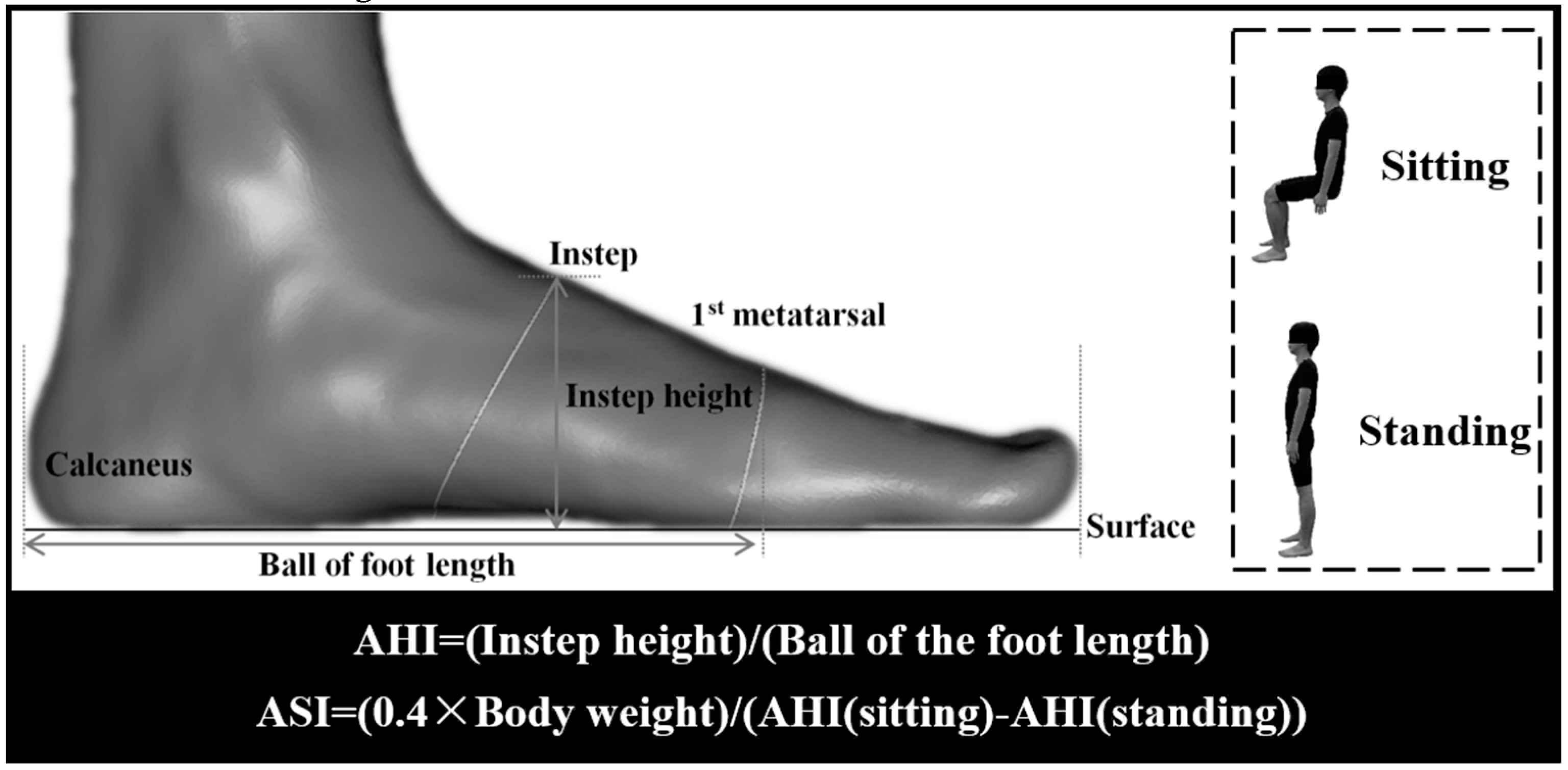
2.2. Static Foot Structure Measurements
2.3. Dynamic Gait Task Measurements
2.4. Data Acquisition
2.5. Statistical Analysis
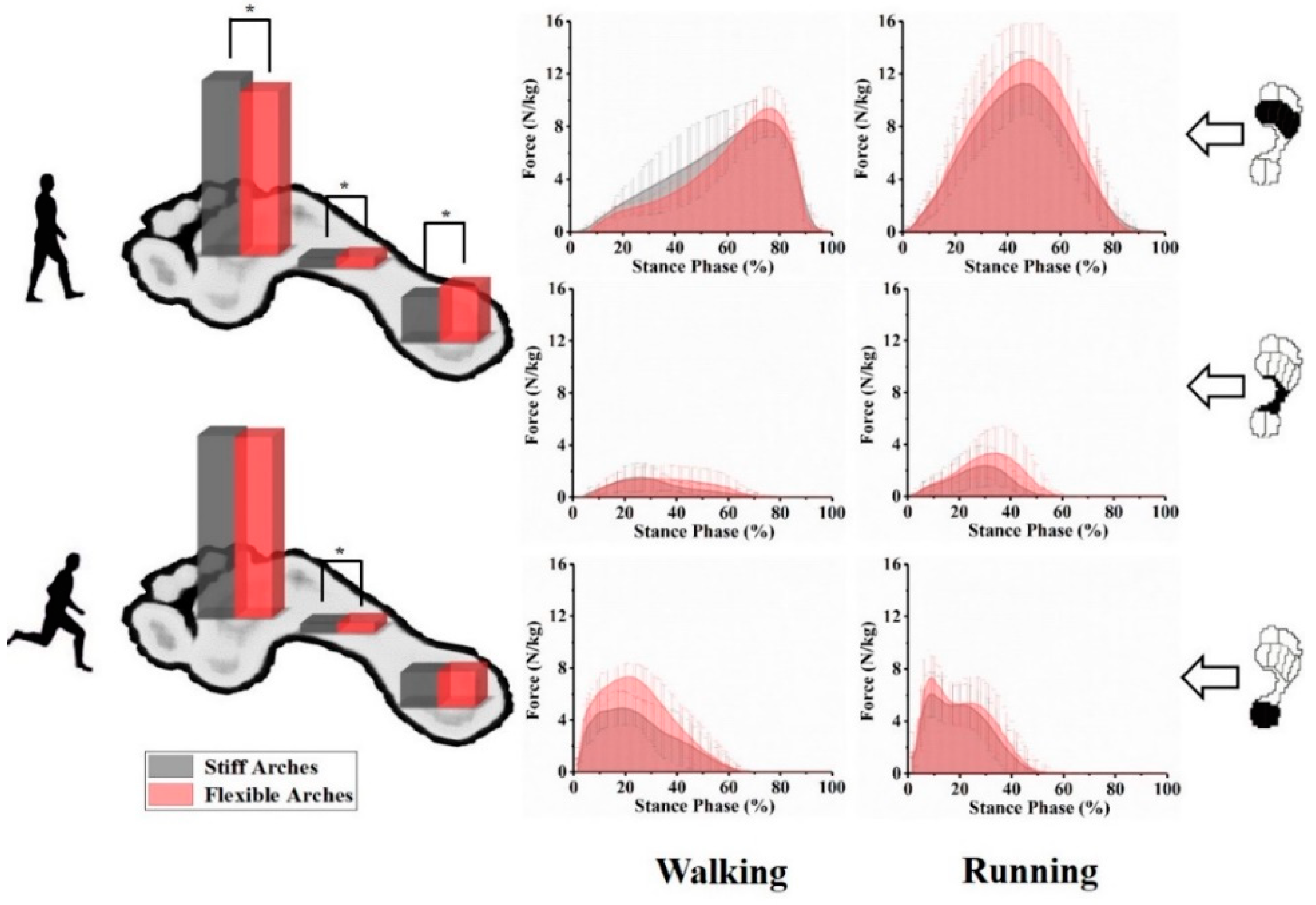
3. Results
4. Discussion
4.1. The Relationship between ASI and Plantar Impulse during Walking and Running
4.2. The Relationship between ASI and Plantar Impulse during Gait Termination
4.3. Clinical Relevance
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jiang, C. The Effect of Basketball Shoe Collar on Ankle Stability: A Systematic Review and Meta-Analysis. Phys. Act. Health. 2020, 4, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Donatelli, R. Normal Biomechanics of the Foot and Ankle. J. Orthop. Sports Phys. Ther. 1985, 7, 91–95. [Google Scholar] [CrossRef]
- Sun, P.; Shih, S.; Chen, Y.; Hsu, Y.; Yang, R.; Chen, C. Biomechanical analysis of foot with different foot arch heights: A finite element analysis. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 563–569. [Google Scholar] [CrossRef]
- Zifchock, R.A.; Davis, I.; Hillstrom, H.; Song, J. The Effect of Gender, Age, and Lateral Dominance on Arch Height and Arch Stiffness. Foot Ankle Int. 2006, 27, 367–372. [Google Scholar] [CrossRef]
- Kelly, L.A.; Cresswell, A.G.; Racinais, S.; Whiteley, R.; Lichtwark, G. Intrinsic foot muscles have the capacity to control deformation of the longitudinal arch. J. R. Soc. Interface 2014, 11, 20131188. [Google Scholar] [CrossRef] [Green Version]
- McKeon, P.O.; Hertel, J.; Bramble, D.; Davis, L. The foot core system: A new paradigm for understanding intrinsic foot muscle function. Br. J. Sports Med. 2015, 49, 290. [Google Scholar] [CrossRef] [Green Version]
- Mann, R.A.; Hagy, J.L. The function of the toes in walking, jogging and running. Clin. Orthop. Rel. Res. 1979, 142, 24–29. [Google Scholar] [CrossRef]
- Fu, F.; Wang, S.; Shu, Y.; Li, J.; Popik, S.; Gu, Y. A Comparative Biomechanical Analysis the Vertical Jump between Flatfoot and Normal Foot. J. Biomim. Biomat. Biomed. Eng. 2016, 28, 26–35. [Google Scholar] [CrossRef]
- Lopez-Lopez, D.; Vilar-Fernandez, J.M.; Barros-Garcia, G.; Losa-Iglesias, M.E.; Palomo-Lopez, P.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C. Foot arch height and quality of life in adults: A strobe observational study. Int. J. Environ. Res. Public Health. 2018, 15, 1555. [Google Scholar] [CrossRef] [Green Version]
- Lopez Lopez, D.; Bouza Prego, M.; Requeijo Constenla, A.; Saleta Canosa, J.L.; Casasnovas, A.B.; Tajes, F.A. The impact of foot arch height on quality of life in 6–12 year olds. Colomb. Med. (Cali). 2014, 45, 168–172. [Google Scholar] [CrossRef]
- Lopez-Lopez, D.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Palomo-Lopez, P.; Rodriguez-Sanz, D.; Brandariz-Pereira, J.M.; Calvo-Lobo, C. Evaluation of foot health related quality of life in individuals with foot problems by gender: A cross-sectional comparative analysis study. Bmj Open. 2018, 8, e023980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, X.; Tsujimoto, T.; Kim, B.; Katayama, Y.; Ogiso, K.; Takenaka, M.; Tanaka, K. Does weight reduction affect foot structure and the strength of the muscles that move the ankle in obese japanese adults? J. Foot Ankle Surg. 2017, 57, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.S.; Mcclay, I.S. Measurements used to characterize the foot and the medial longitudinal arch: Reliability and validity. Phys. Ther. 2000, 80, 864–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weimar, W.H.; Shroyer, J.F. Arch height index normative values of college-aged women using the arch height index measurement system. J. Am. Podiatr. Med. Assoc. 2013, 103, 213–217. [Google Scholar] [CrossRef]
- Boyer, E.R.; Ward, E.D.; Derrick, T.R. Medial Longitudinal Arch Mechanics Before and After a 45-Minute Run. J. Am. Podiatr. Med. Assoc. 2014, 104, 349–356. [Google Scholar] [CrossRef]
- Zifchock, R.; Parker, R.; Wan, W.; Neary, M.; Song, J.; Hillstrom, H. The relationship between foot arch flexibility and medial-lateral ground reaction force distribution. Gait Posture 2019, 69, 46–49. [Google Scholar] [CrossRef]
- Zifchock, R.A.; Theriot, C.; Hillstrom, H.J.; Song, J.; Neary, M. The Relationship Between Arch Height and Arch Flexibility. J. Am. Podiatr. Med. Assoc. 2017, 107, 119–123. [Google Scholar] [CrossRef] [Green Version]
- Bishop, M.D.; Brunt, D.; Pathare, N.; Patela, B. The interaction between leading and trailing limbs during stopping in humans. Neurosci. Lett. 2002, 323, 1–4. [Google Scholar] [CrossRef]
- Bishop, M.D.; Brunt, D.; Kukulka, C.; Tillman, M.D.; Pathare, N. Braking impulse and muscle activation during unplanned gait termination in human subjects with parkinsonism. Neurosci. Lett. 2003, 348, 89–92. [Google Scholar] [CrossRef]
- Sparrow, W.A.; Tirosh, O. Gait termination: A review of experimental methods and the effects of ageing and gait pathologies. Gait Posture 2005, 22, 362–371. [Google Scholar] [CrossRef]
- Ridge, S.T.; Henley, J.; Manal, K.; Miller, F.; Richards, J.G. Kinematic and kinetic analysis of planned and unplanned gait termination in children. Gait Posture 2013, 37, 178–182. [Google Scholar] [CrossRef] [Green Version]
- Cen, X.; Jiang, X.; Gu, Y. Do different muscle strength levels affect stability during unplanned gait termination? Acta Bioeng. Biomech. 2019, 21, 27–35. [Google Scholar] [CrossRef]
- Shu, Y.; Mei, Q.; Fernandez, J.; Li, Z.; Feng, N.; Gu, Y. Foot morphological difference between habitually shod and unshod runners. PLoS ONE 2015, 10, e0131385. [Google Scholar] [CrossRef] [Green Version]
- Telfer, S.; Woodburn, J. The use of 3D surface scanning for the measurement and assessment of the human foot. J. Foot Ankle Res. 2010, 3, 19. [Google Scholar] [CrossRef] [Green Version]
- Yan, S.; Zhang, K.; Tan, G.; Yang, J.; Liu, Z. Effects of obesity on dynamic plantar pressure distribution in Chinese prepubescent children during walking. Gait Posture 2013, 37, 37–42. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Carson, D.W.; Myer, G.D.; Hewett, T.E.; Heidt, R.S.; Ford, K.R. Increased plantar force and impulse in American football players with high arch compared to normal arch. Foot 2012, 22, 310–314. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Seguín, L.M.; Mancha, J.A.D.; Rodríguez, R.S.; Martínez, E.E.; Martín, B.G.; Ortega, J.R. Comparison of plantar pressures and contact area between normal and cavus foot. Gait Posture 2014, 39, 789–792. [Google Scholar] [CrossRef]
- Chuckpaiwong, B.; Nunley, J.A.; Mall, N.A.; Queen, R.M. The effect of foot type on in-shoe plantar pressure during walking and running. Gait Posture 2008, 28, 405–411. [Google Scholar] [CrossRef]
- Dawe, E.J.C.; Davis, J. (vi) Anatomy and biomechanics of the foot and ankle. Orthop Trauma 2011, 25, 279–286. [Google Scholar] [CrossRef]
- Jaeger, R.J.; Vanitchatchavan, P. Ground reaction forces during termination of human gait. J. Biomech. 1992, 25, 1233–1236. [Google Scholar] [CrossRef]
- Hotfiel, T.; Carl, H.D.; Wendler, F.; Jendrissek, A.; Heiß, R.; Swoboda, B. Plantar pressures increase with raising body weight: A standardised approach with paired sample using neutral shoes. J. Back Musculoskelet. Rehabil. 2016, 30, 583. [Google Scholar] [CrossRef] [PubMed]
- Jian, Y.; Winter, D.A.; Ishac, M.G.; Gilchrist, L. Trajectory of the body COG and COP during initiation and termination of gait. Gait Posture 1993, 1, 9–22. [Google Scholar] [CrossRef]
- O’kane, F.W.; Mcgibbon, C.A.; Krebs, D.E. Kinetic analysis of planned gait termination in healthy subjects and patients with balance disorders. Gait Posture 2003, 17, 170–179. [Google Scholar] [CrossRef]
- Perry, S.D.; Radtke, A.; Goodwin, C.R. Influence of footwear midsole material hardness on dynamic balance control during unexpected gait termination. Gait Posture 2007, 25, 94–98. [Google Scholar] [CrossRef]
- Keijsers, N.L.W.; Stolwijk, N.M.; Pataky, T.C. Linear dependence of peak, mean, and pressure–time integral values in plantar pressure images. Gait Posture 2010, 31, 140–142. [Google Scholar] [CrossRef]
- Fekete, G.; Sun, D.; Liu, G.J.; Gu, Y.D.; Balassa, G.P.; Biro, I.; Neis, P.D.; Janosi, E. Preliminary results of size and slide-roll effect on the kinematics of total knee replacements. Acta Polytech. Hung. 2018, 15, 143–153. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total | Groups | p Value * | |
|---|---|---|---|---|
| Stiff arches | Flexible arches | |||
| Number (n) | 61 | 19 | 17 | NA |
| Age (y) | 23.40 ± 0.82 | 23.66 ± 1.03 | 23.50 ± 0.55 | 0.736 |
| Height (cm) | 179.20 ± 4.67 | 182.33 ± 4.13 | 177.33 ± 4.32 | 0.068 |
| Weight (kg) | 73.85 ± 7.11 | 75.83 ± 2.32 | 72.33 ± 5.54 | 0.193 |
| Body mass index (kg/m2) | 22.97 ± 1.72 | 22.82 ± 0.66 | 23.00 ± 1.56 | 0.797 |
| Foot length (mm) | 262.75 ± 4.99 | 265.00 ± 4.47 | 262.50 ± 4.18 | 0.341 |
| ASI | 1557.53 ± 464.40 | 2153.99 ± 345.26 | 1154.67 ± 131.19 | 0.000* |
| RIR (%) | Stiff arches | Flexible arches | 95% CI | p Value | ES d | |||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||||
| Walking | rearfoot | 19.57 | 5.12 | 24.10 | 3.69 | (−5.85,−3.22) | 0.000 * | 1.02 |
| midfoot | 4.30 | 1.12 | 4.80 | 1.54 | (−0.90,−0.11) | 0.013 * | 0.37 | |
| forefoot | 76.03 | 5.43 | 71.09 | 4.13 | (3.52,6.36) | 0.000 * | 1.02 | |
| Running | rearfoot | 15.26 | 2.91 | 15.63 | 2.84 | (−1.22,0.48) | 0.389 | 0.13 |
| midfoot | 3.96 | 1.43 | 4.46 | 1.48 | (−0.93,−0.07) | 0.022 * | 0.34 | |
| forefoot | 80.78 | 3.29 | 79.91 | 3.67 | (−0.16,1.90) | 0.096 | 0.25 | |
| PGT | rearfoot | 29.18 | 11.46 | 24.35 | 5.43 | (2.18,7.47) | 0.000 * | 0.54 |
| midfoot | 8.10 | 2.23 | 5.98 | 1.61 | (1.55,2.70) | 0.000 * | 1.09 | |
| forefoot | 62.67 | 12.24 | 69.84 | 6.39 | (−10.05,−4.29) | 0.000 * | 0.73 | |
| UGT | rearfoot | 26.65 | 7.37 | 22.12 | 5.23 | (2.65,6.41) | 0.000 * | 0.71 |
| midfoot | 4.58 | 1.24 | 4.67 | 1.46 | (−0.48,0.31) | 0.680 | 0.07 | |
| forefoot | 68.77 | 7.22 | 73.22 | 5.47 | (−6.33,−2.56) | 0.000 * | 0.69 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cen, X.; Xu, D.; Baker, J.S.; Gu, Y. Association of Arch Stiffness with Plantar Impulse Distribution during Walking, Running, and Gait Termination. Int. J. Environ. Res. Public Health 2020, 17, 2090. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062090
Cen X, Xu D, Baker JS, Gu Y. Association of Arch Stiffness with Plantar Impulse Distribution during Walking, Running, and Gait Termination. International Journal of Environmental Research and Public Health. 2020; 17(6):2090. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062090
Chicago/Turabian StyleCen, Xuanzhen, Datao Xu, Julien S. Baker, and Yaodong Gu. 2020. "Association of Arch Stiffness with Plantar Impulse Distribution during Walking, Running, and Gait Termination" International Journal of Environmental Research and Public Health 17, no. 6: 2090. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062090