Effect of Steamed Potato Bread Intake on Glucose, Lipids, and Urinary Na+ and K+: A Randomized Controlled Trial with Adolescents

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
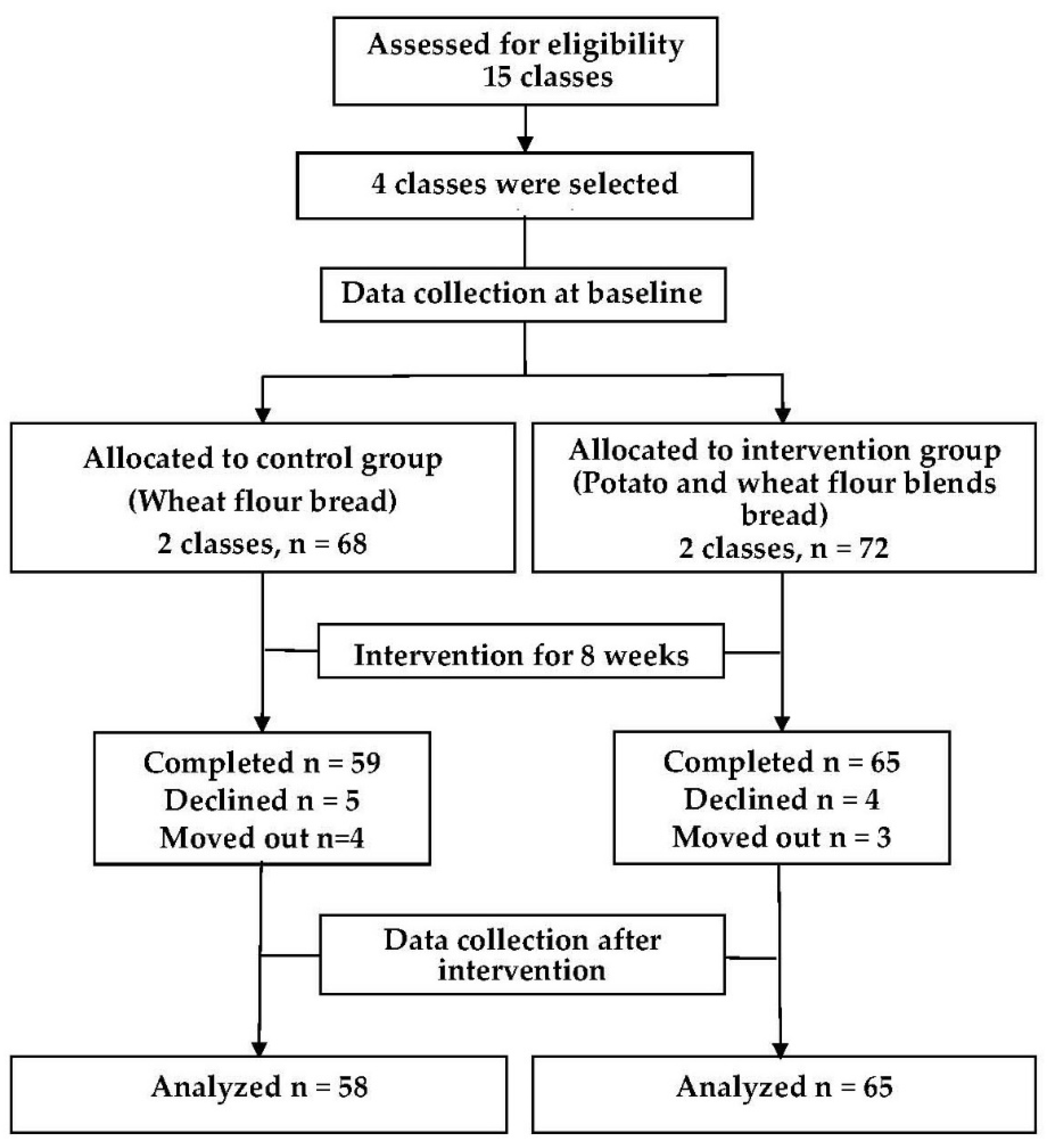
2.1. Study Design (Study Participants)
2.2. Assessment of Intervention Effects
2.3. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Physical Measurement
3.3. Blood Indicators
3.4. Urinary Sodium and Potassium
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Agricultural Marketing Resource Center. Potato Profile. 2019. Available online: https://www.agmrc.org/commodities-products/vegetables/potatoes/ (accessed on 22 October 2019).
- Camire, M.E.; Kubow, S.; Donnelly, D.J. Potatoes and human health. Crit. Rev. Food Sci. Nutr. 2009, 49, 823–840. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. The Nutrient Rich Foods Index helps to identify healthy, affordable foods. Am. J. Clin. Nutr. 2010, 91, 1095S–1101S. [Google Scholar] [CrossRef] [PubMed]
- McGill, C.R.; Kurilich, A.C.; Davignon, J. The role of potatoes and potato components in cardiometabolic health: A review. Ann. Med. 2013, 45, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Gao, B.; Huang, W.; Xue, X.; Hu, Y.; Huang, Y.; Wang, L.; Ding, S.; Cui, S. Comprehensive Environmental Assessment of Potato as Staple Food Policy in China. Int. J. Environ. Res. Public Health 2019, 16, 2700. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Wang, X.; Ma, G. Nutrition feasibility analysis of development of potato as a staple food. Food Nutr. China 2015, 21, 13–17. [Google Scholar]
- Ijah, U.J.; Auta, H.S.; Aduloju, M.O.; Aransiola, S.A. Microbiological, nutritional, and sensory quality of bread produced from wheat and potato flour blends. Int. J. Food Sci. 2014, 2014, 671701. [Google Scholar] [CrossRef] [Green Version]
- Kabira, J.N.; Imungi, J.K. Possibility of incorporating potato flour into three traditional Kenyan foods. Afr. Study Monogr. 1991, 12, 211–217. [Google Scholar]
- Furrer, A.N.; Chegeni, M.; Ferruzzi, M.G. Impact of potato processing on nutrients, phytochemicals, and human health. Crit. Rev. Food Sci. Nutr. 2018, 58, 146–168. [Google Scholar] [CrossRef]
- Curti, E.; Carini, E.; Diantom, A.; Vittadini, E. The use of potato fibre to improve bread physico-chemical properties during storage. Food Chem. 2016, 195, 64–70. [Google Scholar] [CrossRef]
- Willett, W.C. The dietary pyramid: Does the foundation need repair? Am. J. Clin. Nutr. 1998, 68, 218–219. [Google Scholar] [CrossRef] [Green Version]
- Forbes, G.B. The potato’s placement in the dietary pyramid. Am. J. Clin. Nutr. 1999, 69, 572–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, J.C.; Slavin, J.L. White potatoes, human health, and dietary guidance. Adv. Nutr. 2013, 4, 393S–401S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, W.; Tobias, D.K.; Hu, F.B.; Chavarro, J.E.; Zhang, C. Pre-pregnancy potato consumption and risk of gestational diabetes mellitus: Prospective cohort study. BMJ 2016, 352, h6898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinese Nutrition Society. Dietary Guidelines for Chinese (2016 edition), 1st ed.; People’s Medical Publication House: Beijing, China, 2017; pp. 2–29. [Google Scholar]
- Ylönen, S.K.; Virtanen, S.M.; Groop, L.; Botnia Research Group. The intake of potatoes and glucose metabolism in subjects at high risk for Type 2 diabetes. Diabet Med. 2007, 24, 1049–1050. [Google Scholar] [CrossRef] [PubMed]
- Halton, T.L.; Willett, W.C.; Liu, S.; Manson, J.E.; Stampfer, M.J.; Hu, F.B. Potato and french fry consumption and risk of type 2 diabetes in women. Am. J. Clin. Nutr. 2006, 83, 284–290. [Google Scholar] [CrossRef]
- Montonen, J.; Järvinen, R.; Heliövaara, M.; Reunanen, A.; Aromaa, A.; Knekt, P. Food consumption and the incidence of type II diabetes mellitus. Eur. J. Clin. Nutr. 2005, 59, 441–448. [Google Scholar] [CrossRef]
- Xu, H.; Li, Y.; Zhang, Q.; Hu, X.; Liu, A.; Du, S.; Li, T.; Guo, H.; Li, Y.; Xu, G.; et al. Comprehensive school-based intervention to control overweight and obesity in China: A cluster randomized controlled trial. Asia Pac. J. Clin. Nutr. 2017, 26, 1139–1151. [Google Scholar]
- Morita, T.; Oh-hashi, A.; Takei, K.; Ikai, M.; Kasaoka, S.; Kiriyama, S. Cholesterol-lowering effects of soybean, potato and rice proteins depend on their low methionine contents in rats fed a cholesterol-free purified diet. J. Nutr. 1997, 127, 470–477. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Serdula, M.; Janket, S.J.; Cook, N.R.; Sesso, H.D.; Willett, W.C.; Manson, J.E.; Buring, J.E. A prospective study of fruit and vegetable intake and the risk of type 2 diabetes in women. Diabetes Care 2004, 27, 2993–2996. [Google Scholar] [CrossRef] [Green Version]
- Liese, A.D.; Weis, K.E.; Schulz, M.; Tooze, J.A. Food intake patterns associated with incident type 2 diabetes: The Insulin Resistance Atherosclerosis Study. Diabetes Care 2009, 32, 263–268. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Boeing, H. Potatoes and risk of chronic disease: A systematic review and dose-response meta-analysis. Eur. J. Nutr. 2019, 58, 2243–2251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhadnejad, H.; Teymoori, F.; Asghari, G.; Mirmiran, P.; Azizi, F. The Association of Potato Intake with Risk for Incident Type 2 Diabetes in Adults. Can. J. Diabetes 2018, 42, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Feskens, E.J.; Virtanen, S.M.; Räsänen, L.; Tuomilehto, J.; Stengård, J.; Pekkanen, J.; Nissinen, A.; Kromhout, D. Dietary factors determining diabetes and impaired glucose tolerance. A 20-year follow-up of the Finnish and Dutch cohorts of the Seven Countries Study. Diabetes Care 1995, 18, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Arvaniti, F.; Stefanadis, C. Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesteremia, diabetes and obesity, among adults; the accuracy of the MedDietScore. Prev. Med. 2007, 44, 335–340. [Google Scholar] [CrossRef]
- Morimoto, A.; Ohno, Y.; Tatsumi, Y.; Mizuno, S.; Watanabe, S. Effects of healthy dietary pattern and other lifestyle factors on incidence of diabetes in a rural Japanese population. Asia Pac. J. Clin. Nutr. 2012, 21, 601–608. [Google Scholar]
- Hashemian, M.; Murphy, G.; Etemadi, A.; Liao, L.M.; Dawsey, S.M.; Malekzadeh, R.; Abnet, C.C. Potato consumption and the risk of overall and cause specific mortality in the NIH-AARP study. PLoS ONE 2019, 14, e0216348. [Google Scholar] [CrossRef] [Green Version]
- Borgi, L.; Rimm, E.B.; Willett, W.C.; Forman, J.P. Potato intake and incidence of hypertension: Results from three prospective US cohort studies. BMJ 2016, 353, i2351. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International tables of glycemic index and glycemic load values:2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [Green Version]
- Lin Ek, K.; Wang, S.; Brand-Miller, J.; Copeland, L. Properties of starch from potatoes differing in glycemic index. Food Funct. 2014, 5, 2509–2515. [Google Scholar] [CrossRef]
- Holt, S.H.; Miller, J.C.; Petocz, P. An insulin index of foods: The insulin demand generated by 1000-kJ portions of common foods. Am. J. Clin. Nutr. 1997, 66, 1264–1276. [Google Scholar] [CrossRef]
- Riccardi, G.; Rivellese, A.A.; Giacco, R. Role of glycemic index and glycemic load in the healthy state, in prediabetes, and in diabetes. Am. J. Clin. Nutr. 2008, 87, 269S–274S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.; Manson, J.; Liu, S. Glycemic index, glycemic load, and risk of type 2 diabetes. Am. J. Clin. Nutr. 2002, 76, 274S–280S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceriello, A.; Esposito, K.; Piconi, L.; Ihnat, M.A.; Thorpe, J.E.; Testa, R.; Boemi, M.; Giugliano, D. Oscillating glucose is more deleterious to endothelial function and oxidative stress than mean glucose in normal and type 2 diabetic patients. Diabetes 2008, 57, 1349–1354. [Google Scholar] [CrossRef] [Green Version]
- Sahota, P.; Gatenby, L.A.; Greenwood, D.C.; Bryant, M.; Robinson, S.; Wright, J. Ethnic differences in dietary intake at age 12 and 18 months: The Born in Bradford 1000 Study. Public Health Nutr. 2016, 19, 114–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villegas, R.; Liu, S.; Gao, Y.T.; Yang, G.; Li, H.; Zheng, W.; Shu, X.O. Prospective study of dietary carbohydrates, glycemic index, glycemic load, and incidence of type 2 diabetes mellitus in middle-aged Chinese women. Arch. Intern. Med. 2007, 167, 2310–2316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pokorn, J.; Pánek, J.; Trojáková, L. Effect of food component changes during frying on the nutrition value of fried food. Forum Nutr. 2003, 56, 348–350. [Google Scholar]
- Raigond, P.; Ezekiel, R.; Raigond, B. Resistant starch in food: A review. J. Sci. Food Agric. 2015, 95, 1968–1978. [Google Scholar] [CrossRef]
- Tian, J.; Chen, J.; Ye, X.; Chen, S. Health benefits of the potato affected by domestic cooking: A review. Food Chem. 2016, 202, 165–175. [Google Scholar] [CrossRef]
- Boers, H.M.; van Dijk, T.H.; Hiemstra, H.; Hoogenraad, A.R.; Mela, D.J.; Peters, H.; Vonk, R.J.; Priebe, M.G. Effect of fibre additions to flatbread flour mixes on glucose kinetics: A randomised controlled trial. Br. J. Nutr. 2017, 118, 777–787. [Google Scholar] [CrossRef] [Green Version]
- Strazzullo, P.; D’Elia, L.; Kandala, N.B.; Cappuccio, F.P. Salt intake, stroke, and cardiovascular disease: Meta-analysis of prospective studies. BMJ 2009, 339, b4567. [Google Scholar] [CrossRef] [Green Version]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwahori, T.; Ueshima, H.; Torii, S.; Saito, Y.; Kondo, K.; Tanaka-Mizuno, S.; Arima, H.; Miura, K. Diurnal variation of urinary sodium-to-potassium ratio in free-living Japanese individuals. Hypertens. Res. 2017, 40, 658–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gijsbers, L.; Dower, J.I.; Schalkwijk, C.G.; Kusters, Y.H.; Bakker, S.J.; Hollman, P.C.; Geleijnse, J.M. Effects of sodium and potassium supplementation on endothelial function: A fully controlled dietary intervention study. Br. J. Nutr. 2015, 114, 1419–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Nutrients | Wheat Bread | Potato Bread |
|---|---|---|
| Energy (kcal) | 221.1 | 201.0 |
| Water (g) | 45.7 | 49.7 |
| Protein (g) | 7.5 | 6.7 |
| Fat (g) | 1.1 | 1.0 |
| Carbohydrate (g) | 43.9 | 39.5 |
| Fiber (g) | 1.36 | 2.39 |
| Vitamin C (mg) | <0.044 | <0.044 |
| β-Carotene (μg) | <2.00 | <2.00 |
| Vitamin E (mg) | 0.387 | 0.266 |
| Vitamin B1 (mg) | 0.02 | 0.10 |
| Vitamin B2 (mg) | 0.01 | 0.03 |
| Ash (g) | 0.44 | 0.74 |
| Sodium (mg) | 74.07 | 81.36 |
| Potassium (mg) | 61.34 | 159.48 |
| Calcium (mg) | 11.88 | 12.27 |
| Iron (mg) | 0.60 | 0.71 |
| Characteristics | Control Group | Intervention Group |
|---|---|---|
| Total (N) | 58 | 65 |
| Sex (N (%)) # | ||
| Boys | 23 (39.0) | 45 (69.2) ** |
| Girls | 36 (61.0) | 20 (30.8) |
| Nation (N (%)) # | ||
| Han people | 54 (94.7) | 61 (95.3) |
| Minority | 3 (5.3) | 3 (4.7) |
| Menarche/spermorrhea (N (%)) # | ||
| Yes | 56 (94.9) | 57 (87.7) |
| No | 3 (5.1) | 8 (12.3) |
| Age (year, Mean (SD)) † | 16.2 (0.5) | 16.4 (0.6) |
| Height (cm, Mean (SD)) † | 161.5 (7.8) | 168.3 (7.9) * |
| Weight (kg, Mean (SD)) † | 53.3 (8.2) | 60.5 (11.9) * |
| BMI (kg/m2, Mean (SD)) | 20.4 (2.5) | 21.2 (3.4) |
| Bread intake (g/day, Mean (SD)) † | 119.4 (47.3) | 160.8 (70.1) * |
| Energy provided by bread (kcal/day, Mean (SD)) † | 264.0 (104.6) | 323.3 (140.9) * |
| Nutrients | Control Group | Intervention Group | p-Value |
|---|---|---|---|
| Energy (kcal) | 264.0 (104.6) | 323.3 (140.9) | 0.003 |
| Protein (g) | 8.9 ± 3.5 | 10.8 ± 4.4 | 0.005 |
| Fat (g) | 1.3 ± 0.5 | 1.6 ± 0.7 | 0.003 |
| Carbohydrate (g) | 52.3 ± 20.4 | 64.0 ± 25.7 | 0.004 |
| Fiber (g) | 1.62 ± 0.63 | 3.87 ± 1.55 | <0.001 |
| Vitamin E (mg) | 0.46 ± 0.18 | 0.43 ± 0.17 | 0.317 |
| Vitamin B1 (mg) | 0.02 ± 0.01 | 0.16 ± 0.07 | <0.001 |
| Vitamin B2 (mg) | 0.01 ± 0 | 0.05 ± 0.02 | <0.001 |
| Sodium (mg) | 88.32 ± 34.44 | 131.71 ± 52.92 | <0.001 |
| Potassium (mg) | 73.14 ± 28.52 | 258.18 ± 103.74 | <0.001 |
| Calcium (mg) | 14.16 ± 5.52 | 19.86 ± 7.98 | <0.001 |
| Iron (mg) | 0.72 ± 0.28 | 1.15 ± 0.46 | <0.001 |
| Subgroups | Variables | Control Group | Intervention Group | Effect | |||
|---|---|---|---|---|---|---|---|
| Baseline | Changes | Baseline | Changes | Beta (95% CI) | p-Value | ||
| Overall | Weight (kg) | 53.3 ± 8.2 | 1.9 ± 1.4 ** | 60.5 ± 12.1 | 1.9 ± 2.0 ** | 0.1 (−0.6, 0.7) | 0.831 |
| Height (cm) | 161.5 ± 7.8 | 1.8 ± 0.8 ** | 168.3 ± 8.0 | 1.7 ± 1.1 ** | 0 (−0.4, 0.3) | 0.858 | |
| BMI (kg/m2) | 20.4 ± 2.5 | 0.3 ± 0.6 ** | 21.2 ± 3.4 | 0.2 ± 0.8 * | 0 (−0.3, 0.2) | 0.738 | |
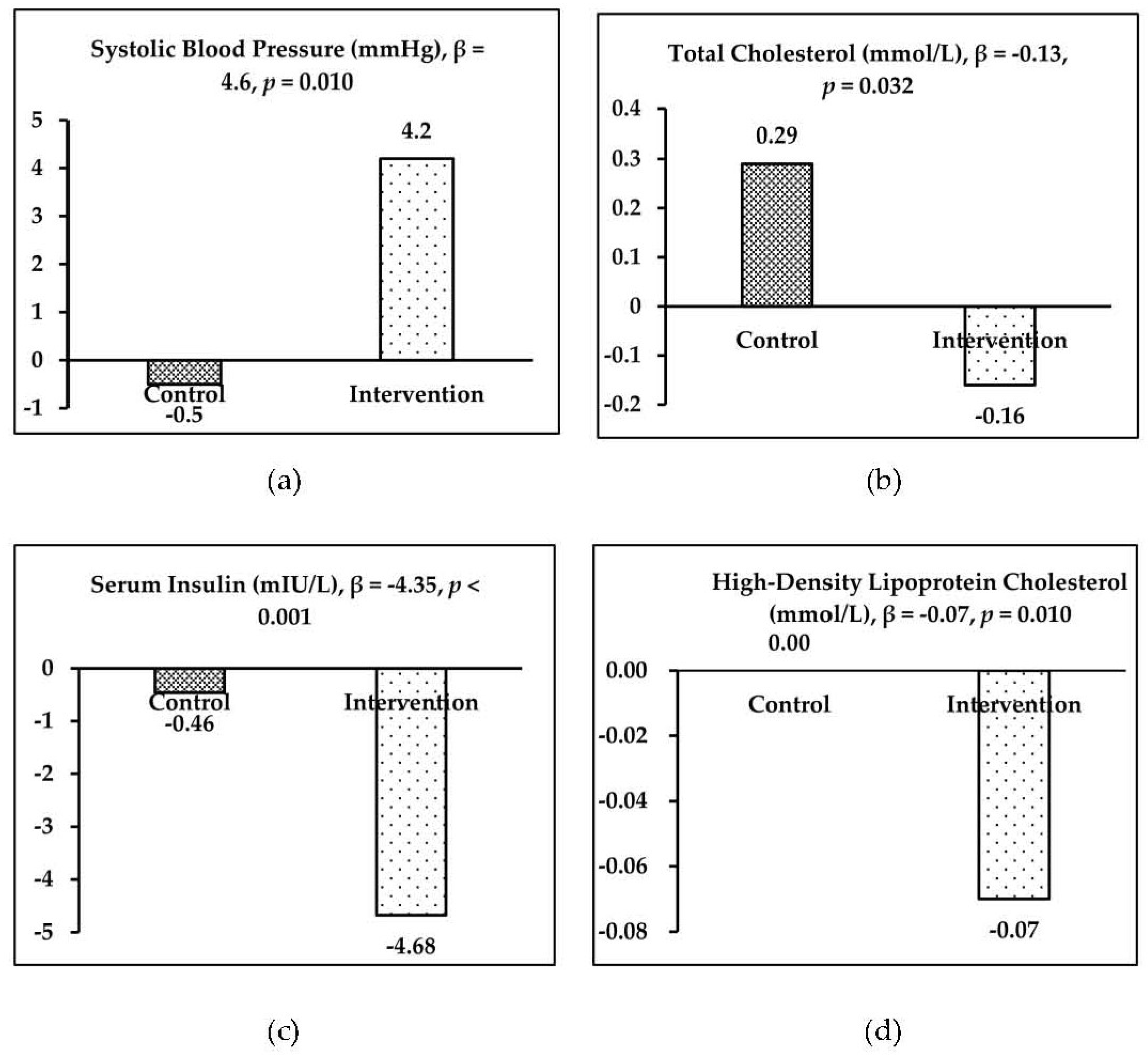
| SBP (mmHg) | 119.6 ± 9.3 | −0.5 ± 0.3 | 118.8 ± 8.9 | 4.2 ± 8.8 ** | 4.6 (1.1, 8.0) | 0.010 | |
| DBP (mmHg) | 75.6 ± 8.0 | −1.9 ± 8.7 | 77.4 ± 9.2 | −3.2 ± 9.2 ** | −1.3 (−4.6, 2.0) | 0.431 | |
| GLU (mmol/L) | 4.45 ± 0.3 | 0.53 ± 0.28 ** | 4.40 ± 0.37 | 0.46 ± 0.36 ** | −0.07 (−0.19, 0.04) | 0.215 | |
| INS (mIU/L) | 11.38 ± 3.1 | −0.46 ± 3.00 | 14.31 ± 4.34 | −4.68 ± 2.98 ** | −4.35 (−5.31, −3.14) | <0.001 | |
| CHO (mmol/L) | 3.42 ± 0.55 | 0.29 ± 0.33 ** | 3.39 ± 0.49 | 0.16 ± 0.35 ** | −0.13 (−0.26, −0.01) | 0.032 | |
| HDL-c (mmol/L) | 1.32 ± 0.26 | 0.00 ± 0.16 | 1.24 ± 0.25 | −0.07 ± 0.14 ** | −0.07 (−0.13, −0.02) | 0.010 | |
| LDL-c (mmol/L) | 1.70 ± 0.5 | 0.08 ± 0.43 | 1.75 ± 0.42 | −0.02 ± 0.23 ** | −0.10 (−0.23, 0.03) | 0.132 | |
| TG (mmol/L) | 0.78 ± 0.25 | 0.0 ± 0.24 | 0.82 ± 0.28 | 0.06 ± 0.27 | 0.06 (−0.03, 0.15) | 0.198 | |
| Urinary Na+ (mmol/L) | 150.6 ± 70.3 | 26.6 ± 89.7 * | 187.6 ± 80.4 | 22.5 ± 87.2 | −4.2 (−38.3, 30.0) | 0.809 | |
| Urinary K+ (mmol/L) | 21.6 ± 17.6 | 1.0 ± 22.2 | 26.6 ± 17.5 | −0.7 ± 20.8 | −1.7 (−10.0, 6.6) | 0.689 | |
| Urinary NA+/K+ | 9.4 ± 4.4 | 1.5 ± 6.0 | 8.7 ± 3.9 | 1.9 ± 5.7 * | 0.5 (−1.8, 2.7) | 0.687 | |
| Boys | Weight (kg) | 59.0 ± 9.4 | 1.4 ± 1.4 ** | 63.7 ± 12.8 | 1.8 ± 2.0 ** | 0.3 (−0.6, 1.3) | 0.478 |
| Height (cm) | 169.4 ± 4.8 | 2.0 ± 0.9 ** | 171.7 ± 6.7 | 2.0 ± 1.2 ** | 0 (−0.6, 0.6) | 0.959 | |
| BMI (kg/m2) | 20.6 ± 3.2 | 0 ± 0.5 | 21.6 ± 3.9 | 0.1 ± 0.8 | 0.1 (−0.3, 0.4) | 0.660 | |
| SBP (mmHg) | 120.7 ± 8.4 | −0.4 ± 9.7 | 120.3 ± 7.3 | 4.5 ± 9.1 * | 4.9 (0, 9.8) | 0.049 | |
| DBP (mmHg) | 74.4 ± 8.6 | −3.3 ± 8.9 | 76.8 ± 9.5 | −1.9 ± 9.8 | 1.4 (−3.6, 6.4) | 0.580 | |
| GLU (mmol/L) | 4.36 ± 0.29 | 0.72 ± 0.30 ** | 4.42 ± 0.4 | 0.41 ± 0.37 ** | −0.31 (−0.49, −0.13) | 0.001 | |
| INS (mIU/L) | 10.02 ± 1.91 | 0.71 ± 2.46 | 14.96 ± 4.89 | −5.25 ± 2.88 ** | −5.95 (−7.39, −4.51) | <0.001 | |
| CHO (mmol/L) | 3.10 ± 0.56 | 0.40 ± 0.23 ** | 3.29 ± 0.44 | 0.12 ± 0.32 * | −0.28 (−0.43, −0.13) | <0.001 | |
| HDL-c(mmol/L) | 1.23 ± 0.23 | 0.05 ± 0.15 | 1.15 ± 0.2 | −0.08 ± 0.13 ** | −0.13 (−0.2, −0.05) | 0.001 | |
| LDL-c(mmol/L) | 1.47 ± 0.54 | 0.21 ± 0.29 | 1.70 ± 0.39 | −0.03 ± 0.22 ** | −0.24 (−0.37, −0.11) | <0.001 | |
| TG (mmol/L) | 0.75 ± 0.24 | −0.05 ± 0.21 | 0.89 ± 0.28 | 0 ± 0.22 | 0.05 (−0.06, 0.17) | 0.338 | |
| Urinary Na+ (mmol/L) | 139.8 ± 57.3 | 45.1 ± 78.9 * | 189.6 ± 80.4 | 21.0 ± 86.1 | −24.1 (−68.2, 19.9) | 0.278 | |
| Urinary K+ (mmol/L) | 20.2 ± 16.2 | 1.9 ± 24.5 | 27.3 ± 18.9 | −2.5 ± 19.5 | −4.4 (−15.6, 6.8) | 0.436 | |
| Urinary NA+/K+ | 9.0 ± 4.1 | 1.9 ± 5.1 | 8.8 ± 4.0 | 2.1 ± 5.2 * | 0.2 (−2.5, 2.9) | 0.896 | |
| Girls | Weight (kg) | 49.8 ± 4.9 | 2.1 ± 1.4 ** | 53.5 ± 6.4 | 2.3 ± 2.2 ** | 0.1 (−1, 1.3) | 0.787 |
| Height (cm) | 156.7 ± 4.8 | 1.6 ± 0.8 ** | 161.0 ± 5.2 | 1.3 ± 0.7 ** | −0.4 (−0.8, 0.1) | 0.087 | |
| BMI (kg/m2) | 20.3 ± 2.0 | 0.4 ± 0.5 ** | 20.6 ± 2.1 | 0.5 ± 0.8 ** | 0.1 (−0.3, 0.5) | 0.663 | |
| SBP (mmHg) | 118.9 ± 9.9 | −0.3 ± 10.7 | 115.6 ± 11.3 | 3.6 ± 8.5 | 3.9 (−1.7, 9.5) | 0.168 | |
| DBP (mmHg) | 76.4 ± 7.6 | −0.9 ± 8.6 | 78.7 ± 8.8 | −5.7 ± 7.6 ** | −4.8 (−9.4, −0.1) | 0.044 | |
| GLU (mmol/L) | 4.50 ± 0.30 | 0.41 ± 0.20 ** | 4.36 ± 0.29 | 0.57 ± 0.33 ** | 0.15 (−0.01, 0.32) | 0.069 | |
| INS (mIU/L) | 12.27 ± 3.42 | −1.21 ± 3.10 * | 12.84 ± 2.19 | −3.47 ± 2.90 ** | −2.26 (−3.98, −0.55) | 0.010 | |
| CHO (mmol/L) | 3.64 ± 0.43 | 0.22 ± 0.36 ** | 3.61 ± 0.54 | 0.24 ± 0.41 * | 0.02 (−0.2, 0.23) | 0.882 | |
| HDL-c (mmol/L) | 1.38 ± 0.27 | −0.03 ± 0.15 | 1.44 ± 0.24 | −0.06 ± 0.16 | −0.03 (−0.11, 0.06) | 0.540 | |
| LDL-c (mmol/L) | 1.84 ± 0.42 | −0.01 ± 0.48 | 1.87 ± 0.45 | 0 ± 0.26 | 0.01 (−0.22, 0.25) | 0.909 | |
| TG (mmol/L) | 0.79 ± 0.26 | 0.03 ± 0.26 | 0.67 ± 0.23 | 0.17 ± 0.32* | 0.15 (−0.01, 0.31) | 0.071 | |
| Urinary Na+ (mmol/L) | 157.8 ± 77.7 | 11.6 ± 96.5 | 182.3 ± 82.7 | 26.7 ± 93.2 | 15.1 (−46.9, 77.2) | 0.624 | |
| Urinary K+ (mmol/L) | 22.5 ± 18.6 | 0.3 ± 20.7 | 24.9 ± 13.4 | 4.4 ± 24.1 | 4.1 (−10.1, 18.4) | 0.561 | |
| Urinary NA+/K+ | 9.7 ± 4.6 | 1.1 ± 6.8 | 8.5 ± 3.6 | 1.5 ± 7.3 | 0.4 (−4.1, 4.9) | 0.864 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, H.; Guo, Y.; Lu, S.; Ma, Y.; Wang, X.; Zhao, L.; Sun, J. Effect of Steamed Potato Bread Intake on Glucose, Lipids, and Urinary Na+ and K+: A Randomized Controlled Trial with Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 2096. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062096
Xu H, Guo Y, Lu S, Ma Y, Wang X, Zhao L, Sun J. Effect of Steamed Potato Bread Intake on Glucose, Lipids, and Urinary Na+ and K+: A Randomized Controlled Trial with Adolescents. International Journal of Environmental Research and Public Health. 2020; 17(6):2096. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062096
Chicago/Turabian StyleXu, Haiquan, Yanzhi Guo, Shijun Lu, Yunqian Ma, Xiuli Wang, Liyun Zhao, and Junmao Sun. 2020. "Effect of Steamed Potato Bread Intake on Glucose, Lipids, and Urinary Na+ and K+: A Randomized Controlled Trial with Adolescents" International Journal of Environmental Research and Public Health 17, no. 6: 2096. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062096