Boda Bodas and Road Traffic Injuries in Uganda: An Overview of Traffic Safety Trends from 2009 to 2017

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Police Reports
2.3. Inpatient Database
2.4. Data Analysis
3. Results
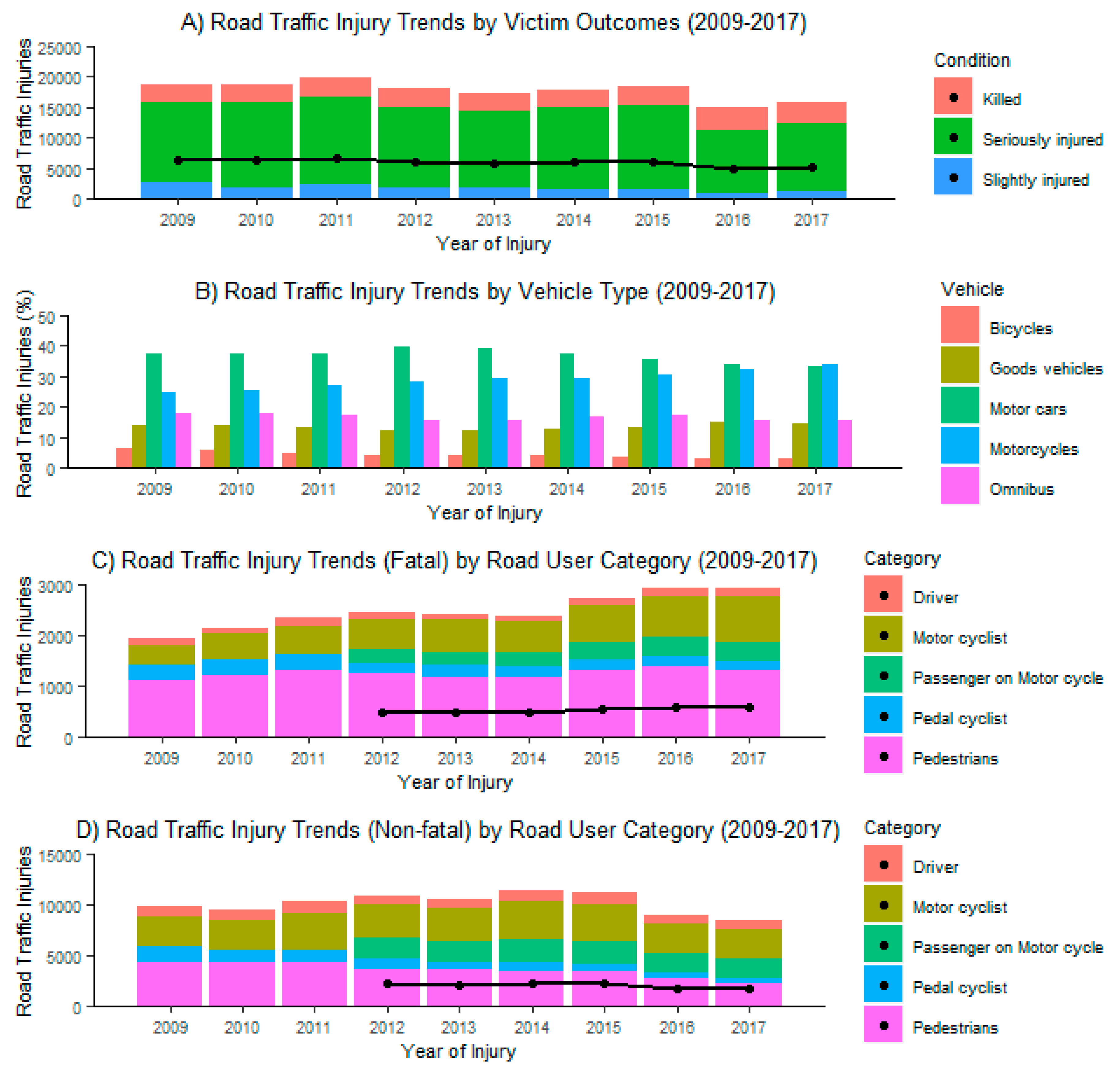
3.1. Police Reports
3.1.1. Demographics
3.1.2. Boda Boda Involvement in RTIs
3.1.3. Mortality
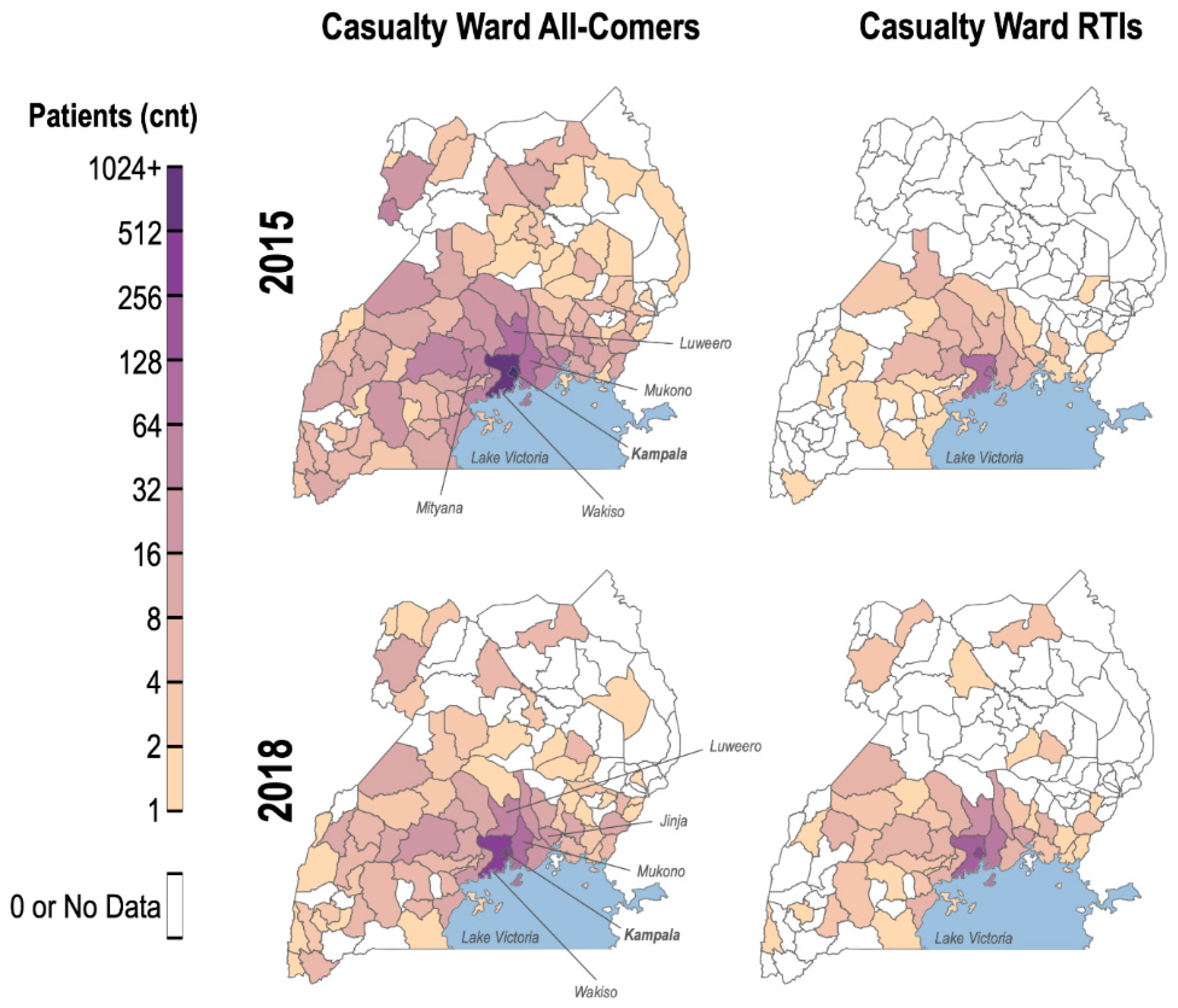
3.2. Casualty Ward Database
4. Discussion
4.1. Trends in RTIs OverTtime
4.2. Literature Review of Ugandan RTI and Boda Bodas
4.3. Motorcycle Helmet Usage in Uganda
4.4. The Impact of Government Road Safety Initiatives: Operation Fika Salama
4.5. Neurosurgical Care in Uganda
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Health Organization Global status report on road safety 2018. Available online: https://www.who.int/violence_injury_prevention/road_safety_status/2018/English-Summary-GSRRS2018.pdf. (accessed on 24 January 2020).
- Dalal, K.; Svanström, L. Economic Burden of Disability Adjusted Life Years (DALYs) of Injuries. Health (Irvine. Calif) 2015, 7, 487–494. [Google Scholar] [CrossRef] [Green Version]
- Hyder, A.A.; Wunderlich, C.A.; Puvanachandra, P.; Gururaj, G.; Kobusingye, O.C. The impact of traumatic brain injuries: a global perspective. NeuroRehabilitation 2007, 22, 341–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nantulya, V.M. The neglected epidemic: road traffic injuries in developing countries. BMJ 2002, 324, 1139–1141. [Google Scholar] [CrossRef] [Green Version]
- Galukande, M.; Jombwe, J.; Fualal, J.; Gakwaya, A. Boda-boda injuries a health problem and a burden of disease in Uganda: A tertiary hospital survey. J. Surgery 2009, 14, 33–37. [Google Scholar]
- Chalya, P.L.; Mabula, J.B.; Dass, R.M.; Mbelenge, N.; Ngayomela, I.H.; Chandika, A.B.; Gilyoma, J.M. Injury characteristics and outcome of road traffic crash victims at Bugando Medical Centre in Northwestern Tanzania. J. Trauma Manag. Outcomes 2012, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naddumba E, K. A Cross-Sectional Retrospective Study of Boda Boda Injuries At Mulago Hospital IN Kampala-Uganda. East Cent. African J. Surg. 2001, 9, 1–4. [Google Scholar]
- Kitara, D.L. Boda Boda Injuries in Gulu Regional Hospital, Northern Uganda. East Cent. African J. Surg. 2011, 16, 97–101. [Google Scholar]
- Tran, T.M.; Fuller, A.T.; Kiryabwire, J.; Mukasa, J.; Muhumuza, M.; Ssenyojo, H.; Haglund, M.M. Distribution and characteristics of severe traumatic brain injury at mulago national referral hospital in Uganda. World Neurosurg. 2015, 83, 269–277. [Google Scholar] [CrossRef]
- Kigera, L.; Nguku, E.K.N. The Impact of Bodaboda Motor Crashes on the Budget for Clinical Services at Mulago. East Cent. African J. Surg. 2010, 15, 57–61. [Google Scholar]
- Afukaar, F.K. Speed control in developing countries: issues, challenges and opportunities in reducing road traffic injuries. Inj. Control Saf. Promot. 2003, 10, 77–81. [Google Scholar] [CrossRef]
- Waters, H.R.; Hyder, A.A.; Phillips, T.L. Economic evaluation of interventions to reduce road traffic injuries - A review of the literature with applications to low and middle-income countries. Asia-Pacific J. Public Heal. 2004, 16, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.C.; Ivers, R.; Norton, R.; Boufous, S.; Blows, S.; Lo, S.K. Helmets for preventing injury in motorcycle riders. Cochrane Database Syst. Rev. 2008.
- Kamulegeya, L.H.; Kizito, M.; Nassali, R.; Bagayana, S.; Elobu, A.E. The scourge of head injury among commercial motorcycle riders in Kampala; A preventable clinical and public health menace. Afr. Health Sci. 2015, 15, 1016–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uganda Police. Uganda Police Force Annual Traffic Report 2010; Uganda Police Force: Kampala, Uganda, 2011. [Google Scholar]
- Uganda Police. Uganda Police Force Annual Traffic Report 2011; Uganda Police Force: Kampala, Uganda, 2012. [Google Scholar]
- Uganda Police. Uganda Police Force Annual Traffic Report 2012; Uganda Police Force: Kampala, Uganda, 2013. [Google Scholar]
- Uganda Police. Uganda Police Force Annual Traffic Report 2013; Uganda Police Force: Kampala, Uganda, 2014. [Google Scholar]
- Uganda Police. Uganda Police Force Annual Traffic Report 2014; Uganda Police Force: Kampala, Uganda, 2015. [Google Scholar]
- Uganda Police. Uganda Police Force Annual Traffic Report 2015; Uganda Police Force: Kampala, Uganda, 2016. [Google Scholar]
- Uganda Police. Uganda Police Force Annual Traffic Report 2016; Uganda Police Force: Kampala, Uganda, 2017. [Google Scholar]
- Uganda Police. Uganda Police Force Annual Traffic Report 2017; Uganda Police Force: Kampala, Uganda, 2018. [Google Scholar]
- UBOS Uganda Bureau of Statistics; 2011 Statistical Abstract. Uganda Bur. Stat. Stat. 2013, 1, 38–40.
- UBOS Uganda Bureau of Statistics. The 2018 Statistical Abstract. 2018, 345.
- Roehler, D.R.; Naumann, R.B.; Mutatina, B.; Nakitto, M.; Mwanje, B.; Brondum, L.; Blanchard, C.; Baldwin, G.T.; Dellinger, A.M. Using baseline and formative evaluation data to inform the Uganda Helmet Vaccine Initiative. Glob. Health Promot. 2013, 20, 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adogu, P.O.; Ilika, A.L.; Asuzu, A.L. Predictors of road traffic accident, road traffic injury and death among commercial motorcyclists in an urban area of Nigeria. Niger. J. Med. 2009, 18, 393–397. [Google Scholar] [CrossRef]
- Nordfjærn, T.; Jørgensen, S.; Rundmo, T. Cultural and socio-demographic predictors of car accident involvement in Norway, Ghana, Tanzania and Uganda. Saf. Sci. 2012, 50, 1862–1872. [Google Scholar] [CrossRef]
- Haworth, N.; Ozanne-smith, J.; Fox, B.; Brumen, I. Motorcycle-Related Injuries to Children and Adolescents; Monash University Accident Research Centre: Melbourne, Australia, 1994; ISBN 0732600553. Available online: https://www.monash.edu/__data/assets/pdf_file/0007/216574/muarc056.pdf. (accessed on 24 January 2020).
- Tran, T.M.; Fuller, A.T.; Butler, E.K.; Makumbi, F.; Luboga, S.; Muhumuza, C.; Ssennono, V.F.; Chipman, J.G.; Galukande, M.; Haglund, M.M. Burden of Surgical Conditions in Uganda: A Cross-sectional Nationwide Household Survey. Ann. Surg. 2016, 1. [Google Scholar] [CrossRef]
- Kimuli Balikuddembe, J.; Ardalan, A.; Khorasani-Zavareh, D.; Nejati Kasiima Stephen Munanura, A. Road Traffic Incidents in Uganda: A Systematic Review of a Five-Year Trend. J. Inj. Violence Res. 2017, 9, 17–25. [Google Scholar]
- Zwi, A.B.; Forjuoh, S.; Murugusampillay, S.; Odero, W.; Watts, C. Injuries in developing countries: Policy response needed now. Trans. R. Soc. Trop. Med. Hyg. 1996, 90, 593–595. [Google Scholar] [CrossRef] [Green Version]
- Baker, S.P. The man in the street: a tale of two cities. Am. J. Public Health 1975, 65, 524–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Works and Transport. The Study on Greater Kampala Road Network and Transport Improvement in the Republic of Uganda: Final Report-Executive Summary; Ministry of Works and Transport: Kampala, Uganda, 2010; p. 172. [Google Scholar]
- Ministry of Works and Transport. Statutory Instruments 2004 No. 30 the Traffic and Road Safety (Motorcycles) Regulations; Ministry of Works and Transport: Kampala, Uganda, 2004; Available online: https://www.works.go.ug/wp-content/uploads/2016/08/THE-TRAFFIC-AND-ROAD-SAFETY-MOTORCYCLES-REGULATIONS-2004.pdf. (accessed on 24 January 2020).
- Safeboda. Safeboda Observation Surve; Safeboda: Kampala, Uganda, 2016. [Google Scholar]
- Safeboda. Q2 2016 Impact Scorecard; Safeboda: Kampala, Uganda, 2016. [Google Scholar]
- Craft, G.; Van Bui, T.; Sidik, M.; Moore, D.; Ederer, D.J.; Parker, E.M.; Ballesteros, M.F.; Sleet, D.A. A comprehensive approach to motorcycle-related head injury prevention: Experiences from the field in Vietnam, Cambodia, and Uganda. Int. J. Environ. Res. Public Health 2017, 14, 1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, B.J.; Vaca, S.D.; Vissoci, J.R.N.; Staton, C.A.; Xu, L.; Muhumuza, M.; Ssenyonjo, H.; Mukasa, J.; Kiryabwire, J.; Nanjula, L.; et al. A prospective neurosurgical registry evaluating the clinical care of traumatic brain injury patients presenting to Mulago National Referral Hospital in Uganda. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Category | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 |
|---|---|---|---|---|---|---|---|---|
| Total casualties | 18,808 | 19,955 | 18,016 | 17,283 | 17,848 | 18,435 | 15,754 | 14,854 |
| Gender | ||||||||
| Male, n (%) | 14,145 (75%) | 14,785 (74%) | 13,158 (73%) | 12,709 (74%) | 13,059 (73%) | 13,558 (74%) | 11,558 (73%) | 10,862 (73%) |
| Female, n (%) | 4663 (25%) | 5170 (26%) | 4858 (27%) | 4574 (26%) | 4789 (27%) | 4877 (26%) | 4196 (27%) | 3992 (27%) |
| Age | ||||||||
| <18 | 2516 | 2634 | 2718 | 2388 | 2422 | 2480 | 2213 | 1934 |
| 18–24 | 16292 * | 17321 * | 3480 | 3078 | 3000 | 3298 | 2800 | 2553 |
| 25–34 | 5477 | 5640 | 6005 | 5808 | 5203 | 4747 | ||
| 35–44 | 3144 | 3083 | 3131 | 3274 | 2677 | 2435 | ||
| 45–54 | 1123 | 1111 | 1367 | 1391 | 1154 | 1173 | ||
| 55–64 | 392 | 412 | 467 | 599 | 484 | 574 | ||
| 65–74 | 198 | 190 | 206 | 252 | 225 | 328 | ||
| >75 | 116 | 88 | 151 | 135 | 118 | 242 | ||
| Unknown | 1368 | 1293 | 1099 | 1198 | 880 | 868 | ||
| Seasons | ||||||||
| Wet † | 11,207 | 10,870 | 9810 | 9384 | 9215 | 9272 | 6915 | 6725 |
| Dry † | 11,254 | 11,402 | 10,060 | 8984 | 9471 | 9223 | 7559 | 6519 |
| Time of RTI | ||||||||
| [0:00–5:59] | 1811 | 2058 | 1992 | 1645 | 1585 | 1599 | 1309 | 1329 |
| [6:00–11:59] | 5872 | 5780 | 5096 | 4794 | 4815 | 4685 | 3630 | 3337 |
| [12:00–17:59] | 8280 | 8097 | 6782 | 6318 | 6511 | 6535 | 5037 | 4604 |
| [17:59–23:59] | 6498 | 6337 | 6000 | 5611 | 5774 | 5676 | 4498 | 3974 |
| Wet season †: | 3–5, 9–11 | |||||||
| Dry season †: | 12–2, 6–8 | |||||||
| Age *: | adults (>18) |
| Cause (%) | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 |
|---|---|---|---|---|---|---|---|---|---|
| Careless driving | 9112 (42.0) | 9316 (41.5) | 8659 (38.9) | 8694 (42.1) | 7901 (41.0) | 8708 (42.9) | 8048 (40.6) | 6567 (45.4) | 5698 (41.6) |
| Careless pedestrian | 889 (4.1) | 881 (3.9) | 1141 (5.1) | 1079 (5.2) | 1095 (5.7) | 815 (4.0) | 885 (4.5) | 933 (6.5) | 652 (4.7) |
| Dazzled by lights | 85 (0.4) | 114 (0.5) | 152 (0.7) | 46 (0.2) | 25 (0.1) | 28 (0.1) | 44 (0.2) | 49 (0.3) | 150 (1.1) |
| Dangerous loading | - | - | 82 (0.4) | 93 (0.5) | 94 (0.5) | 117 (0.6) | 56 (0.4) | 162 (1.2) | |
| DMC * | 738 (3.4) | 720 (3.2) | 929 (4.2) | - | - | - | - | - | 475 (3.5) |
| Obstacle on carriage way | 96 (0.4) | 76 (0.3) | 266 (1.2) | 59 (0.3) | 3 (0.0) | 4 (0.0) | 6 (0.0) | 1 (0.0) | 118 (0.9) |
| Over loading | 202 * (0.9) | 240 * (1.1) | 113 * (0.5) | 29 (0.1) | 78 (0.4) | 85 (0.4) | 58 (0.3) | 30 (0.2) | 161 (1.2) |
| Over speeding | 973 (4.5) | 839 (3.7) | 867 (3.9) | 308 (1.5) | 492 (2.6) | 677 (3.3) | 954 (4.8) | 588 (4.1) | 461 (3.3) |
| Passenger falls | 228 (1.1) | 238 (1.1) | 501 (2.2) | 270 (1.3) | 296 (1.5) | 218 (1.1) | 184 (0.9) | 209 (1.4) | 390 (2.8) |
| Reckless driving | 6948 (32.0) | 6579 (29.3) | 6514 (29.3) | 5831 (28.2) | 5502 (28.6) | 5670 (27.9) | 5614 (28.3) | 5140 (35.5) | 4661 (33.9) |
| Under influence of alcohol | 249 (1.2) | 194 (0.9) | 299 (1.3) | 216 (1.1) | 208 (1.1) | 310 (1.5) | 238 (1.2) | 201 (1.4) | 234 (1.7) |
| Unknown causes | 2057 (9.5) | 2129 (9.5) | 1818 (8.2) | 2971 (14.4) | 2895 (15.1) | 2985 (14.7) | 2981 (15.0) | 701 (4.8) | 557 (4.1) |
| Weather/road conditions | 112 (0.5) | 1135 (5.0) | 1013 (4.5) | 1076 (5.2) | 646 (3.4) | 714 (3.6) | 717 (3.6) | - | - |
| Total | 21,689 | 22,461 | 22,272 | 20,661 | 19,234 | 20,308 | 19,846 | 14,475 | 13,719 |
| Category | July 2015 | July 2018 | p-Value |
|---|---|---|---|
| Casualty ward population | |||
| # of patients | 2962 | 1306 | |
| Gender | <0.001 | ||
| Male, n (%) | 1752 (59%) | 937 (72%) | |
| Female, n (%) | 1210 (41%) | 369 (28%) | |
| Age, years | 35.4 | 30.1 | <0.001 |
| Road Traffic Injuries | |||
| # of patients | 299 | 469 | |
| % of casualty ward patients | 10% | 36% | |
| Age | 29.4 | 29.6 | 0.817 |
| Gender | 0.235 | ||
| Male | 231 | 379 | |
| Female | 68 | 90 | |
| Neurosurgery consult (n) | 162 | 291 | |
| % of RTI neurosurgery consult | 54% | 62% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaca, S.D.; Feng, A.Y.; Ku, S.; Jin, M.C.; Kakusa, B.W.; Ho, A.L.; Zhang, M.; Fuller, A.; Haglund, M.M.; Grant, G. Boda Bodas and Road Traffic Injuries in Uganda: An Overview of Traffic Safety Trends from 2009 to 2017. Int. J. Environ. Res. Public Health 2020, 17, 2110. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062110
Vaca SD, Feng AY, Ku S, Jin MC, Kakusa BW, Ho AL, Zhang M, Fuller A, Haglund MM, Grant G. Boda Bodas and Road Traffic Injuries in Uganda: An Overview of Traffic Safety Trends from 2009 to 2017. International Journal of Environmental Research and Public Health. 2020; 17(6):2110. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062110
Chicago/Turabian StyleVaca, Silvia D., Austin Y. Feng, Seul Ku, Michael C. Jin, Bina W. Kakusa, Allen L. Ho, Michael Zhang, Anthony Fuller, Michael M. Haglund, and Gerald Grant. 2020. "Boda Bodas and Road Traffic Injuries in Uganda: An Overview of Traffic Safety Trends from 2009 to 2017" International Journal of Environmental Research and Public Health 17, no. 6: 2110. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062110