Physical Disorders are Associated with Health Risk Behaviors in Chinese Adolescents: A Latent Class Analysis



Abstract
:1. Introduction
2. Methods
2.1. Study Design: Participants and Procedures
2.2. Characteristics of the Sample
2.3. Questionnaire and Measures
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
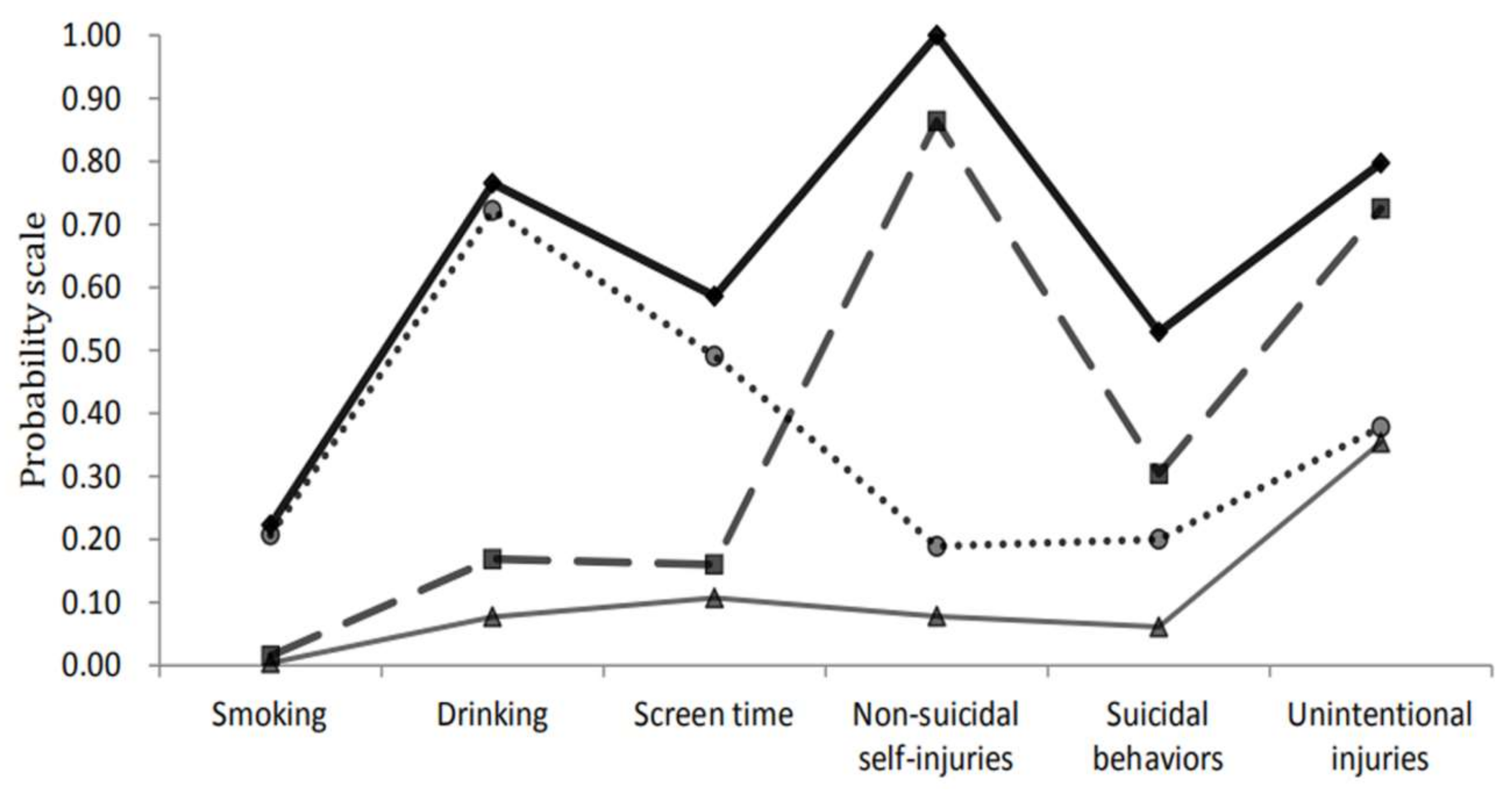
3.2. Latent Class Analysis of HRBs
3.3. Multiple Logistic Regression Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviation
| Abbreviation | Full Name |
| HRBs | Health risk behaviors |
| LCA | Latent class analysis |
| AIC | Akaike information criteria |
| BIC | Bayesian information criteria |
| aBIC | Adjusted Bayesian information criterion |
| LMR | Lo–Mendell–Rubin |
| BLRT | Bootstrapped likelihood ratio test |
| LMR-LRT | Lo–Mendell–Rubin likelihood ratio |
| OR | Odds ratio |
| CI | Confidence interval |
References
- Mokdad, A.H.; Forouzanfar, M.H.; Daoud, F.; Mokdad, A.A.; El Bcheraoui, C.; Moradi-Lakeh, M.; Kyu, H.H.; Barber, R.M.; Wagner, J.; Cercy, K.; et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 2383–2401. [Google Scholar] [CrossRef]
- Ssewanyana, D.; Van Baar, A.; Newton, C.R. A contextually relevant approach to assessing health risk behavior in a rural sub-Saharan Africa setting: The Kilifi health risk behavior questionnaire. BMC Public Health 2018, 18, 774. [Google Scholar] [CrossRef] [PubMed]
- Franke, K.H.; Krumkamp, R.; Mohammed, A.; Sarpong, N.; Owusu-Dabo, E.; Brinkel, J.; Fobil, J.N.; Marinovic, A.B.; Asihene, P.; Boots, M.; et al. A mobile phone based tool to identify symptoms of common childhood diseases in Ghana: Development and evaluation of the integrated clinical algorithm in a cross-sectional study. BMC Med. Inform. Decis. Mak. 2018, 18, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Zouini, B.; Sfendla, A.; Senhaji, M.; Rastam, M.; Kerekes, N. Somatic health and its association with negative psychosocial factors in a sample of Moroccan adolescents. SAGE Open Med. 2019, 7, 2050312119852527. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Wang, F.; Wang, X.; Li, L.; Zhou, X. Inequalities in the health survey using validation question to filter insufficient effort responding: Reducing overestimated effects or creating selection bias? Int. J. Equity Health 2019, 18, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crump, J.A.; Newton, P.N.; Baird, S.J.; Lubell, Y. Febrile Illness in Adolescents and Adults. In Source Major Infectious Diseases, 3rd ed.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2017; Chapter 14; pp. 365–384. [Google Scholar]
- Thipmontree, W.; Suputtamongkol, Y.; Tantibhedhyangkul, W.; Suttinont, C.; Wongswat, E.; Silpasakorn, S. Human leptospirosis trends: northeast Thailand, 2001-2012. Int. J. Environ. Res. Public. Health 2014, 11, 8542–8551. [Google Scholar] [CrossRef] [Green Version]
- Dal Negro, R.W.; Zanasi, A.; Turco, P.; Povero, M. Acute cough in Italian children: parents’ beliefs, approach to treatment, and the family impact. Multidiscip. Respir. Med. 2019, 14, 16. [Google Scholar] [CrossRef] [Green Version]
- Marchello, C.S.; Ebell, M.H.; McKay, B.; Shen, Y.; Harvill, E.T.; Whalen, C.C. Clinical management decisions for adults with prolonged acute cough: Frequency and associated factors. Am. J. Emerg. Med. 2018, 37, 1681–1685. [Google Scholar] [CrossRef]
- Song, W.J.; Chang, Y.S.; Faruqi, S.; Kim, J.Y.; Kang, M.G.; Kim, S.; Jo, E.J.; Kim, M.H.; Plevkova, J.; Park, H.W.; et al. The global epidemiology of chronic cough in adults: A systematic review and meta-analysis. Eur. Respir. J. 2015, 45, 1479–1481. [Google Scholar] [CrossRef] [Green Version]
- Kurteva, G.; Chilingirova, N.; Rizzi, G.; Caccia, T.; Stella, V.; Bernareggi, A. Pharmacokinetic profile and safety of intravenous NEPA, a fixed combination of fosnetupitant and palonosetron, in cancer patients: Prevention of chemotherapy-induced nausea and vomiting associated with highly emetogenic chemotherapy. Eur. J. Pharm. Sci. 2019, 139, 105041. [Google Scholar] [CrossRef] [PubMed]
- Köchling, J.; Geis, B.; Wirth, S.; Hensel, K.O. Grape or grain but never the twain? A randomized controlled multiarm matched-triplet crossover trial of beer and wine. Am. J. Clin. Nutr. 2019, 109, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Harding, A.K.; Stone, D.L.; Cardenas, A.; Lesser, V. Risk behaviors and self-reported illnesses among Pacific Northwest surfers. J. Water Health 2015, 13, 230–242. [Google Scholar] [CrossRef] [Green Version]
- Çolak, Y.; Nordestgaard, B.G.; Laursen, L.C.; Afzal, S.; Lange, P.; Dahl, M. Risk Factors for Chronic Cough Among 14,669 Individuals From the General Population. Chest 2017, 152, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Imai, N.; Kitamura, E. Differences in clinical features of cluster headache between drinkers and nondrinkers in Japan. PLoS ONE 2019, 14, e0224407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merrill, J.E.; Rosen, R.K.; Boyle, H.K.; Carey, K.B. The influence of context in the subjective evaluation of “negative” alcohol-related consequences. Psychol. Addict. Behav. 2018, 32, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Do, Y.K.; Shin, E. Bidirectional relationship between time preference and adolescent smoking and alcohol use: Evidence from longitudinal data. Addict. Behav. 2017, 70, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Baiden, P.; Tadeo, S.K.; Peters, K.E. The association between excessive screen-time behaviors and insufficient sleep among adolescents: Findings from the 2017 youth risk behavior surveillance system. Psychiatry Res. 2019, 281, 112586. [Google Scholar] [CrossRef]
- Koo, H.K.; Jeong, I.; Kim, J.H.; Kim, S.K.; Shin, J.W.; Park, S.Y.; Rhee, C.K.; Choi, E.Y.; Moon, J.Y.; Kim, Y.H.; et al. Development and validation of the cough Assessment Test (COAT). Respirology 2019, 24, 551–557. [Google Scholar] [CrossRef] [Green Version]
- Hagiya, K.; Mizutani, T.; Yasuda, S.; Kawano, S. Nicotine poisoning due to intravenous injection of cigarette soakage. Hum. Exp. Toxicol. 2010, 29, 427–429. [Google Scholar] [CrossRef] [Green Version]
- Svirko, E.; Hawton, K. Self-injurious behavior and eating disorders: The extent and nature of the association. Suicide Life Threat. Behav. 2017, 37, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, C.A.; Kuja-Halkola, R.; Thornton, L.M.; Hübel, C.; Leppä, V.; Bulik, C.M. Prolonged constipation and diarrhea in childhood and disordered eating in adolescence. J. Psychosom. Res. 2019, 126, 109797. [Google Scholar] [CrossRef] [PubMed]
- Crowell, M.D.; Cheskin, L.J.; Musial, F. Prevalence of gastrointestinal symptoms in obese and normal weight binge eaters. Am. J. Gastroenterol. 1994, 89, 387–391. [Google Scholar] [PubMed]
- Carroll, R.; Metcalfe, C.; Gunnell, D. Hospital presenting self-harm and risk of fatal and non-fatal repetition: Systematic review and meta-analysis. PLoS ONE 2014, 9, e89944. [Google Scholar] [CrossRef]
- Zhang, L.; Li, X.; Wu, R.; Chen, H.; Liu, J.; Wang, Z.; Xing, Y.; Ishaq, H.M.; Wang, J.; Yu, P.; et al. A gastroenteritis outbreak associated with drinking water in a college in northwest China. J. Water Health 2018, 16, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Trommel, N.; Hofland, H.W.; Van Komen, R.S.; Dokter, J.; Van Baar, M.E. Nursing problems in patients with toxic epidermal necrolysis and Stevens-Johnson syndrome in a Dutch burn centre: A 30-year retrospective study. Burns 2019, 45, 1625–1633. [Google Scholar] [CrossRef]
- Singh, A.K.; Jena, R.K.; Pal, R.; Munivenkatappa, A.; Reddy, V.U.; Hegde, K.V.; Kumar, S.S.; Agrawal, A. Morbidity Audit of 704 Traumatic Brain Injury Cases in a Dedicated South Indian Trauma Center. Asian J. Neurosurg. 2018, 13, 714–720. [Google Scholar] [CrossRef]
- Driskell, M.M.; Dyment, S.; Mauriello, L.; Castle, P.; Sherman, K. Relationships among multiple behaviors for childhood and adolescent obesity prevention. Prev. Med. 2008, 46, 209–215. [Google Scholar] [CrossRef]
- Lanza, S.T.; Rhoades, B.L. Latent class analysis: An alternative perspective on subgroup analysis in prevention and treatment. Prev. Sci. 2013, 14, 157–168. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Zheng, H. Socioeconomic Status and Morbidity Rate Inequality in China: Based on NHSS and CHARLS Data. Int. J. Environ. Res. Public Health 2019, 16, 215. [Google Scholar] [CrossRef] [Green Version]
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J.; et al. Youth Risk Behavior Surveillance-United States, 2017. MMWR Surveill. Summ. 2018, 67, 1–114. [Google Scholar] [CrossRef]
- Brener, N.D.; Billy, J.O.G.; Grady, W.R. Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: Evidence from the scientific literature. J. Adolesc. Health 2003, 33, 436–457. [Google Scholar] [CrossRef] [Green Version]
- Malta, D.C.; De Andreazzi, M.A.; Oliveira-Campos, M.; Andrade, S.S.; De Sá, N.N.; De Moura, L.; Dias, A.J.; Crespo, C.D.; Da Silva Júnior, J.B. Trend of the risk and protective factors of chronic diseases in adolescents, National Adolescent School-based Health Survey (PeNSE 2009 e 2012). Rev. Bras. Epidemiol. 2014, 17, 77–91. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics; Committee on Public Education. American Academy of Pediatrics: Children, adolescents, and television. Pediatrics 2001, 107, 423–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, Y.H.; Xu, S.J.; Chen, J.; Hu, C.L.; Tao, F.B. Longitudinal effects of psychological symptoms on non-suicidal self-injury: A difference between adolescents and young adults in China. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 237–247. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. Methods for Injury Surveillance among Child and Adolescent; GB/T 31180-2014[S]; National Health Commission of the People’s Republic of China: Beijing, China, 2015. [Google Scholar]
- Jiang, L.; Beals, J.; Zhang, L.; Mitchell, C.M.; Manson, S.M.; Acton, K.J.; Roubideaux, Y. Latent class analysis of stages of change for multiple health behaviors: Results from the Special Diabetes Program for Indians Diabetes Prevention Program. Prev. Sci. 2012, 13, 449–461. [Google Scholar] [CrossRef]
- Carragher, N.; Adamson, G.; Bunting, B.; McCann, S. Subtypes of depression in a nationally representative sample. J. Affect. Disord. 2009, 113, 88–99. [Google Scholar] [CrossRef]
- Yang, R.; Li, D.; Hu, J.; Tian, R.; Wan, Y.; Tao, F.; Fang, J.; Zhang, S.C. Association between Health Literacy and Subgroups of Health Risk Behaviors among Chinese Adolescents in Six Cities: A Study Using Regression Mixture Modeling. Int. J. Environ. Res. Public Health 2019, 16, 3680. [Google Scholar] [CrossRef] [Green Version]
- Saps, M.; Velasco-Benitez, C.A.; Blom, P.J.J.; Benninga, M.A.; Nichols-Vinueza, D.X. Prospective Study of Gastrointestinal Symptoms in School Children of South-America. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 391–394. [Google Scholar] [CrossRef]
- Staff, J.; Maggs, J.L.; Seto, C.; Dillavou, J.; Vuolo, M. Electronic and Combustible Cigarette Use in Adolescence: Links with Adjustment, Delinquency, and Other Substance Use. J. Adolesc. Health 2020, 66, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Zhang, J.; Wang, S.; Xu, W.; Liang, W.; Yan, M.; Wang, D.; Diao, B.; Pang, B.; Lu, X.; et al. Bacterial pathogen spectrum of acute diarrheal outpatients in an urbanized rural district in Southwest China. Int. J. Infect. Dis. 2018, 70, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pappas, D.E.; Hendley, J.O.; Hayden, F.G.; Winther, B. Symptom profile of common colds in school-aged children. Pediatr. Infect. Dis. J. 2008, 27, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Grudzinska, F.S.; Brodlie, M.; Scholefield, B.R.; Jackson, T.; Scott, A.; Thickett, D.R.; Sapey, E. Neutrophils in community-acquired pneumonia: Parallels in dysfunction at the extremes of age. Thorax 2020, 75, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koskela, H.O.; Lätti, A.M.; Pekkanen, J. Risk factors for repetitive doctor’s consultations due to cough: A cross-sectional study in a Finnish employed population. BMJ Open 2019, 9, e030945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weaver, E.R.N.; Agius, P.A.; Veale, H.; Dorning, K.; Hlang, T.T.; Aung, P.P.; Fowkes, F.J.I.; Hellard, M.E. Water, Sanitation, and Hygiene Facilities and Hygiene Practices Associated with Diarrhea and Vomiting in Monastic Schools, Myanmar. Am. J. Trop. Med. Hyg. 2016, 95, 278–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiolero, A.; Wietlisbach, V.; Ruffieux, C.; Paccaud, F.; Cornuz, J. Clustering of risk behaviors with cigarette consumption: A population-based survey. Prev. Med. 2006, 42, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Münzel, T.; Hahad, O.; Daiber, A. Double hazard of smoking and alcohol on vascular function in adolescents. Eur. Heart J. 2018, 40, 354–356. [Google Scholar] [CrossRef] [Green Version]
- Stiglic, N.; Viner, R.M. Effects of screentime on the health and well-being of children and adolescents: A systematic review of reviews. BMJ Open 2019, 9, e023191. [Google Scholar] [CrossRef] [Green Version]
- Leonardi-Bee, J.; Nderi, M.; Britton, J. Smoking in movies and smoking initiation in adolescents: Systematic review and meta-analysis. Addiction 2016, 111, 1750–1763. [Google Scholar] [CrossRef] [Green Version]
- Meader, N.; King, K.; Moe-Byrne, T.; Wright, K.; Graham, H.; Petticrew, M.; Power, C.; White, M.; Sowden, A.J. A systematic review on the clustering and co-occurrence of multiple risk behaviours. BMC Public Health 2016, 16, 657. [Google Scholar] [CrossRef] [Green Version]
- Sorenson, S.B.; Shen, H.; Kraus, J.F. Undetermined manner of death. A comparison with unintentional injury, suicide, and homicide death. Eval. Rev. 1997, 21, 43–57. [Google Scholar] [CrossRef] [PubMed]
- Khalsa, H.M.; Salvatore, P.; Hennen, J.; Baethge, C.; Tohen, M.; Baldessarini, R.J. Suicidal events and accidents in 216 first-episode bipolar I disorder patients: Predictive factors. J. Affect. Disord. 2008, 106, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Uddin, R.; Lee, E.Y.; Khan, S.R.; Tremblay, M.S.; Khan, A. Clustering of lifestyle risk factors for non-communicable diseases in 304,779 adolescents from 89 countries: A global perspective. Prev. Med. 2019, 131, 105955. [Google Scholar] [CrossRef] [PubMed]
- Sagiv, E.; Hadlaczky, G.; Sheetrit, N.; Gur, E.; Horesh, N.; Gvion, Y. The Fear of Losing-Nonsuicidal Self-Injury as a Protective Mechanism in Eating Disorders. Front. Psychiatry 2019, 10, 825. [Google Scholar] [CrossRef]
- Stickley, A.; Koyanagi, A.; Ueda, M.; Inoue, Y.; Waldman, K.; Oh, H. Physical multimorbidity and suicidal behavior in the general population in the United States. J. Affect. Disord. 2020, 260, 604–609. [Google Scholar] [CrossRef]
- Tomori, Z.; Donic, V.; Benacka, R.; Gresova, S.; Peregrim, I.; Kundrik, M.; Pallayova, M.; Jakus, J. Reversal of functional disorders by aspiration, expiration, and cough reflexes and their voluntary counterparts. Front. Physiol. 2012, 3, 467. [Google Scholar] [CrossRef] [Green Version]
- Szpilman, D. Near-drowning and drowning classification: A proposal to stratify mortality based on the analysis of 1831 cases. Chest 1997, 112, 660–665. [Google Scholar] [CrossRef] [Green Version]
- Fan, X.; Cao, Z.B. Physical activity among Chinese school-aged children: National prevalence estimates from the 2016 Physical Activity and Fitness in China-The Youth Study. J. Sport Health Sci. 2017, 6, 388–394. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total (n = 22,628) | Diarrhea | Fever | Cough | Vomiting | ||||
|---|---|---|---|---|---|---|---|---|---|
| n (%) | χ2 | n (%) | χ2 | n (%) | χ2 | n (%) | χ2 | ||
| Grade | 47.132 ** | 86.194 ** | 213.329 ** | 6.858 ** | |||||
| Middle school | 11,993 | 2599 (21.7) | 2168 (18.1) | 6620 (55.2) | 1345 (11.2) | ||||
| High school | 10,635 | 2717 (25.5) | 1441 (13.5) | 4836 (45.5) | 1078 (10.1) | ||||
| Gender | 0.482 | 5.955 * | 15.706 ** | 0.124 | |||||
| Male | 10,990 | 2604 (23.7) | 1820 (16.6) | 5415 (49.3) | 1185 (10.8) | ||||
| Female | 11,638 | 2712 (23.3) | 1789 (15.4) | 6041 (51.9) | 1238 (10.6) | ||||
| Registered residence | 14.299 ** | 0.117 | 0.013 | 0.488 | |||||
| Rural | 10,882 | 2267 (24.6) | 1745 (16.0) | 5505 (50.6) | 1149 (10.6) | ||||
| Urban | 11,746 | 2639 (22.5) | 1864 (15.9) | 5951 (50.7) | 1274 (10.8) | ||||
| Any siblings | 0.935 | 1.401 | 22.861 ** | 0.668 | |||||
| Yes | 9720 | 2253 (23.2) | 1518 (15.6) | 5099 (52.5) | 1022 (10.5) | ||||
| No | 12,908 | 3063 (23.7) | 2091 (16.2) | 6357 (49.2) | 1401 (10.9) | ||||
| Boarding on school days | 41.975 ** | 16.089 ** | 2.221 | 14.691 ** | |||||
| Yes | 11,320 | 2866 (25.3) | 1695 (15.0) | 5675 (50.1) | 1123 (9.9) | ||||
| No | 11,308 | 2450 (21.7) | 1914 (16.9) | 5781 (51.1) | 1300 (11.5) | ||||
| Father’s educational level a | 2.439 | 1.580 | 1.163 | 0.012 | |||||
| <High school degree | 13,006 | 3096 (23.8) | 2028 (15.6) | 6542 (50.3) | 1381 (10.6) | ||||
| ≥High school degree | 9424 | 2159 (22.9) | 1528 (16.2) | 4809 (51.0) | 1005 (10.7) | ||||
| Mother’s educational level b | 1.410 | 4.432 * | 0.480 | 0.558 | |||||
| <High school degree | 14,335 | 3397 (23.7) | 2222 (15.5) | 7232 (50.4) | 1507 (10.5) | ||||
| ≥High school degree | 8105 | 1864 (23.0) | 1343 (16.6) | 4128 (50.9) | 878 (10.8) | ||||
| Self-reported family economy | 28.549 ** | 18.598 ** | 0.286 | 12.501 ** | |||||
| Bad | 3240 | 880 (27.2) | 549 (16.9) | 1628 (50.2) | 380 (11.7) | ||||
| General | 16,345 | 3729 (22.8) | 2506 (15.3) | 8292 (50.7) | 1677 (10.3) | ||||
| Good | 3043 | 707 (23.2) | 554 (18.2) | 1536 (50.5) | 366 (12.0) | ||||
| Number of friends | 19.061 ** | 19.312 ** | 5.738 | 25.362 ** | |||||
| ≤ 2 | 5514 | 1398 (25.4) | 947 (17.2) | 2842 (51.5) | 691 (12.5) | ||||
| 3–5 | 9620 | 2264 (23.5) | 1417 (14.7) | 4901 (50.9) | 974 (10.1) | ||||
| ≥ 6 | 7494 | 1654 (22.1) | 1245 (16.6) | 3713 (49.5) | 758 (10.1) | ||||
| Statistic | 2 Classes | 3 Classes | 4 Classes | 5 Classes |
|---|---|---|---|---|
| AIC | 120,896.912 | 119,991.261 | 119,844.588 | 119,822.264 |
| BIC | 121,001.263 | 120,151.800 | 120,061.315 | 120,095.180 |
| aBIC | 120,959.949 | 120,088.241 | 119,975.510 | 119,987.129 |
| LMR-LRT | <0.001 | <0.001 | <0.001 | 0.0592 |
| BLRT | <0.001 | <0.001 | <0.001 | <0.001 |
| Entropy | 0.549 | 0.725 | 0.692 | 0.579 |
| Health Risk Behaviors (n) | Diarrhea | Fever | Cough | Vomiting | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | Crude OR (95% CI) | Adjusted OR (95% CI)a | n (%) | Crude OR (95% CI) | Adjusted OR (95% CI)a | n (%) | Crude OR (95% CI) | Adjusted OR (95% CI)a | n (%) | Crude OR (95% CI) | Adjusted OR (95% CI)a | |
| Low-risk class (14502) | 2891 (19.9) | Ref. | Ref. | 1954 (13.5) | Ref. | Ref. | 6585 (45.4) | Ref. | Ref. | 1185 (8.2) | Ref. | Ref. |
| Moderate-risk class 1 (1012) | 299 (29.5) | 1.684 (1.463–1.939) *** | 1.682 (1.460–1.938) *** | 229 (22.6) | 1.878 (1.609–2.192) *** | 1.870 (1.595–2.192) *** | 523 (51.7) | 1.286 (1.132–1.461) *** | 1.379 (1.212–1.569) *** | 205 (20.3) | 2.855 (2.422–3.365) *** | 2.884 (2.445–3.401) *** |
| Moderate-risk class 2 (6511) | 1890 (29.0) | 1.643 (1.536–1.757) *** | 1.643 (1.535–1.758) *** | 1222 (18.8) | 1.484 (1.372–1.605) *** | 1.447 (1.337–1.567) *** | 3964 (60.9) | 1.871 (1.763–1.986) *** | 1.871 (1.762–1.987) *** | 880 (13.5) | 1.756 (1.601–1.927) *** | 1.748 (1.592–1.918) *** |
| High-risk class (603) | 236 (39.1) | 2.583 (2.182–3.057) *** | 2.655 (2.242–3.144) *** | 204 (33.8) | 3.283 (2.755–3.912) *** | 3.135 (2.619–3.754) *** | 384 (63.7) | 2.108 (1.780–2.497) *** | 2.158 (1.819–2.560) *** | 153 (25.4) | 3.821 (3.151–4.633) *** | 3.776 (3.113–4.581) *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, B.; Hu, W.; Hu, W.; Yang, R.; Li, D.; Guo, C.; Xia, Z.; Hu, J.; Tao, F.; Fang, J.; et al. Physical Disorders are Associated with Health Risk Behaviors in Chinese Adolescents: A Latent Class Analysis. Int. J. Environ. Res. Public Health 2020, 17, 2139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062139
Song B, Hu W, Hu W, Yang R, Li D, Guo C, Xia Z, Hu J, Tao F, Fang J, et al. Physical Disorders are Associated with Health Risk Behaviors in Chinese Adolescents: A Latent Class Analysis. International Journal of Environmental Research and Public Health. 2020; 17(6):2139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062139
Chicago/Turabian StyleSong, Bingdong, Weirong Hu, Wanxia Hu, Rong Yang, Danlin Li, Chunyu Guo, Zhengmei Xia, Jie Hu, Fangbiao Tao, Jun Fang, and et al. 2020. "Physical Disorders are Associated with Health Risk Behaviors in Chinese Adolescents: A Latent Class Analysis" International Journal of Environmental Research and Public Health 17, no. 6: 2139. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062139