Total Worker Health Leadership and Business Strategies Are Related to Safety and Health Climates in Small Business

 , ,
, ,
Abstract
:1. Introduction
1.1. Safety and Health Climates
1.2. Predictors of Safety and Health Climates
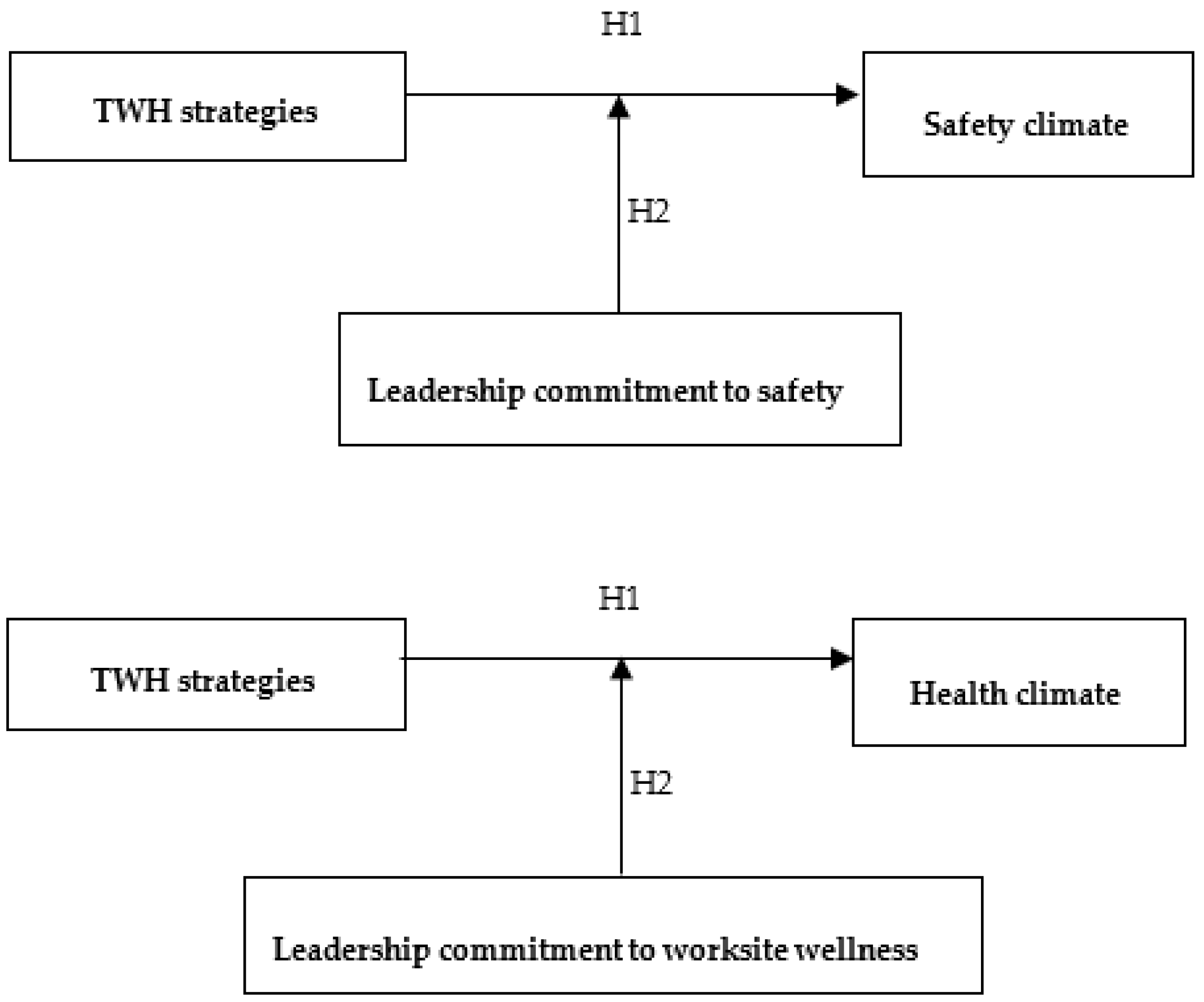
1.2.1. TWH Strategies
1.2.2. Moderating Effects of Leadership Commitment
1.3. Study Purpose
2. Materials and Methods
2.1. Participants
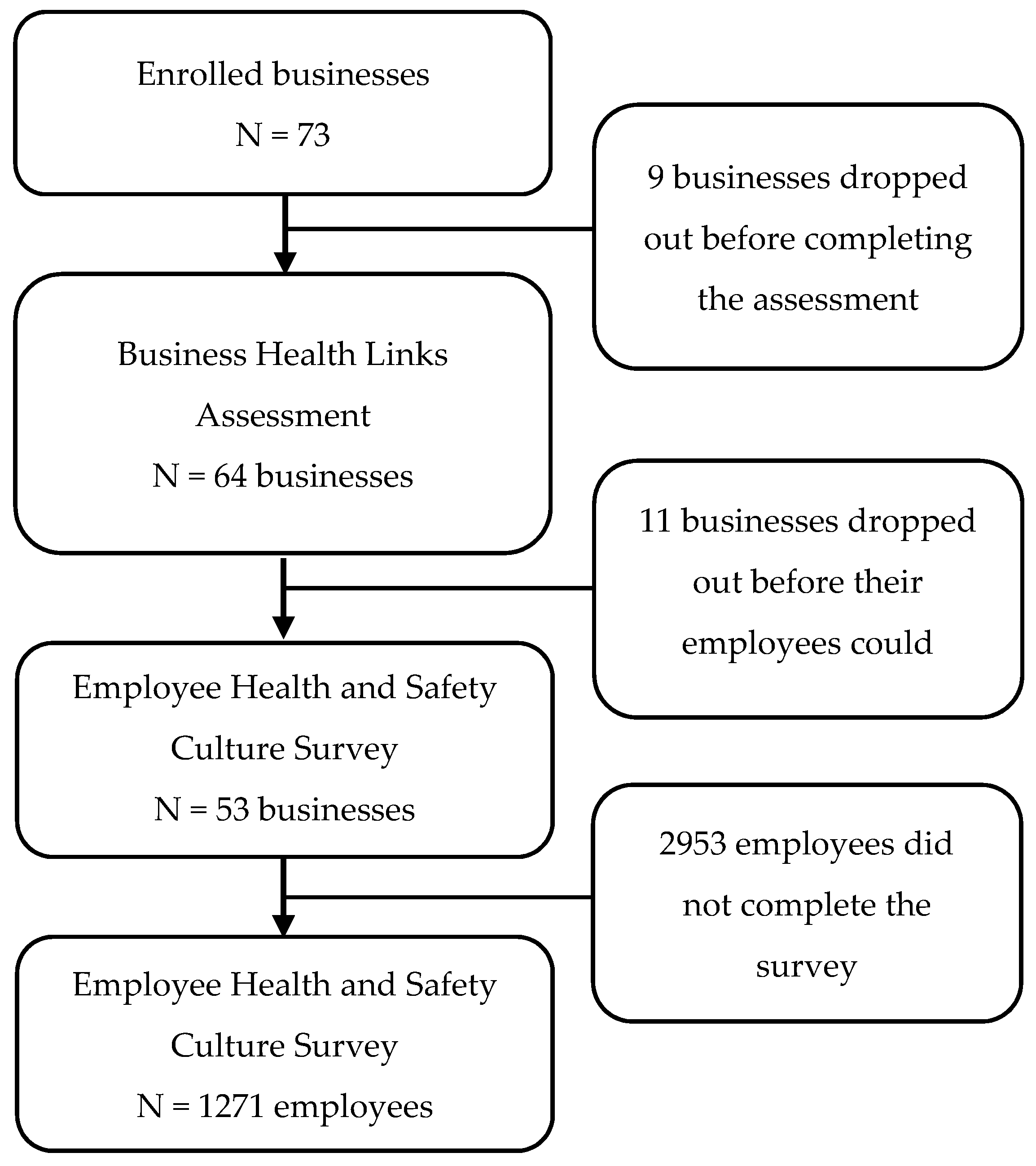
2.1.1. Businesses
2.1.2. Employees
2.2. Data Collection and Measures
2.2.1. TWH Strategies
2.2.2. Safety and Health Climates
2.2.3. Leadership Commitment
2.3. Analysis
3. Results
3.1. Sample
3.2. Confirmatory Factor Analysis
3.3. Bi-Variable Analyses
3.4. Regression Analyses–Safety Climate
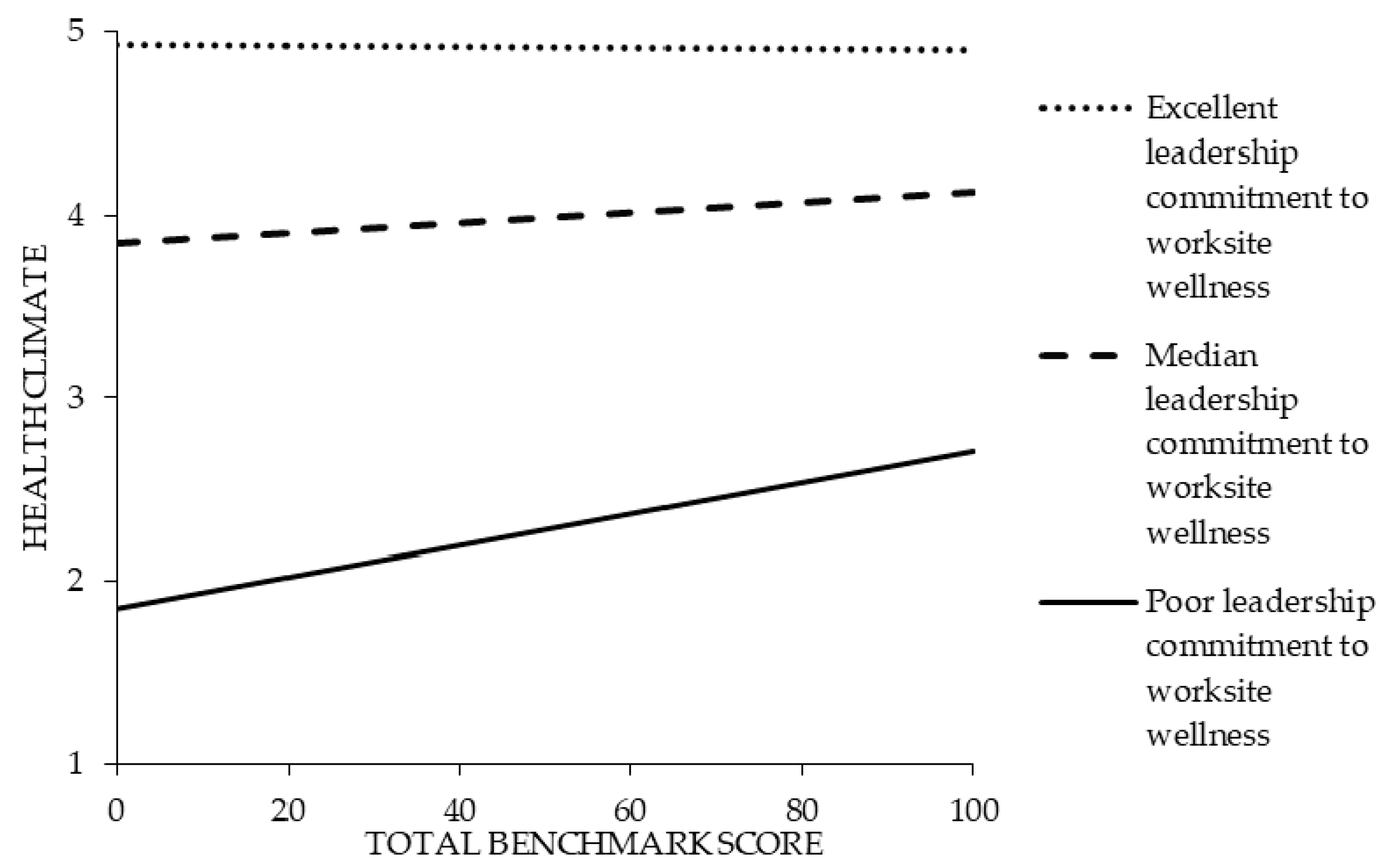
3.5. Regression Analyses–Health Climate
4. Discussion
4.1. Future Research
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- NIOSH. What is Total Worker Health? Available online: https://www.cdc.gov/niosh/twh/default.html (accessed on 19 October 2019).
- United States Census Bureau. 2016 SUSB Annual Data Tables by Establishment Industry. Available online: https://www.census.gov/data/tables/2016/econ/susb/2016-susb-annual.html (accessed on 17 January 2020).
- Schwatka, N.; Atherly, A.; Dally, M.J.; Fang, H.; Brockbank, C.V.; Tenney, L.; Goetzel, R.Z.; Jinnett, K.; Witter, R.; Reynolds, S.; et al. Health risk factors as predictors of workers’ compensation claim occurrence and cost. Occup. Environ. Med. 2017, 74, 14–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenney, L.; Newman, L. Total worker health approaches in small to medium-sized enterprises. In Total Worker Health; Hudson, H., Nigam, J., Sauter, S., Chosewood, L., Schill, A., Howard, J., Eds.; American Psychological Association: Washington, DC, USA, 2019. [Google Scholar]
- Tenney, L.; Fan, W.; Dally, M.; Scott, J.; Haan, M.; Rivera, K.; Newman, M.; Newman, L. Health LinksTM assessment of Total Worker Health practices as indicators of organizational behavior in small business. J. Occup. Environ. Med. 2019, 61, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, T.; Sinclair, R.; Schulte, P.A. Better understanding the small business construct to advance research on delivering workplace health and safety. Small Enterp. Res. 2014, 21, 148–160. [Google Scholar] [CrossRef]
- Schneider, B. Organizational climates: An essay. Pers. Psychol. 1975, 28, 447–479. [Google Scholar] [CrossRef]
- Zohar, D. Safety climate: Conceptual and measurement issues. In Handbook of Occupational Health Psychology, 2nd ed.; Quick, J.C., Tetrick, L.E., Eds.; American Psychological Association: Washington, DC, USA, 2011. [Google Scholar]
- Schneider, B.; Gonzalez-Roma, V.; Ostroff, C.; West, M. Organizational climate and culture: Reflections on the history of the constructs in the Journal of Applied Psychology. J. Appl. Psychol. 2017, 102, 468–482. [Google Scholar] [CrossRef] [Green Version]
- Tamers, S.; Goetzel, R.; Kelly, K.; Luckhaupt, S.; Nigam, J.; Pronk, N.; Rohlman, D.; Baron, S.; Brosseau, L.; Bushnell, T.; et al. Research Methodologies for Total Worker Health®. J. Occup. Environ. Med. 2018, 60, 968–978. [Google Scholar] [CrossRef]
- Schwatka, N.; Tenney, L.; Dally, M.; Scott, J.; Brown, C.; Weitzenkamp, D.; Shore, E.; Newman, L. Small business Total Worker Health: A conceptual and methodological approach to facilitating organizational change. Occup. Health Sci. 2018, 2, 25–41. [Google Scholar] [CrossRef]
- Zohar, D. Safety climate in industrial organizations: Theoretical and applied implications. J. Appl. Psychol. 1980, 65, 96–102. [Google Scholar] [CrossRef]
- Christian, M.S.; Bradley, J.C.; Wallace, J.C.; Burke, M.J. Workplace safety: A meta-analysis of the roles of person and situation factors. J. Appl. Psychol. 2009, 94, 1103–1127. [Google Scholar] [CrossRef]
- Nahrgang, J.D.; Morgeson, F.P.; Hofmann, D.A. Safety at work: A meta-analytic investigation of the link between job demands, job resources, burnout, engagement, and safety outcomes. J. Appl. Psychol. 2011, 96, 71–94. [Google Scholar] [CrossRef]
- Clarke, S. The relationship between safety climate and safety performance: A meta-analytic review. J. Occup. Health Psychol. 2006, 11, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Beus, J.; Payne, S.; Bergman, E.; Arthur, W. Safety Climate and Injuries: An Examination of Theoretical and Empirical Relationships. J. Appl. Psychol. 2010, 95, 713–727. [Google Scholar] [CrossRef] [PubMed]
- Sawhney, G.; Sinclair, R.R.; Cox, A.R.; Munc, A.H.; Sliter, M.T. One Climate or Many: Examining the Structural Distinctiveness of Safety, Health, and Stress Prevention Climate Measures. J. Occup Environ. Med. 2018, 60, 1015–1025. [Google Scholar] [CrossRef]
- Zweber, Z.M.; Henning, R.A.; Magley, V.J. A practical scale for Multi-Faceted Organizational Health Climate Assessment. J. Occup. Health Psychol. 2016, 21, 250–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basen-Engquist, K.; Hudmon, K.S.; Tripp, M.; Chamberlain, R. Worksite Health and Safety Climate: Scale Development and Effects of a Health Promotion Intervention. Prev. Med. 1998, 27, 111–119. [Google Scholar] [CrossRef]
- Ribisl, K.M.; Reischl, T.M. Measuring the climate for health at organizations. Development of the worksite health climate scales. J. Occup. Med. 1993, 35, 812–824. [Google Scholar] [CrossRef] [PubMed]
- Zohar, D. Thirty years of safety climate research: Reflections and future directions. Accid. Anal. Prev. 2010, 42, 1517–1522. [Google Scholar] [CrossRef]
- Kuenzi, M.; Schminke, M. Assembling Fragments Into a Lens: A Review, Critique, and Proposed Research Agenda for the Organizational Work Climate Literature. J. Manag. 2009, 35, 634–717. [Google Scholar] [CrossRef]
- DeJoy, D.; Schaffer, B.; Wilson, M.; Vandenberg, R.; Butts, M. Creating safer workplaces: Assessing the determinants and role of safety climate. J. Saf. Res. 2004, 35, 81–90. [Google Scholar] [CrossRef]
- Lee, J.; Huang, Y.H.; Cheung, J.H.; Chen, Z.; Shaw, W.S. A systematic review of the safety climate intervention literature: Past trends and future directions. J. Occup. Health Psychol. 2019, 24, 66. [Google Scholar] [CrossRef]
- Clarke, S. Safety leadership: A meta-analytic review of transformational and transactional leadership styles as antecedents of safety behaviours. J. Occup. Organ. Psychol. 2013, 86, 22–49. [Google Scholar] [CrossRef]
- Kelloway, E.; Mullen, J.; Francis, L. Divergent effects of transformational and passive leadership on employee safety. J. Occup. Health Psychol. 2006, 11, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Mullen, J.; Kelloway, K.; Teed, M. Inconsistent style of leadership as a predictor of safety behavior. Work Stress 2011, 25, 41–54. [Google Scholar] [CrossRef]
- Mullen, J.; Kelloway, E. Safety leadership: A longitudinal study of the effects of transformational leadership on safety outcomes. J. Occup. Organ. Psychol. 2009, 82, 253–272. [Google Scholar] [CrossRef]
- von Thiele Schwarz, U.; Hasson, H.; Tafvelin, S. Leadership training as an occupational health intervention: Improved safety and sustained productivity. Saf. Sci. 2016, 81, 35–45. [Google Scholar] [CrossRef]
- Bronkhorst, B.; Tummers, L.; Steijn, B. Improving safety climate and behavior through a multifaceted intervention: Results from a field experiment. Saf. Sci. 2018, 103, 293–304. [Google Scholar] [CrossRef] [Green Version]
- Schwatka, N.; Tenney, L.; Newman, L. Health Protection and Health Promotion in Small Business. In Increasing Occupational Health and Safety in Workplaces: Research and Practice; Richardsen, A., Burke, R., Eds.; Edward Elgar Publishing: Cheltenham, UK, 2019. [Google Scholar]
- Lee, J.; Huang, Y.-H.; Robertson, M.M.; Murphy, L.A.; Garabet, A.; Chang, W.-R. External validity of a generic safety climate scale for lone workers across different industries and companies. Accid. Anal. Prev. 2014, 63, 138–145. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; The Guildford Press: New York, NY, USA, 2006. [Google Scholar]
- Hu, L.; Bentler, P. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Murphy, L.; Robertson, M.; Carayon, P. The next generation of macroergonomics: Integrating safety climate. Accid. Anal. Prev. 2014, 68, 16–24. [Google Scholar] [CrossRef]
- Anger, W.K.; Elliot, D.L.; Bodner, T.; Olson, R.; Rholman, D.S.; Truxillo, D.M.; Kuehl, K.S.; Hammer, L.B.; Montgomery, D. Effectiveness of Total Worker Health Interventions. J. Occup. Health Psychol. 2015, 20, 226–247. [Google Scholar] [CrossRef] [Green Version]
- Kuoppala, J.; Lamminp, A.; Liira, J.; Vainio, H. Leadership, job well-being, and health effects—A systematic review and a meta-analysis. J Occup Environ. Med 2008, 50, 904–915. [Google Scholar] [CrossRef] [PubMed]
- Akerjordet, K.; Furunes, T.; Haver, A. Health-promoting leadership: An integrative review and future research agenda. J. Adv. Nurs. 2018, 74, 1505–1516. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.; Axelsson, R.; Bihari Axelsson, S. Health promoting leadership—Different views of the concept. Work A J. Prev. Assess. Rehabil. 2011, 40, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, P.; Winkler, B.; Dunkl, A. Creating a healthy working environment with leadership: The concept of health-promoting leadership. Int. J. Hum. Resour. Manag. 2016, 28, 2430–2448. [Google Scholar] [CrossRef]
- Hoert, J.; Herd, A.M.; Hambrick, M. The Role of Leadership Support for Health Promotion in Employee Wellness Program Participation, Perceived Job Stress, and Health Behaviors. Am. J. Health Promot. 2018, 32, 1054–1061. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.; Schwatka, N.; Tenney, L.; Newman, L. Total Worker Health: A Small Business Leader Perspective. Int. J. Environ. Res. Public Health 2018, 15, 2416. [Google Scholar] [CrossRef] [Green Version]
- Spector, P.E. Method variance in organizational research—Truth or urban legend? Organ. Res. Methods 2006, 9, 221–232. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristic | N | % | Mean | SD |
|---|---|---|---|---|
| Age | 41.3 | 13.1 | ||
| Gender | ||||
| Male | 419 | 33.1 | ||
| Female | 842 | 66.6 | ||
| Other | 4 | 0.3 | ||
| Race | ||||
| White | 1184 | 80.23 | ||
| Black or African American | 34 | 2.3 | ||
| Asian | 30 | 2.0 | ||
| Native American or Alaskan Native | 21 | 1.4 | ||
| Native Hawaiian or Other Pacific Islander | 7 | 0.5 | ||
| Ethnicity | ||||
| Hispanic or Latino or Spanish Origin | 123 | 9.78 | ||
| Not Hispanic or Latino or Spanish Origin | 1135 | 90.2 | ||
| Education | ||||
| Did not complete high school | 8 | 0.7 | ||
| High school diploma or GED | 110 | 9.9 | ||
| Some college or 2-year degree | 288 | 25.8 | ||
| 4-year college degree | 462 | 41.4 | ||
| Graduate or professional degree | 247 | 22.2 | ||
| Job Level | ||||
| Supervisor | 500 | 39.4 | ||
| Non-supervisor | 768 | 60.6 | ||
| Job Tenure (years) | 5.3 | 6.7 | ||
| Household income | ||||
| <$50,000 | 396 | 36.0 | ||
| $50,001–$100,000 | 351 | 31.9 | ||
| >$100,000 | 353 | 32.1 | ||
| Type of Work | ||||
| Full-time | 1090 | 86.4 | ||
| Part-time | 171 | 13.6 | ||
| Work hours per week | 39.4 | 12.4 | ||
| Salaried employment | 661 | 52.4 | ||
| Hourly employment | 600 | 47.6 | ||
| Contractor or consultant | 48 | 3.8 | ||
| Shift work | 181 | 14.4 |
| Model | χ2 | Df | χ2 diff | Df diff | CFI | SRMR | RMSEA (90% CI) |
|---|---|---|---|---|---|---|---|
| Hypothesized 4 Factors | 1057 | 164 | - | - | 0.95 | 0.03 | 0.07 (0.07–0.08) |
| Alternative 1 Factor | 5140 | 170 | 4083 | 6 * | 0.73 | 0.09 | 0.17 (0.16–0.17) |
| Alternative 2 Factors | 4105 | 169 | 3048 | 5 * | 0.79 | 0.09 | 0.15 (0.15–0.15) |
| Variable | Mean | SD | Safety Climate | Health Climate | Leadership Commitment to Safety | Leadership Commitment to Worksite Wellness | Total Benchmark Score |
|---|---|---|---|---|---|---|---|
| Climate | |||||||
| Safety climate | 3.83 | 0.79 | (0.92) | 0.63 * | 0.77 * | 0.56 * | 0.16 * |
| Health climate | 3.88 | 0.82 | (0.86) | 0.61 * | 0.76 * | 0.16 * | |
| Leadership commitment | |||||||
| Leadership commitment to safety | 3.68 | 0.84 | (0.90) | 0.69 * | 0.10 * | ||
| Leadership commitment to worksite wellness | 3.49 | 0.91 | (0.94) | 0.11 * | |||
| TWH strategy | |||||||
| Total benchmark score | 48.07 | 18.96 | - |
| Variable | Model 1 | Model 2 | ||
|---|---|---|---|---|
| Estimate | 95% CI | Estimate | 95% CI | |
| Safety climate (DV) | ||||
| Total benchmark score | 0.01 * | (0.00, 0.01) | 0.00 | (−0.01, 0.01) |
| Leadership commitment to safety | 0.66 *** | (0.56, 0.76) | ||
| Total benchmark score * Leadership commitment to safety | 0.00 | (−0.00, 0.00) | ||
| Health climate (DV) | ||||
| Total benchmark score | 0.01 ** | (0.00, 0.02) | 0.01 ** | (0.00, 0.02) |
| Leadership commitment to worksite wellness | 0.77 *** | (0.67, 0.86) | ||
| Total benchmark score * Leadership commitment to worksite wellness | −0.002 * | (−0.004, −0.000) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwatka, N.V.; Dally, M.; Tenney, L.; Shore, E.; Brown, C.E.; Newman, L.S. Total Worker Health Leadership and Business Strategies Are Related to Safety and Health Climates in Small Business. Int. J. Environ. Res. Public Health 2020, 17, 2142. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062142
Schwatka NV, Dally M, Tenney L, Shore E, Brown CE, Newman LS. Total Worker Health Leadership and Business Strategies Are Related to Safety and Health Climates in Small Business. International Journal of Environmental Research and Public Health. 2020; 17(6):2142. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062142
Chicago/Turabian StyleSchwatka, Natalie V., Miranda Dally, Liliana Tenney, Erin Shore, Carol E. Brown, and Lee S. Newman. 2020. "Total Worker Health Leadership and Business Strategies Are Related to Safety and Health Climates in Small Business" International Journal of Environmental Research and Public Health 17, no. 6: 2142. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062142