A Lean Quality Improvement Initiative to Enhance Tobacco Use Treatment in a Cancer Hospital

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
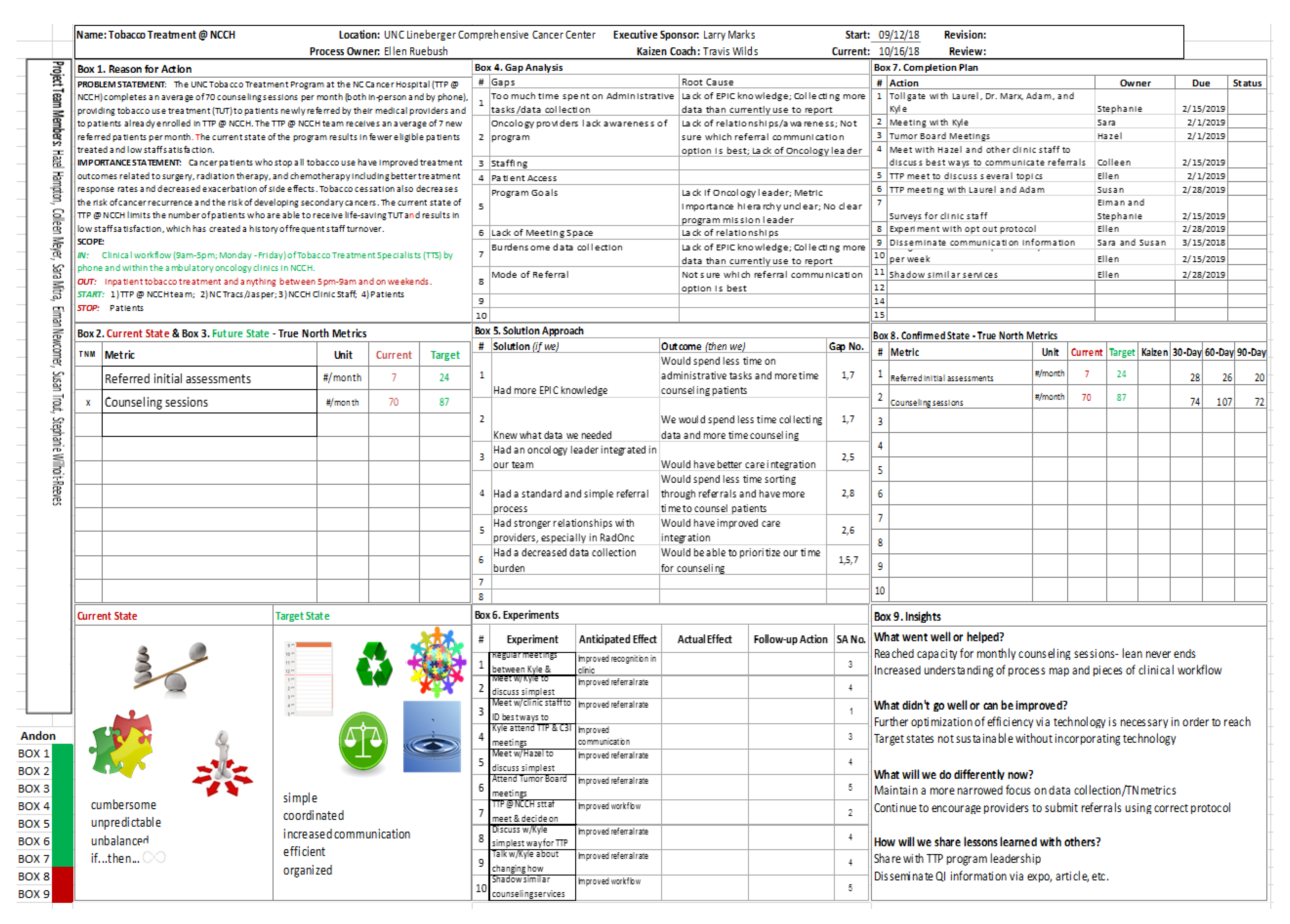
2.2. Application of the Lean QI Tools
2.3. Lean Experiments
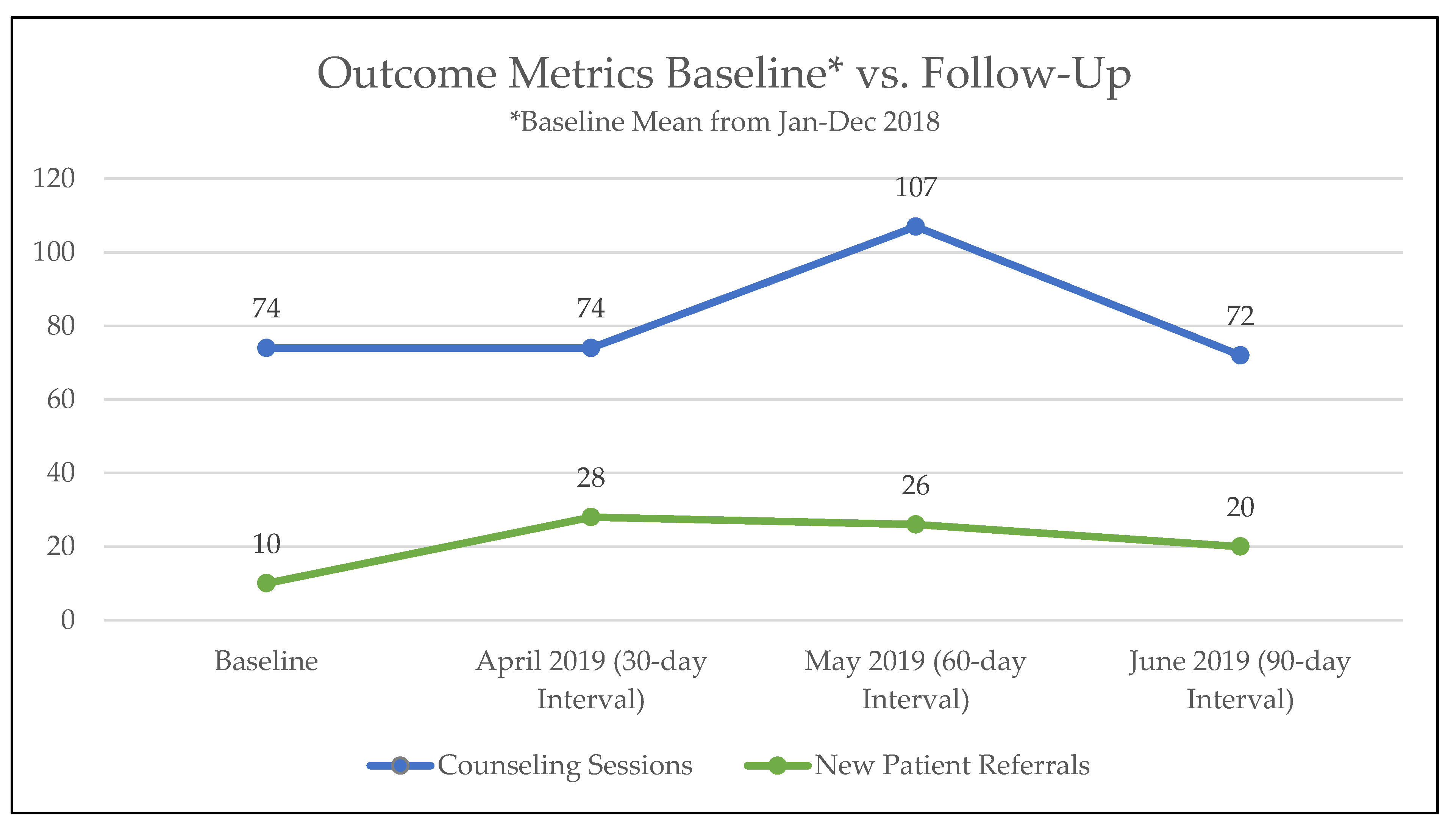
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Balogh, E.P.; Dresler, C.; Fleury, M.E.; Gritz, E.R.; Kean, T.J.; Myers, M.L.; Nass, S.J.; Nevidjon, B.; Toll, B.A.; Warren, G.W.; et al. Reducing Tobacco-Related Cancer Incidence and Mortality: Summary of an Institute of Medicine Workshop. Oncologist 2014, 19, 21–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gritz, E.R.; Toll, B.A.; Warren, G.W. Tobacco Use in the Oncology Setting: Advancing Clinical Practice and Research. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, P.G.; Herbst, R.S.; Arenberg, D.; Benowitz, N.L.; Bierut, L.; Luckart, J.B.; Scavone, J. Smoking Cessation, Version 1.2016, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2016, 14, 1430–1468. [Google Scholar] [CrossRef] [PubMed]
- Croyle, R.T.; Morgan, G.D.; Fiore, M.C. Addressing a Core Gap in Cancer Care—The NCI Moonshot Program to Help Oncology Patients Stop Smoking. N. Engl. J. Med. 2019, 380, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.W.; Dibaj, S.; Hutson, A.; Cummings, K.M.; Dresler, C.; Marshall, J.R. Identifying Targeted Strategies to Improve Smoking Cessation Support for Cancer Patients. J. Thorac. Oncol. 2015, 10, 1532–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trout, S.; Dirkes, J.; Silver, S.; Ripley-Moffitt, C.; Goldstein, A.O.; Davis, J. Incorporating tobacco treatment programs within cancer centers. In Proceedings of the 2017 National Conference on Tobacco or Health, Austin, TX, USA, 22–24 March 2017. [Google Scholar]
- Thompson, D.N.; Wolf, G.A.; Spear, S.J. Driving Improvement in Patient Care: Lessons from Toyota. J. Nurs. Adm. 2003, 33, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Sisler, L.; Omofoye, O.; Paci, K.; Hadar, E.; Goldstein, A.O.; Ripley-Moffitt, C. Using Lean Quality Improvement Tools to Increase Delivery of Evidence-Based Tobacco Use Treatment in Hospitalized Neurosurgical Patients. JCJQPS 2017, 43, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Niaura, R. Nonpharmacologic Therapy for Smoking Cessation: Characteristics and Efficacy of Current Approaches. Am. J. Med. 2008, 121 (Suppl. 1), S11–S19. [Google Scholar] [CrossRef] [PubMed]
- Regan, S.; Reyen, M.; Lockhart, A.C.; Richards, A.E.; Rigotti, N.A. An Interactive Voice Response System to Continue a Hospital-Based Smoking Cessation Intervention after Discharge. Nicotine Tob. Res. 2011, 13, 255–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, M.H.; Kirchhoff, A.C.; Schlotthauer, A.E.; Graber, J.E.; Brown, S.E.S.; Rimington, A.; Drum, M.L.; Schaefer, C.T.; Heuer, L.J.; Huang, E.S.; et al. Sustaining Quality Improvement in Community Health Centers: Perceptions of Leaders and Staff. J. Ambul. Care Manage 2008, 31, 319–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindholm, C.; Adsit, R.; Bain, P.; Reber, P.M.; Brein, T.; Redmond, L.; Smith, S.S.; Fiore, M.C. A Demonstration Project for Using the Electronic Health Record to Identify and Treat Tobacco Users. WMJ 2010, 109, 335–340. [Google Scholar] [PubMed]
- Adsit, R.T.; Fox, B.M.; Tsiolis, T.; Ogland, C.; Simerson, M.; Vind, L.M.; Bell, S.M.; Skora, A.D.; Baker, T.B.; Fiore, M.C. Using the Electronic Health Record to Connect Primary Care Patients to Evidence-Based Telephonic Tobacco Quitline Services: A Closed-Loop Demonstration Project. Transl. Behav. Med. 2014, 4, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, L.; Sharee, K.; Boreta, L.; Silveira, W.R.; Braunstein, S.; Fogh, S. Quality Improvement Initiative to Improve Tobacco Cessation Efforts in Radiation Oncology. J. Oncol. Pract. 2019, 15, e382–e388. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.O.; Ripley-Moffitt, C.E.; Pathman, D.E.; Patsakham, K.M. Tobacco use treatment at the U.S. National Cancer Institute's designated Cancer Centers. Nicotine Tob. Res 2013, 15, 52–58. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Gap | Experiment | Rationale for Experiment | Outcome Metric Impacted | Project Goal |
|---|---|---|---|---|
| Oncology providers lack awareness of TTP | (1) TTS will attend oncology tumor board meetings to present about the program and services | Oncology providers will have improved awareness of the program | New patient referrals | Increased patient care |
| Oncology providers are unfamiliar with how to refer new patients to TTP | (2) TTS will attend oncology tumor board meetings to provide education on how to refer new patients via the Electronic Health Record | New patients will be referred using one standard protocol, which will allow TTS more time to counsel patients each month | New patient referrals & counseling sessions | Increased patient care and improved workflow efficiency |
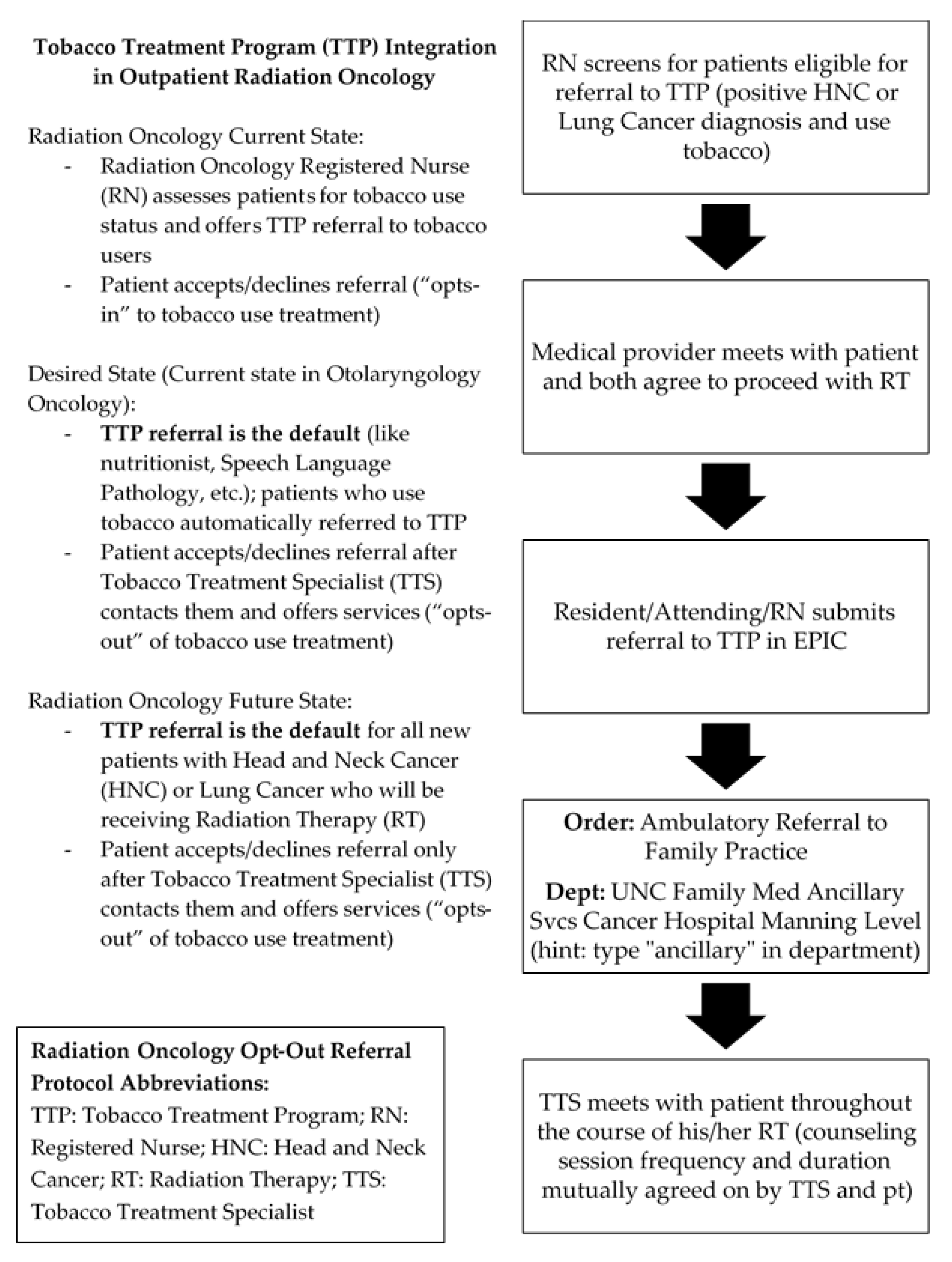
| Low referral rate from Radiation Oncology department | (3) Radiation Oncology department will implement an opt-out protocol based on ENT department model | Implementing an opt-out protocol will increase the number of new patients referred for TUT | New patient referrals | Increased patient care |
| Too much time spent by TTS collecting burdensome data | (4) TTS will meet with program leadership to agree on a reduced data collection burden | Less time spent by TTS collecting, recording, and analyzing data will allow for more time to counsel patients each month | Counseling sessions | Improved workflow efficiency |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, C.; Mitra, S.; Ruebush, E.; Sisler, L.; Wang, K.; Goldstein, A.O. A Lean Quality Improvement Initiative to Enhance Tobacco Use Treatment in a Cancer Hospital. Int. J. Environ. Res. Public Health 2020, 17, 2165. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062165
Meyer C, Mitra S, Ruebush E, Sisler L, Wang K, Goldstein AO. A Lean Quality Improvement Initiative to Enhance Tobacco Use Treatment in a Cancer Hospital. International Journal of Environmental Research and Public Health. 2020; 17(6):2165. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062165
Chicago/Turabian StyleMeyer, Colleen, Sara Mitra, Ellen Ruebush, Laurel Sisler, Kyle Wang, and Adam O. Goldstein. 2020. "A Lean Quality Improvement Initiative to Enhance Tobacco Use Treatment in a Cancer Hospital" International Journal of Environmental Research and Public Health 17, no. 6: 2165. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17062165