Development and Validation of the Overall Foot Pain Questionnaire in Motorcycle Riders

 ,
,  , ,
, , 
 and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Ethical Approval
2.2. Study Design
2.3. Participants
2.4. Outcome Measurements and Procedure
2.5. Translation Method
- (a)
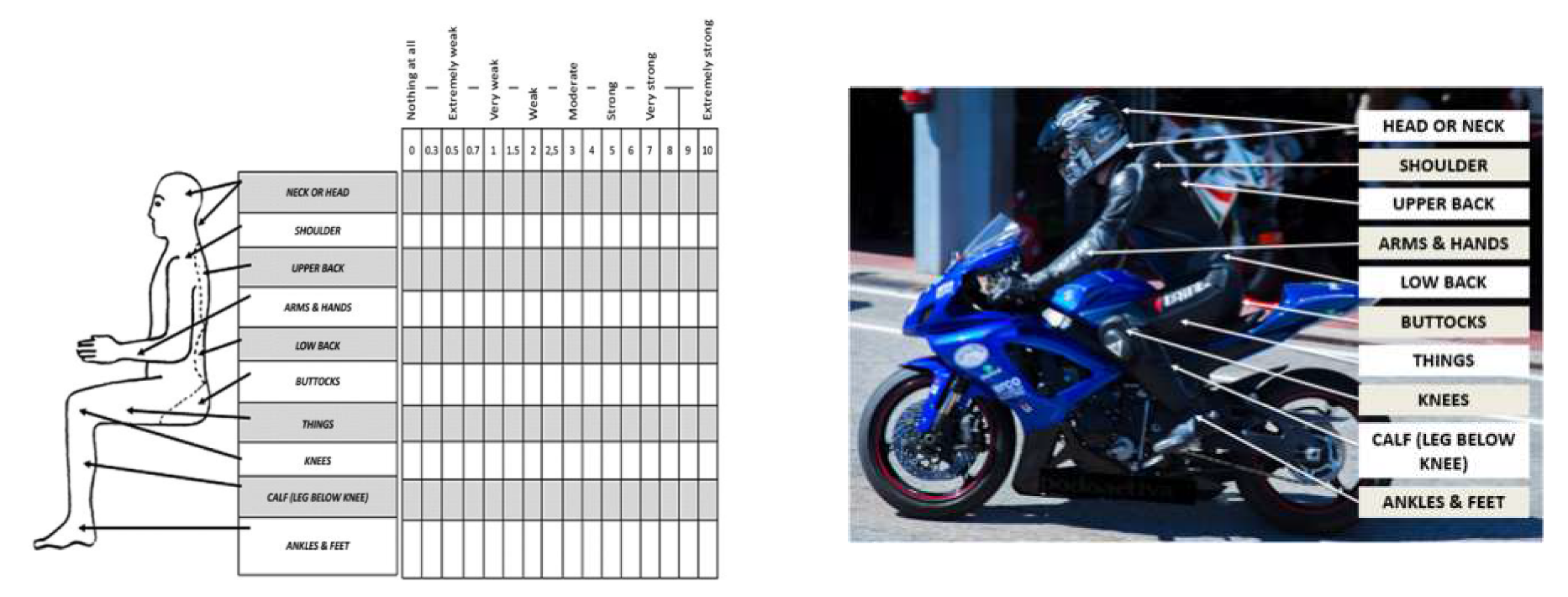
- Request to the author, Borg. G. of the original questionnaire to translate the original questionnaire Borg CR10 Scale® and Scales with instructions, which may be obtained from [email protected], and the foot and cycling questionnaire permission was given by Hayley Uden from University of South Australia, Australia [18] that we adapted to MQ-21.
- (b)
- New translation: two freelance bilingual physicians from Spain (native Spanish speakers) translated the MQ-21 and Borg CR10 Scale® into Spanish. In addition, the main author adapted the questionnaire and was part of the translation at all times according to the suggestions above [17].
- (c)
- Accommodation: a meeting was undertaken to find any discrepancies in the new translations with every translator separately. A written memory documented the translation procedure.
- (d)
- The accommodate new translated version of the MQ-21 and Borg CR10 Scale® was translated again to English by other two native English speaker physicians. The translators were blinded and did not seen the version of the MQ-21 and Borg CR10 Scale®.
- (e)
- The new translated version and the original version were compared to guarantee the analogy of the version translation, and any difference or unsure phrasings were adapted.
- (f)
- Harmonization: the unify group was composed by the preceding and onwards translators, a investigation physician, and a performer language expert.
- (g)
- Cognitive meetings of the new version were realized in a privy physician praxis. Eight physicians and eight non-clinicians, with no foot disorders, took part. The main author, retrospectively, accomplished the cognitive polls orally. Firstly, each participant accomplished the MQ-21 and Borg CR10 Scale® and was afterwards questioned about the purpose of the item and their reply to supply potential mistakes and problems to reduce future mistakes and non-reply [19].
- (h)
- The outcomes from the deliberate interviews were analyzed and a closed adapted version was approved. Any arguments as to the composition of the MQ-21 and Borg CR10 Scale® were provided in writing [17].
- (i)
- The concluded version was edited, probed for spelling and grammar arguments, and disposal was finished.
- (j)
- An end report kept a record of the translation method. A language domain of Spanish secondary school scale was the purpose of the latest translation.
2.6. Sample Magnitude
2.7. Statistical Analysis
3. Results
3.1. Descriptive Data
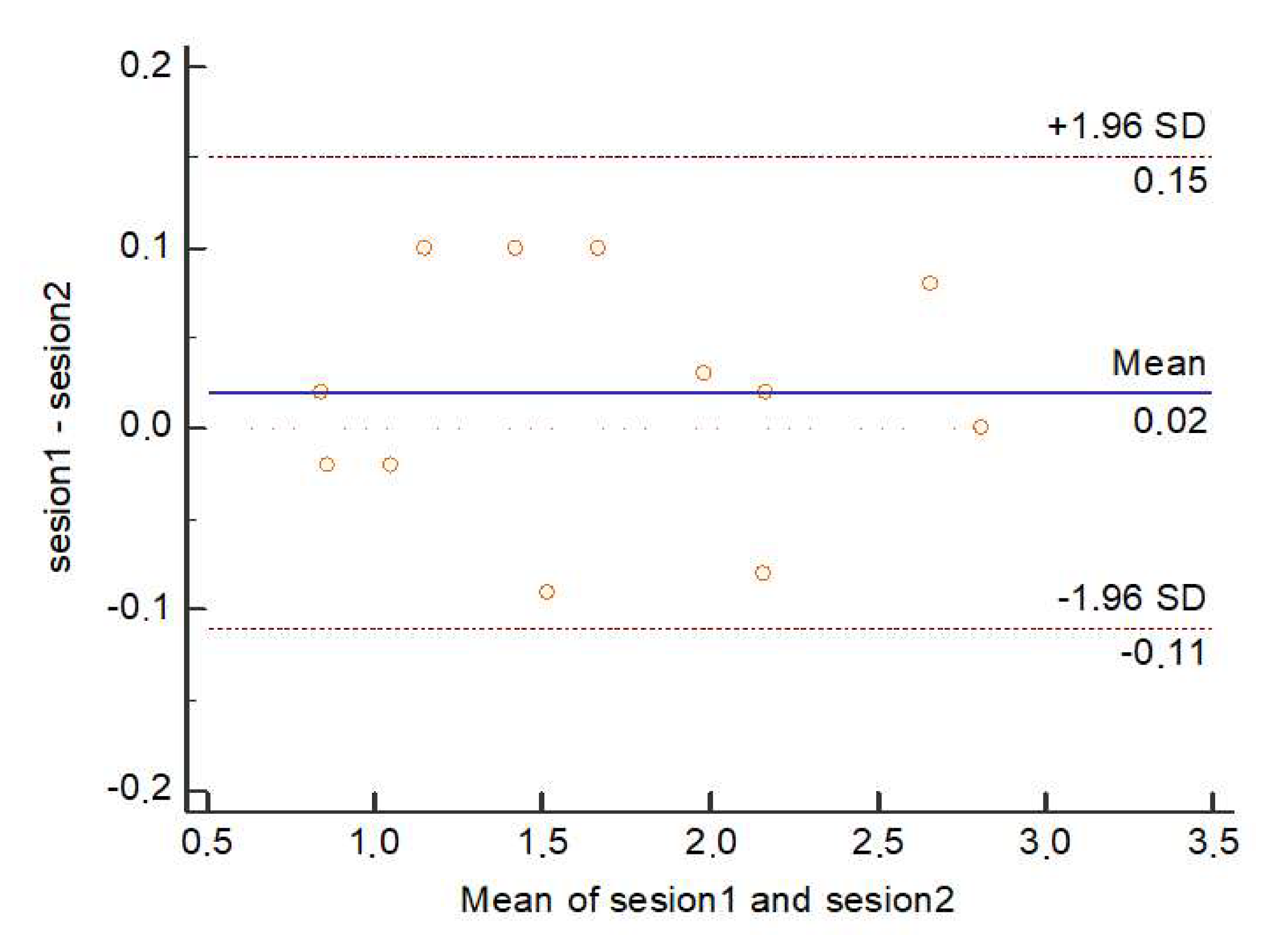
3.2. Reliability and Reproducibility
4. Discussion
4.1. Reliability and Reproducibility
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Anesdor—Asociación Nacional de Empresas del Sector Dos Ruedas. Available online: https://www.anesdor.com/ (accessed on 6 November 2018).
- Anuario Estadístico General. Available online: http://www.dgt.es/es/seguridad-vial/estadisticas-e-indicadores/publicaciones/anuario-estadistico-general/ (accessed on 6 November 2018).
- Mobility and Transport; European Commission: Brussel, Belgium, 2018.
- Khanna, A.; Bagouri, E.O.; Gougoulias, N.; Maffulli, N. Sport injuries in enduro riders: A review of literature. Muscle Ligaments Tendons J. 2019, 5, 200. [Google Scholar] [CrossRef]
- Guo, Y.; Wang, J.; Peeta, S.; Anastasopoulos, P.C. Personal and societal impacts of motorcycle ban policy on motorcyclists’ home-to-work morning commute in China. Travel Behav. Soc. 2020, 19, 137–150. [Google Scholar] [CrossRef]
- Chang, F.; Li, M.; Xu, P.; Zhou, H.; Haque, M.M.; Huang, H. Injury severity of motorcycle riders involved in traffic crashes in Hunan, China: A mixed ordered logit approach. Int. J. Environ. Res. Public Health 2016, 13, 714. [Google Scholar] [CrossRef]
- Priego Quesada, J.I.; Kerr, Z.Y.; Bertucci, W.M.; Carpes, F.P. The association of bike fitting with injury, comfort, and pain during cycling: An international retrospective survey. Eur. J. Sport Sci. 2019, 19, 842–849. [Google Scholar] [CrossRef]
- Priego Quesada, J.I.; Kerr, Z.Y.; Bertucci, W.M.; Carpes, F.P. A retrospective international study on factors associated with injury, discomfort and pain perception among cyclists. PLoS ONE 2019, 14, e0211197. [Google Scholar] [CrossRef]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work. Environ. Health 1990, 16 (Suppl. 1), 55–58. [Google Scholar] [CrossRef]
- Borg, E.; Borg, G.; Larsson, K.; Letzter, M.; Sundblad, B.-M. An index for breathlessness and leg fatigue. Scand. J. Med. Sci. Sports 2010, 20, 644–650. [Google Scholar] [CrossRef]
- Landorf, K.B. Reliability of the foot function index: A report of the AOFAS outcomes committee. Foot ankle Int. 2006, 27, 867–868. [Google Scholar] [CrossRef]
- Agel, J.; Beskin, J.L.; Brage, M.; Guyton, G.P.; Kadel, N.J.; Saltzman, C.L.; Sands, A.K.; Sangeorzan, B.J.; SooHoo, N.F.; Stroud, C.C.; et al. Reliability of the Foot Function Index:: A report of the AOFAS Outcomes Committee. Foot ankle Int. 2005, 26, 962–967. [Google Scholar] [CrossRef]
- Kalsom Mohd Shafiei, U.; Karmegam, K.; Shamsul Bahri Mohd, T.; Goh Yong, M.; Irniza, R.; Ayuni Nabilah, A. The effectiveness of new model of motorcycle seat with built-in lumbar support. J. Teknol. Sci. Eng. 2015, 77, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Karmegam, K.; Sapuan, S.; Ismail, M.; Ismail, N.; Bahr, S. Motorcyclist’s Riding Discomfort in Malaysia: Comparison of BMI, Riding Experience, Riding Duration and Riding Posture. Hum. Factors Ergon. Manuf. Serv. Ind. 2013, 23, 267–278. [Google Scholar] [CrossRef]
- Beaton, D.; Bombadier, C.; Guilleman, F.; Ferraz, M. Recommendations for the Cross-Cultural Adaption of the DASH and QuickDASH Outcome Measures; Institute for Work of Health: Toronto, ON, USA, 2007. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. ISPOR Task Force for Translation and Cultural Adaptation Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uden, H.; Jones, S.; Grimmer, K. Foot Pain and Cycling: A survey of frequency, type, location, associations and amelioration of foot pain. J. Sci. Cycl. 2012, 1, 28–34. [Google Scholar]
- Willis, G.; DeMaio, T.; Harris-Kojetin, B. Is the bandwagon headed to the methodological promised land? Evaluating the validity of cognitive interviewing techniques. In Cognition and Survey Research; Sirken, M., Herrmann, D., Schechter, S., Schwarz, N., Tanur, J., Tourangeau, R., Eds.; Wiley Blackwell: New York, NY, USA, 1999; pp. 133–154. [Google Scholar]
- de Vet, H.; Terwee, C.; Mokkink, L.; Knol, D. Measurement in Medicine; Cambridge University Press: New York, NY, USA, 2011; ISBN 978-0-521-13385-2. [Google Scholar]
- Portney, L.; Watkins, M. Foundations of Clinical Research: Applications to Practice. Surv. Ophthalmol. 2002, 47, 598. [Google Scholar]
- Giraudeau, B.; Mary, J.Y. Planning a reproducibility study: How many subjects and how many replicates per subject for an expected width of the 95 per cent confidence interval of the intraclass correlation coefficient. Stat. Med. 2001, 20, 3205–3214. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Khamis, N.K.; Deros, B.M.; Nuawi, M.Z. Understanding the Effect of Discomfort Level towards Motorcycle Riders among Teenagers: A Preliminary Study. Appl. Mech. Mater. 2014, 663, 480–484. [Google Scholar] [CrossRef]
- Casado-Hernández, I.; Becerro-de-Bengoa-Vallejo, R.; López-López, D.; Gómez-Bernal, A.; Losa-Iglesias, M.E. Aluminum foot insoles reduce plantar forefoot pressure and increase foot comfort for motorcyclists. Prosthet. Orthot. Int. 2018, 42, 606–611. [Google Scholar] [CrossRef]
- Jeffers, R.F.; Boon Tan, H.; Nicolopoulos, C.; Kamath, R.; Giannoudis, P.V. Prevalence and patterns of foot injuries following motorcycle trauma. J. Orthop. Trauma 2004, 18, 87–91. [Google Scholar] [CrossRef]
- de Rome, L.; Fitzharris, M.; Baldock, M.; Fernandes, R.; Ma, A.; Brown, J. The prevalence of crash risk factors in a population-based study of motorcycle riders. Injury 2016, 47, 2025–2033. [Google Scholar] [CrossRef]
- De Rome, L.; Ivers, R.; Fitzharris, M.; Du, W.; Haworth, N.; Heritier, S.; Richardson, D. Motorcycle protective clothing: Protection from injury or just the weather? Accid. Anal. Prev. 2011, 43, 1893–1900. [Google Scholar] [CrossRef]
- Wu, D.; Hours, M.; Ndiaye, A.; Coquillat, A.; Martin, J.L. Effectiveness of protective clothing for motorized 2-wheeler riders. Traffic Inj. Prev. 2019, 20, 196–203. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Individal Demographics | Total Group Mean ± SD Range N = 48 | Men Mean ± SD Range N = 45 | Women Mean ± SD Range N = 3 | p Value |
|---|---|---|---|---|
| Age (years) | 37.66 ± 6.11 (35.93–39.39) | 37.68 ± 6.12 (35.89–39.47) | 37.33 ± 7.37 (19.02–55.64) | 0.942 * |
| Weight (kg) | 73.58 ± 7.11 (71.57–75.59) | 74.62 ± 6.00 (72.86–76.37) | 58 ± 2.64 (51.44–64.56) | 0.001 * |
| Height (cm) | 175.54 ± 5.30 (174.04–177.04) | 176.31 ± 4.51( 174.99–177.62) | 164 ± 1.00 (161.52–166.48) | 0.001 ** |
| BMI (kg/m2) | 23.83 ± 1.50 (23.40–24.26 | 23.98 ± 1.41 (23.56–24.39) | 21.56 ± 0.96 (19.18–23.94) | 0.001 * |
| Type of Motorcycle | n (%) | Reason for Motorcycling | n (%) |
|---|---|---|---|
| Sport | 35 (72.91%) | Work | 4 (8.33%) |
| Turismo | 4 (8.33%) | Competition | 8 (16.66%) |
| Naked/Seminaked | 5 (10.41%) | Recreation | 35 (72.91%) |
| Trail | 1 (2.08%) | Other | 1 (2.08%) |
| Custom | 1(2.08%) |
| Comfort Items | Test (n = 48) Mean ± SD (95% CI) | Retest (n = 48) MEAN ± SD (95% CI) | Total Mean ± SD (95% CI) | ICC (95% CI) | p Value |
|---|---|---|---|---|---|
| Item 1: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you ever driving the motorcycle (head/neck) | 2.70 ± 2.96 (1.87–3.54) | 2.62 ± 2.87 (1.81–3.43) | 2.66 ± 0.05 (2.62–2.69) | 0.991 (0.985–0.995) | 0.874 |
| Item 2: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you ever driving the motorcycle (shoulder) | 1.47 ± 2.52 (0.76–2.19) | 1.56 ± 2.63 (0.81–2.30) | 1.51 ± 0.06 (1.47–1.55) | 0.995 (0.992–0.997) | 0.970 |
| Item 3: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you ever driving the motorcycle (back) | 2.18 ± 2.80 (1.39–2.98) | 2.16 ± 2.77 (1.38–2.95) | 2.17 ± 0.05 (2.16–2.17) | 0.987 (0.977–0.993) | 0.968 |
| Item 4: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you at any time driving the motorcycle (arm) | 2.00 ± 2.55 (1.27–2.72) | 1.97 ± 2.52 (1.26–2.69) | 1.98 ± 0.02 (1.97–1.99) | 0.982 (0.969–0.990) | 0.874 |
| Item 5: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you ever driving the motorcycle (lumbar) | 2.12 ± 2.52 (1.41–2.83) | 2.20 ± 2.62 (1.46–2.95) | 2.16 ± 0.05 (2.12–2.19) | 0.971 (0.947–0.983) | 0.799 |
| Item 6: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you ever driving the motorcycle (buttocks) | 1.47 ± 2.07 (0.89–2.06) | 1.37 ± 1.94 (0.82–1.92) | 1.42 ± 0.07 (1.38–1.46) | 0.947 (0.905–0.970) | 0.956 |
| Item 7: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you ever driving the motorcycle (back thigh) | 1.04 ± 1.94 (0.49–1.59) | 1.06 ± 1.76 (0.56–1.56) | 1.05 ± 0.01 (1.04–1.05) | 0.963 (0.935–0.979) | 0.839 |
| Item 8: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you ever driving the motorcycle (knee) | 1.72 ± 2.57 (1.00–2.45) | 1.62 ± 2.43 (0.93–2.31) | 1.67 ± 0.07 (1.63–1.72) | 0.988 (0.978–0.993) | 0.958 |
| Item 9: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you ever driving the motorcycle (calf) | 0.85 ± 1.99 (0.28–1.41) | 0.87 ± 1.86 (0.34–1.40) | 0.86 ± 0.01 (0.85–0.86) | 0.881 (0.787–0.933) | 0.956 |
| Item 10: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you ever driving the motorcycle (ankle) | 0.85 ± 1.89 (0.31–1.38) | 0.83 ± 1.86 (0.30–1.35) | 0.84 ± 0.01 (0.83–0.84) | 0.909 (0.838–0.949) | 0.780 |
| Item 11: Indicates according to a scale of discomfort, 0 being no pain and 10 very painful, what part has bothered you at any time driving the motorcycle (foot) | 1.20 ± 1.91 (0.66–1.74) | 1.10 ± 1.74 (0.61–1.59) | 1.15 ± 0.07 (1.11–1.19) | 0.924 (0.864–0.957) | 0.461 |
| Item 12: About the foot. This discomfort or pain (select + from 1 reply). Does not let me ride a motorcycle = 1; reduces my performance = 2; it bothers me but I can still drive the motorcycle = 3; it does not bother me at all = 4; other = 5 | 2.81 ± 0.73 (2.60–3.02) | 2.81 ± 0.73 (2.60–3.02) | 2.81 ± 0.73 (2.60–3.02) | 1.000 (1.000–1.000) | 1.000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casado-Hernández, I.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Soriano-Medrano, A.; Morales-Ponce, Á.; Martiniano, J.; López-López, D.; Calvo-Lobo, C. Development and Validation of the Overall Foot Pain Questionnaire in Motorcycle Riders. Int. J. Environ. Res. Public Health 2020, 17, 2233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072233
Casado-Hernández I, Becerro-de-Bengoa-Vallejo R, Losa-Iglesias ME, Soriano-Medrano A, Morales-Ponce Á, Martiniano J, López-López D, Calvo-Lobo C. Development and Validation of the Overall Foot Pain Questionnaire in Motorcycle Riders. International Journal of Environmental Research and Public Health. 2020; 17(7):2233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072233
Chicago/Turabian StyleCasado-Hernández, Israel, Ricardo Becerro-de-Bengoa-Vallejo, Marta Elena Losa-Iglesias, Alfredo Soriano-Medrano, Ángel Morales-Ponce, João Martiniano, Daniel López-López, and César Calvo-Lobo. 2020. "Development and Validation of the Overall Foot Pain Questionnaire in Motorcycle Riders" International Journal of Environmental Research and Public Health 17, no. 7: 2233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072233