Respiratory Health in a Community Living in Close Proximity to Gold Mine Waste Dumps, Johannesburg, South Africa

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
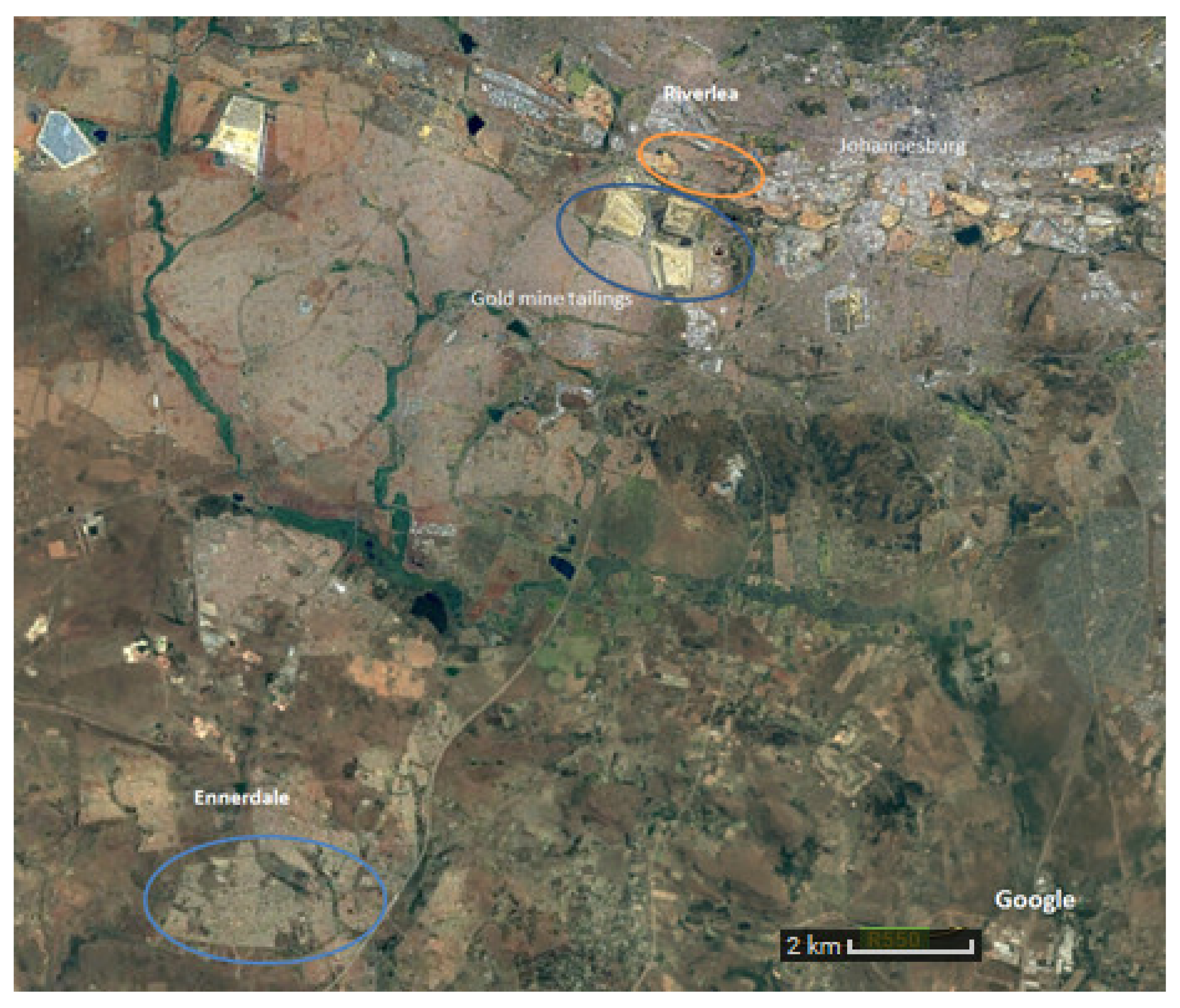
2.1. Study Population and Setting
2.2. Exposure Estimation
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethical Approval and Permissions
3. Results
4. Discussion
4.1. Symptoms
4.2. Silicosis
4.3. Tuberculosis
4.4. COPD
4.5. Spirometry
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hobbs, P.J.; Oelofse, S.H.H.; Rascher, J.; Cobbing, J.E. Pollution reality of gold mining waste on the Witwatersrand. Resource. 2010, 12, 51–55. [Google Scholar]
- AngloGold Ashanti. Report to Society. 2008. Available online: http://www.debeersgroup.com/Media-Centre-Landing-page/Reports/ (accessed on 3 March 2017).
- Andraos, C.; Utembe, W.; Gulumian, M. Exceedance of environmental exposure limits to crystalline silica in communities surrounding gold mine tailings storage facilities in South Africa. Sci. Total Environ. 2018, 619, 504–516. [Google Scholar] [CrossRef]
- Malatse, M.; Ndlovu, S. The viability of using the Witwatersrand gold mine tailings for brickmaking. J S. Afr. Inst. Min. Metall. 2015, 115, 321–327. [Google Scholar] [CrossRef]
- Belle, B.K. Respirable dust dosimeter (RDD) for personal dust exposure assessment-a laboratory investigation. Clean Air J. Tydskr vir Skoon Lug. 2005, 14, 7–12. [Google Scholar]
- Ojelede, M.; Annegarn, H.J.; Kneen, M.A. Evaluation of aeolian emissions from gold mine tailings on the Witwatersrand. Aeolian Res. 2012, 3, 477–486. [Google Scholar] [CrossRef]
- Kneen, M.A.; Ojelede, M.E.; Brikowski, T.H.; Annegarn, H.J. Increased Aeolian Particulate Health Risk From Ultrafine Silicic Gold Mine Tailings on the Witwatersrand. In Proceedings of the GSA Denver Annual Meeting, Denver, CO, USA, 2 November 2010; No. 157. Available online: https://gsa.confex.com/gsa/2010AM/webprogram/Paper178597.html (accessed on 3 March 2018).
- Kneen, M.A.; Ojelede, M.E.; Annegarn, H.J. Housing and population sprawl near tailings storage facilities in the Witwatersrand: 1952 to current. S. Afr. J. Sci. 2015, 111, 1–9. [Google Scholar] [CrossRef]
- Trivedi, R.; Chakraborty, M.K.; Tewary, B.K. Dust dispersion modeling using fugitive dust model at an opencast coal project of Western Coalfields Limited, India. J. Sci. Ind. Res. (India) 2009, 68, 71–78. [Google Scholar]
- The United States Agency of Natural Resources. Air Toxics Report. 1998. Available online: https://dec.vermont.gov/sites/dec/files/documents/Air_Toxics_Report_Feb_1998_complete_0.pdf (accessed on 13 September 2018).
- United States Environmental Protection Agency. Ambient Levels and Non-cancer Health Effects of Inhaled Crystalline and Amorphous Silica: Health Issue Assessment. 1996. Available online: http://ofmpub.epa.gov/eims/eimscomm.getfile?p_download_id=4608 (accessed on 26 January 2018).
- Taylor, A.N.; Cullinan, P.; Blanc, P.; Pickerin, A. Parkes’ Occupational Lung Disorders, 4th ed.; CRC Press: London, UK, 2016; pp. 190–191. [Google Scholar]
- Rees, D.; Murray, J. Silica, silicosis and tuberculosis. Int. J. Tuberc. Lung Dis. 2007, 11, 474–484. [Google Scholar]
- Mayan, O.N.; Gomes, M.J.; Henriques, A.; Silva, S.; Begonha, A. Health survey among people living near an abandoned mine. A case study: Jales Mine, Portugal. Environ. Monit. Assess. 2006, 123, 31–40. [Google Scholar] [CrossRef]
- Nkosi, V.; Wichmann, J.; Voyi, K. Mine dumps, wheeze, asthma, and rhinoconjunctivitis among adolescents in South Africa: Any association? Int. J. Environ. Health Res. 2015, 25, 583–600. [Google Scholar] [CrossRef] [Green Version]
- Nkosi, V.; Wichmann, J.; Voyi, K. Chronic respiratory disease among the elderly in South Africa: Any association with proximity to mine dumps? Environ. Health 2015, 14, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathee, A.; Harpham, T.; Naicker, N.; Barnes, B.R.; Plagerson, S.; Feit, M.; Swart, A.; Naidoo, S. Overcoming fieldwork challenges in urban health research in developing countries: A research note. Int. J. Soc. Res. Methodol. 2010, 13, 171–178. [Google Scholar] [CrossRef]
- Makene, C. Housing-Related Risk Factors for Respiratory Disease in Low Cost Housing Settlements in Johannesburg, South Africa. 2007. Available online: http://hdl.handle.net/10539/5762 (accessed on 14 March 2018).
- Statistics South Africa. Census 2011 Statistical Release-P0301.4. Pretoria Statistics South Africa. 2012. Available online: https://www.statssa.gov.za/publications/P03014/P030142011.pdf (accessed on 4 September 2017).
- International Labour Office. International Classification of Radiographs of Pneumoconioses rev ed. 2002 Occupational Safety and Health Series No. 22. Br. J. Ind. Med. 2002, 422, 93–96. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef] [PubMed]
- Norboo, T.; Angchuk, P.T.; Yahya, M.; Kamat, S.R.; Pooley, F.D.; Corrin, B.; Kerr, I.H.; Bruce, N.; Ball, K.P. Silicosis in a Himalayan village population: Role of environmental dust. Thorax 1991, 46, 341–343. [Google Scholar] [CrossRef] [Green Version]
- Saiyed, H.N.; Sharma, Y.K.; Sadhu, H.G.; Norboo, T.; Patel, P.D.; Patel, T.S.; Venkaiah, K.; Kashyap, S.K. Non-occupational pneumoconiosis at high altitude villages in central Ladakh. Br. J. Ind. Med. 1991, 48, 825–829. [Google Scholar] [CrossRef] [Green Version]
- Bhagia, L.J. Non-occupational exposure to silica dust. Indian J. Occup. Environ. Med. 2012, 16, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Derbyshire, E. Natural Minerogenic Dust and Human Health. AMBIO J. Hum. Environ. 2007, 36, 73–78. [Google Scholar] [CrossRef]
- Den Boon, S.; Van Lill, S.W.P.; Borgdorff, M.W.; Enarson, D.A.; Verver, S.; Bateman, E.D.; Irusen, E.; Lombard, C.J.; White, N.W.; de Villiers, C.; et al. High prevalence of tuberculosis in previously treated patients, Cape Town, South Africa. Emerg. Infect. Dis. 2007, 13, 1189–1194. [Google Scholar] [CrossRef]
- Buist, A.S.; McBurnie, M.A.; Vollmer, W.M.; Gillespie, S.; Burney, P.; Mannino, D.M.; Menezes, A.M.; Sullivan, S.D.; Lee, T.A.; Weiss, K.B.; et al. International variation in the prevalence of COPD (the BOLD Study): A population-based prevalence study. Lancet 2007, 370, 741–750. [Google Scholar] [CrossRef]
- Guo, C.; Zhang, Z.; Lau, A.K.H.; Lin, C.Q.; Chuang, Y.C.; Chan, J.; Jiang, W.K.; Tam, T.; Yeoh, E.K.; Chan, T.C.; et al. Articles Effect of long-term exposure to fine particulate matter on lung function decline and risk of chronic obstructive pulmonary disease in Taiwan: A longitudinal, cohort study. Lancet Planet Health 2018, 2, e114–e125. [Google Scholar] [CrossRef]
- Park, S.W.; Kim, B.G.; Kim, J.W.; Park, J.W.; Kim, J.I. A cross-sectional study on the pulmonary function of residents in two urban areas with different PM 10 concentrations: Data from the fourth Korea national health and nutrition examination survey ( KNHANES ) 2007–2009. Ann. Occup. Environ. Med. 2018, 30, 47. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhou, Y.; Liu, S.; Chen, X.; Zou, W.; Zhao, D.; Li, X.; Pu, J.; Huang, L.; Chen, J.; et al. Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease: Results from a cross-sectional study in China. Thorax 2017, 72, 788–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardie, J.A.; Buist, A.S.; Vollmer, W.M.; Ellingsen, I.; Bakke, P.S.; Mørkve, O. Risk of over-diagnosis of COPD in asymptomatic elderly never-smokers. Eur. Respir. J. 2002, 20, 1117–1122. [Google Scholar] [CrossRef] [Green Version]
- Miller, M.R.; Quanjer, P.H.; Swanney, M.P.; Ruppel, G.; Enright, P.L. Interpreting lung function data using 80% predicted and fixed thresholds misclassifies more than 20% of patients. Chest 2011, 139, 52–59. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Data Collection Method | Definition |
|---|---|---|
| Independent Variables | ||
| Cumulative exposure index | Study questionnaire | Derived using the quotient of number of years lived in an exposure group and the intensity weighting as determined by Ojelede et al. [6] |
| Occupational history of exposure to vapours, gas, dust and fumes | Study questionnaire | Exposure for a year or more to vapors, gas, dust, and/or fumes. |
| Exposure to biomass fuels | Study questionnaire | If a biomass fuel is used for either cooking or heating. |
| Mean monthly household income | Study questionnaire | We used mean monthly household income as a proxy for socio-economic status. |
| Smoking history | Study questionnaire | Positive history is at least one pack-year of smoking cigarettes in current or ex-smokers. |
| Smoking pack-years | Study questionnaire | Number of cigarettes smoked per day divided by 20 and multiplied by the number of years of smoking. |
| Dependent respiratory variables | ||
| Upper respiratory tract symptoms | Study questionnaire | At least one of the following: rhinorrhoea, nasal congestion, oro-pharyngitis, a hoarse voice, or chronic sneezing in the last two weeks without having the flu. |
| Ocular symptoms | Study questionnaire | The presence of itchy/watery eyes in the last two weeks. |
| Lower respiratory tract symptoms | ||
| Shortness of breath | Study questionnaire | Breathlessness walking up a slight hill. |
| Chronic cough | Study questionnaire | A cough most days for 3 consecutive months or more during the year. |
| Chronic bronchitis | Study questionnaire | Productive cough for at least three months in a year for at least two consecutive years. |
| Wheezy chest | Study questionnaire | A wheezing or whistling chest in the last year. |
| Self-reported diagnosis by a healthcare practitioner | ||
| Emphysema or chronic obstructive pulmonary disease (COPD) | Study questionnaire | Diagnosed or treated by a nurse or a doctor. |
| Asthma | Study questionnaire | Diagnosed or treated by a nurse or a doctor. |
| Pulmonary tuberculosis | Study questionnaire | Diagnosed or treated by a nurse or a doctor. |
| Objective findings of disease | ||
| COPD on spirometry | Spirometry | Forced expiratory volume in one second (FEV1)/ forced vital capacity (FVC) ratio < lower limit of normal using the Global Lung Function Initiative (GLI) 2012 reference equations |
| Radiological evidence of probable tuberculosis | Chest X-ray | Typical signs of past or present tuberculosis, such as presence of a focal infiltrate, cavity formation, hilar adenopathy, or a miliary pattern. A positive diagnosis required agreement by 2 of the 3 readers. |
| Radiological silicosis | Chest X-ray | Diagnosis based on the ILO International Classification of Radiographs of Pneumoconioses. Silicosis was defined as a profusion of 1/0 or more reported by at least two of the three readers. |
| Characteristics | Riverlea | Ennerdale | |
|---|---|---|---|
| High Exposure | Medium Exposure | Low Exposure | |
| n (%) | n (%) | n (%) | |
| Population Size | 93 (30.0) | 133 (42.9) | 84 (27.1) |
| Median age in years (IQR) | 49 (22–72) Range (18–81) | 53 (21–81) Range (18–88) | 46 (20–68) Range (19–73) |
| Sex | |||
| Men | 36 (38.7) | 50 (37.6) | 27 (32.1) |
| Women | 57 (61.3) | 83 (62.4) | 56 (67.9) |
| Smoking history | 60 (64.5) | 58 (43.6) | 39 (46.4) |
| Smoking pack-years | |||
| Never smoked (<1 pack-year) | 35 (37.6) | 77 (57.9) | 45 (53.6) |
| 1–10 | 24 (25.8) | 22 (16.5) | 22 (26.2) |
| 11–20 | 15 (16.3) | 20 (15.0) | 10 (11.9) |
| >20 | 19 (20.4) | 14 (10.5) | 7 (8.3) |
| Education | |||
| None/Primary | 21 (23.1) | 14 (10.5) | 10 (11.9) |
| Secondary | 65 (71.4) | 82 (61.7) | 56 (66.7) |
| Tertiary | 5 (5.5) | 37 (27.8) | 18 (21.4) |
| Monthly mean income for households | |||
| <R1000 | 36 (39.6) | 27 (20.3) | 15 (17.9) |
| R1000–R5000 | 40 (43.9) | 34 (25.6) | 28 (33.3) |
| R5001–R9999 | 11 (12.1) | 40 (30.10 | 25 (29.8) |
| ≥R10000 | 4 (4.4) | 32 (24.0) | 16 (19.0) |
| Median years lived in exposure group (IQR) | 38 (15–68) Range (2–76) | 20 (3–65) Range (1–80) | 16 (4–44) Range (2–61) |
| Reported dustiness outdoors during windy weather | 85 (93.4) | 119 (90.2) | 75 (89.3) |
| Reported dustiness indoors during windy weather | 58 (63.7) | 86 (65.2) | 55 (65.5) |
| Use of biomass fuels | 3 (4.9) | 24 (21.6) | 20 (24.4) |
| House had an asbestos roof | 65 (71.4) | 39 (29.6) | 1 (1.2) |
| Occupational history of exposure to vapour, gas, dust, or fumes | 49 (53.9) | 37 (27.8) | 15 (17.9) |
| No. of people who participated in chest X-rays | 55 (59.1) | 69 (51.9) | 53 (63.1) |
| No. of people who participated in spirometry | 43 (46.2) | 59 (44.3) | 47 (56.0) |
| Variables | Riverlea | Ennerdale | Crude Odds Ratio (95% CI) | |||
|---|---|---|---|---|---|---|
| High Exposure | Medium Exposure | Low Exposure | High vs. Low Exposure | High vs. Medium Exposure | Medium vs. Low Exposure | |
| n (%) | n (%) | n (%) | ||||
| Population Size | 93 (30.0) | 133 (42.9) | 84 (27.1) | |||
| Upper respiratory tract symptoms | 63 (67.7) | 59 (44.4) | 34 (40.5) | 2.83 (1.58–5.08) | 2.63 (1.52–4.58) | 1.17 (0.67–2.04) |
| Ocular symptoms | 30 (32.3) | 31 (23.3) | 13 (15.5) | 2.63 (1.52–4.58) | 1.57 (0.87–2.83) | 1.66 (0.81–3.39) |
| Shortness of breath | 30 (32.6) | 31 (23.5) | 23 (27.4) | 1.26 (0.66–2.41) | 1.57 (0.87–2.83) | 0.81 (0.43–1.51) |
| Chronic cough | 32 (34.4) | 21 (15.8) | 27 (32.1) | 1.11 (0.59–2.07) | 2.80 (1.49–5.27) | 0.40 (0.21–0.76) |
| Chronic bronchitis | 19 (20.4) | 10 (7.5) | 12 (14.3) | 1.54 (0.70–3.40) | 3.16 (1.39–7.16) | 0.49 (0.21–1.19) |
| Wheezy chest | 40 (43.5) | 28 (21.2) | 16 (19.1) | 3.21 (1.62–6.34) | 2.83 (1.58–5.08) | 1.13 (0.57–2.25) |
| Self-reported HCP a diagnosis of emphysema or COPD | 8 (8.6) | 10 (7.5) | 7 (8.3) | 1.03 (0.36–2.99) | 1.16 (0.44–3.05) | 0.89 (0.33–2.45) |
| Self-reported HCP diagnosis of asthma | 8 (8.6) | 10 (7.5) | 7 (8.3) | 1.03 (0.36–2.99) | 1.16 (0.44–3.05) | 0.89 (0.33–2.45) |
| Self-reported HCP diagnosis of TB b | 4 (4.3) | 4 (3.0) | 6 (7.1) | 0.58 (0.16–2.15) | 1.45 (0.35–5.95) | 0.40 (0.11–1.47) |
| n = 55 | n = 69 | n = 53 | ||||
| Radiological evidence of probable TB | 6 (10.9) | 12 (17.4) | 4 (7.5) | 1.50 (0.40–5.65) | 0.58 (0.20–1.67) | 2.58 (0.78–8.51) |
| Evidence of silicosis on chest X-ray | 0 (0) | 0 (0) | 0 (0) | |||
| n = 43 | n = 59 | n = 47 | ||||
| COPD on spirometry | 8 (18.6) | 6 (10.2) | 5 (10.6) | 1.92 (0.58–6.40) | 2.00 (0.67–5.95) | 0.95 (0.27–3.33) |
| Median FEV1 (IQR) | 98 (59–121) Range (45–132) | 91 (48–110) Range (30–121) | 93 (75–120) Range (25–143) | - | - | - |
| Median FVC (IQR) | 102 (71–134) Range (57–154) | 94 (60–117) Range (48–120) | 98 (79–119) Range (22–138) | - | - | - |
| Respiratory Health Outcomes | High vs. Low Exposure | High vs. Medium Exposure | Medium vs. Low Exposure |
|---|---|---|---|
| Upper respiratory tract symptoms | 2.76 (1.28–5.97) | 2.12 (1.01–4.42) | 1.31 (0.70–2.44) |
| Ocular symptoms | 4.68 (1.87–11.68) | 3.01 (1.32–6.89) | 1.55 (0.70–3.43) |
| Shortness of breath | 1.52 (0.67–3.44) | 2.21 (0.997–4.91) | 0.69 (0.34–1.39) |
| Chronic cough | 0.80 (0.34–1.84) | 2.18 (0.93–5.15) | 0.36 (0.17–0.77) |
| Chronic bronchitis | 1.76 (0.59–5.31) | 4.57 (1.35–15.48) | 0.39 (0.13–1.16) |
| Wheezy chest | 3.78 (1.60–8.96) | 3.60 (1.60–8.11) | 1.05 (0.48–2.32) |
| Self-reported diagnosis of COPD or emphysema by HCP a | 0.69 (0.17–2.78) | 1.14 (0.28–4.71) | 1.67 (0.51–5.46) |
| Self-reported diagnosis of asthma by HCP | 0.73 (0.18–2.99) | 0.96 (0.25–3.72) | 0.77 (0.25–2.37) |
| Self-reported diagnosis of TB b by HCP | 1.80 (0.33–9.81) | 0.52 (0.12–2.18) | 3.45 (0.83–14.41) |
| Radiological evidence of probable TB | 1.86 (0.34–10.35) | 0.46 (0.11–2.00) | 4.03 (0.93–17.49) |
| COPD on spirometry | 8.17 (1.01–65.85) | 3.40 (0.59–19.62) | 2.41 (0.37–15.54) |
| Respiratory Health Outcomes | Crude OR (95% CI) | aOR * (95% CI) |
|---|---|---|
| Upper respiratory tract symptoms | 1.0032 (1.0010–1.0053) | 1.0034 (1.00051–1.0064) |
| Ocular symptoms | 1.0028 (1.00050–1.0051) | 1.0031 (0.99987–1.0063) |
| Shortness of breath | 1.0029 (1.00064–1.0052) | 1.0027 (0.99958–1.0058) |
| Chronic cough | 1.00088 (0.9986–1.0032) | 0.99946 (0.9962–1.0027) |
| Chronic bronchitis | 1.0025 (0.99961–1.0053) | 1.0020 (0.9978–1.0062) |
| Wheezy chest | 1.0039 (1.0017–1.0062) | 1.0043 (1.0011–1.0075) |
| Self-reported diagnosis of COPD or emphysema by HCP a | 1.0033 (0.99989–1.0067) | 1.0017 (0.9963–1.0070) |
| Self-reported diagnosis of asthma by HCP | 1.0020 (0.9985–1.0056) | 0.9987 (0.9934–1.0039) |
| Self-reported diagnosis of TB b by HCP | 1.0018 (0.9978–1.0059) | 1.0005 (0.9949–1.0061)) |
| Radiological evidence of probable TB | 1.0019 (0.9978–1.0059) | 1.00084 (0.9953–1.0065) |
| COPD on spirometry | 1.0036 (0.99935–1.0078) | 1.010 (1.0014–1.019) |
| Variables | β | 95% CI | p-Value |
|---|---|---|---|
| FEV1 Cumulative Exposure Index (CEI) | 0.029 | −0.022-0.080 | 0.27 |
| Interaction term | |||
| smoking pack-years # CEI | |||
| <1 | Ref | ||
| 1–10 | 0.00014 | -0.080–0.080 | 0.997 |
| 11–20 | −0.19 | −0.30–(–0.077) | 0.001 |
| >20 | −0.040 | −0.12–0.38 | 0.31 |
| FVC Cumulative Exposure Index (CEI) | 0.062 | 0.016–0.11 | 0.008 |
| Interaction term | |||
| smoking pack-years # CEI | |||
| <1 | Ref | ||
| 1–10 | 3.39e–06 | -0.077-0.077 | 1.00 |
| 11–20 | −0.18 | −0.27–(–0.093) | <0.001 |
| >20 | –0.036 | –0.13–0.054 | 0.43 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iyaloo, S.; Kootbodien, T.; Naicker, N.; Kgalamono, S.; Wilson, K.S.; Rees, D. Respiratory Health in a Community Living in Close Proximity to Gold Mine Waste Dumps, Johannesburg, South Africa. Int. J. Environ. Res. Public Health 2020, 17, 2240. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072240
Iyaloo S, Kootbodien T, Naicker N, Kgalamono S, Wilson KS, Rees D. Respiratory Health in a Community Living in Close Proximity to Gold Mine Waste Dumps, Johannesburg, South Africa. International Journal of Environmental Research and Public Health. 2020; 17(7):2240. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072240
Chicago/Turabian StyleIyaloo, Samantha, Tahira Kootbodien, Nisha Naicker, Spo Kgalamono, Kerry S. Wilson, and David Rees. 2020. "Respiratory Health in a Community Living in Close Proximity to Gold Mine Waste Dumps, Johannesburg, South Africa" International Journal of Environmental Research and Public Health 17, no. 7: 2240. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072240