Health Literacy among Health and Social Care University Students

 ,
,
Abstract
:1. Introduction
1.1. Health Literacy
1.2. Health Literacy Levels
1.3. Research Justification
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurement Instruments
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
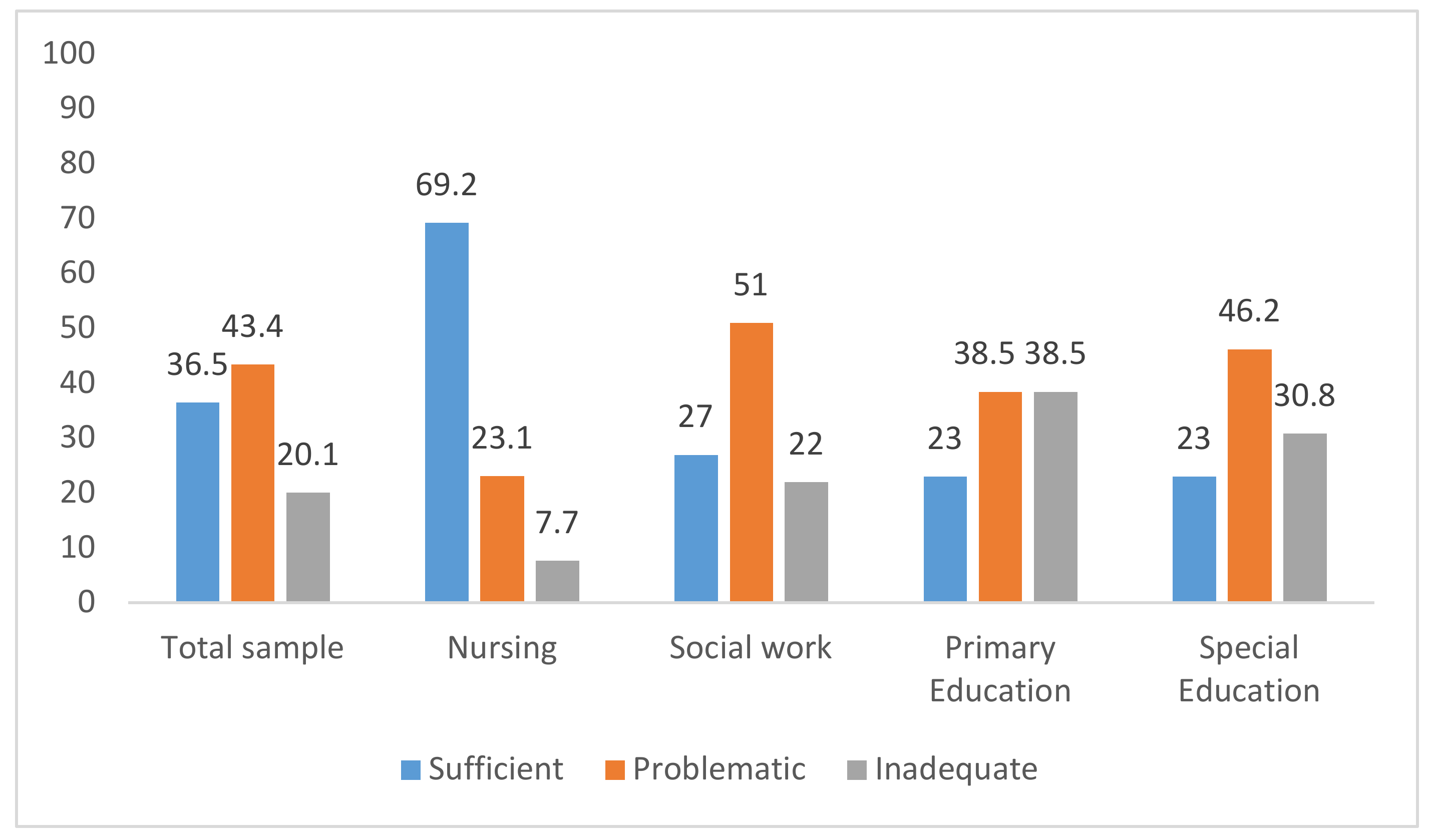
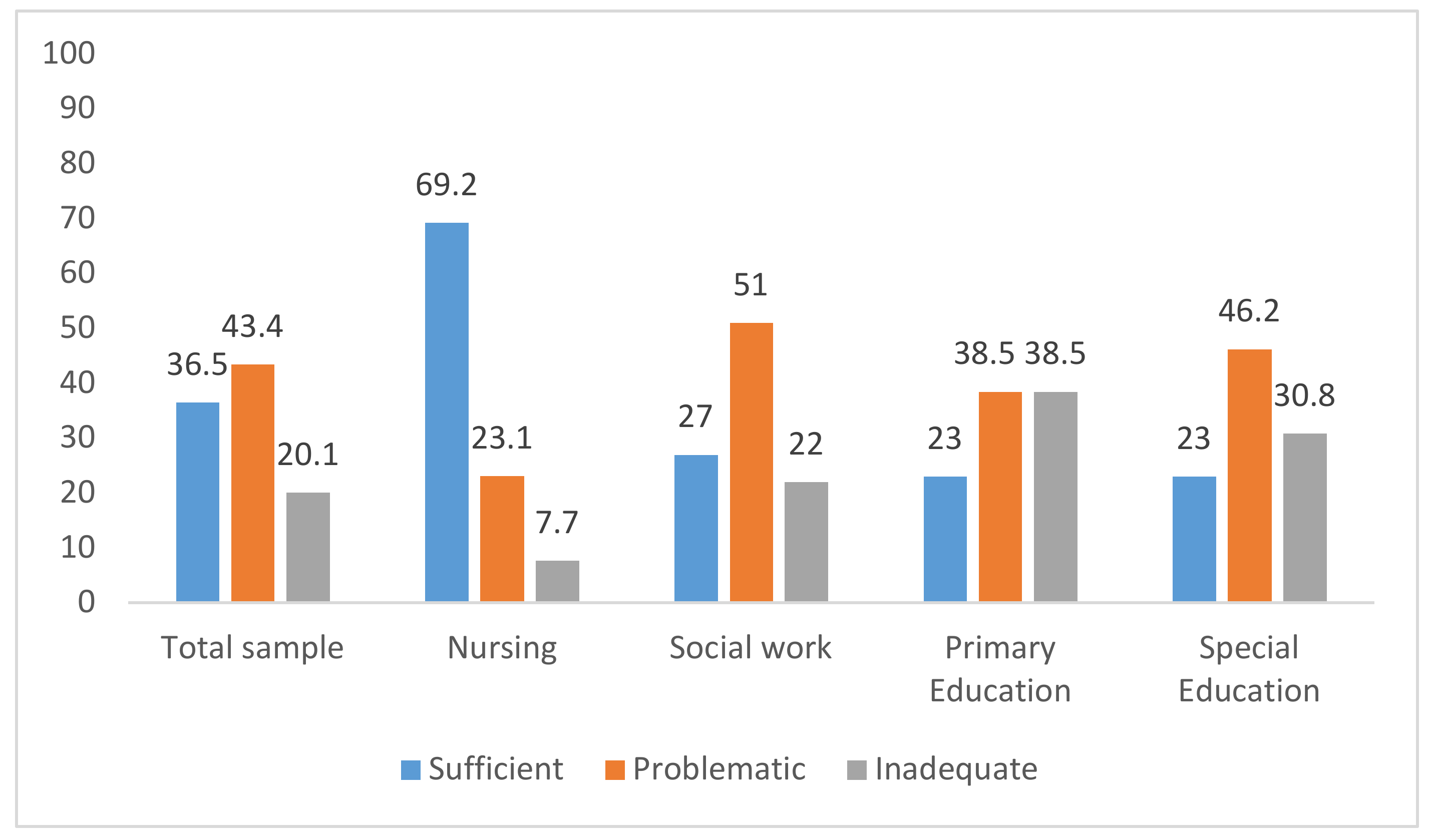
3.2. Health Literacy Results
4. Discussion
4.1. Limitations
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Health Promotion Glossary; World Health Organization: Geneve, Switzerland, 1998. [Google Scholar]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Codina, O.; Juvinyà-Canal, D.; Amil-Bujan, P.; Bertran-Noguer, C.; González-Mestre, M.A.; Masachs-Fatjo, E.; Santaeugenia, S.J.; Magrinya-Rull, P.; Salto-Cerezuela, E. Determinants of health literacy in the general population: Results of the Catalan health survey. BMC Public Health 2019, 19, 1122. [Google Scholar] [CrossRef] [PubMed]
- Runk, L.; Durham, J.; Vongxay, V.; Sychareun, V. Measuring health literacy in university students in Vientiane, Lao PDR. Health Promot. Int. 2016, 32, daw087. [Google Scholar] [CrossRef] [PubMed]
- Ozen, N.; Bal Ozkaptan, B.; Coskun, S.; Terzioglu, F. Health literacy of nursing students and its effective factors. Nurs. Forum 2019, 54, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Kickbusch, I.; Wait, S.; Maag, D. Navigating Health: The role of Health Literacy; Alliance for Health and the Future, International Longevity Centre-UK: London, UK, 2006; p. 22. [Google Scholar]
- Baker, D.W.; Wolf, M.S.; Feinglass, J.; Thompson, J.A. Health Literacy, Cognitive Abilities, and Mortality Among Elderly Persons. J. Gen. Intern. Med. 2008, 23, 723–726. [Google Scholar] [CrossRef] [Green Version]
- Bostock, S.; Steptoe, A. Association between low functional health literacy and mortality in older adults: Longitudinal cohort study. BMJ 2012, 344, e1602. [Google Scholar] [CrossRef] [Green Version]
- Pignone, M.P.; DeWalt, D.A. Literacy and health outcomes. J. Gen. Intern. Med. 2006, 21, 896–8997. [Google Scholar] [CrossRef] [Green Version]
- Laramee, A.S.; Morris, N.; Littenberg, B. Relationship of literacy and heart failure in adults with diabetes. BMC Health Serv. Res. 2007, 7, 98. [Google Scholar] [CrossRef] [Green Version]
- McCleary-Jones, V. Assessing Nursing Students’ Knowledge of Health Literacy. Nurse Educ. 2012, 37, 214–217. [Google Scholar] [CrossRef]
- Hadden, K.B. Health literacy training for health professions students. Patient Educ. Couns. 2015, 98, 918–920. [Google Scholar] [CrossRef]
- Brooks, C.; Ballinger, C.; Nutbeam, D.; Mander, C.; Adams, J. Nursing and allied health professionals’ views about using health literacy screening tools and a universal precautions approach to communication with older adults: A qualitative study. Disabil. Rehabil. 2018, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sukys, S.; Cesnaitiene, V.J.; Ossowsky, Z.M. Is Health Education at University Associated with Students’ Health Literacy? Evidence from Cross-Sectional Study Applying HLS-EU-Q. Biomed. Res. Int. 2017, 2017, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Budhathokia, S.; Pokharela, P.K.; Jhaa, N.; Moselenb, E.; Dixonb, R.; Bhattachana, M.; Osbornec, R.H. Health literacy of future healthcare professionals: A cross-sectional study among health sciences students in Nepal. Int. Health 2019, 11, 15–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rababah, J.A.; Al-Hammouri, M.M.; Drew, B.L.; Aldalaykeh, M. Health literacy: Exploring disparities among college students. BMC Public Health 2019, 19, 1401. [Google Scholar] [CrossRef] [Green Version]
- Pelikan, J.M.; Röthlin, F.; Ganahl, K. Measuring comprehensive health literacy in general populations: Validation of instrument, indices and scales of the HLS-EU study. In Proceedings of the 6th Annual Health Literacy Research Conference, Hyatt Regency, Bethesda, Rockville, MD, USA, 3–4 November 2014; Available online: http://www.bumc.bu.edu/healthliteracyconference/files/2014/06/Pelikan-et-al-HARC-2014-fin.pdf (accessed on 27 December 2019).
- Nolasco, A.; Barona, C.; Tamayo-Fonseca, N.; Irles, M.Á.; Más, R.; Tuells, J.; Pereyra-Zamora, P. Alfabetización en salud: Propiedades psicométricas del cuestionario HLS-EU-Q16. Gac. Sanit. 2018. pii: S0213-9111(18)30227-9. [Google Scholar] [CrossRef]
- Rouquette, A.; Nadot, T.; Labitrie, P.; Van den Broucke, S.; Mancini, J.; Rigal, L.; Ringa, V. Validity and measurement invariance across sex, age, and education level of the French short versions of the European Health Literacy Survey Questionnaire. PLoS ONE 2018, 13, e0208091. [Google Scholar] [CrossRef]
- Vamos, S.; Yeung, P.; Bruckermann, T.; Moselen, E.F.; Dixon, R.; Osborne, R.H.; Chapa, O.; Stringer, D. Exploring health literacy profiles of Texas university students. Health Behav. Policy Rev. 2016, 3, 209–225. [Google Scholar] [CrossRef]
- Elsborg, L.; Krossdal, F.; Kayser, L. Health literacy among Danish university students enrolled in health-related study programmes. Scand. J. Public Health 2017, 45, 831–838. [Google Scholar] [CrossRef]
- Mather, C.; Douglas, T.; Angela Jacques, A. Health literacy of undergraduate health profession students in Australia: A comparison of the island state of Tasmania and other Australian universities. Kontakt 2018, 20, e386–e393. [Google Scholar] [CrossRef] [Green Version]
- Bröder, J.; Chang, P.; Kickbusch, I.; Levin-Zamir, D.; McElhinney, E.; Nutbeam, D.; Okan, O.; Osborne, R.; Pelikan, J.; Rootman, I.; et al. IUHPE Position Statement on Health Literacy: A practical vision for a health literate world. Glob. Health Promot. 2018, 25, 79–88. [Google Scholar] [CrossRef]
- Mosley, C.M.; Taylor, B.J. Integration of Health Literacy Content Into Nursing Curriculum Utilizing the Health Literacy Expanded Model. Teach. Learn. Nurs. 2017, 12, 109–116. [Google Scholar] [CrossRef]
- Ayaz-Alkaya, S.; Terzi, H. Investigation of health literacy and affecting factors of nursing students. Nurse Educ. Pract. 2019, 34, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Bröder, J.; Okan, O.; Bauer, U.; Schlupp, S.; Pinheiro, P. Advancing perspectives on health literacy in childhood and youth. Health Promot. Int. 2019. pii:daz041. [Google Scholar] [CrossRef]

{kind=link}
| Item HLS-EU-Q16 | Total Sample N: 219 | Nursing Students N: 52 | Social Work Students N: 141 | Primary Education Students N: 13 | Special Education Students N:13 | p | |
|---|---|---|---|---|---|---|---|
| 1 | —find information on treatments or illnesses that concern you? | 2.9 (0.6) | 3.1 (0.5) | 2.9 (0.6) | 2.6 (0.8) | 2.6 (0.7) | 0.004 |
| 2 | —find out where to get professional help when you are ill? | 3.1 (0.6) | 3.2 (0.6) | 3.1 (0.6) | 3 (0.9) | 2.8 (0.5) | 0.179 |
| 3 | —understand what the doctor says to you? | 2.8 (0.7) | 3.2 (0.6) | 2.7 (0.7) | 3 (0.5) | 3 (0.6) | 0.000 |
| 4 | —understand your doctor’s or pharmacist’s instructions on how to take a prescribed medicine? | 3.2 (0.6) | 3.4 (0.5) | 3 (0.6) | 3.5 (0.5) | 3.1 (0.6) | 0.002 |
| 5 | —judge when you need to get a second opinion from your doctor? | 2.4 (0.8) | 2.7 (0.7) | 2.3 (0.7) | 2.2 (1) | 2 (0.8) | 0.002 |
| 6 | —use information the doctor gives you to make decisions about your illness? | 2.7 (0.7) | 2.9 (0.6) | 2.6 (0.7) | 2.2 (0.6) | 2.5 (0.4) | 0.003 |
| 7 | —follow instructions from your doctor or pharmacist? | 3.1 (0.6) | 3.4 (0.5) | 3.1 (0.6) | 3.1 (0.6) | 3 (0.7) | 0.031 |
| 8 | —find information on how to manage mental health problems like stress or depression? | 2.4 (0.8) | 2.6 (0.8) | 2.3 (0.8) | 1.8 (0.6) | 2.3 (0.7) | 0.012 |
| 9 | —understand health warnings about behaviour such as smoking, low physical activity and drinking too much? | 3.2 (0.6) | 3.4 (0.5) | 3.1 (0.6) | 3 (0.8) | 3.3 (0.4) | 0.013 |
| 10 | —understand why you need health screenings? | 3.1 (0.6) | 3.2 (0.6) | 3.1 (0.6) | 3 (0.6) | 3.4 (0.5) | 0.123 |
| 11 | —judge if the information on health risks in the media is reliable? | 2.4 (0.7) | 2.7 (0.5) | 2.4 (0.7) | 2 (0.7) | 1.8 (0.5) | 0.000 |
| 12 | —decide how you can protect yourself from illness based on information in the media? | 2.5 (0.7) | 2.8 (0.6) | 2.4 (0.7) | 2.2 (0.7) | 2.4 (0.7) | 0.007 |
| 13 | —find out what activities are good for your mental well-being? | 2.6 (0.8) | 2.7 (0.8) | 2.4 (0.8) | 3 (0.7) | 2.9 (0.6) | 0.022 |
| 14 | —understand advice on health from family members or friends | 2.9 (0.6) | 3.2 (0.6) | 2.8 (0.6) | 3.2 (0.7) | 2.6 (0.4) | 0.000 |
| 15 | —understand information in the media on how to get healthier? | 2.8 (0.7) | 3 (0.6) | 2.8 (0.7) | 2.6 (0.6) | 2.6 (0.6) | 0.062 |
| 16 | —judge which everyday behaviour is related to your health? | 2.9 (0.7) | 3.2 (0.6) | 2.8 (0.7) | 2.8 (0.8) | 2.6 (0.7) | 0.002 |
| Total Sample N: 219 | Nursing Students N: 52 | Social Work Students N: 141 | Primary Education Students N:13 | Special Education Students N:13 | p | |
|---|---|---|---|---|---|---|
| Health care (HL-1, HL-2, HL-3, HL-4, HL-5, HL-6, HL-7) | 2.9 (0.4) | 3.1 (0.4) | 2.8 (0.4) | 2.8 (0.4) | 2.7 (0.3) | 0.000 |
| Disease prevention (HL-8, HL-9, HL-10, HL-11, HL-12) | 2.7 (0.4) | 3 (0.4) | 2.7 (0.4) | 2.4 (0.4) | 2.6 (0.3) | 0.000 |
| Health promotion (HL-13, HL-14, HL-15, HL-16) | 2.8 (0.5) | 3 (0.5) | 2.7 (0.5) | 2.9 (0.4) | 2.7 (0.3) | 0.001 |
| B | Standard Error | Wald | Sig. | OR | CI 95% OR | ||
|---|---|---|---|---|---|---|---|
| Lower | Higher | ||||||
| Age | 0.029 | 0.031 | 0.879 | 0.348 | 1.030 | 0.968 | 1.095 |
| Sex (Male) | 0.283 | 0.430 | 0.435 | 0.509 | 1.328 | 0.572 | 3.081 |
| University Studies (Nursing) | 30.159 | 0.000 | |||||
| University Studies (Social Work) | −1.858 | 0.361 | 26.494 | 0.000 | 0.156 | 0.077 | 0.316 |
| University Studies (Primary Education) | −2.307 | 0.783 | 8.683 | 0.003 | 0.100 | 0.021 | 0.462 |
| University Studies (Special Education) | −2.965 | 0.929 | 10.197 | 0.001 | 0.052 | 0.008 | 0.318 |
| Second Degree (No) | −1.659 | 0.844 | 3.868 | 0.049 | 0.190 | 0.036 | 0.994 |
| Constant | 1.716 | 1.102 | 2.425 | 0.119 | 5.561 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juvinyà-Canal, D.; Suñer-Soler, R.; Boixadós Porquet, A.; Vernay, M.; Blanchard, H.; Bertran-Noguer, C. Health Literacy among Health and Social Care University Students. Int. J. Environ. Res. Public Health 2020, 17, 2273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072273
Juvinyà-Canal D, Suñer-Soler R, Boixadós Porquet A, Vernay M, Blanchard H, Bertran-Noguer C. Health Literacy among Health and Social Care University Students. International Journal of Environmental Research and Public Health. 2020; 17(7):2273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072273
Chicago/Turabian StyleJuvinyà-Canal, Dolors, Rosa Suñer-Soler, Adela Boixadós Porquet, Marion Vernay, Hervé Blanchard, and Carme Bertran-Noguer. 2020. "Health Literacy among Health and Social Care University Students" International Journal of Environmental Research and Public Health 17, no. 7: 2273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072273