Effects of Double-Taped Kinesio Taping on Pain and Functional Performance due to Muscle Fatigue in Young Males: A Randomized Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants
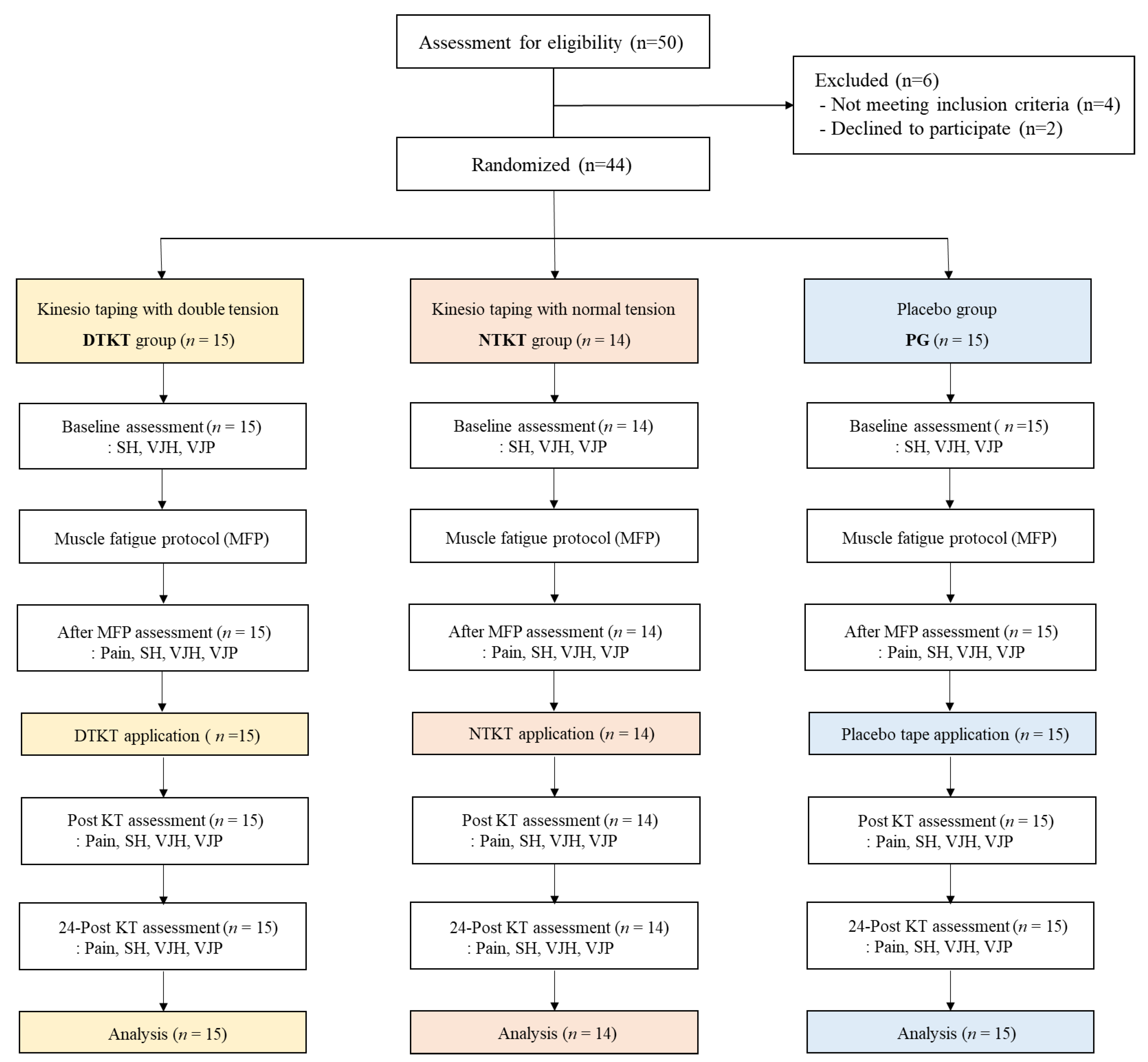
2.3. Procedure
2.4. Muscle Fatigue Protocol
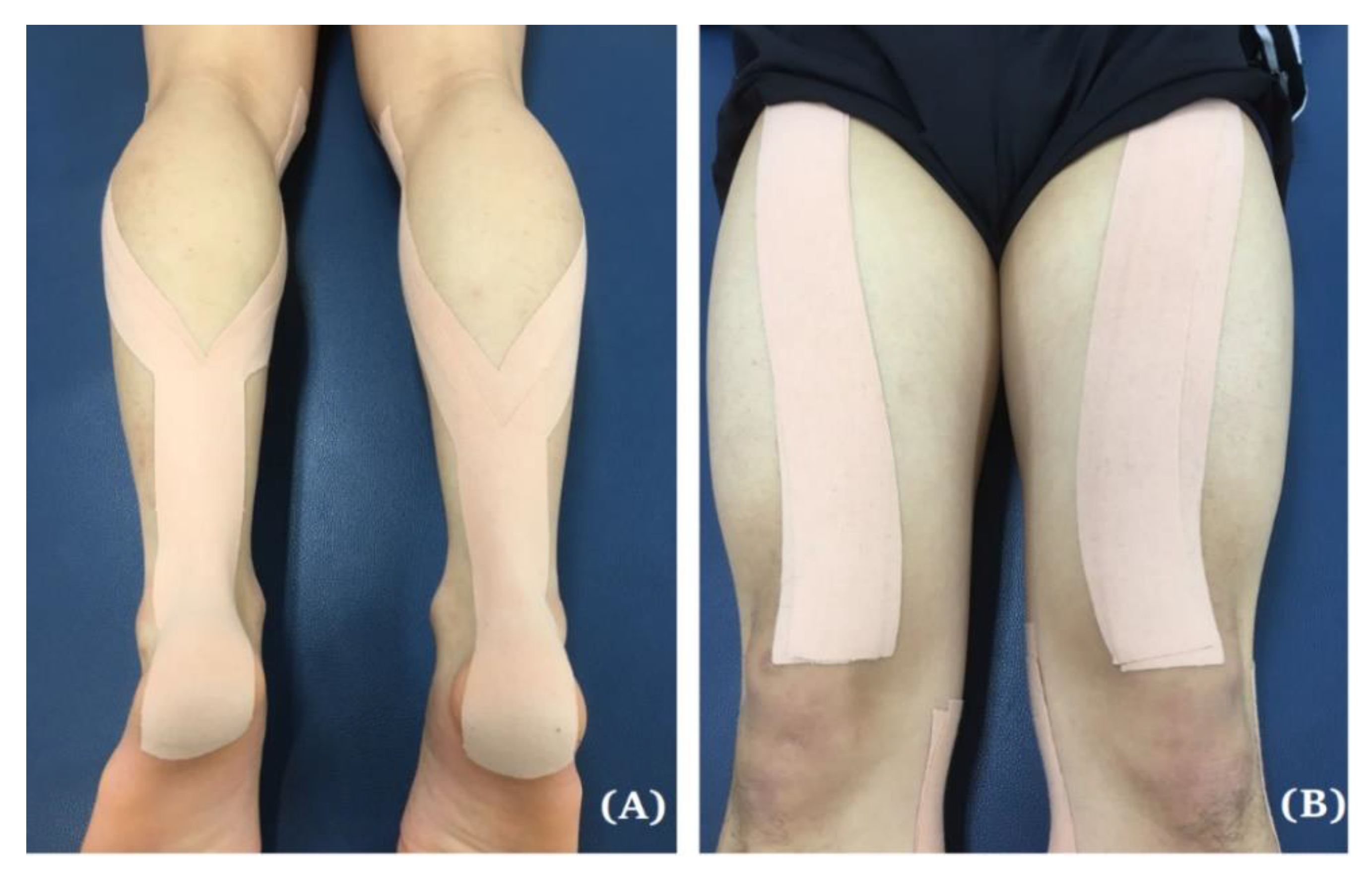
2.5. Intervention (Applying Kinesio Taping)
2.6. Outcome Measures
2.7. Statistical Analysis
3. Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gonzalez-Iglesias, J.; Fernandez-de-Las-Penas, C.; Cleland, J.A.; Huijbregts, P.; Del Rosario Gutierrez-Vega, M. Short-term effects of cervical kinesio taping on pain and cervical range of motion in patients with acute whiplash injury: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2009, 39, 515–521. [Google Scholar] [CrossRef]
- Yoshida, A.; Kahanov, L. The effect of kinesio taping on lower trunk range of motions. Res. Sports Med. 2007, 15, 103–112. [Google Scholar] [CrossRef]
- Thelen, M.D.; Dauber, J.A.; Stoneman, P.D. The clinical efficacy of kinesio tape for shoulder pain: A randomized, double-blinded, clinical trial. J. Orthop. Sports Phys. Ther. 2008, 38, 389–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, Y.H.; Chen, W.Y.; Lin, H.C.; Wang, W.T.; Shih, Y.F. The effects of taping on scapular kinematics and muscle performance in baseball players with shoulder impingement syndrome. J. Electromyogr. Kinesiol. 2009, 19, 1092–1099. [Google Scholar] [CrossRef] [PubMed]
- Slupik, A.; Dwornik, M.; Bialoszewski, D.; Zych, E. Effect of Kinesio Taping on bioelectrical activity of vastus medialis muscle. Preliminary report. Ortop. Traumatol. Rehabil. 2007, 9, 644–651. [Google Scholar] [PubMed]
- Wong, O.M.; Cheung, R.T.; Li, R.C. Isokinetic knee function in healthy subjects with and without Kinesio taping. Phys. Ther. Sport 2012, 13, 255–258. [Google Scholar] [CrossRef]
- Simon, J.; Garcia, W.; Docherty, C.L. The effect of kinesio tape on force sense in people with functional ankle instability. Clin. J. Sport Med. 2014, 24, 289–294. [Google Scholar] [CrossRef]
- Jaraczewska, E.; Long, C. Kinesio taping in stroke: Improving functional use of the upper extremity in hemiplegia. Top. Stroke Rehabilit. 2006, 13, 31–42. [Google Scholar] [CrossRef] [Green Version]
- Yasukawa, A.; Patel, P.; Sisung, C. Pilot study: Investigating the effects of Kinesio Taping in an acute pediatric rehabilitation setting. Am. Occup. Ther. 2006, 60, 104–110. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.Y.; Chou, K.Y.; Lin, J.J.; Lin, C.F.; Wang, C.H. Immediate effect of forearm Kinesio taping on maximal grip strength and force sense in healthy collegiate athletes. Phys. Ther. Sport 2010, 11, 122–127. [Google Scholar] [CrossRef]
- Vanezis, A.; Lees, A. A biomechanical analysis of good and poor performers of the vertical jump. Ergonomics 2005, 48, 1594–1603. [Google Scholar] [CrossRef] [PubMed]
- Bobbert, M.F.; Gerritsen, K.G.; Litjens, M.C.; Van Soest, A.J. Why is countermovement jump height greater than squat jump height? Med. Sci. Sports Exerc. 1996, 28, 1402–1412. [Google Scholar] [CrossRef]
- Huang, C.Y.; Hsieh, T.H.; Lu, S.C.; Su, F.C. Effect of the Kinesio tape to muscle activity and vertical jump performance in healthy inactive people. Biomed. Eng. Online 2011, 10, 70. [Google Scholar] [CrossRef] [Green Version]
- Magalhaes, I.; Bottaro, M.; Freitas, J.R.; Carmo, J.; Matheus, J.P.; Carregaro, R.L. Prolonged use of Kinesiotaping does not enhance functional performance and joint proprioception in healthy young males: Randomized controlled trial. Braz. J. Phys. Ther. 2016, 20, 213–222. [Google Scholar] [CrossRef] [Green Version]
- Lees, A.; Vanrenterghem, J.; De Clercq, D. The maximal and submaximal vertical jump: Implications for strength and conditioning. J. Strength Cond. Res. 2004, 18, 787–791. [Google Scholar] [CrossRef]
- AragonVargas, L.F.; Gross, M.M. Kinesiological factors in vertical jump performance: Differences among individuals. J. Appl. Biomech. 1997, 13, 24–44. [Google Scholar] [CrossRef]
- Stedge, H.L.; Kroskie, R.M.; Docherty, C.L. Kinesio taping and the circulation and endurance ratio of the gastrocnemius muscle. J. Athl. Train. 2012, 47, 635–642. [Google Scholar] [CrossRef]
- Cai, C.; Au, I.P.; An, W.; Cheung, R.T. Facilitatory and inhibitory effects of Kinesio tape: Fact or fad? J. Sci. Med. Sport 2016, 19, 109–112. [Google Scholar] [CrossRef]
- Martinez-Gramage, J.; Merino-Ramirez, M.A.; Amer-Cuenca, J.J.; Lison, J.F. Effect of Kinesio Taping on gastrocnemius activity and ankle range of movement during gait in healthy adults: A randomized controlled trial. Phys. Ther. Sport 2016, 18, 56–61. [Google Scholar] [CrossRef]
- Williams, S.; Whatman, C.; Hume, P.A.; Sheerin, K. Kinesio taping in treatment and prevention of sports injuries: A meta-analysis of the evidence for its effectiveness. Sports Med. 2012, 42, 153–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, R.T.; Yau, Q.K.; Wong, K.; Lau, P.; So, A.; Chan, N.; Kwok, C.; Poon, K.Y.; Yung, P.S. Kinesiology tape does not promote vertical jumping performance: A deceptive crossover trial. Man Ther. 2016, 21, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Mendez-Rebolledo, G.; Ramirez-Campillo, R.; Guzman-Munoz, E.; Gatica-Rojas, V.; Dabanch-Santis, A.; Diaz-Valenzuela, F. Short-term effects of Kinesio Taping on muscle recruitment order during a vertical jump: A pilot study. J. Sport Rehabil. 2018, 27, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, M.A.; Baldridge, C. The effect of Kinesio(R) Tape on vertical jump and dynamic postural control. Int. J. Sports Phys. Ther. 2013, 8, 393–406. [Google Scholar] [PubMed]
- Callaghan, M.J.; Selfe, J.; McHenry, A.; Oldham, J.A. Effects of patellar taping on knee joint proprioception in patients with patellofemoral pain syndrome. Man Ther. 2008, 13, 192–199. [Google Scholar] [CrossRef]
- Macedo, L.B.; Richards, J.; Borges, D.T.; Melo, S.A.; Brasileiro, J.S. Kinesio Taping reduces pain and improves disability in low back pain patients: A randomised controlled trial. Physiotherapy 2018. [Google Scholar] [CrossRef] [Green Version]
- Perlau, R.; Frank, C.; Fick, G. The effect of elastic bandages on human knee proprioception in the uninjured population. Am. J. Sports Med. 1995, 23, 251–255. [Google Scholar] [CrossRef]
- Long, Z.; Wang, R.W.; Han, J.; Waddington, G.; Adams, R.; Anson, J. Optimizing ankle performance when taped: Effects of kinesiology and athletic taping on proprioception in full weight-bearing stance. J. Sci. Med. Sport 2017, 20, 236–240. [Google Scholar] [CrossRef]
- De Jesus, J.F.; Franco, Y.R.; Nannini, S.B.; Nakaoka, G.B.; Dos Reis, A.C.; Bryk, F.F. The effects of varied tensions of kinesiology taping on quadriceps strength and lower limb function. Int. J. Sports Phys. Ther. 2017, 12, 85–93. [Google Scholar]
- Lessi, G.C.; Dos Santos, A.F.; Batista, L.F.; de Oliveira, G.C.; Serrao, F.V. Effects of fatigue on lower limb, pelvis and trunk kinematics and muscle activation: Gender differences. J. Electromyogr. Kinesiol. 2017, 32, 9–14. [Google Scholar] [CrossRef]
- Gervasio, S.; Finocchietti, S.; Stevenson, A.J.T.; Mrachacz-Kersting, N. Delayed muscle onset soreness in the gastrocnemius muscle attenuates the spinal contribution to interlimb communication. Eur. J. Appl. Physiol. 2018, 118, 2393–2402. [Google Scholar] [CrossRef]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work Environ. Health 1990, 16 (Suppl. 1), 55–58. [Google Scholar] [CrossRef] [PubMed]
- Zanca, G.G.; Gruninger, B.; Mattiello, S.M. Effects of Kinesio taping on scapular kinematics of overhead athletes following muscle fatigue. J. Electromyogr. Kinesiol. 2016, 29, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Fuller, J.R.; Lomond, K.V.; Fung, J.; Cote, J.N. Posture-movement changes following repetitive motion-induced shoulder muscle fatigue. J. Electromyogr. Kinesiol. 2009, 19, 1043–1052. [Google Scholar] [CrossRef] [PubMed]
- Kase, K.; Wallis, J.; Kase, T. Clinical therapeutic applications of the Kinesio Taping Method, 3rd ed.; Kinesio Taping Association: Tokyo, Japan, 2003; p. 249. [Google Scholar]
- Jensen, M.P.; Karoly, P.; Braver, S. The measurement of clinical pain intensity: A comparison of six methods. Pain 1986, 27, 117–126. [Google Scholar] [CrossRef]
- Carlsson, A.M. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain 1983, 16, 87–101. [Google Scholar] [CrossRef]
- Ross, M.D.; Langford, B.; Whelan, P.J. Test-retest reliability of 4 single-leg horizontal hop tests. J. Strength Cond. Res. 2002, 16, 617–622. [Google Scholar]
- Petschnig, R.; Baron, R.; Albrecht, M. The relationship between isokinetic quadriceps strength test and hop tests for distance and one-legged vertical jump test following anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 1998, 28, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Tenelsen, F.; Brueckner, D.; Muehlbauer, T.; Hagen, M. Validity and reliability of an electronic contact mat for drop jump assessment in physically active adults. Sports 2019, 7, 114. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, D.S.A.; Pellitero, L.; Ferrer-Roca, V. Validation of the photoelectric optogait system to measure racewalking biomechanical parameters on a treadmill. ISBS Proc. 2017, 35, 253. [Google Scholar]
- OPTOGAIT User Manual. 2010. Available online: http://www.optogait.com/OptoGaitPortal/Media/Manuals/Manual-EN.PDF (accessed on 26 March 2020).
- Maratou, E.; Theophilidis, G. An axon pacemaker: Diversity in the mechanism of generation and conduction of action potentials in snail neurons. Neuroscience 2000, 96, 1–2. [Google Scholar] [CrossRef]
- Konishi, Y. Tactile stimulation with kinesiology tape alleviates muscle weakness attributable to attenuation of Ia afferents. J. Sci. Med. Sport 2013, 16, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Fu, W.; Pan, J.; Wang, L.; Xia, R.; Liu, Y. Acute effects of Kinesio taping on muscle strength and fatigue in the forearm of tennis players. J. Sci. Med. Sport 2016, 19, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Fernandes de Jesus, J.; de Almeida Novello, A.; Bezerra Nakaoka, G.; Curcio Dos Reis, A.; Fukuda, T.Y.; Fernandes Bryk, F. Kinesio taping effect on quadriceps strength and lower limb function of healthy individuals: A blinded, controlled, randomized, clinical trial. Phys. Ther. Sport 2016, 18, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Al-Shareef, A.T.; Omar, M.T.; Ibrahim, A.H. Effect of kinesio taping on pain and functional disability in chronic nonspecific low back pain: A randomized clinical trial. Spine 2016, 41, E821–E828. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| DTKT (n = 15) | NTKT (n = 14) | PG (n = 15) | p Values | |
|---|---|---|---|---|
| Age (years) | 23.2 ± 2.0 | 23.2 ± 2.7 | 23.4 ± 2.1 | 0.98 |
| Height (cm) | 172.9 ± 4.3 | 171.6 ± 7.6 | 174.3 ± 4.5 | 0.45 |
| Weight (kg) | 69.6 ± 8.4 | 69.6 ± 12.7 | 69.5 ± 8.2 | 0.99 |
| BMI (kg/m2) | 23.2 ± 2.4 | 23.6 ± 3.2 | 22.9 ± 2.4 | 0.80 |
| Baseline SH distance (cm) | 173.1 ± 16.1 | 178.6 ± 13.3 | 180.5 ± 15.0 | 0.40 |
| Baseline VJH (cm) | 31.5 ± 4.7 | 30.3 ± 5.4 | 33.7 ± 6.1 | 0.30 |
| Baseline VJP (w/kg) | 15.4 ± 2.5 | 15.9 ± 3.6 | 15.7 ± 2.5 | 0.97 |
| DTKT (n = 15) | NTKT (n = 14) | PG (n = 15) | F 1 | P 1 | η2 1 | ||
|---|---|---|---|---|---|---|---|
| Pain | After MFP | 3.5 ± 1.9 | 3.5 ± 2.9 | 2.3 ± 1.8 | 0.54 | 0.67 | 0.03 |
| Post | 2.5 ± 1.6 * | 2.9 ± 1.8 | 2.1 ± 1.9 | ||||
| 24-post | 3.3 ± 2.4 | 3.0 ± 2.3 | 2.2 ± 2.2 |
| DTKT (n = 15) | NTKT (n = 14) | PG (n = 15) | F 1 | P 1 | η21 | ||
|---|---|---|---|---|---|---|---|
| SH distance (cm) | Baseline | 173.1 ± 16.1 | 178.6 ± 13.3 | 180.5 ± 15.0 | |||
| After MFP | 163.9 ± 20.0 * | 165.0 ± 20.7 * | 170.3 ± 22.3 * | 0.32 | 0.86 | 0.02 | |
| Post KT | 168.2 ± 15.6 | 165.9 ± 21.4 | 170.8 ± 23.9 | ||||
| 24-post KT | 168.6 ± 14.1 | 166.3 ± 20.7 | 172.2 ± 23.1 | ||||
| VJH (cm) | Baseline | 31.5 ± 4.7 | 30.3 ± 5.4 | 33.7 ± 6.1 | |||
| After MFP | 29.1 ± 4.6 * | 26.2 ± 5.5 * | 29.8 ± 7.3 * | 1.55 | 0.20 | 0.07 | |
| Post KT | 28.6 ± 3.7 | 26.9 ± 6.7 | 30.9 ± 6.8 | ||||
| 24-post KT | 29.8 ± 4.2 | 27.3 ± 6.3 | 29.4 ± 8.5 | ||||
| VJP (w/kg) | Baseline | 15.4 ± 2.5 | 15.9 ± 3.6 | 15.7 ± 2.5 | |||
| After MFP | 14.4 ± 1.0 * | 13.8 ± 2.8 * | 14.7 ± 2.3 * | 0.86 | 0.45 | 0.04 | |
| Post KT | 14.3 ± 1.0 | 14.2 ± 3.7 | 14.8 ± 2.4 | ||||
| 24-post KT | 15.9 ± 1.2 | 14.9 ± 4.2 | 14.7 ± 3.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Lim, H. Effects of Double-Taped Kinesio Taping on Pain and Functional Performance due to Muscle Fatigue in Young Males: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 2364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072364
Lee H, Lim H. Effects of Double-Taped Kinesio Taping on Pain and Functional Performance due to Muscle Fatigue in Young Males: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(7):2364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072364
Chicago/Turabian StyleLee, Haneul, and Hyoungwon Lim. 2020. "Effects of Double-Taped Kinesio Taping on Pain and Functional Performance due to Muscle Fatigue in Young Males: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 7: 2364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072364