Infant Motor Milestones and Childhood Overweight: Trends over Two Decades in A Large Twin Cohort

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
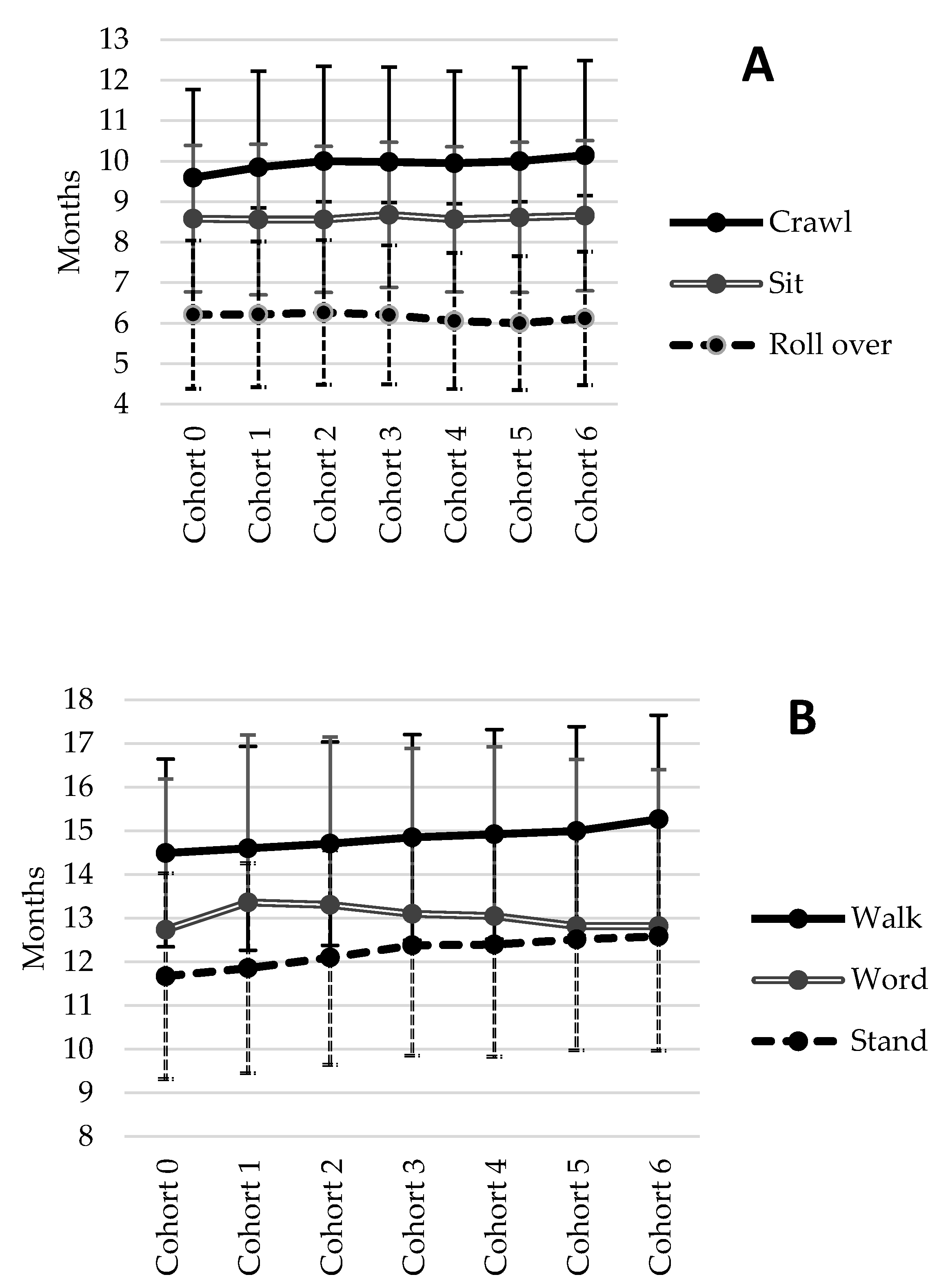
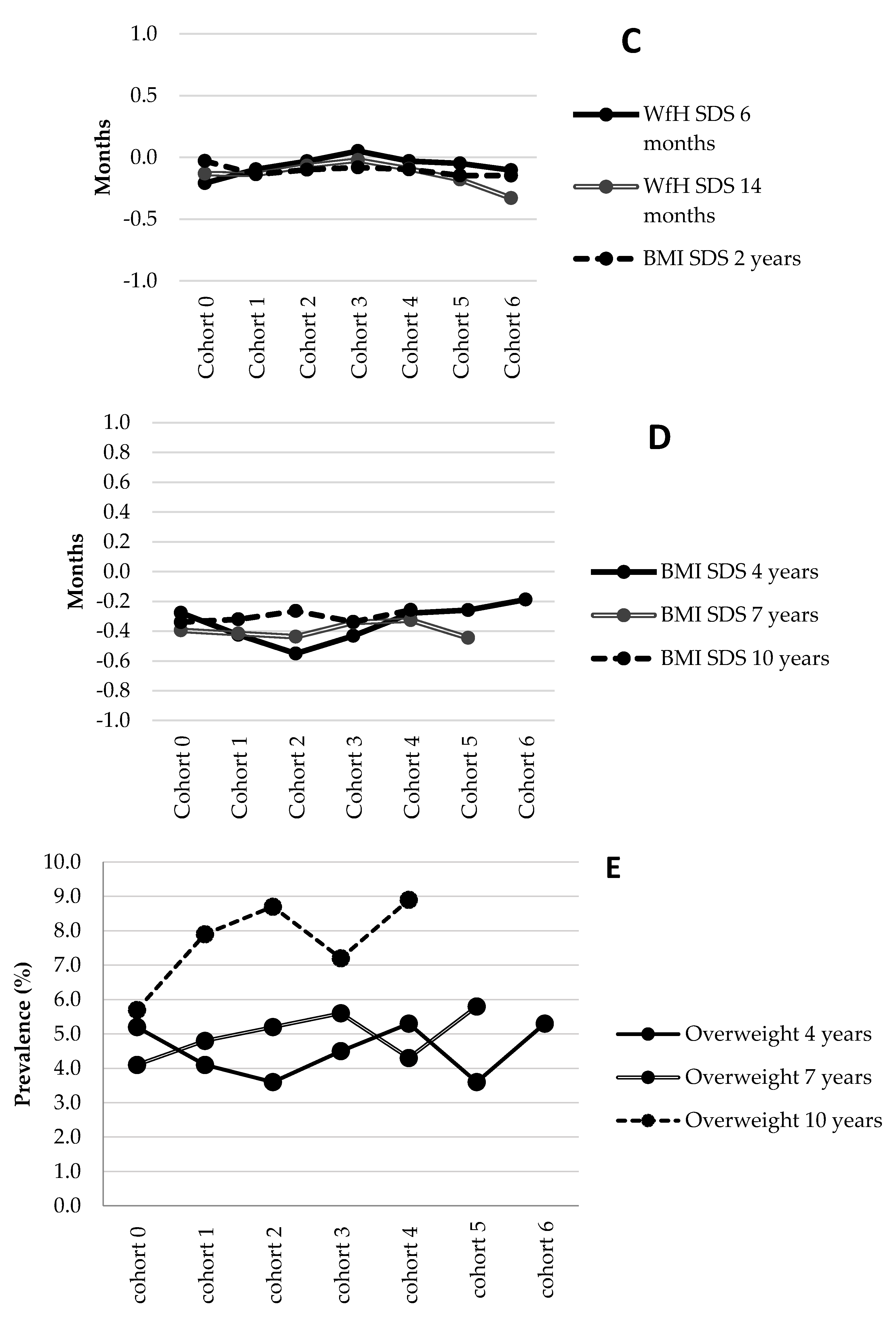
3.1. Cohort Effects
3.2. Association between BW and Early Weight-for-Length and Motor Milestone Achievement
3.3. Association between Motor Milestone Achievement and Childhood Overweight at Age 2, 4, 7, and 10 Years
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- De Onis, M.; Blossner, M.; Borghi, E. Global prevalence and trends of overweight and obesity among preschool children. Am. J. Clin. Nutr. 2010, 92, 1257–1264. [Google Scholar] [CrossRef] [Green Version]
- Herman, K.M.; Craig, C.L.; Gauvin, L.; Katzmarzyk, P.T. Tracking of obesity and physical activity from childhood to adulthood: The Physical Activity Longitudinal Study. Pediatrics Obes. 2009, 4, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.J.; Lagerpusch, M.; Enderle, J.; Schautz, B.; Heller, M.; Bosy-Westphal, A. Beyond the body mass index: Tracking body composition in the pathogenesis of obesity and the metabolic syndrome. Obes. Rev. 2012, 13, 6–13. [Google Scholar] [CrossRef]
- Weiss, R.; Dziura, J.; Burgert, T.S.; Tamborlane, W.V.; Taksali, S.E.; Yeckel, C.W.; Allen, K.; Lopes, M.; Savoye, M.; Morrison, J.; et al. Obesity and the metabolic syndrome in children and adolescents. N. Engl. J. Med. 2004, 350, 2362–2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stodden, D.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; García, L.E. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Barnett, L.M.; Lai, S.K.; Veldman, S.L.C.; Hardy, L.L.; Cliff, D.P.; Morgan, P.J.; Zask, A.; Lubans, D.R.; Shultz, S.P.; Ridgers, N.D.; et al. Correlates of Gross Motor Competence in Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2016, 46, 1663–1688. [Google Scholar] [CrossRef] [Green Version]
- Roth, K.; Ruf, K.; Obinger, M.; Mauer, S.; Ahnert, J.; Schneider, W.; Graf, C.; Hebestreit, H. Is there a secular decline in motor skills in preschool children? Scand. J. Med. Sci. Sports 2010, 20, 670–678. [Google Scholar] [CrossRef]
- Runhaar, J.; Collard, D.; Singh, A.; Kemper, H.; Van Mechelen, W.; Chinapaw, M. Motor fitness in Dutch youth: Differences over a 26-year period (1980–2006). J. Sci. Med. Sport 2010, 13, 323–328. [Google Scholar] [CrossRef]
- Brouwer, S.I.; van Beijsterveldt, T.C.; Bartels, M.; Hudziak, J.J.; Boomsma, D.I. Influences on achieving motor milestones: A twin-singleton study. Twin. Res. Hum. Genet. 2006, 9, 424–430. [Google Scholar] [CrossRef]
- Monterosso, L.; Kristjanson, L.; Cole, J. Neuromotor development and the physiologic effects of positioning in very low birth weight infants. J. Obstet. Gynecol. Neonatal. Nurs. 2002, 31, 138–146. [Google Scholar] [CrossRef]
- Duch, H.; Fisher, E.M.; Ensari, I.; Harrington, A. Screen time use in children under 3 years old: A systematic review of correlates. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 102. [Google Scholar] [CrossRef] [Green Version]
- Garrett, M.; McElroy, A.M.; Staines, A. Locomotor milestones and babywalkers: Cross sectional study. BMJ 2002, 324, 1494. [Google Scholar] [CrossRef] [Green Version]
- Shibli, R.; Rubin, L.; Akons, H.; Shaoul, R. Morbidity of Overweight (>=85th Percentile) in the First 2 Years of Life. Pediatrics 2008, 122, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, M.; Kosakov, C. The Motor Development of Fat Babies. Clin. Pediatrics 1982, 21, 619–621. [Google Scholar] [CrossRef] [PubMed]
- Martins, D.; Maia, J.; Seabra, A.; Garganta, R.; Lopes, V.P.; Katzmarzyk, P.T.; Beunen, G. Correlates of changes in BMI of children from the Azores islands. Int. J. Obes. 2010, 34, 1487–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, V.P.; Stodden, D.; Bianchi, M.M.; Maia, J.; Rodrigues, L.P. Correlation between BMI and motor coordination in children. J. Sci. Med. Sport 2012, 15, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Ridgway, C.; Ong, K.K.; Tammelin, T.H.; Sharp, S.; Ekelund, U.; Jarvelin, M.-R. Infant Motor Development Predicts Sports Participation at Age 14 Years: Northern Finland Birth Cohort of 1966. PLoS ONE 2009, 4, e6837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgen, C.S.; Due, P.; Neelon, S.B.; Gamborg, M.; Sørensen, T.I.A.; Andersen, A.-M.N. Timing of motor milestones achievement and development of overweight in childhood: A study within the Danish National Birth Cohort. Pediatrics Obes. 2013, 9, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Slining, M.; Adair, L.S.; Goldman, B.D.; Borja, J.B.; Bentley, M. Infant Overweight Is Associated with Delayed Motor Development. J. Pediatrics 2010, 157, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Neelon, S.E.B.; Oken, E.; Taveras, E.M.; Rifas-Shiman, S.L.; Gillman, M.W. Age of achievement of gross motor milestones in infancy and adiposity at age 3 years. Matern. Child Heal. J. 2012, 16, 1015–1020. [Google Scholar] [CrossRef] [Green Version]
- van Beijsterveldt, C.E.; Groen-Blokhuis, M.; Hottenga, J.J.; Franic, S.; Hudziak, J.J.; Lamb, D.; Huppertz, C.; de Zeeuw, E.; Nivard, M.; Schutte, N.; et al. The Young Netherlands Twin Register (YNTR): Longitudinal twin and family studies in over 70,000 children. Twin. Res. Hum. Genet. 2013, 16, 252–267. [Google Scholar] [CrossRef] [Green Version]
- Langendonk, J.M.; Van Beijsterveldt, C.E.M.; Brouwer, S.I.; Stroet, T.; Hudziak, J.J.; Boomsma, R.I. Assessment of Motor Milestones in Twins. Twin Res. Hum. Genet. 2007, 10, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, I.; Boomsma, R.I.; Berg, S.M.V.D. Mathematical Ability and Socio-Economic Background: IRT Modeling to Estimate Genotype by Environment Interaction. Twin Res. Hum. Genet. 2017, 20, 511–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fredriks, A.M.; Van Buuren, S.; Burgmeijer, R.J.F.; Meulmeester, J.F.; Beuker, R.J.; Brugman, E.; Roede, M.J.; Verloove-Vanhorick, S.P.; Wit, J.-M. Continuing Positive Secular Growth Change in the Netherlands 1955–1997. Pediatrics Res. 2000, 47, 316–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatrics Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Gielen, M.; Van Beijsterveldt, C.; Derom, C.; Vlietinck, R.; Nijhuis, J.G.; Zeegers, M.P.; I Boomsma, D. Secular trends in gestational age and birthweight in twins. Hum. Reprod. 2010, 25, 2346–2353. [Google Scholar] [CrossRef] [Green Version]
- Darrah, J.; Bartlett, D.J. Infant rolling abilities—The same or different 20years after the back to sleep campaign? Early Hum. Dev. 2013, 89, 311–314. [Google Scholar] [CrossRef]
- Darrah, J.; Bartlett, D.; Maguire, T.O.; Avison, W.R.; Lacaze-Masmonteil, T. Have infant gross motor abilities changed in 20 years? A re-evaluation of the Alberta Infant Motor Scale normative values. Dev. Med. Child. Neurol. 2014, 56, 877–881. [Google Scholar] [CrossRef] [Green Version]
- Jeng, S.-F.; Yau, K.-I.T.; Chen, L.-C.; Hsiao, S.-F. Alberta Infant Motor Scale: Reliability and Validity When Used on Preterm Infants in Taiwan. Phys. Ther. 2000, 80, 168–178. [Google Scholar] [CrossRef]
- Allen, M.C.; Alexander, G.R. Gross motor milestones in preterm infants: correction for degree of prematurity. J. Pediatrics 1990, 116, 955–959. [Google Scholar] [CrossRef]
- Lima, R.A.; Bugge, A.; Pfeiffer, K.A.; Andersen, L.B. Tracking of Gross Motor Coordination From Childhood Into Adolescence. Res. Q. Exerc. Sport 2017, 88, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dewey, C.; Fleming, P.J.; Golding, J.; the ALSPAC Study Team. Does the Supine Sleeping Position Have Any Adverse Effects on the Child? II. Development in the First 18 Months. Pediatrics 1998, 101, e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lung, F.W.; Shu, B.C. Sleeping position and health status of children at six-, eighteen- and thirty-six-month development. Res. Dev. Disabil. 2011, 32, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Siegel, A.C.; Burton, R.V. Effects of baby walkers on motor and mental development in human infants. J. Dev. Behav. Pediatrics 1999, 20, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Who Multicentre Growth Reference Study Group; de Onis, M. Relationship between physical growth and motor development in the WHO Child Growth Standards. Acta Pædiatrica 2006, 95, 96–101. [Google Scholar]
- D’Hondt, E.; Gentier, I.; Deforche, B.; Tanghe, A.; De Bourdeaudhuij, I.; Lenoir, M. Weight Loss and Improved Gross Motor Coordination in Children as a Result of Multidisciplinary Residential Obesity Treatment. Obesity 2011, 19, 1999–2005. [Google Scholar] [CrossRef]
- Nervik, D.; Martin, K.; Rundquist, P.; Cleland, J. The Relationship Between Body Mass Index and Gross Motor Development in Children Aged 3 to 5 Years. Pediatrics Phys. Ther. 2011, 23, 144–148. [Google Scholar] [CrossRef] [Green Version]
- Mond, J.M.; Stich, H.; Hay, P.; Kraemer, A.; Baune, B.T. Associations between obesity and developmental functioning in pre-school children: A population-based study. Int. J. Obes. 2007, 31, 1068–1073. [Google Scholar] [CrossRef] [Green Version]
- Lara-Pompa, N.; Williams, J.; Macdonald, S.; Valente, J.; Wells, J.; Hill, S.; Fewtrell, M. MON-PP254: Measuring Body Composition in Hospitalized Children: Validity, Practicality and Acceptability of Different Methods. Clin. Nutr. 2015, 34, S221. [Google Scholar] [CrossRef]
- Available online: http://www.cbs.nl/nl-NL/menu/themas/bevolking/publicaties/artikelen/archief/2007/2007-90090-wk.htm (accessed on 29 March 2020).
- Ahrens, W.; Pigeot, I.; Pohlabeln, H.; De Henauw, S.; Lissner, L.; Molnár, D.; Moreno, L.A.; Tornaritis, M.; Veidebaum, T.; Siani, A. Prevalence of overweight and obesity in European children below the age of 10. Int. J. Obes. 2014, 38, S99–S107. [Google Scholar] [CrossRef] [Green Version]
- Van Dommelen, P.; De Gunst, M.; Van Der Vaart, A.; Van Buuren, S.; Boomsma, R. Growth references for height, weight and body mass index of twins aged 02.5 years. Acta Paediatrics 2008, 97, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Estourgie-van Burk, G.F.; Bartels, M.; Boomsma, D.I.; Delemarre-van de Waal, H.A. Body size of twins compared with siblings and the general population: From birth to late adolescence. J. Pediatrics 2010, 156, 586–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doom, E.; Delbaere, I.; Martens, G.; Temmerman, M. Birth weight for gestational age among Flemish twin population. Facts Views Vis. ObGyn. 2012, 4, 42–49. [Google Scholar] [PubMed]
- Schellong, K.; Schulz, S.; Harder, T.; Plagemann, A. Birth weight and long-term overweight risk: Systematic review and a meta-analysis including 643,902 persons from 66 studies and 26 countries globally. PLoS ONE 2012, 7, e47776. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Survey | |
|---|---|
| Age 0–6 months | Pregnancy and birth Table for keeping track of motor milestones |
| Age 2 years | Growth and motor milestone achievement |
| Age 4–10 years | Growth and socioeconomic status |
| Birth | 6 months | 14 months | 2 years | 4 years | 7 years | 10 years | |
|---|---|---|---|---|---|---|---|
| Infants | |||||||
| Total (N) | 18,514 | 15,619 | 12,998 | 12,261 | 6793 | 6152 | 5325 |
| Girls, (N) | 9282 | 7857 | 6568 | 6186 | 3461 | 3176 | 2750 |
| Gestational age (weeks) | 37.0 ± 2.0 | - | - | - | - | - | - |
| Age (years) | 0.5 ± 0.0 | 1.2 ± 0.1 | 2.1 ± 0.2 | 3.9 ± 0.2 | 7.3 ± 0.3 | 10.0 ± 0.5 | |
| Anthropometrics | |||||||
| Weight (kg) | 2.6 ± 0.5 | 7.1 ± 0.8 | 10.1 ± 1.1 | 12.6 ± 1.5 | 16.6 ± 2.1 | 25.1 ± 4.0 | 33.8 ± 6.1 |
| Length (cm) | 65.5 ± 2.7 | 77.5 ± 3.1 | 88.3 ± 3.8 | 104.3 ± 4.4 | 127.6 ± 6.0 | 143.2 ± 7.1 | |
| WfL (SDS) | −0.05 ± 0.98 | −0.09 ± 0.93 | - | - | - | - | |
| BMI (kg/m2) | - | - | 16.2 ± 1.3 | 15.2 ± 1.3 | 15.4 ± 1. 8 | 16.4 ± 2.2 | |
| BMI-for-age (SDS) | - | - | −0.10 ± 1.02 | −0.32 ± 1.03 | −0.40 ± 1.06 | −0.31 ± 1.10 | |
| Overweight/obese (%) * | - | - | - | 5.4 | 7.7 | 8.2 |
| Rolling | Sitting | Crawling | Standing | Walking | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age of achievement | (months) | 6.2 ± 1.7 | 8.6 ± 1.8 | 9.9 ± 2.3 | 12.2 ± 2.5 | 14.8 ± 2.3 | |||||
| Birth weight (grams) | birth | −0.235 | [−0.311; −0.160] ** | −0.130 | [−0.208; −0.052] ** | −0.125 | [−0.228; −0.023] ** | −0.157 | [−0.266; −0.048] ** | −0.085 | [−0.184; 0.015] |
| Weight-for-length SDS | 6 months | 0.055 | [0.025; 0.085] ** | −0.148 | [−0.179; −0.117] ** | −0.030 | [−0.071; 0.011] | −0.099 | [−0.143; −0.055] ** | −0.111 | [−0.151; −0.071] ** |
| 14 months | 0.016 | [−0.007; 0.063] | −0.149 | [−0.185; −0.112] ** | −0.063 | [−0.111; −0.016] ** | −0.150 | [−0.201; −0.099] ** | −0.165 | [−0.212; −0.119] ** | |
| Age of Achievement (Months) | BMI SDS | ||||
|---|---|---|---|---|---|
| age 2 years | age 4 years | age 7 years | age 10 years | ||
| Rolling | 6.2 ± 1.7 | 0.014 [0.003; 0.025] * | 0.012 [−0.002; 0.026] | −0.001 [−0.016; 0.014] | −0.011 [−0.029; 0.007] |
| Sitting | 8.6 ± 1.8 | −0.023 [−0.033; −0.012] ** | −0.019 [−0.033; −0.005] ** | −0.032 [−0.046; −0.018] ** | −0.039 [−0.056; −0.021] ** |
| Crawling | 9.9 ± 2.3 | 0.001 [−0.007; 0.009] | 0.000 [−0.010; −0.010] | −0.012 [−0.023; - 0.001] * | −0.016 [−0.030; −0.003] * |
| Standing | 12.2 ± 2.5 | −0.003 [−0.010; 0.005] | −0.013 [−0.022; −0.003] ** | −0.023 [−0.033; −0.012] ** | −0.029 [−0.042; −0.017] ** |
| Walking | 14.8 ± 2.3 | −0.005 [−0.013; −0.003] | −0.009 [−0.020; −0.001] | −0.024 [−0.035; −0.013] ** | −0.031 [−0.045; −0.018] ** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brouwer, S.I.; Stolk, R.P.; Bartels, M.; van Beijsterveld, T.C.E.M.; Boomsma, D.I.; Corpeleijn, E. Infant Motor Milestones and Childhood Overweight: Trends over Two Decades in A Large Twin Cohort. Int. J. Environ. Res. Public Health 2020, 17, 2366. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072366
Brouwer SI, Stolk RP, Bartels M, van Beijsterveld TCEM, Boomsma DI, Corpeleijn E. Infant Motor Milestones and Childhood Overweight: Trends over Two Decades in A Large Twin Cohort. International Journal of Environmental Research and Public Health. 2020; 17(7):2366. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072366
Chicago/Turabian StyleBrouwer, Silvia I., Ronald P. Stolk, Meike Bartels, Toos C.E.M. van Beijsterveld, Dorret I. Boomsma, and Eva Corpeleijn. 2020. "Infant Motor Milestones and Childhood Overweight: Trends over Two Decades in A Large Twin Cohort" International Journal of Environmental Research and Public Health 17, no. 7: 2366. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072366