Cognitive Function and Mortality: Results from Kaunas HAPIEE Study 2006–2017

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Cognitive Function
2.3. Covariates
2.4. Mortality
2.5. Statistical Analysis
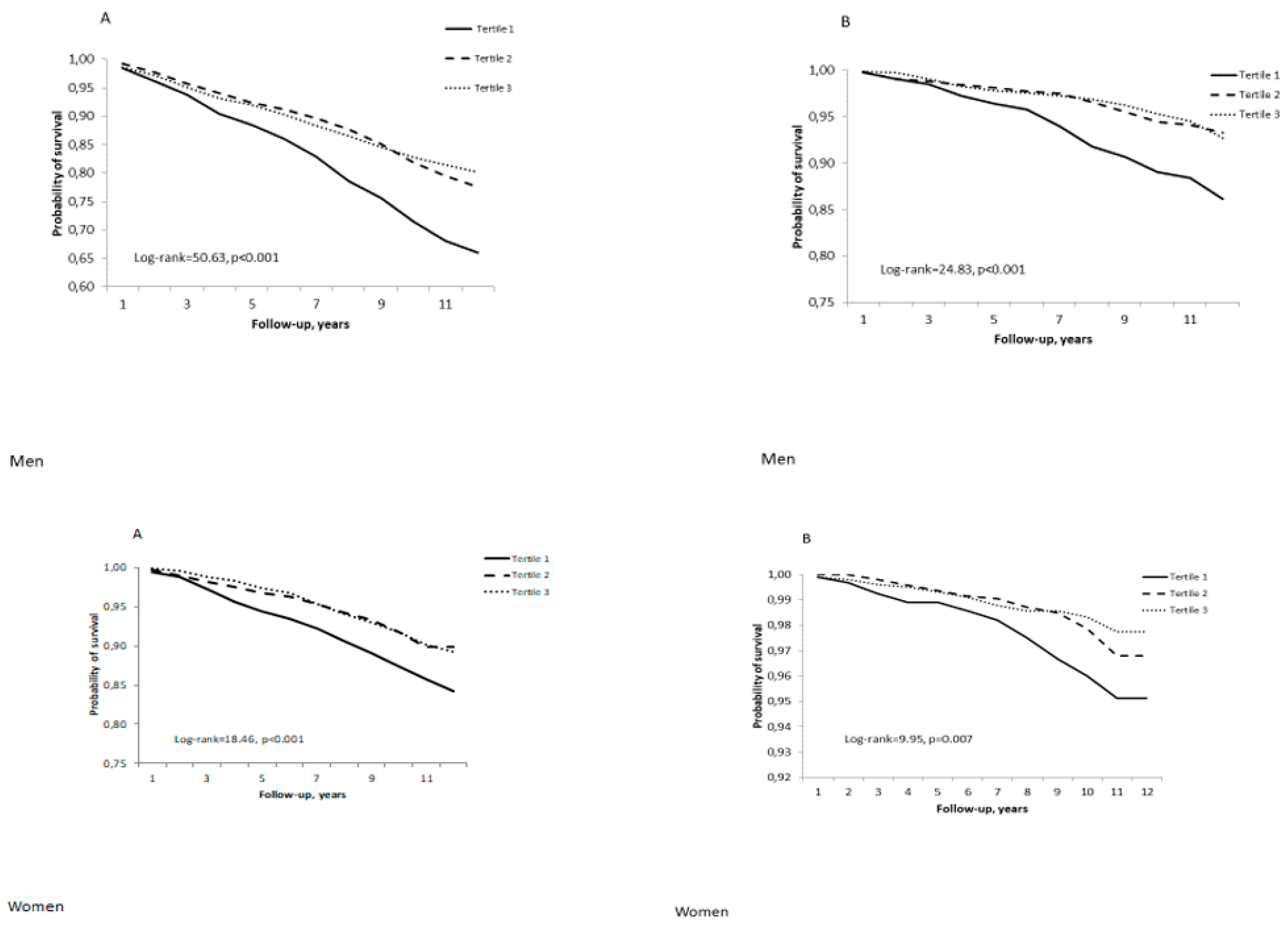
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hagger-Johnson, G.; Deary, I.J.; Davies, C.A.; Weiss, A.; Batty, G.D. Reaction time and mortality from the major causes of death: The NHANES-III study. PLoS ONE 2014, 9, e82959. [Google Scholar] [CrossRef] [Green Version]
- Lo Coco, D.; Lopez, G.; Corrao, S. Cognitive impairment and stroke in elderly patients. Vasc. Health Risk Manag. 2016, 12, 105–116. [Google Scholar] [CrossRef] [Green Version]
- Ayalon, L. Subjective cognitive functioning as a predictor of all cause mortality in an Israeli national sample of community dwelling older adults. Int. J. Geriatr. Psychiatry 2008, 23, 830–836. [Google Scholar] [CrossRef]
- Gillum, R.; Obisesan, T. Physical Activity, Cognitive Function, and Mortality in a US National Cohort. Ann. Epidemiol. 2010, 20, 251–257. [Google Scholar] [CrossRef] [Green Version]
- Perna, L.; Wahl, H.; Mons, U.; Saum, K.; Holleczek, B.; Brenner, H. Cognitive impairment, all-cause and cause-specific mortality among non-demented older adults. Age Ageing 2015, 44, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Gillum, R.F.; Kwagyan, J.; Obisesan, T.O. Smoking, cognitive function and mortality in a U.S. national cohort study. Int. J. Environ. Res. Public Health 2011, 8, 3628–3636. [Google Scholar] [CrossRef] [PubMed]
- Ensrud, K.E.; Lui, L.Y.; Paudel, M.L.; Schousboe, J.T.; Kats, A.M.; Cauley, J.A.; McCulloch, C.E.; Yaffe, K.; Cawthon, P.M.; Hillier, T.A.; et al. Effects of Mobility and Cognition on Risk of Mortality in Women in Late Life: A Prospective Study. J. Gerontol. A. Biol. Sci. Med. Sci. 2016, 71, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, I.; Wharton, W.; Mack, W.J.; Levey, A.I.; Goldstein, F.C. Racial Disparity in Cognitive and Functional Disability in Hypertension and All-Cause Mortality. Am. J. Hypertens. 2016, 29, 185–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strand, B.H.; Knapskog, A.B.; Persson, K.; Edwin, T.H.; Amland, R.; Mjørud, M.; Bjertness, E.; Engedal, K.; Selbæk, G. Survival and years of life lost in various aetiologies of dementia, mild cognitive impairment (MCI) and subjective cognitive decline (SCD) in Norway. PLoS ONE 2018, 13, e0204436. [Google Scholar] [CrossRef] [PubMed]
- Roehr, S.; Luck, T.; Heser, K.; Fuchs, A.; Ernst, A.; Wiese, B.; Werle, J.; Bickel, H.; Brettschneider, C.; Koppara, A.; et al. Incident Subjective Cognitive Decline Does Not Predict Mortality in the Elderly--Results from the Longitudinal German Study on Ageing, Cognition, and Dementia (AgeCoDe). PLoS ONE 2016, 11, e0147050. [Google Scholar] [CrossRef] [Green Version]
- Siersma, V.; Waldemar, G.; Waldorff, F.B. Subjective memory complaints in primary care patients and death from all causes: A four-year follow-up. Scand. J. Prim. Health Care 2013, 31, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, W.C.; Chou, M.Y.; Peng, L.N.; Lin, Y.T.; Liang, C.K.; Chen, L.K. Synergistic effects of cognitive impairment on physical disability in all-cause mortality among men aged 80 years and over: Results from longitudinal older veterans study. PLoS ONE 2017, 12, e0181741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, X.; Li, W.; Ma, Y.; Chen, H.; Zeng, Y.; Yu, X.; Hofman, A.; Wang, H. Cognitive decline and mortality among community-dwelling Chinese older people. BMC Med. 2019, 17, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obisesan, T.O.; Gillum, R.F. Cognitive function, social integration and mortality in a U.S. national cohort study of older adults. BMC Geriatr. 2009, 9, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, J.; Li, H.; Tang, Z.; Zheng, D.; Guo, J.; Liu, Y.; Feng, W.; Li, X.; Wang, A.; Liu, X.; et al. Cognitive Impairment and Risk of All-Cause and Cardiovascular Disease Mortality Over 20-Year Follow-up: Results From the BLSA. J. Am. Heart. Assoc. 2018, 7, e008252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dichgans, M.; Leys, D. Vascular Cognitive Impairment. Circ. Res. 2017, 120, 573–591. [Google Scholar] [CrossRef]
- Wu, T.; Fratiglioni, L.; Matthews, F.; Lobo, A.; Breteler, M.; Skoog, I.; Brayne, C. Dementia in Western Europe: Epidemiological Evidence and Implications for Policy Making. Lancet. Neurol. 2016, 15, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Yaffe, K.; Peltz, C.B.; Ewing, S.K.; McCulloch, C.E.; Cummings, S.R.; Cauley, J.A.; Hillier, T.A.; Ensrud, K.E. Long-term Cognitive Trajectories and Mortality in Older Women. J. Gerontol. A. Biol. Sci. Med. Sci. 2016, 71, 1074–1080. [Google Scholar] [CrossRef]
- Batty, G.D.; Deary, I.J.; Zaninotto, P. Association of Cognitive Function With Cause-Specific Mortality in Middle and Older Age: Follow-up of Participants in the English Longitudinal Study of Ageing. Am. J. Epidemiol. 2016, 183, 183–190. [Google Scholar] [CrossRef] [Green Version]
- Benito-León, J.; Romero, J.P.; Louis, E.D.; Bermejo-Pareja, F. Faster cognitive decline in elders without dementia and decreased risk of cancer mortality: NEDICES Study. Neurology 2014, 82, 1441–1448. [Google Scholar] [CrossRef] [Green Version]
- Peng, T.C.; Chen, W.L.; Wu, L.W.; Chen, Y.J.; Liaw, F.Y.; Wang, G.C.; Wang, C.C.; Yang, Y.H. The Effect of Neurobehavioral Test Performance on the All-Cause Mortality among US Population. BioMed. Res. Int. 2016, 2016, 5927289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kochan, N.A.; Bunce, D.; Pont, S.; Crawford, J.D.; Brodaty, H.; Sachdev, P.S. Is intraindividual reaction time variability an independent cognitive predictor of mortality in old age? Findings from the Sydney Memory and Ageing Study. PLoS ONE 2017, 12, e0181719. [Google Scholar] [CrossRef] [PubMed]
- Peasey, A.; Bobak, M.; Kubinova, R.; Malyutina, S.; Pajak, A.; Tamosiunas, A.; Pikhart, H.; Nicholson, A.; Marmot, M. Determinants of cardiovascular disease and other non-communicable diseases in Central and Eastern Europe: Rationale and design of the HAPIEE study. BMC Public Health 2006, 6, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamosiunas, A.; Baceviciene, M.; Reklaitiene, R.; Radisauskas, R.; Jureniene, K.; Azaraviciene, A.; Luksiene, D.; Malinauskiene, V.; Daugeliene, E.; Sapranaviciute-Zabazlajeva, L. Cardiovascular risk factors and cognitive function in middle aged and elderly Lithuanian urban population: Results from the HAPIEE study. BMC Neurol. 2012, 12, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.R.; Netuveli, G.; Blane, D.; Peasey, A.; Malyutina, S.; Simonova, G.; Kubinova, R.; Pajak, A.; Croezen, S.; Bobak, M.; et al. Psychometric properties and confirmatory factor analysis of the CASP-19, a measure of quality of life in early old age: The HAPIEE study. Aging Ment. Health. 2015, 19, 595–609. [Google Scholar] [CrossRef] [PubMed]
- Sapranaviciute-Zabazlajeva, L.; Luksiene, D.; Virviciute, D.; Kranciukaite-Butylkiniene, D.; Bobak, M.; Tamosiunas, A. Changes in psychological well-being among older Lithuanian city dwellers: Results from a cohort study. Int. J. Clin. Health. Psychol. 2018, 18, 218–226. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Crush, E.; Joyner, C. Cardiovascular disease biomarkers on cognitive function in older adults: Joint effects of cardiovascular disease biomarkers and cognitive function on mortality risk. Prev. Med. 2017, 94, 27–30. [Google Scholar] [CrossRef]
- Hayat, S.A.; Luben, R.; Dalzell, N.; Moore, S.; Hogervorst, E.; Matthews, F.E.; Wareham, N.; Brayne, C.; Khaw, K.T. Understanding the relationship between cognition and death: A within cohort examination of cognitive measures and mortality. Eur. J. Epidemiol. 2018, 33, 1049–1062. [Google Scholar] [CrossRef] [Green Version]
- Bostock, S.; Steptoe, A. Association between low functional health literacy and mortality in older adults: Longitudinal cohort study. BMJ 2012, 344, e1602. [Google Scholar] [CrossRef] [Green Version]
- Sabia, S.; Guéguen, A.; Marmot, M.G.; Shipley, M.J.; Ankri, J.; Singh-Manoux, A. Does cognition predict mortality in midlife? Results from the Whitehall II cohort study. Neurobiol. Aging 2010, 31, 688–695. [Google Scholar] [CrossRef] [Green Version]
- At, J.; Bryce, R.; Prina, M.; Acosta, D.; Ferri, C.P.; Guerra, M.; Huang, Y.; Rodriguez, J.J.; Salas, A.; Sosa, A.L.; et al. Frailty and the prediction of dependence and mortality in low- and middle-income countries: A 10/66 population-based cohort study. BMC Med. 2015, 13, 138. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.J.; Peng, L.N.; Liang, C.K.; Loh, C.H.; Chen, L.K. Cognitive frailty predicting all-cause mortality among community-living older adults in Taiwan: A 4-year nationwide population-based cohort study. PLoS ONE 2018, 13, e0200447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, L.; Zin Nyunt, M.S.; Gao, Q.; Yap, K.B.; Ng, T.P. Cognitive Frailty and Adverse Health Outcomes: Findings From the Singapore Longitudinal Ageing Studies (SLAS). J. Am. Med. Dir. Assoc. 2017, 18, 252–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojagbemi, A.; Bello, T.; Gureje, O. Cognitive Reserve, Incident Dementia, and Associated Mortality in the Ibadan Study of Ageing. J. Am. Geriatr. Soc. 2016, 64, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Contador, I.; Bermejo-Pareja, F.; Mitchell, A.J.; Trincado, R.; Villarejo, A.; Sánchez-Ferro, Á.; Benito-León, J. Cause of death in mild cognitive impairment: A prospective study (NEDICES). Eur. J. Neurol. 2014, 21, 253-e259. [Google Scholar] [CrossRef] [Green Version]
- Gorelick, P.B.; Scuteri, A.; Black, S.; Decarli, C.; Greenberg, S.M.; Iadecola, C.; Launer, L.J.; Laurent, S.; Lopez, O.L. Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011, 42, 2672–2713. [Google Scholar] [CrossRef]
- Guehne, U.; Angermeyer, M.C.; Riedel-Heller, S. Is mortality increased in mildly cognitively impaired individuals? A systematic literature review. Dement. Geriatr. Cogn. Disord. 2006, 21, 403–410. [Google Scholar] [CrossRef]
- Santabárbara, J.; Lopez-Anton, R.; Marcos, G.; De-la-Cámara, C.; Lobo, E.; Saz, P.; Gracia-García, P.; Ventura, T.; Campayo, A.; Rodríguez-Mañas, L.; et al. Degree of cognitive impairment and mortality: A 17-year follow-up in a community study. Epidemiol. Psychiatr. Sci. 2015, 24, 503–511. [Google Scholar] [CrossRef]
- Rajan, K.B.; Aggarwal, N.T.; Wilson, R.S.; Everson-Rose, S.A.; Evans, D.A. Association of cognitive functioning, incident stroke, and mortality in older adults. Stroke 2014, 45, 2563–2567. [Google Scholar] [CrossRef] [Green Version]
- Cukierman-Yaffe, T.; Gerstein, H.C.; Miller, M.E.; Launer, L.J.; Williamson, J.D.; Horowitz, K.R.; Ismail-Beigi, F.; Lazar, R.M. The Relationship Between the Score on a Simple Measure of Cognitive Function and Incident CVD in People With Diabetes: A Post Hoc Epidemiological Analysis From the ACCORD-MIND Study. J. Clin. Endocrinol. Metab. 2017, 102, 3218–3225. [Google Scholar] [CrossRef]
- Georgakis, M.K.; Protogerou, A.D.; Kalogirou, E.I.; Kontogeorgi, E.; Pagonari, I.; Sarigianni, F.; Papageorgiou, S.G.; Kapaki, E.; Papageorgiou, C.; Tousoulis, D.; et al. Blood Pressure and All-Cause Mortality by Level of Cognitive Function in the Elderly: Results From a Population-Based Study in Rural Greece. J. Clin. Hypertens. (Greenwich) 2017, 19, 161–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Igari, R.; Davy, P.; Sato, H.; Takahashi, Y.; Iseki, C.; Kato, H.; Koyama, S.; Ishizawa, K.; Allsopp, R.; Kato, T. Cognitive impairment, brain ischemia and shorter telomeres are predictors of mortality in the Japanese elderly: A 13-year prospective community-based study. J. Neurol. Sci. 2019, 397, 129–134. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| MEN | WOMEN | |||||
|---|---|---|---|---|---|---|
| Variables | Alive | All-Cause Deaths | CVD Deaths c | Alive | All-Cause Deaths | CVD Deaths c |
| n = 2462 | n = 667 | n = 160 | n = 3391 | n = 384 | n = 81 | |
| Age, years | 56.1 ± 0.15 | 62.0 ± 0.34 b | 62.7 ± 0.50 b | 56.3 ± 0.13 | 63.0 ± 0.46 b | 66.4 ± 0.53 b |
| Immediate verbal recall sum a, score | 21.9 ± 0.08 | 19.5 ± 0.18 b | 19.1 ± 0.27 b | 23.3 ± 0.06 | 21.2 ± 0.25 b | 19.9 ± 0.41 |
| Delayed verbal recall a, score | 7.72 ± 0.36 | 6.76 ± 0.09 b | 6.61 ± 0.14 b | 8.32 ± 0.27 | 7.39 ± 0.11 b | 6.93 ± 0.20 b |
| Semantic verbal fluency a | 22.6 ± 0.12 | 20.0 ± 0.26 b | 19.4 ± 0.37 b | 22.4 ± 0.10 | 19.5 ± 0.38 b | 17.3 ± 0.55 b |
| Numerical ability a, score | 3.14 ± 0.01 | 2.95 ± 0.04 b | 2.89 ± 0.06 b | 2.91 ± 0.01 | 2.71 ± 0.05 b | 2.57 ± 0.08 b |
| Cognitive speed and attention a | 16.5 ± 0.09 | 13.7 ± 0.20 b | 13.2 ± 0.32 b | 17.6 ± 0.08 | 14.6 ± 0.30 b | 13.5 ± 0.52 b |
| Composite score of cognitive function a | –0.08 ± 0.01 | –0.27 ± 0.03 b | –0.34 ± 0.05 b | 0.11 ± 0.01 | -0.06 ± 0.04 b | –0.17 ± 0.07 b |
| Systolic blood pressure a, mm Hg | 143.3 ± 0.40 | 150.9 ± 1.04 b | 153.7 ± 1.63 b | 133.4 ± 0.34 | 143.0 ± 1.43 b | 150.8 ± 2.47 b |
| Diastolic blood pressure a, mm Hg | 92.4 ± 0.25 | 94.9 ± 0.61 b | 95.9 ± 0.93 b | 87.4 ± 0.20 | 90.8 ± 0.76 b | 93.0 ± 1.33 b |
| Total cholesterol a, mmol/L | 5.83 ± 0.02 | 5.74 ± 0.05 | 5.80 ± 0.08 | 6.07 ± 0.02 | 5.96 ± 0.07 | 5.94 ± 0.12 |
| HDL cholesterol a, mmol/L | 1.41 ± 0.01 | 1.40 ± 0.02 | 1.31 ± 0.02 b | 1.60 ± 0.01 | 1.51 ± 0.02 b | 1.46 ± 0.03 b |
| LDL cholesterol a, mmol/L | 3.74 ± 0.02 | 3.64 ± 0.05 b | 3.73 ± 0.07 | 3.83 ± 0.02 | 3.73 ± 0.06 | 3.72 ± 0.10 |
| Triglyceridea, mmol/L | 1.51 ± 0.02 | 1.57 ± 0.05 | 1.76 ± 0.08 b | 1.40 ± 0.02 | 1.53 ± 0.05 b | 1.67 ± 0.10 b |
| Fasting blood glucose a, mmol/L | 5.72 ± 0.02 | 6.05 ± 0.07 b | 6.29 ± 0.13 b | 5.75 ± 0.02 | 6.19 ± 0.10 b | 6.55 ± 0.21 b |
| Body mass index a, kg/m2 | 28.3 ± 0.09 | 28.5 ± 0.23 | 29.6 ± 0.36 b | 29.3 ± 0.10 | 31.5 ± 0.37 b | 31.9 ± 0.67 b |
| Physical activity in leisure time a, hours/week | 17.1 ± 0.24 | 16.1 ± 0.59 | 15.5 ± 0.84 | 19.7 ± 0.19 | 17.1 ± 0.62 b | 16.7 ± 1.06 b |
| Absolute alcohol a, drinks/week | 58.7 ± 2.13 | 65.4 ± 7.09 | 72.3 ± 12.9 | 20.1 ± 0.55 | 14.7 ± 1.65 b | 10.5 ± 2.32 b |
| Psychological well-being, PWB a, score | 39.7 ± 0.11 | 37.7 ± 0.26 b | 37.8 ± 0.37 b | 38.1 ± 0.10 | 36.0 ± 0.40 b | 34.3 ± 0.64 b |
| Ischemic heart disease % (n) | 11.1 (287) | 32.5 (172) b | 43.9 (105) b | 15.6 (547) | 29.4 (87) b | 43.9 (47) b |
| Stroke % (n) | 2.7 (70) | 8.4 (44) b | 10.5 (25) b | 2.9 (100) | 5.1 (15) b | 10.5 (11) b |
| Diabetes mellitus % (n) | 6.0 (150) | 14.7 (74) b | 19.4 (44) b | 6.5 (223) | 19.9 (57) b | 29.8 (31) b |
| Arterial hypertension % (n) | 68.9 (1771) | 80.1 (418) b | 82.6 (194) b | 56.0 (1957) | 73.0 (214) b | 81.7 (85) b |
| Body mass index, % (n) | p = 0.11 | p < 0.001 | ||||
| <25.0 kg/m2 | 22.8 (587) | 26.1 (138) | 21.3 (25) | 23.8 (833) | 14.2 (42) b | 16.8 (18) |
| 25.0–29.9 kg/m2 | 45.3 (1166) | 38.2 (202) b | 34.7 (83) b | 36.2 (1269) | 30.5 (90) b | 25.2 (27) |
| >= 30.0 kg/m2 | 31.9 (821) | 35.7 (189) | 43.9 (105) b | 40.0 (1402) | 55.3 (163) b | 57.9 (62) b |
| Smoking habits % (n) | p < 0.001 | p = 0.051 | ||||
| Smokers | 34.9 (895) | 40.2 (211) b | 38.2 (91) | 13.9 (487) | 9.2 (27) b | 5.7 (6) |
| Former smokers | 28.2 (724) | 31.8 (167) | 32.8 (78) | 8.5 (298) | 10.6 (31) | 9.5 (10) |
| Never smokers | 36.9 (948) | 28.0 (147) b | 29.0 (69) | 77.6 (2715) | 80.1 (234) | 84.8 (89) |
| Marital status % (n) | p < 0.001 | p < 0.001 | ||||
| Single | 2.0 (51) | 2.9 (15) | 2.5 (6) | 6.3 (220) | 5.5 (16) | 2.8 (3) |
| Married | 84.8 (2176) | 77.0 (405) b | 76.9 (183) b | 60.1 (2106) | 50.2 (147) b | 50.9 (54) |
| Cohabiting | 1.9 (49) | 1.5 (8) | 1.3 (3) | 1.2 (42) | 0.7 (2) | 0.0 (0) |
| Divorced | 8.0 (206) | 10.5 (55) | 9.7 (23) | 17.1 (598) | 18.1 (53) | 16.0 (17) |
| Widowed | 3.3 (84) | 8.2 (43) b | 9.7 (23) b | 15.3 (537) | 25.6 (75) b | 30.2 (32) b |
| Education % (n) | p < 0.001 | p < 0.001 | ||||
| Primary | 3.3 (84) | 11.0 (58) b | 11.8 (28) b | 3.5 (123) | 13.0 (38) b | 20.8 (22) b |
| Vocational | 7.6 (195) | 15.0 (79) b | 13.4 (32) b | 6.1 (212) | 11.3 (33) b | 10.4 (11) |
| Secondary | 32.7 (839) | 34.2 (180) | 34.5 (82) | 26.0 (910) | 25.7 (75) | 27.4 (29) |
| College | 20.1 (206) | 16.0 (84) b | 15.5 (37) | 29.1 (1018) | 23.3 (68) b | 20.8 (22) |
| University | 36.3 (932) | 23.8 (125) b | 24.8 (59) b | 35.4 (1240) | 26.7 (78) b | 20.8 (22) b |
| Depression scale score % (n) | p < 0.001 | p = 0.101 | ||||
| >= 4 | 14.3 (359) | 21.3 (109) b | 23.7 (55) b | 27.9 (961) | 32.5 (93) | 36.5 (38) |
| <4 | 85.7 (2158) | 78.7 (402) b | 76.3 (177) b | 72.1 (2485) | 67.5 (193) | 63.5 (66) |
| Cognitive function % (n) | p < 0.001 | p < 0.001 | ||||
| Normal | 80.9 (2084) | 73.0 (386) b | 69.5 (166) b | 89.2 (3129) | 78.7 (233) b | 71.0 (76) b |
| Lowered | 19.1 (491) | 27.0 (143) b | 30.5 (73) b | 10.8 (378) | 21.3 (63) b | 29.0 (31) b |
| PWB % (n) | p < 0.001 | p < 0.001 | ||||
| Higher | 55.9 (1323) | 41.7 (201) b | 41.6 (91) b | 58.2 (1894) | 42.7 (114) b | 32.3 (31) b |
| Lower | 44.1 (1042) | 58.3 (281) b | 58.4 (128) b | 41.8 (1358) | 57.3 (153) b | 67.7 (65) b |
| Cognitive Function/Cox | MEN | WOMEN | ||||||
|---|---|---|---|---|---|---|---|---|
| Models | All-Cause | Deaths | CVD | Deaths | All-cause | Deaths | CVD | Deaths |
| n = 667 | n = 160 | n = 384 | n = 81 | |||||
| Hazard Ratios (HR) | 95% CI | HR | 95% CI | HR | 95% CI | HR | 95% CI | |
| Immediate verbal recall sum | ||||||||
| Model 1 | 1.19 | 1.10–1.29 | 1.26 | 1.08–1.47 | 1.26 | 1.12–1.41 | 1.46 | 1.15–1.84 |
| Model 2 | 1.14 | 1.05–1.24 | 1.17 | 0.99–1.38 | 1.24 | 1.10–1.40 | 1.50 | 1.15–1.95 |
| Model 3 | 1.16 | 1.06–1.27 | 1.18 | 0.99–1.40 | 1.25 | 1.10–1.41 | 1.70 | 1.29–2.24 |
| Model 4 | 1.14 | 1.04–1.25 | 1.17 | 0.98–1.40 | 1.25 | 1.10–1.42 | 1.69 | 1.28–2.23 |
| Delayed verbal recall | ||||||||
| Model 1 | 1.17 | 1.09–1.27 | 1.27 | 1.09–1.47 | 1.20 | 1.08–1.33 | 1.35 | 1.07–1.70 |
| Model 2 | 1.12 | 1.04–1.23 | 1.17 | 0.99–1.38 | 1.19 | 1.06–1.33 | 1.46 | 1.14–1.88 |
| Model 3 | 1.15 | 1.05–1.25 | 1.19 | 1.004–1.42 | 1.17 | 1.04–1.32 | 1.58 | 1.21–2.05 |
| Model 4 | 1.13 | 1.04–1.23 | 1.19 | 1.003–1.42 | 1.17 | 1.04–1.32 | 1.57 | 1.21–2.04 |
| Semantic verbal fluency | ||||||||
| Model 1 | 1.21 | 1.11–1.31 | 1.24 | 1.03–1.48 | 1.22 | 1.08–1.37 | 1.81 | 1.38–2.37 |
| Model 2 | 1.16 | 1.07–1.27 | 1.16 | 0.96–1.39 | 1.19 | 1.06–1.34 | 1.81 | 1.37–2.40 |
| Model 3 | 1.16 | 1.06–1.28 | 1.13 | 0.93–1.38 | 1.18 | 1.03–1.34 | 1.89 | 1.39–2.57 |
| Model 4 | 1.15 | 1.05–1.27 | 1.14 | 0.94–1.38 | 1.18 | 1.04–1.34 | 1.00 | 0.76–1.31 |
| Numerical ability | ||||||||
| Model 1 | 1.07 | 0.99–1.17 | 1.20 | 1.01–1.41 | 1.07 | 0.97–1.18 | 1.04 | 0.85–1.28 |
| Model 2 | 1.03 | 0.94–1.13 | 1.09 | 0.90–1.31 | 1.08 | 0.97–1.20 | 1.11 | 0.89–1.38 |
| Model 3 | 1.03 | 0.94–1.13 | 1.02 | 0.85–1.24 | 1.09 | 0.98–1.22 | 1.24 | 0.99–1.56 |
| Model 4 | 1.03 | 0.94–1.13 | 1.03 | 0.85–1.24 | 1.09 | 0.97–1.21 | 1.24 | 0.99–1.56 |
| Cognitive speed and attention | ||||||||
| Model 1 | 1.33 | 1.22–1.45 | 1.48 | 1.23–1.77 | 1.43 | 1.27–1.60 | 1.40 | 1.09–1.80 |
| Model 2 | 1.29 | 1.17–1.41 | 1.39 | 1.14–1.70 | 1.37 | 1.21–1.54 | 1.43 | 1.10–1.87 |
| Model 3 | 1.28 | 1.16–1.42 | 1.32 | 1.08–1.62 | 1.34 | 1.18–1.51 | 1.47 | 1.11–1.95 |
| Model 4 | 1.24 | 1.12–1.37 | 1.32 | 1.08–1.62 | 1.33 | 1.17–1.51 | 1.00 | 0.77–1.31 |
| Composite score of cognitive function | ||||||||
| Model 1 | 1.27 | 1.18–1.36 | 1.38 | 1.20–1.60 | 1.31 | 1.19–1.45 | 1.56 | 1.26–1.94 |
| Model 2 | 1.20 | 1.11–1.30 | 1.24 | 1.06–1.46 | 1.30 | 1.17–1.44 | 1.68 | 1.31–2.14 |
| Model 3 | 1.20 | 1.07–1.34 | 1.23 | 1.04–1.45 | 1.29 | 1.16–1.45 | 1.91 | 1.47–2.48 |
| Model 4 | 1.19 | 1.10–1.30 | 1.32 | 1.08–1.62 | 1.30 | 1.16–1.45 | 1.91 | 1.48–2.48 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamosiunas, A.; Sapranaviciute-Zabazlajeva, L.; Luksiene, D.; Virviciute, D.; Bobak, M. Cognitive Function and Mortality: Results from Kaunas HAPIEE Study 2006–2017. Int. J. Environ. Res. Public Health 2020, 17, 2397. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072397
Tamosiunas A, Sapranaviciute-Zabazlajeva L, Luksiene D, Virviciute D, Bobak M. Cognitive Function and Mortality: Results from Kaunas HAPIEE Study 2006–2017. International Journal of Environmental Research and Public Health. 2020; 17(7):2397. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072397
Chicago/Turabian StyleTamosiunas, Abdonas, Laura Sapranaviciute-Zabazlajeva, Dalia Luksiene, Dalia Virviciute, and Martin Bobak. 2020. "Cognitive Function and Mortality: Results from Kaunas HAPIEE Study 2006–2017" International Journal of Environmental Research and Public Health 17, no. 7: 2397. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072397