Perinatal and Antibiotic Exposures and the Risk of Developing Childhood-Onset Inflammatory Bowel Disease: A Nested Case-Control Study Based on a Population-Based Birth Cohort

 ,
,
Abstract
:1. Introduction
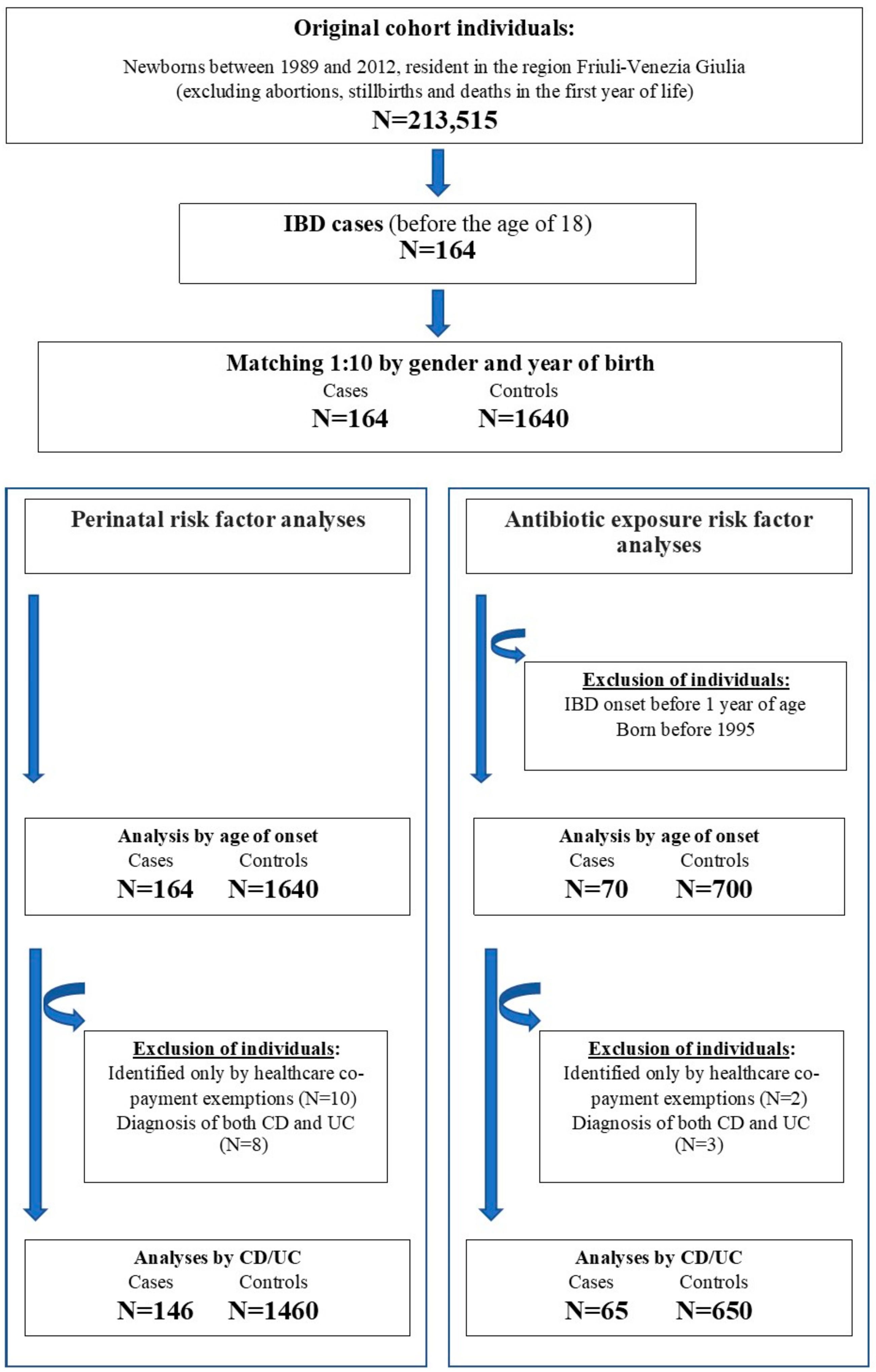
2. Methods
2.1. IBD Case Identification
2.2. Perinatal Conditions and Antibiotic Exposures
2.3. Data Analysis
3. Results
3.1. Perinatal Exposure
3.2. Antibiotic Exposure
4. Discussion
4.1. Main Results
4.2. Previous Literature
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rosen, M.J.; Dhawan, A.; Saeed, S.A. Inflammatory Bowel Disease in Children and Adolescents. JAMA Pediatrics 2015, 169, 1053–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benchimol, E.I.; Fortinsky, K.J.; Gozdyra, P.; Van den Heuvel, M.; Van Limbergen, J.; Griffiths, A.M. Epidemiology of pediatric inflammatory bowel disease: A systematic review of international trends. Inflamm. Bowel Dis. 2011, 17, 423–439. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Griffiths, A.; Markowitz, J.; Wilson, D.C.; Turner, D.; Russell, R.K.; Fell, J.; Ruemmele, F.M.; Walters, T.; Sherlock, M.; et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: The Paris classification. Inflamm. Bowel Dis. 2011, 17, 1314–1321. [Google Scholar] [CrossRef]
- Gupta, N.; Bostrom, A.G.; Kirschner, B.S.; Cohen, S.A.; Abramson, O.; Ferry, G.D.; Gold, B.D.; Winter, H.S.; Baldassano, R.N.; Smith, T.; et al. Presentation and disease course in early-compared to later-onset pediatric Crohn’s disease. Am. J. Gastroenterol. 2008, 103, 2092–2098. [Google Scholar] [CrossRef] [PubMed]
- Snapper, S.B. Very-Early-Onset Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2015, 11, 554–556. [Google Scholar]
- Bequet, E.; Sarter, H.; Fumery, M.; Vasseur, F.; Armengol-Debeir, L.; Pariente, B.; Ley, D.; Spyckerelle, C.; Coevoet, H.; Laberenne, J.E.; et al. Incidence and Phenotype at Diagnosis of Very-early-onset Compared with Later-onset Paediatric Inflammatory Bowel Disease: A Population-based Study [1988–2011]. J. Crohn’s Colitis 2017, 11, 519–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tysk, C.; Lindberg, E.; Jarnerot, G.; Floderus-Myrhed, B. Ulcerative colitis and Crohn’s disease in an unselected population of monozygotic and dizygotic twins. A study of heritability and the influence of smoking. Gut 1988, 29, 990–996. [Google Scholar] [CrossRef] [Green Version]
- Khalili, H.; Granath, F.; Smedby, K.E.; Ekbom, A.; Neovius, M.; Chan, A.T.; Olen, O. Association Between Long-term Oral Contraceptive Use and Risk of Crohn’s Disease Complications in a Nationwide Study. Gastroenterology 2016, 150, 1561–1567.e1. [Google Scholar] [CrossRef] [Green Version]
- Ananthakrishnan, A.N.; Khalili, H.; Konijeti, G.G.; Higuchi, L.M.; de Silva, P.; Fuchs, C.S.; Willett, W.C.; Richter, J.M.; Chan, A.T. Long-term intake of dietary fat and risk of ulcerative colitis and Crohn’s disease. Gut 2014, 63, 776–784. [Google Scholar] [CrossRef] [Green Version]
- Andersson, R.E.; Olaison, G.; Tysk, C.; Ekbom, A. Appendectomy is followed by increased risk of Crohn’s disease. Gastroenterology 2003, 124, 40–46. [Google Scholar] [CrossRef]
- Lowenfels, A.B.; Maisonneuve, P. Appendectomy and protection against ulcerative colitis. N. Engl. J. Med. 2001, 345, 223–224. [Google Scholar]
- Xu, L.; Lochhead, P.; Ko, Y.; Claggett, B.; Leong, R.W.; Ananthakrishnan, A.N. Systematic review with meta-analysis: Breastfeeding and the risk of Crohn’s disease and ulcerative colitis. Aliment. Pharmacol. Ther. 2017, 46, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Barclay, A.R.; Russell, R.K.; Wilson, M.L.; Gilmour, W.H.; Satsangi, J.; Wilson, D.C. Systematic review: The role of breastfeeding in the development of pediatric inflammatory bowel disease. J. Pediatrics 2009, 155, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Bager, P.; Simonsen, J.; Nielsen, N.M.; Frisch, M. Cesarean section and offspring’s risk of inflammatory bowel disease: A national cohort study. Inflamm. Bowel Dis. 2012, 18, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N.; Banerjee, A.; Targownik, L.E.; Singh, H.; Ghia, J.E.; Burchill, C.; Chateau, D.; Roos, L.L. Cesarean Section Delivery Is Not a Risk Factor for Development of Inflammatory Bowel Disease: A Population-based Analysis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2016, 14, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Mendall, M.; Jensen, C.B.; Angquist, L.H.; Baker, J.L.; Jess, T. Childhood growth and risk of inflammatory bowel disease: A population-based study of 317,030 children. Scand. J. Gastroenterol. 2019, 54, 863–868. [Google Scholar] [CrossRef] [PubMed]
- Fanaro, S.; Chierici, R.; Guerrini, P.; Vigi, V. Intestinal microflora in early infancy: Composition and development. Acta Paediatr. (Oslo Nor. 1992). Suppl. 2003, 91, 48–55. [Google Scholar] [CrossRef]
- Penders, J.; Thijs, C.; Vink, C.; Stelma, F.F.; Snijders, B.; Kummeling, I.; van den Brandt, P.A.; Stobberingh, E.E. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics 2006, 118, 511–521. [Google Scholar] [CrossRef] [Green Version]
- Tannock, G.W. The search for disease-associated compositional shifts in bowel bacterial communities of humans. Trends Microbiol. 2008, 16, 488–495. [Google Scholar] [CrossRef]
- Salzman, N.H.; Underwood, M.A.; Bevins, C.L. Paneth cells, defensins, and the commensal microbiota: A hypothesis on intimate interplay at the intestinal mucosa. Semin. Immunol. 2007, 19, 70–83. [Google Scholar] [CrossRef]
- Shaw, S.Y.; Blanchard, J.F.; Bernstein, C.N. Association between the use of antibiotics in the first year of life and pediatric inflammatory bowel disease. Am. J. Gastroenterol. 2010, 105, 2687–2692. [Google Scholar] [CrossRef] [PubMed]
- Kronman, M.P.; Zaoutis, T.E.; Haynes, K.; Feng, R.; Coffin, S.E. Antibiotic exposure and IBD development among children: A population-based cohort study. Pediatrics 2012, 130, e794–e803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortqvist, A.K.; Lundholm, C.; Halfvarson, J.; Ludvigsson, J.F.; Almqvist, C. Fetal and early life antibiotics exposure and very early onset inflammatory bowel disease: A population-based study. Gut 2019, 68, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Troelsen, F.S.; Jick, S. Antibiotic Use in Childhood and Adolescence and Risk of Inflammatory Bowel Disease: A Case-Control Study in the UK Clinical Practice Research Datalink. Inflamm. Bowel Dis. 2019, 26, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Canova, C.; Zabeo, V.; Pitter, G.; Romor, P.; Baldovin, T.; Zanotti, R.; Simonato, L. Association of Maternal Education, Early Infections, and Antibiotic Use With Celiac Disease: A Population-Based Birth Cohort Study in Northeastern Italy. Am. J. Epidemiol. 2014, 180, 76–85. [Google Scholar] [CrossRef] [Green Version]
- Certificato di Assistenza al Parto (CeDAP). Analisi dell’Evento Nascita—Anno 2015. Available online: http://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=2766 (accessed on 1 April 2020).
- Di Domenicantonio, R.; Cappai, G.; Arca, M.; Agabiti, N.; Kohn, A.; Vernia, P.; Biancone, L.; Armuzzi, A.; Papi, C.; Davoli, M. Occurrence of inflammatory bowel disease in central Italy: A study based on health information systems. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2014, 46, 777–782. [Google Scholar] [CrossRef]
- Pitter, G.; Ludvigsson, J.F.; Romor, P.; Zanier, L.; Zanotti, R.; Simonato, L.; Canova, C. Antibiotic exposure in the first year of life and later treated asthma, a population based birth cohort study of 143,000 children. Eur. J. Epidemiol. 2016, 31, 85–94. [Google Scholar] [CrossRef]
- Cholapranee, A.; Ananthakrishnan, A.N. Environmental Hygiene and Risk of Inflammatory Bowel Diseases: A Systematic Review and Meta-analysis. Inflamm. Bowel Dis. 2016, 22, 2191–2199. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, C.N.; Burchill, C.; Targownik, L.E.; Singh, H.; Roos, L.L. Events Within the First Year of Life, but Not the Neonatal Period, Affect Risk for Later Development of Inflammatory Bowel Diseases. Gastroenterology 2019, 156, 2190–2197.e10. [Google Scholar] [CrossRef] [Green Version]
- Butwicka, A.; Sariaslan, A.; Larsson, H.; Halfvarson, J.; Myrelid, P.E.; Olen, O.; Frisen, L.; Lichtenstein, P.; Ludvigsson, J.F. No association between urbanisation, neighbourhood deprivation and IBD: A population-based study of 4 million individuals. Gut 2019, 68, 947–948. [Google Scholar] [CrossRef]
- Dharmaraj, R.; Jaber, A.; Arora, R.; Hagglund, K.; Lyons, H. Seasonal variations in onset and exacerbation of inflammatory bowel diseases in children. BMC Res. Notes 2015, 8, 696. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.J.; Dotson, J.L.; Kappelman, M.D.; King, E.; Pratt, J.M.; Colletti, R.B.; Bistrick, S.; Burkam, J.L.; Crandall, W.V. Seasonality and pediatric inflammatory bowel disease. J. Pediatric Gastroenterol. Nutr. 2014, 59, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Hviid, A.; Svanstrom, H.; Frisch, M. Antibiotic use and inflammatory bowel diseases in childhood. Gut 2011, 60, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Virta, L.; Auvinen, A.; Helenius, H.; Huovinen, P.; Kolho, K.L. Association of repeated exposure to antibiotics with the development of pediatric Crohn’s disease—a nationwide, register-based finnish case-control study. Am. J. Epidemiol. 2012, 175, 775–784. [Google Scholar] [CrossRef] [Green Version]
- Shaw, S.Y.; Blanchard, J.F.; Bernstein, C.N. Association between the use of antibiotics and new diagnoses of Crohn’s disease and ulcerative colitis. Am. J. Gastroenterol. 2011, 106, 2133–2142. [Google Scholar] [CrossRef]
- Card, T.; Logan, R.F.; Rodrigues, L.C.; Wheeler, J.G. Antibiotic use and the development of Crohn’s disease. Gut 2004, 53, 246–250. [Google Scholar] [CrossRef] [Green Version]
- Hildebrand, H.; Malmborg, P.; Askling, J.; Ekbom, A.; Montgomery, S.M. Early-life exposures associated with antibiotic use and risk of subsequent Crohn’s disease. Scand. J. Gastroenterol. 2008, 43, 961–966. [Google Scholar] [CrossRef]
- Ungaro, R.; Bernstein, C.N.; Gearry, R.; Hviid, A.; Kolho, K.L.; Kronman, M.P.; Shaw, S.; Van Kruiningen, H.; Colombel, J.F.; Atreja, A. Antibiotics associated with increased risk of new-onset Crohn’s disease but not ulcerative colitis: A meta-analysis. Am. J. Gastroenterol. 2014, 109, 1728–1738. [Google Scholar] [CrossRef]
- Tanaka, S.; Kobayashi, T.; Songjinda, P.; Tateyama, A.; Tsubouchi, M.; Kiyohara, C.; Shirakawa, T.; Sonomoto, K.; Nakayama, J. Influence of antibiotic exposure in the early postnatal period on the development of intestinal microbiota. FEMS Immunol. Med Microbiol. 2009, 56, 80–87. [Google Scholar] [CrossRef] [Green Version]
- Fouhy, F.; Guinane, C.M.; Hussey, S.; Wall, R.; Ryan, C.A.; Dempsey, E.M.; Murphy, B.; Ross, R.P.; Fitzgerald, G.F.; Stanton, C.; et al. High-throughput sequencing reveals the incomplete, short-term recovery of infant gut microbiota following parenteral antibiotic treatment with ampicillin and gentamicin. Antimicrob. Agents Chemother. 2012, 56, 5811–5820. [Google Scholar] [CrossRef] [Green Version]
- Olszak, T.; An, D.; Zeissig, S.; Vera, M.P.; Richter, J.; Franke, A.; Glickman, J.N.; Siebert, R.; Baron, R.M.; Kasper, D.L.; et al. Microbial exposure during early life has persistent effects on natural killer T cell function. Science 2012, 336, 489–493.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.C.; Khalili, H.; Gower-Rousseau, C.; Olen, O.; Benchimol, E.I.; Lynge, E.; Nielsen, K.R.; Brassard, P.; Vutcovici, M.; Bitton, A.; et al. Sex-Based Differences in Incidence of Inflammatory Bowel Diseases-Pooled Analysis of Population-Based Studies From Western Countries. Gastroenterology 2018, 155, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, D. Preclinical and Undiagnosed Crohn’s Disease: The Submerged Iceberg. Inflamm. Bowel Dis. 2016, 22, 476–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, J.R.; Ferguson, E.; Simms, L.A.; Hanigan, K.; Doecke, J.D.; Langguth, D.; Arnott, A.; Radford-Smith, G. Detectable Laboratory Abnormality Is Present up to 12 Months Prior to Diagnosis in Patients with Crohn’s Disease. Dig. Dis. Sci. 2019, 64, 503–517. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All IBD Cases | IBD Cases for Antibiotic Exposure ^ | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total (n = 164), (%) | EO-IBD † (n = 62), n (%) | P-IBD ‡ (n = 140), n (%) | Crohn’s Disease * (n = 83), n (%) | Ulcerative Colitis * (n = 63), n (%) | Total (n = 70), n (%) | EO-IBD † (n = 34), n (%) | P-IBD ‡ (n = 36), n (%) | Crohn’s Disease § (n = 38), n (%) | Ulcerative Colitis§ (n = 27), n (%) | |
| Sex | ||||||||||
| Male | 95 (58) | 38 (61) | 57 (56) | 52 (63) | 34 (54) | 44 (63) | 23 (64) | 21 (62) | 26 (68) | 16 (59) |
| Female | 69 (42) | 24 (39) | 45 (44) | 31 (37) | 29 (46) | 26 (37) | 13 (36) | 13 (38) | 12 (32) | 11 (41) |
| Calendar year of birth | ||||||||||
| 1989–1993 | 67 (41) | 12 (19) | 55 (54) | 31 (38) | 29 (46) | / | / | / | / | / |
| 1994–1998 | 57 (35) | 16 (26) | 41 (40) | 29 (35) | 19 (30) | 39 (56) | 11 (31) | 28 (82) | 20 (53) | 16 (59) |
| 1999–2004 | 23 (14) | 17 (27) | 6 (6) | 12 (14) | 9 (14) | 18 (26) | 12 (33) | 6 (18) | 11 (29) | 5 (19) |
| 2005–2012 | 17 (10) | 17 (27) | / | 11 (13) | 6 (10) | 13 (19) | 13 (36) | / | 7 (18) | 6 (22) |
| Characteristics | Cases (n = 164), n (%) | Controls (n = 1640), n (%) | Adj OR (95% CI) | Fully Adjusted OR (95% CI) |
|---|---|---|---|---|
| Season of birth | ||||
| May–September | 76 (46.4) | 700 (42.7) | 1.16 (0.84–1.60) | 1.19 (0.86–1.65) |
| October-April | 88 (53.7) | 940 (57.3) | 1 | 1 |
| Siblings | ||||
| Yes | 66 (40.2) | 762 (46.5) | 1 | 1 |
| No | 98 (59.8) | 878 (53.5) | 1.29 (0.93–1.79) | 1.21 (0.85–1.72) |
| Singleton/Multiple births | ||||
| 1 | 159 (97.0) | 1607 (98.0) | 1 | 1 |
| ≥2 | 5 (3.1) | 33 (2.0) | 1.54 (0.59–4.03) | 1.44 (0.49–4.18) |
| Birth weight | ||||
| ≥2500 | 154 (93.9) | 1563 (95.3) | 1 | 1 |
| <2500 | 10 (6.1) | 77 (4.7) | 1.31 (0.67–2.57) | 1.12 (0.42–3.00) |
| Gestational age, weeks | ||||
| ≥36 | 156 (95.7) | 1586 (97.1) | 1 | 1 |
| ≤35 | 7 (4.3) | 47 (2.9) | 1.50 (0.67–3.38) | 1.26 (0.40–4.03) |
| Apgar score | ||||
| ≥7 | 154 (93.9) | 1542 (94.1) | 1 | 1 |
| <7 | 10 (6.1) | 96 (5.9) | 1.05 (0.53–2.07) | 0.96 (0.47–1.96) |
| Maternal age, years | ||||
| <25 | 22 (13.4) | 196 (12.0) | 0.97 (0.58–1.62) | 0.97 (0.57–1.63) |
| 25–29 | 64 (39.0) | 547 (33.4) | 1 | 1 |
| 30–34 | 50 (30.5) | 586 (35.7) | 0.72 (0.49–1.07) | 0.76 (0.51–1.14) |
| 35–39 | 22 (113.4) | 273 (16.7) | 0.68 (0.41–1.14) | 0.74 (0.43–1.27) |
| ≥40 | 6 (3.7) | 38 (2.3) | 1.34 (80.54–3.31) | 1.55 (0.61–3.91) |
| Maternal education | ||||
| Primary/middle school | 62 (37.8) | 673 (41.2) | 1 | 1 |
| High school | 86 (52.4) | 765 (46.8) | 1.22 (0.86–1.72) | 1.23 (0.87–1.76) |
| University | 16 (9.8) | 195 (12.0) | 0.89 (0.50–1.58) | 0.96 (0.53–1.76) |
| Cases (n = 70), n (%) | Controls (n = 700), n (%) | Adj OR (95% CI) | Adj 2 OR (95% CI) | Adj 3 OR (95% CI) | |
|---|---|---|---|---|---|
| Antibiotic prescription in the first 6 months of life | |||||
| No | 52 (74.3) | 560 (80.0) | 1 | 1 | 1 |
| Yes | 18 (25.7) | 140 (20.0) | 1.38 (0.79–2.43) | 1.458 (0.81–2.63) | 1.45 (0.80–2.62) |
| 1 † | 6 (8.6) | 92 (13.1) | 0.70 (0.29–1.67) | 0.746 (0.31–1.81) | 0.74 (0.31–1.81) |
| 2–3 † | 8 (11.4) | 41 (5.9) | 2.09 (0.95–4.64) | 2.29 (1.01–5.24) | 2.31 (1.01–5.28) |
| ≥4 † | 4 (5.7) | 7 (1.0) | 6.07 (1.76–20.96) | 6.25 (1.70–23.05) | 6.34 (1.68–24.02) |
| Antibiotic prescription in the first 12 months of life | |||||
| No | 37 (52.9) | 380 (54.3) | 1 | 1 | 1 |
| Yes | 33 (47.1) | 320 (45.7) | 1.06 (0.65–1.73) | 1.08 (0.64–1.80) | 1.07 (0.64–1.79) |
| 1 † | 13 (18.6) | 164 (23.4) | 1.12 (0.57–2.18) | 0.80 (0.40–1.58) | 0.80 (0.40–1.58) |
| 2–3 † | 9 (12.9) | 116 (16.6) | 0.79 (0.37–1.70) | 0.87 (0.40–1.88) | 0.86 (0.40–1.87) |
| ≥4 † | 11 (15.7) | 40 (5.7) | 3.75 (1.69–8.32) | 2.92 (1.32–6.46) | 2.91 (1.31–6.45) |
| EO-IBD (1–9 Years) | P-IBD (10–17 Years) | |||||
|---|---|---|---|---|---|---|
| Cases (n = 36) n (%) | Controls (n = 360) n (%) | Adj 2 OR (95% CI) | Cases (n = 34), n (%) | Controls (n = 340), n (%) | Adj 2 OR (95% CI) | |
| Antibiotic prescription in the first 6 months of life | ||||||
| No | 24 (66.7) | 292 (81.1) | 1 (1–1) | 28 (82.4) | 268 (78.8) | 1 (1–1) |
| Yes | 12 (33.3) | 68 (18.9) | 2.36 (1.06–5.24) | 6 (17.7) | 72 (21.2) | 0.82 (0.31–2.13) |
| 1 † | 3 (8.3) | 48 (13.3) | 0.84 (0.24–2.99) | 3 (8.8) | 44 (12.9) | 0.64 (0.18–2.26) |
| 2–3 † | 6 (16.7) | 17 (4.7) | 5.83 (1.77–19.18) | 2 (5.9) | 24 (7.1) | 0.92 (0.21–4.12) |
| ≥4 † | 3 (8.3) | 3 (0.8) | 15.07 (2.45–92.63) | 1 (2.9) | 4 (1.2) | 2.43 (0.24–24.52) |
| Antibiotic prescription in the first 12 months of life | ||||||
| No | 17 (47.2) | 201 (55.8) | 1 (1–1) | 20 (58.8) | 179 (52.7) | 1 (1–1) |
| Yes | 36 (52.8) | 159 (44.2) | 1.43 (0.69–2.96) | 14 (41.2) | 161 (47.3) | 0.81 (0.37–1.76) |
| 1 † | 6 (16.7) | 84 (23.3) | 0.86 (0.31–2.36) | 7 (20.6) | 80 (23.5) | 0.74 (0.28–1.98) |
| 2–3 † | 3 (8.3) | 60 (16.7) | 0.64 (0.18–2.3) | 6 (17.7) | 56 (16.5) | 1.14 (0.41–3.15) |
| ≥4 † | 10 (27.8) | 15 (4.2) | 11.10 (3.41–36.13) | 1 (2.9) | 25 (7.4) | 0.37 (0.05–2.97) |
| Crohn’s Disease (n = 38) n (%) | Controls (n = 380) n (%) | Adj 2 OR (95% CI) | UC (n = 27) n (%) | Controls (n = 270) n (%) | Adj 2 OR (95% CI) | |
|---|---|---|---|---|---|---|
| Antibiotic prescription in the first 6 months of life | ||||||
| No | 25 (65.8) | 313 (82.4) | 1 (1–1) | 22 (81.48) | 207 (76.7) | 1 (1–1) |
| Yes | 13 (34.2) | 67 (17.6) | 2.61 (1.17–5.81) | 5 (18.52) | 63 (23.3) | 0.85 (0.29–2.52) |
| 1 † | 4 (10.5) | 40 (10.5) | 1.36 (0.42–4.34) | 2 (7.41) | 44 (16.3) | 0.48 (0.10–2.26) |
| 2–3 † | 5 (13.2) | 24 (6.3) | 3.30 (1.08–10.09) | 3 (11.11) | 15 (5.6) | 2.40 (0.55–10.47) |
| ≥4 † | 4 (10.5) | 3 (0.8) | 13.02 (2.47–68.47) | 0 (0) | 4 (1.5) | - |
| Antibiotic prescription in the first 12 months of life | ||||||
| No | 16 (42.1) | 208 (54.7) | 1 (1–1) | 18 (66.67) | 147 (54.4) | 1 (1–1) |
| Yes | 22 (57.9) | 172 (45.7) | 1.72 (0.84–3.53) | 9 (33.33) | 123 (45.6) | 0.72 (0.28–1.86) |
| 1 † | 8 (21.1) | 90 (23.7) | 1.26 (0.50–3.19) | 4 (14.81) | 61 (22.6) | 0.58 (0.17–1.97) |
| 2–3 † | 6 (15.8) | 60 (15.8) | 1.35 (0.49–3.70) | 3 (11.11) | 48 (17.8) | 0.71 (0.18–2.78) |
| ≥4 † | 8 (21.1) | 22 (5.8) | 4.86 (1.70–13.90) | 2 (7.41) | 14 (5.2) | 1.42 (0.25–7.97) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canova, C.; Ludvigsson, J.F.; Di Domenicantonio, R.; Zanier, L.; Barbiellini Amidei, C.; Zingone, F. Perinatal and Antibiotic Exposures and the Risk of Developing Childhood-Onset Inflammatory Bowel Disease: A Nested Case-Control Study Based on a Population-Based Birth Cohort. Int. J. Environ. Res. Public Health 2020, 17, 2409. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072409
Canova C, Ludvigsson JF, Di Domenicantonio R, Zanier L, Barbiellini Amidei C, Zingone F. Perinatal and Antibiotic Exposures and the Risk of Developing Childhood-Onset Inflammatory Bowel Disease: A Nested Case-Control Study Based on a Population-Based Birth Cohort. International Journal of Environmental Research and Public Health. 2020; 17(7):2409. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072409
Chicago/Turabian StyleCanova, Cristina, Jonas F Ludvigsson, Riccardo Di Domenicantonio, Loris Zanier, Claudio Barbiellini Amidei, and Fabiana Zingone. 2020. "Perinatal and Antibiotic Exposures and the Risk of Developing Childhood-Onset Inflammatory Bowel Disease: A Nested Case-Control Study Based on a Population-Based Birth Cohort" International Journal of Environmental Research and Public Health 17, no. 7: 2409. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072409