Impact of the Severities of Glaucoma on the Incidence of Subsequent Dementia: A Population-Based Cohort Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Declaration and Data Source
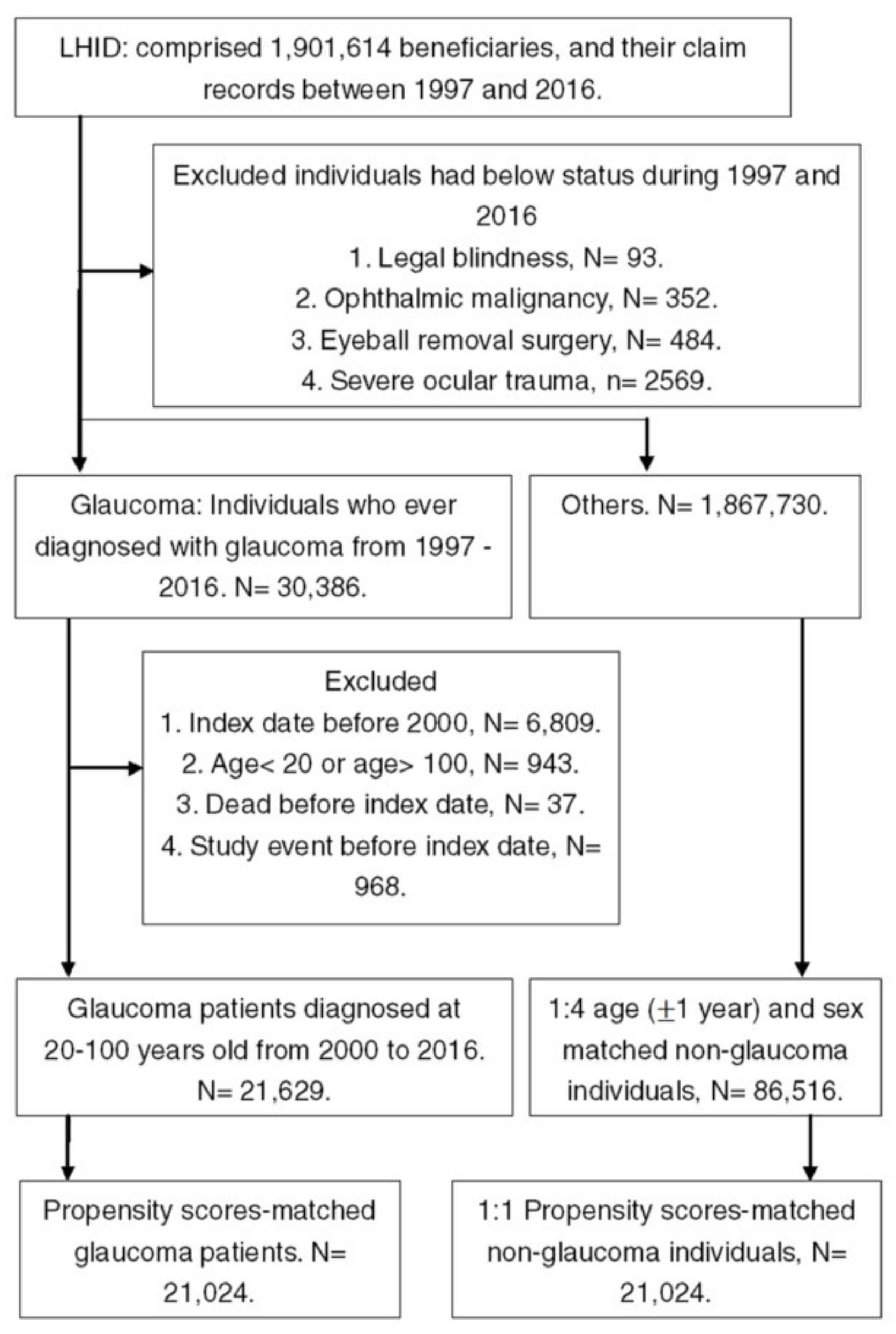
2.2. Subject Selection
2.3. Main Outcome Measurement
2.4. Demographic Variables and Co-Morbidities
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gale, S.A.; Acar, D.; Daffner, K.R. Dementia. Am. J. Med. 2018, 131, 1161–1169. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimers Dement. 2013, 9, 63–75.e62. [Google Scholar] [CrossRef] [PubMed]
- Mehta, K.M.; Yeo, G.W. Systematic review of dementia prevalence and incidence in United States race/ethnic populations. Alzheimers Dement. 2017, 13, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Zhang, P.; Liang, X.; Wu, Z.; Wang, J.; Liang, Y. Association between dementia and mortality in the elderly patients undergoing hip fracture surgery: A meta-analysis. J. Orthop. Surg. Res. 2018, 13, 298. [Google Scholar] [CrossRef]
- Cheng, H.L.; Lin, C.W.; Yang, J.S.; Hsieh, M.J.; Yang, S.F.; Lu, K.H. Zoledronate blocks geranylgeranylation not farnesylation to suppress human osteosarcoma u2os cells metastasis by emt via rho a activation and fak-inhibited jnk and p38 pathways. Oncotarget 2016, 7, 9742–9758. [Google Scholar] [CrossRef] [Green Version]
- Killin, L.O.; Starr, J.M.; Shiue, I.J.; Russ, T.C. Environmental risk factors for dementia: A systematic review. BMC Geriatr. 2016, 16, 175. [Google Scholar] [CrossRef] [Green Version]
- Sierra, C. Hypertension and the risk of dementia. Front. Cardiovasc. Med. 2020, 7, 5. [Google Scholar] [CrossRef] [Green Version]
- Strandberg, T.E.; Tienari, P.J.; Kivimaki, M. Vascular and alzheimer’s disease in dementia. Ann. Neurol. 2020. [Google Scholar] [CrossRef]
- Bellou, V.; Belbasis, L.; Tzoulaki, I.; Middleton, L.T.; Ioannidis, J.P.A.; Evangelou, E. Systematic evaluation of the associations between environmental risk factors and dementia: An umbrella review of systematic reviews and meta-analyses. Alzheimers Dement. 2017, 13, 406–418. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, F.T.; Hou, X.H.; Li, J.Q.; Cao, X.P.; Tan, L.; Wang, J.; Yu, J.T. Predictors of cognitive impairment in parkinson’s disease: A systematic review and meta-analysis of prospective cohort studies. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Ford, A.H.; Hankey, G.J.; Yeap, B.B.; Golledge, J.; Flicker, L.; Almeida, O.P. Hearing loss and the risk of dementia in later life. Maturitas 2018, 112, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Vitale, C.; Marcelli, V.; Abate, T.; Pianese, A.; Allocca, R.; Moccia, M.; Spina, E.; Barone, P.; Santangelo, G.; Cavaliere, M. Speech discrimination is impaired in parkinsonian patients: Expanding the audiologic findings of parkinson’s disease. Parkinsonism Relat. Disord. 2016, 22 (Suppl. 1), S138–S143. [Google Scholar] [CrossRef]
- Lee, A.T.C.; Richards, M.; Chan, W.C.; Chiu, H.F.K.; Lee, R.S.Y.; Lam, L.C.W. Higher dementia incidence in older adults with poor visual acuity. J. Gerontol. A Biol. Sci. Med. Sci. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rong, S.S.; Lee, B.Y.; Kuk, A.K.; Yu, X.T.; Li, S.S.; Li, J.; Guo, Y.; Yin, Y.; Osterbur, D.L.; Yam, J.C.S.; et al. Comorbidity of dementia and age-related macular degeneration calls for clinical awareness: A meta-analysis. Br. J. Ophthalmol. 2019, 103, 1777–1783. [Google Scholar] [CrossRef]
- Quigley, H.A. Glaucoma. Lancet 2011, 377, 1367–1377. [Google Scholar] [CrossRef]
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancino, R.; Martucci, A.; Cesareo, M.; Giannini, C.; Corasaniti, M.T.; Bagetta, G.; Nucci, C. Glaucoma and alzheimer disease: One age-related neurodegenerative disease of the brain. Curr. Neuropharmacol. 2018, 16, 971–977. [Google Scholar] [CrossRef]
- Sen, S.; Saxena, R.; Tripathi, M.; Vibha, D.; Dhiman, R. Neurodegeneration in alzheimer’s disease and glaucoma: Overlaps and missing links. Eye 2020. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef] [Green Version]
- Schneider, J.A.; Arvanitakis, Z.; Bang, W.; Bennett, D.A. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology 2007, 69, 2197–2204. [Google Scholar] [CrossRef]
- Wiels, W.; Baeken, C.; Engelborghs, S. Depressive symptoms in the elderly-an early symptom of dementia? A systematic review. Front. Pharmacol. 2020, 11, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, J.T.; Thomas, A. Vascular dementia. Lancet 2015, 386, 1698–1706. [Google Scholar] [CrossRef] [Green Version]
- Moretti, R.; Caruso, P. Small vessel disease-related dementia: An invalid neurovascular coupling? Int. J. Mol. Sci. 2020, 21, E1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dashtipour, K.; Tafreshi, A.; Lee, J.; Crawley, B. Speech disorders in parkinson’s disease: Pathophysiology, medical management and surgical approaches. Neurodegener. Dis. Manag. 2018, 8, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, U.; Colijn, J.M.; Ikram, M.A.; Bonnemaijer, P.W.M.; Licher, S.; Wolters, F.J.; Tiemeier, H.; Koudstaal, P.J.; Klaver, C.C.W.; Ikram, M.K. Association of retinal neurodegeneration on optical coherence tomography with dementia: A population-based study. JAMA Neurol. 2018, 75, 1256–1263. [Google Scholar] [CrossRef]
- Zabel, P.; Kaluzny, J.J.; Wilkosc-Debczynska, M.; Gebska-Toloczko, M.; Suwala, K.; Zabel, K.; Zaron, A.; Kucharski, R.; Araszkiewicz, A. Comparison of retinal microvasculature in patients with Alzheimer’s disease and primary open-angle glaucoma by optical coherence tomography angiography. Invest. Ophthalmol. Vis. Sci. 2019, 60, 3447–3455. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.; Liew, G.; Gopinath, B.; Wong, T.Y. Age-related macular degeneration. Lancet 2018, 392, 1147–1159. [Google Scholar] [CrossRef]
- Pohl, H.; Tarnutzer, A.A. Acute angle-closure glaucoma. N. Engl. J. Med. 2018, 378, e14. [Google Scholar] [CrossRef]
- Yerramothu, P.; Vijay, A.K.; Willcox, M.D.P. Inflammasomes, the eye and anti-inflammasome therapy. Eye 2018, 32, 491–505. [Google Scholar] [CrossRef]
- Wu, Y.T.; Beiser, A.S.; Breteler, M.M.B.; Fratiglioni, L.; Helmer, C.; Hendrie, H.C.; Honda, H.; Ikram, M.A.; Langa, K.M.; Lobo, A.; et al. The changing prevalence and incidence of dementia over time - Current evidence. Nat. Rev. Neurol. 2017, 13, 327–339. [Google Scholar] [CrossRef] [Green Version]
- Moon, J.Y.; Kim, H.J.; Park, Y.H.; Park, T.K.; Park, E.C.; Kim, C.Y.; Lee, S.H. Association between open-angle glaucoma and the risks of alzheimer’s and parkinson’s diseases in south korea: A 10-year nationwide cohort study. Sci. Rep. 2018, 8, 11161. [Google Scholar] [CrossRef] [PubMed]
- Su, C.W.; Lin, C.C.; Kao, C.H.; Chen, H.Y. Association between glaucoma and the risk of dementia. Medicine 2016, 95, e2833. [Google Scholar] [CrossRef] [PubMed]
- Killer, H.E.; Pircher, A. Normal tension glaucoma: Review of current understanding and mechanisms of the pathogenesis. Eye 2018, 32, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Huang, W.; Zhang, X. Efficacy and safety of different regimens for primary open-angle glaucoma or ocular hypertension: A systematic review and network meta-analysis. Acta Ophthalmol. 2018, 96, e277–e284. [Google Scholar] [CrossRef] [PubMed]
- Loughrey, D.G.; Kelly, M.E.; Kelley, G.A.; Brennan, S.; Lawlor, B.A. Association of age-related hearing loss with cognitive function, cognitive impairment, and dementia: A systematic review and meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 115–126. [Google Scholar] [CrossRef]
- Baumgart, M.; Snyder, H.M.; Carrillo, M.C.; Fazio, S.; Kim, H.; Johns, H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimers Dement. 2015, 11, 718–726. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Study | Control | ASD |
|---|---|---|---|
| N | 21024 | 21024 | |
| Age | 0.008 | ||
| 20–30 | 1109 (5.27%) | 1073 (5.10%) | |
| 30–40 | 1717 (8.17%) | 1632 (7.76%) | |
| 40–50 | 3112 (14.8%) | 2976 (14.16%) | |
| 50–60 | 4708 (22.39%) | 4672 (22.22%) | |
| 60–70 | 5126 (24.38%) | 5183 (24.65%) | |
| 70–80 | 3752 (17.85%) | 3919 (18.64%) | |
| 80–100 | 1500 (7.13%) | 1569 (7.46%) | |
| Sex | 0.055 | ||
| Male | 10,494 (49.91%) | 10,543 (50.15%) | |
| Female | 10,530 (50.09%) | 10,481 (49.85%) | |
| Education | 0.037 | ||
| <6 | 7467 (35.52%) | 7556 (35.94%) | |
| 6–9 | 3104 (14.76%) | 3047 (14.49%) | |
| 9–12 | 7350 (34.96%) | 7304 (34.74%) | |
| > = 12 | 3103 (14.76%) | 3117 (14.83%) | |
| Marry | 0.001 | ||
| Not marriage | 3464 (16.48%) | 3322 (15.80%) | |
| Marriage | 15,046 (71.57%) | 15,197 (72.28%) | |
| Divorce | 1123 (5.34%) | 1087 (5.17%) | |
| Death of spouse | 1391 (6.62%) | 1418 (6.74%) | |
| Co-morbidities | |||
| Hypertension | 7692 (36.59%) | 7918 (37.66%) | 0.022 |
| DM | 4858 (23.11%) | 4883 (23.23%) | 0.003 |
| Ischemic heart diseases | 1818 (8.65%) | 1863 (8.86%) | 0.008 |
| Hyperlipidemia | 4574 (21.76%) | 4603 (21.89%) | 0.003 |
| Congestive heart failure | 607 (2.89%) | 632 (3.01%) | 0.007 |
| Peripheral vascular disease | 331 (1.57%) | 342 (1.63%) | 0.004 |
| Cerebrovascular disease | 1399 (6.65%) | 1385 (6.59%) | 0.003 |
| SNHL | 101 (0.48%) | 97 (0.46%) | 0.003 |
| AMD | 479 (2.28%) | 471 (2.24%) | 0.003 |
| Hemiplegia or paraplegia | 136 (0.65%) | 107 (0.51%) | 0.018 |
| Study Event | Study | Control | Crude IRR (95% CI) | ||
|---|---|---|---|---|---|
| Event Number/ Person-months | Incidence Rate, per 1000 PMs (95% CI) | Event Number/ Person-Months | Incidence Rate, per 1000 PMs (95% CI) | ||
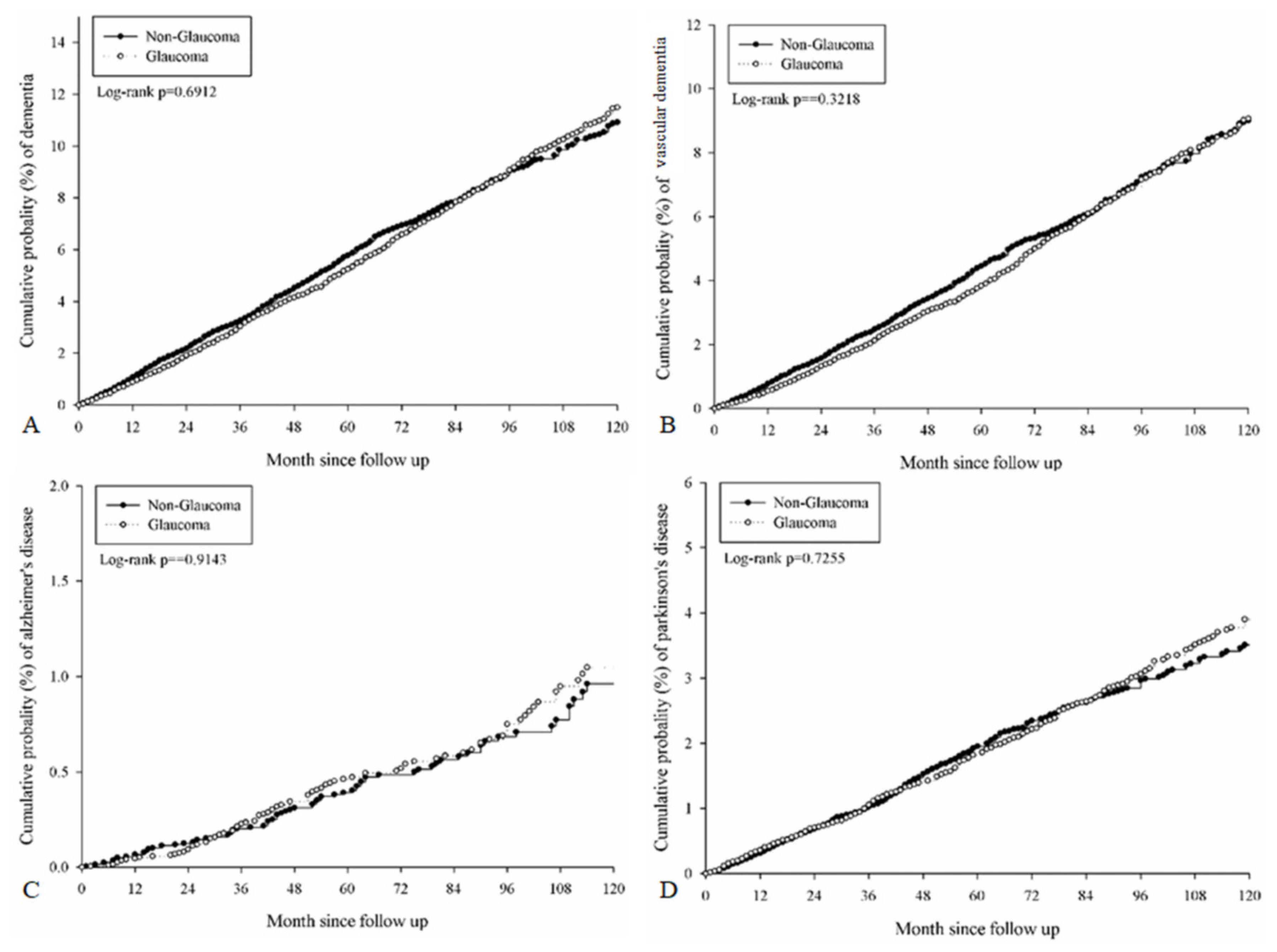
| Any dementia | 1185/1222688 | 9.69 (9.16–10.26) | 1119/1138846 | 9.83 (9.27–10.42) | 0.99 (0.91–1.07) |
| VD | 906/1234948 | 7.34 (6.87–7.83) | 878/1149290 | 7.64 (7.15–8.16) | 0.96 (0.88–1.05) |
| AD | 97/1262946 | 0.77 (0.63–0.94) | 86/1177323 | 0.73 (0.59–0.90) | 1.05 (0.79–1.41) |
| PD | 405/1249010 | 3.24 (2.94–3.57) | 368/1166108 | 3.16 (2.85–3.50) | 1.03 (0.89–1.18) |
| Parameters | aHR (95% CI) | p Value |
|---|---|---|
| Glaucoma for all dementia (ref = Control) | 0.961 (0.886–1.043) | 0.3443 |
| Glaucoma for VD | 0.928 (0.846–1.018) | 0.1154 |
| Glaucoma for AD | 1.018 (0.761–1.362) | 0.9025 |
| Glaucoma for PD | 1.021 (0.886–1.176) | 0.7744 |
| Age (ref = 50–60) | ||
| 20–30 | 0.106 (0.033–0.341) | 0.0002 |
| 30–40 | 0.099 (0.036–0.269) | <0.0001 |
| 40–50 | 0.293 (0.185–0.462) | <0.0001 |
| 60–70 | 4.681 (3.832–5.717) | <0.0001 |
| 70–80 | 11.244 (9.239–13.683) | <0.0001 |
| 80–100 | 18.864 (15.331–23.210) | <0.0001 |
| Sex (ref= Male) | ||
| Female | 1.064 (0.971–1.165) | 0.1826 |
| Education (ref = 9–12 years) | ||
| <6 | 0.996 (0.894–1.110) | 0.9492 |
| 6–9 | 0.870 (0.749–1.009) | 0.0663 |
| > = 12 | 0.906 (0.762–1.076) | 0.2612 |
| Marry (ref= not marriage) | ||
| Marriage | 0.975 (0.775–1.226) | 0.8276 |
| Divorce | 1.112 (0.823–1.503) | 0.4899 |
| Death of spouse | 1.097 (0.856–1.406) | 0.4642 |
| Co-morbidities | ||
| Hypertension | 1.160 (1.060–1.269) | 0.0013 |
| DM | 1.232 (1.123–1.351) | <0.0001 |
| Ischemic heart diseases | 1.196 (1.073–1.335) | 0.0013 |
| Hyperlipidemia | 1.003 (0.911–1.106) | 0.9457 |
| Congestive heart failure | 1.258 (1.063–1.490) | 0.0077 |
| Peripheral vascular disease | 1.204 (0.952–1.522) | 0.1204 |
| Cerebrovascular disease | 1.580 (1.410–1.771) | <0.0001 |
| SNHL | 1.543 (1.086–2.192) | 0.0155 |
| AMD | 0.981 (0.794–1.213) | 0.8596 |
| Hemiplegia or paraplegia | 1.849 (1.323–2.585) | 0.0003 |
| Events | aHR (95% CI) for Dementia | ||||
|---|---|---|---|---|---|
| Control N = 21024 | No more than Two Medications N = 16690 | More than Two Medications N = 3665 | Drainage Surgery N = 582 | Destructive Surgery N = 87 | |
| Any dementia | Reference | 0.930 (0.851–1.017) | 1.043 (0.913–1.192) | 1.186 (0.886–1.589) | 0.820 (0.389–1.727) |
| VD | Reference | 0.886 (0.800–0.981) | 1.049 (0.903–1.218) | 1.168 (0.840–1.623) | 0.736 (0.305–1.776) |
| AD | Reference | 1.027 (0.751–1.404) | 1.044 (0.647–1.683) | 0.575 (0.141–2.338) | 1.677 (0.232–12.125) |
| PD | Reference | 0.989 (0.849–1.153) | 1.131 (0.902–1.419) | 1.183 (0.706–1.984) | 0.366 (0.051–2.606) |
| Events | aHR (95% CI) for Dementia | |||
|---|---|---|---|---|
| Control | OAG | NTG | ACG | |
| Any dementia | Reference | 0.874 (0.761–1.004) | 1.169 (0.977–1.399) | 0.913 (0.814–1.024) |
| VD | Reference | 0.833 (0.709–0.977) | 1.073 (0.869–1.325) | 0.899 (0.791–1.023) |
| AD | Reference | 0.825 (0.490–1.390) | 0.928 (0.449–1.916) | 0.927 (0.622–1.381) |
| PD | Reference | 0.982 (0.780–1.236) | 1.440 (1.086–1.909) | 0.962 (0.786–1.176) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, F.-H.; Chung, J.-F.; Hsu, M.-Y.; Lee, C.-Y.; Huang, J.-Y.; Hsieh, M.-J.; Yang, S.-F. Impact of the Severities of Glaucoma on the Incidence of Subsequent Dementia: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 2426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072426
Kuo F-H, Chung J-F, Hsu M-Y, Lee C-Y, Huang J-Y, Hsieh M-J, Yang S-F. Impact of the Severities of Glaucoma on the Incidence of Subsequent Dementia: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(7):2426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072426
Chicago/Turabian StyleKuo, Fu-Hsuan, Jui-Fu Chung, Min-Yen Hsu, Chia-Yi Lee, Jing-Yang Huang, Ming-Ju Hsieh, and Shun-Fa Yang. 2020. "Impact of the Severities of Glaucoma on the Incidence of Subsequent Dementia: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 17, no. 7: 2426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072426