Effects of Brain Breaks Videos on the Motives for the Physical Activity of Malaysians with Type-2 Diabetes Mellitus

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
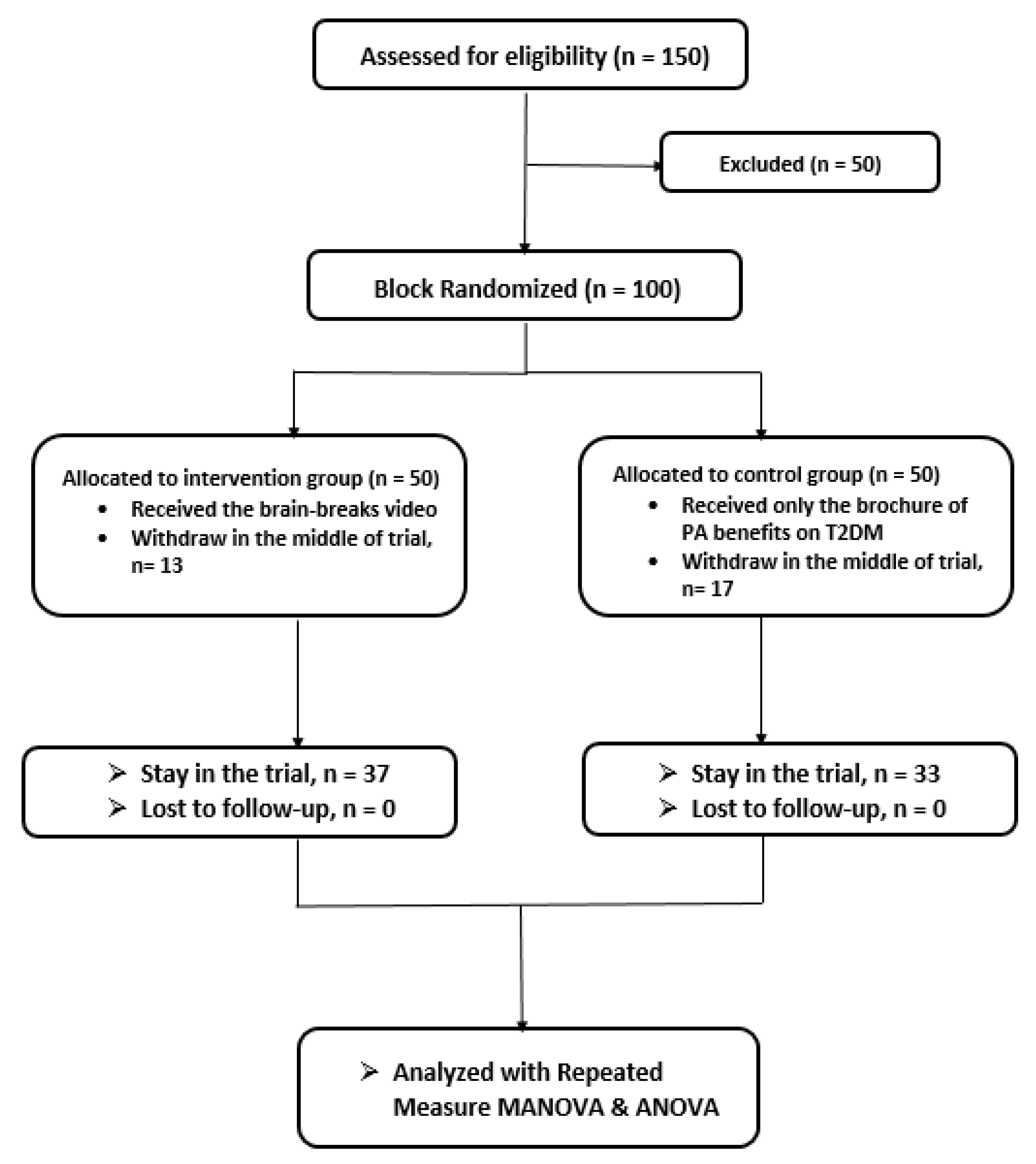
2.1. Study Design and Recruitment
2.2. Participants
2.3. Procedures
2.4. Instruments
- (a)
- Physical Activity and Leisure Motivation Scale-Malay (PALMS-M)
- (b)
- Malay Version of International Physical Activity Questionnaire (IPAQ-M)
2.5. Data Analysis
3. Results
3.1. Effects on Patients’ Motives for PA
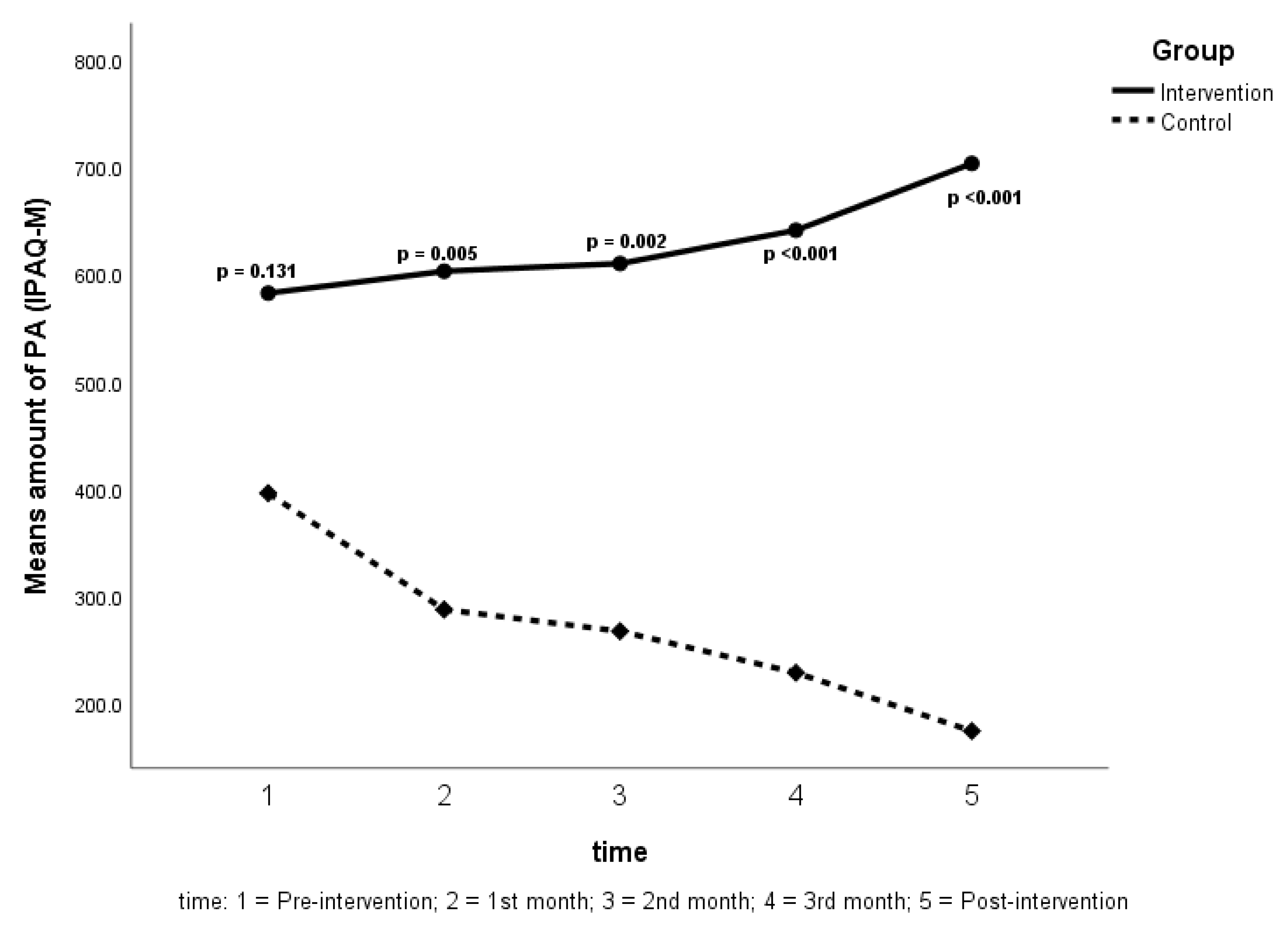
3.2. Effects on the Patients’ Amount of PA
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kokkinos, P.; Myers, J. Exercise and physical activity: Clinical outcomes and applications. Circulation 2010, 122, 1637–1648. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Macera, C.A. Physical Activity and Public Health Practice; CRC Press: New York, NY, USA, 2012. [Google Scholar]
- Fletcher, G.F.; Balady, G.; Blair, S.N.; Blumenthal, J.; Caspersen, C.; Chaitman, B.; Epstein, S.; Froelicher, E.S.S.; Froelicher, V.F.; Pina, I.L.; et al. Statement on exercise: Benefits and recommendations for physical activity programs for all Americans: A statement for health professionals by the Committee on Exercise and Cardiac Rehabilitation of the Council on Clinical Cardiology. Am. Heart Assoc. Circ. 1996, 94, 857–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, K.N.; Majeed, Z.; Yoruk, Y.B.; Yang, H.; Hilton, T.N.; McMahon, J.M.; Hall, W.J.; Walck, D.; Luque, A.E.; Ryan, R.M. Enhancing physical function in HIV-infected older adults: A randomized controlled clinical trial. Health Psychol. 2016, 35, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Beekman, E.; Mesters, I.; Hendriks, E.J.; Muris, J.W.; Wesseling, G.; Evers, S.M.; Asijee, G.M.; Fastenau, A.; Hoffenkamp, H.N.; Gosselink, R.; et al. Exacerbations in patients with chronic obstructive pulmonary disease receiving physical therapy: A cohort-nested randomised controlled trial. BMC Pulm. Med. 2014, 14, 71–84. [Google Scholar] [CrossRef] [Green Version]
- Pinto, B.M.; Papandonatos, G.D.; Goldstein, M.G. A randomized trial to promote physical activity among breast cancer patients. Health Psychol. 2013, 32, 616–626. [Google Scholar] [CrossRef]
- Poh, B.K.; Safiah, M.; Tahir, A.; Siti Haslinda, N.; Siti Norazlin, N.; Norimah, A.; Wan Manan, W.M.; Mirnalini, K.; Zalilah, M.S.; Azmi, M.Y.; et al. Physical activity pattern and energy expenditure of Malaysian adults: Findings from the Malaysian adult nutrition survey (MANS). Malays. J. Nutr. 2010, 16, 13–37. [Google Scholar]
- Institute for Public Health. National Health and Morbidity Survey 2015: Non-Communicable Diseases, Risk Factors & Other Health Problems; Ministry of Health Malaysia: Kuala Lumpur, Malaysia, 2015; Volume II, NMRR-14-1064-21877.
- National Health and Morbidity Survey (NHMS) 2017. Key Findings from the Adolescent; Health and Nutrition Surveys, Ministry of Health Malaysia: Kuala Lumpur, Malaysia, 2018. Available online: http://iku.moh.gov.my/images/IKU/Document/REPORT/NHMS2017/NHMS2017Infographic.pdf (accessed on 2 February 2020).
- Gordon-Larsen, P.; Adair, L.S.; Nelson, M.C.; Popkin, B.M. Five-year obesity incidence in the transition period between adolescence and adulthood: The national longitudinal study of adolescent health. Am. J. Clin. Nutr. 2004, 80, 569–575. [Google Scholar]
- World Health Organization. Diabetes. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 2 February 2020).
- Mustaffa, B. Diabetes epidemic in Malaysia. Med. J. Malays. 2004, 59, 295–296. [Google Scholar]
- Tee, E.; Yap, R. Type 2 diabetes mellitus in Malaysia: Current trends and risk factors. Eur. J. Clin. Nutr. 2017, 71, 844–849. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 2 February 2020).
- Gould, D.; Dieffenbach, K.; Moffett, A. Psychological characteristics and their development in Olympic champions. J. Appl. Sport Psychol. 2002, 14, 172–204. [Google Scholar] [CrossRef]
- Aaltonen, S.; Leskinen, T.; Morris, T.; Alen, M.; Kaprio, J.; Liukkonen, J.; Kujala, U. Motives for and barriers to physical activity in twin pairs discordant for leisure time physical activity for 30 years. Int. J. Sports Med. 2012, 33, 157–163. [Google Scholar] [CrossRef] [PubMed]
- André, N.; Dishman, R.K. Evidence for the construct validity of self-motivation as a correlate of exercise adherence in French older adults. J. Aging Phys. Act. 2012, 20, 231–245. [Google Scholar] [CrossRef]
- Vallerand, R.J. Intrinsic and extrinsic motivation in sport and physical activity. Handb. Sport Psychol. 2007, 3, 59–83. [Google Scholar]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Nicholls, J.G. The Competitive Ethos and Democratic Education; Harvard University Press: London, UK, 1989. [Google Scholar]
- Kilpatrick, M.; Hebert, E.; Bartholomew, J. College students’ motivation for physical activity: Differentiating men’s and women’s motives for sport participation and exercise. J. Am. Coll. Health 2005, 54, 87–94. [Google Scholar] [CrossRef]
- Frederick, C.M.; Ryan, R.M. Differences in motivation for sport and exercise and their relations with participation and mental health. J. Sport Behav. 1993, 16, 124. [Google Scholar]
- Rogers, H.; Morris, T. New approaches to exercise and sport psychology: Theories, methods and applications. In An Overview of the Development and Validation of the Recreational Exercise Motivation Measure (REMM). In Proceedings of the XIth European Congress of Sport Psychology, Copenhagen, Denmark, 22–27 July 2003. [Google Scholar]
- Hu, L.; Morris, T.; Lu, J.; Zhu, L.; Zhang, T.; Chen, L. Development and validation of a youth version of physical activity and lesuire motivation scale (PALMS-Y). In Proceedings of the 14th European Congress of Sport Psychology, Bern, Switzerland, 14–19 July 2015. [Google Scholar]
- Kueh, Y.C.; Kuan, G.; Morris, T. The physical activity and leisure motivation scale: A confirmatory study of the Malay language version. Int. J. Sport Exerc. Psychol. 2019, 17, 250–265. [Google Scholar] [CrossRef]
- Tan, M.Y.; Magarey, J. Self-care practices of Malaysian adults with diabetes and sub-optimal glycaemic control. Patient Educ. Couns. 2008, 72, 252–267. [Google Scholar] [CrossRef]
- Jan Mohamed, H.J.B.; Yap, R.W.K.; Loy, S.L.; Norris, S.A.; Biesma, R.; Aagaard-Hansen, J. Prevalence and determinants of overweight, obesity, and type 2 diabetes mellitus in adults in Malaysia. Asia Pac. J. Public Health 2015, 27, 123–135. [Google Scholar] [CrossRef]
- Mendoza, L.; Horta, P.; Espinoza, J.; Aguilera, M.; Balmaceda, N.; Castro, A.; Ruiz, M.; Díaz, O.; Hopkinson, N.S. Pedometers to enhance physical activity in COPD: A randomised controlled trial. Eur. Respir. J. 2015, 45, 347–354. [Google Scholar] [CrossRef] [Green Version]
- Simmons, D.; Jelsma, J.G.; Galjaard, S.; Devlieger, R.; Van Assche, A.; Jans, G.; Corcoy, R.; Adelantado, J.M.; Dunne, F.; Desoye, G.; et al. Results from a European multicenter randomized trial of physical activity and/or healthy eating to reduce the risk of gestational diabetes mellitus: The DALI lifestyle pilot. Diabetes Care 2015, 38, 1650–1656. [Google Scholar] [CrossRef] [Green Version]
- Travier, N.; Velthuis, M.J.; Bisschop, C.N.S.; Van den Buijs, B.; Monninkhof, E.M.; Backx, F.; Los, M.; Erdkamp, F.; Bloemendal, H.J.; Rodenhuis, C.; et al. Effects of an 18-week exercise programme started early during breast cancer treatment: A randomised controlled trial. BMC Med. 2015, 13, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassidy, S.; Thoma, C.; Hallsworth, K.; Parikh, J.; Hollingsworth, K.G.; Taylor, R.; Jakovljevic, D.G.; Trenel, M.I. High intensity intermittent exercise improves cardiac structure and function and reduces liver fat in patients with type 2 diabetes: A randomised controlled trial. Diabetologia 2016, 59, 56–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Interactive Youth Physical Education Training System: HopSports. 2014. Available online: http://www.hopsports.com (accessed on 15 February 2020).
- Kuan, G.; Rizal, H.; Hajar, M.S.; Chin, M.-K.; Mok, M. Bright sports, physical activity investments that work: Implementing brain breaks in Malaysian primary schools. Br. J. Sports Med. 2019, 1, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Rizal, H.; Hajar, M.S.; Muhamad, A.S.; Kueh, Y.C.; Kuan, G. The effect of brain breaks on physical activity behaviour among primary school children: A transtheoretical perspective. Int. J. Environ. Res. Public Health 2019, 16, 4283. [Google Scholar] [CrossRef] [Green Version]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [Green Version]
- Hajar, M.S.; Rizal, H.; Kueh, Y.C.; Muhamad, A.S.; Kuan, G. The effects of brain breaks on motives of participation in physical activity among primary school children in Malaysia. Int. J. Environ. Res. Public Health 2019, 16, 2331. [Google Scholar] [CrossRef] [Green Version]
- Biddle, S.J.; Mutrie, N. Psychology of Physical Activity: Determinants, Well-Being and Interventions; Routledge: New York, NY, USA, 2007. [Google Scholar]
- Ebben, W.; Brudzynski, L. Motivations and barriers to exercise among college students. J. Exerc. Physiol. Online 2008, 11, 1–11. [Google Scholar]
- Aaltonen, S.; Rottensteiner, M.; Kaprio, J.; Kujala, U.M. Motives for physical activity among active and inactive persons in their mid-30s. Scand. J. Med. Sci. Sports 2014, 24, 727–735. [Google Scholar] [CrossRef] [Green Version]
- Duda, J.L. Goals and achievement orientations of Anglo and Mexican-American adolescents in sport and the classroom. Int. J. Intercult. Relat. 1985, 9, 131–150. [Google Scholar] [CrossRef]
- Duda, J.L. Perceptions of sport success and failure among white, black, and Hispanic adolescents. In Sport Science; Watkins, J., Reilly, T., Burwitz, L., Eds.; E. & F.N Spon: London, UK, 1986; pp. 214–222. [Google Scholar]
- Li, F.; Harmer, P.; Chi, L.; Vongjaturapat, N. Cross-cultural validation of the task and ego orientation in sport questionnaire. J. Sport Exerc. Psychol. 1996, 18, 392–407. [Google Scholar] [CrossRef]
- Zach, S.; Bar-Eli, M.; Morris, T.; Moore, M. Measuring motivation for physical activity: An exploratory study of PALMS-the physical activity and leisure motivation scale. Athl. Insight 2012, 4, 141–152. [Google Scholar]
- Caglar, E.; Canlan, Y.; Demir, M. Recreational exercise motives of adolescents and young adults. J. Hum. Kinet. 2009, 22, 83–89. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 7th ed.; Pearson: Edinburgh, UK, 2019. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Mean (SD) | Frequency (%) |
|---|---|---|
| Age | 57.6 (8.5) | |
| Group | ||
| Experimental | 37 (52.9) | |
| Control | 33 (47.1) | |
| Gender | ||
| Male | 39 (55.7) | |
| Female | 31 (44.3) | |
| Ethnicity | ||
| Malay | 63 (9.0) | |
| Chinese | 4 (5.7) | |
| Indian | 1 (1.4) | |
| Others | 2 (2.9) |
| PALMS-M Motives | Mean (SD) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Intervention | 1st Month | 2nd Month | 3rd Month | Post-Intervention | ||||||
| Exp a | Con b | Exp a | Con b | Exp a | Con b | Exp a | Con b | Exp a | Con b | |
| Competition | 15.05 (0.76) | 17.67 (0.56) | 16.78 (0.60) | 17.48 (0.55) | 18.62 (0.44) | 17.42 (0.54) | 20.57 (0.32) | 17.09 (0.52) | 20.92 (0.32) | 16.45 (0.46) |
| Appearance | 17.22 (0.78) | 15.21 (0.77) | 17.30 (0.77) | 15.12 (0.75) | 17.30 (0.77) | 15.06 (0.73) | 17.62 (0.68) | 14.94 (0.71) | 18.16 (0.57) | 14.58 (0.63) |
| Others’ expectation | 14.49 (0.53) | 16.36 (0.34) | 16.16 (0.43) | 16.18 (0.37) | 18.16 (0.34) | 15.88 (0.36) | 20.57 (0.30) | 15.55 (0.35) | 20.89 (0.30) | 15.09 (0.32) |
| Affiliation | 15.43 (0.71) | 15.09 (0.60) | 15.51 (0.70) | 15.00 (0.58) | 15.51 (0.70) | 15.00 (0.58) | 16.11 (0.61) | 14.91 (0.54) | 16.68 (0.58) | 14.73 (0.49) |
| Physical condition | 19.89 (0.51) | 18.67 (0.71) | 19.89 (0.51) | 18.42 (0.67) | 19.89 (0.51) | 18.27 (0.65) | 20.00 (0.49) | 18.03 (0.62) | 20.43 (0.47) | 17.52 (0.54) |
| Psychological condition | 18.05 (0.51) | 17.48 (0.72) | 18.14 (0.50) | 17.27 (0.68) | 18.14 (0.50) | 17.24 (0.67) | 18.24 (0.49) | 17.03 (0.62) | 19.00 (0.44) | 16.45 (0.53) |
| Mastery | 16.78 (0.65) | 15.00 (0.72) | 16.81 (0.65) | 14.94 (0.71) | 16.81 (0.65) | 14.94 (0.71) | 17.03 (0.60) | 14.88 (0.68) | 17.70 (0.55) | 14.58 (0.60) |
| Enjoyment | 17.14 (0.61) | 16.64 (0.70) | 17.19 (0.60) | 16.58 (0.69) | 17.19 (0.64) | 16.58 (0.69) | 17.27 (0.59) | 16.33 (0.62) | 17.89 (0.55) | 15.91 (0.56) |
| Comparison on PALMS-M Motives (Experimental and Control Groups) | Mean Difference (95% CI) | p-Value |
|---|---|---|
| Competition | 1.17 (−0.19, 2.52) | 0.090 |
| Appearance | 2.54 * (0.53, 4.55) | 0.014 |
| Others’ expectation | 2.24 * (1.27, 3.21) | <0.001 |
| Affiliation | 0.90 (−0.81, 2.62) | 0.297 |
| Physical condition | 1.84 * (0.26, 3.42) | 0.023 |
| Psychological condition | 1.21 (−0.35, 2.78) | 0.125 |
| Mastery | 2.16 * (0.33, 3.98) | 0.021 |
| Enjoyment | 0.93 (−0.80, 2.66) | 0.288 |
| Comparison | Competition | Appearance | Others’ Expectation | Affiliation | Physical Condition | Psychological Condition | Mastery | Enjoyment | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | |
| Pre vs. 1st month | −1.73 * (−2.41, −1.05) | <0.001 | −0.08 (−0.22, 0.06) | 0.831 | −1.68 * (−2.20, −1.16) | <0.001 | −0.08 (−0.22, 0.06) | 0.831 | 0.00 (-) | - | −0.08 (−0.22, 0.06) | 0.831 | −0.03 (−0.11, 0.05) | 1.000 | −0.05 (−0.17, 0.06) | 1.000 |
| Pre vs. 2nd month | −3.57 * (−4.92, −2.21) | <0.001 | −0.08 (−0.22, 0.06) | 0.831 | −3.68 * (−4.55, −2.80) | <0.001 | −0.08 (−0.22, 0.06) | 0.831 | 0.00 (-) | - | −0.08 (−0.22, 0.06) | 0.831 | −0.03 (−0.11, 0.05) | 1.000 | −0.05 (−0.17, 0.06) | 1.000 |
| Pre vs. 3rd month | −5.51 * (−7.39, −3.64) | <0.001 | −0.41 (−0.99, 0.18) | 0.453 | −6.08 * (−7.22, −4.94) | <0.001 | −0.68 * (−1.30, −0.05) | 0.026 | −0.11 (−0.30, 0.09) | 1.000 | −0.19 (−0.47, 0.91) | 0.508 | −0.24 (−0.62, 0.13) | 0.595 | −0.14 (−0.37, 0.10) | 0.960 |
| Pre vs. post intervention | −5.87 * (−7.83, −3.90) | <0.001 | −0.95 (−1.98, 0.90) | 0.097 | −6.40 * (−7.65, −5.16) | <0.001 | −1.24 * (−2.48, −0.01) | 0.047 | −0.54 (−1.19, 0.11) | 0.179 | −0.95 * (−1.85, −0.04) | 0.035 | −0.92 * (−1.71, −0.07) | 0.025 | −0.76 * (−1.39, −0.13) | 0.009 |
| 1st month vs. 2nd month | −1.84 * (−2.64, −1.04) | <0.001 | 0.00 (-) | - | −2.00 * (−2.53, −1.47) | <0.001 | 0.00 (-) | - | 0.00 (-) | - | 0.00 (-) | - | 0.00 (-) | - | 0.00 (-) | - |
| 1st month vs. 3rd month | −3.78 * (−5.11, −2.46) | <0.001 | −0.32 (−0.86, 0.21) | 0.764 | −4.41 * (−5.31, −3.50) | <0.001 | −0.60 * (−1.17, −0.02) | 0.037 | −0.11 (−0.30, 0.09) | 1.000 | −0.11 (−0.26, 0.05) | 0.438 | −0.22 (−0.53, 0.09) | 0.438 | −0.08 (−0.26, 0.10) | 1.000 |
| 1st month vs. post | −4.14 * (−5.57, −2.71) | <0.001 | −0.87 (−1.87, 0.14) | 0.143 | −4.73 * (−5.70, −3.76) | <0.001 | −1.16 (−2.33, 0.01) | 0.052 | −0.54 (−1.19, 0.11) | 0.179 | −0.87 (−1.73, 0.01) | 0.052 | −0.89 * (−1.71, −0.07) | 0.024 | −0.70 * (−1.31, −0.09) | 0.015 |
| 2nd month vs. 3rd month | −1.95 * (−2.64, −1.25) | <0.001 | −0.32 (−0.86, 0.21) | 0.764 | −2.41 * (−2.98, −1.83) | <0.001 | −0.60 * (−1.17, −0.02) | 0.037 | −0.11 (−0.30, 0.09) | 1.000 | −0.11 (−0.26, 0.05) | 0.438 | −0.22 (−0.53, 0.09) | 0.438 | −0.08 (−0.26, 0.10) | 1.000 |
| 2nd month vs. post | −2.30 * (−3.15, −1.45) | <0.001 | −0.87 (−1.87, 0.14) | 0.143 | −2.73 * (−3.31, −2.14) | <0.001 | −1.16 (−2.33, 0.01) | 0.052 | −0.54 (−1.19, 0.11) | 0.179 | −0.87 (−1.73, 0.01) | 0.052 | −0.89 * (−1.71, −0.07) | 0.024 | −0.70 * (−1.31, −0.09) | 0.015 |
| 3rd month vs. post | −0.35 (−0.76, 0.05) | 0.136 | −0.54 (−1.21, 0.13) | 0.214 | −0.32 (−0.71, 0.06) | 0.164 | −0.57 (−1.38, 0.23) | 0.406 | −0.43 (−1.06, 0.20) | 0.474 | −0.76 (−1.61, 0.10) | 0.120 | −0.68 * (−1.31, −0.04) | 0.030 | −0.62 * (−1.21, −0.04) | 0.030 |
| Comparison | Competition | Appearance | Others’ Expectation | Affiliation | Physical Condition | Psychological Condition | Mastery | Enjoyment | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | MD (95% CI) | p-value | |
| Pre vs. 1st month | 0.18 (−0.06, 0.43) | 0.316 | 0.09 (−0.06, 0.24) | 0.831 | 0.18 (0.02, 0.39) | 0.119 | 0.09 (−0.11, 0.29) | 1.000 | 0.24 (−0.05, 0.54) | 0.184 | 0.21 (−0.74, 0.50) | 0.326 | 0.06 (−0.07, 0.19) | 1.000 | 0.06 (−0.07, 0.19) | 1.000 |
| Pre vs. 2nd month | 0.24 (−0.08, 0.57) | 0.302 | 0.15 (−0.80, 0.38) | 0.575 | 0.49 * (0.16, 0.81) | 0.001 | 0.09 (−0.11, 0.29) | 1.000 | 0.39 * (0.01, 0.79) | 0.048 | 0.24 (−0.05, 0.54) | 0.184 | 0.06 (−0.07, 0.19) | 1.000 | 0.06 (−0.07, 0.19) | 1.000 |
| Pre vs. 3rd month | 0.58 * (0.08, 1.07) | 0.013 | 0.27 (−0.06, 0.60) | 0.176 | 0.82 * (0.34, 1.30) | <0.001 | 0.18 (−0.15, 0.52) | 1.000 | 0.64 * (0.15, 1.12) | 0.004 | 0.46 (−0.02, 0.93) | 0.069 | 0.12 (−0.10, 0.34) | 1.000 | 0.30 (−0.14, 0.75) | 0.482 |
| Pre vs. post intervention | 1.21 * (0.43, 1.99) | 0.001 | 0.64 (−0.01, 1.28) | 0.052 | 1.27 * (0.76, 1.79) | <0.001 | 0.36 (−0.22, 0.95) | 0.697 | 1.15 * (0.41, 1.90) | 0.001 | 1.03 * (0.04, 2.02) | 0.035 | 0.42 (−0.28, 1.13) | 0.798 | 0.73 (−0.04, 1.50) | 0.075 |
| 1st month vs. 2nd month | 0.06 (−0.07, 0.19) | 1.000 | 0.06 (−0.07, 0.19) | 1.000 | 0.30 * (0.76, 0.55) | 0.007 | 0.00 (-) | - | 0.15 (−0.08, 0.38) | 0.575 | 0.03 (−0.06, 0.12) | 1.000 | 0.00 (-) | - | 0.00 (-) | - |
| 1st month vs. 3rd month | 0.39 (−0.02, 0.81) | 0.072 | 0.18 (−0.10, 0.46) | 0.564 | 0.64 * (0.76, 1.07) | 0.001 | 0.09 (−0.18, 0.37) | 1.000 | 0.39 * (0.05, 0.74) | 0.017 | 0.24 (−0.11, 0.59) | 0.436 | 0.06 (−0.07, 0.19) | 1.000 | 0.24 (−0.17, 0.66) | 0.882 |
| 1st month vs. post | 1.03 * (−0.28, 1.78) | 0.002 | 0.55 (−0.07, 1.16) | 0.119 | 1.09 * (0.59, 1.59) | <0.001 | 0.27 (−0.19, 0.73) | 0.831 | −0.91 * (−1.54, −0.28) | 0.001 | 0.82 (−0.01, 1.64) | 0.053 | 0.36 (−0.25, 0.98) | 0.831 | 0.67 (−0.07, 1.41) | 0.104 |
| 2nd month vs. 3rd month | 0.33 (−0.05, 0.72) | 0.139 | 0.12 (−0.10, 0.34) | 1.000 | 0.33 * (0.20, 0.65) | 0.030 | 0.09 (−0.18, 0.37) | 1.000 | 0.24 (−0.02, 0.51) | 0.091 | 0.21 (−0.07, 0.50) | 0.326 | 0.06 (−0.07, 0.19) | 1.000 | 0.24 (−0.17, 0.66) | 0.882 |
| 2nd month vs. post | 0.97 * (0.23, 1.71) | 0.004 | 0.49 (−0.06, 1.03) | 0.112 | 0.79 * (0.36, 1.22) | <0.001 | 0.27 (−0.19, 0.73) | 0.831 | 0.76 * (0.19, 1.33) | 0.004 | 0.79 * (0.01, 1.56) | 0.043 | 0.36 (−0.25, 0.98) | 0.831 | 0.67 (−0.07, 1.41) | 0.104 |
| 3rd month vs. post | 0.64 * (0.15, 1.12) | 0.004 | 0.36 (−0.07, 0.80) | 0.161 | 0.46 * (0.16, 0.75) | 0.001 | 0.18 (−0.13, 0.49) | 0.184 | 0.52 * (0.06, 0.97) | 0.018 | 0.58 * (0.02, 1.13) | 0.039 | 0.30 (−0.20, 0.80) | 0.766 | 0.42 * (0.03, 0.82) | 0.028 |
| Motives | Time | Groups | Mean (95% CI) | Motives | Time | Groups | Mean (95% CI) |
|---|---|---|---|---|---|---|---|
| Competition | Pre-intervention | Experimental | 15.05 (13.74, 16.37) | Physical condition | Pre-intervention | Experimental | 19.89 (18.71,21.07) |
| Control | 17.67 (16.28,19.06) | Control | 18.67 (17.42, 19.92) | ||||
| 1st month | Experimental | 16.78 (15.66, 17.91) | 1st month | Experimental | 19.89 (18.75, 21.04) | ||
| Control | 17.49 (16.29, 18.68) | Control | 18.42 (17.21, 19.64) | ||||
| 2nd month | Experimental | 18.62 (17.67, 19.58) | 2nd month | Experimental | 19.89 (18.77, 21.01) | ||
| Control | 17.42 (16.41, 18.68) | Control | 18.27 (17.08, 19.46) | ||||
| 3rd month | Experimental | 20.57 (19.75, 21.38) | 3rd month | Experimental | 20.00 (18.93, 21.07) | ||
| Control | 17.09 (16.23, 17.95) | Control | 18.03 (16.90, 19.17) | ||||
| Post-intervention | Experimental | 20.92 (20.17, 21.67) | Post-intervention | Experimental | 20.43 (19.45, 21.41) | ||
| Control | 16.46 (15.66, 17.25) | Control | 17.52 (16.48, 18.56) | ||||
| Appearance | Pre-intervention | Experimental | 17.22 (15.71, 18.72) | Psychological condition | Pre-intervention | Experimental | 18.05 (16.86, 19.25) |
| Control | 15.21 (13.62, 16.81) | Control | 17.48 (16.22, 18.75) | ||||
| 1st month | Experimental | 17.30 (15.81, 18.78) | 1st month | Experimental | 18.13 (17.00, 19.27) | ||
| Control | 15.12 (13.55, 16.69) | Control | 17.27 (16.07, 18.48) | ||||
| 2nd month | Experimental | 17.30 (15.83, 18.76) | 2nd month | Experimental | 18.14 (17.01, 19.26) | ||
| Control | 15.06 (13.51, 16.61) | Control | 17.24 (16.05, 18.44) | ||||
| 3rd month | Experimental | 17.62 (16.27, 18.97) | 3rd month | Experimental | 18.24 (17.17, 19.32) | ||
| Control | 14.94 (13.51, 16.37) | Control | 17.03 (15.89, 18.17) | ||||
| Post-intervention | Experimental | 18.16 (17.00, 19.32) | Post-intervention | Experimental | 19.00 (18.07, 19.93) | ||
| Control | 14.58 (13.35, 15.80) | Control | 16.46 (15.47, 17.44) | ||||
| Others’ expectation | Pre-intervention | Experimental | 14.49 (13.61, 15.37) | Mastery | Pre-intervention | Experimental | 16.78 (15.45, 18.12) |
| Control | 16.36 (15.43, 17.30) | Control | 15.00 (13.59, 16.41) | ||||
| 1st month | Experimental | 16.16 (15.39, 16.94) | 1st month | Experimental | 16.81 (15.50, 18.12) | ||
| Control | 16.18 (15.36, 17.01) | Control | 14.94 (13.55, 16.33) | ||||
| 2nd month | Experimental | 18.16 (17.48, 18.85) | 2nd month | Experimental | 16.81 (15.50, 18.12) | ||
| Control | 15.88 (15.16, 16.60) | Control | 14.94 (13.55, 16.33) | ||||
| 3rd month | Experimental | 20.57 (19.94, 21.20) | 3rd month | Experimental | 17.23 (15.78, 18.27) | ||
| Control | 15.55 (14.88, 16.21) | Control | 14.88 (13.56, 16.20) | ||||
| Post-intervention | Experimental | 20.89 (20.30, 21.49) | Post-intervention | Experimental | 17.70 (16.59, 18.82) | ||
| Control | 15.09 (14.46, 15.72) | Control | 14.58 (13.39, 15.76) | ||||
| Affiliation | Pre-intervention | Experimental | 15.43 (14.13, 16.73) | Enjoyment | Pre-intervention | Experimental | 17.14 (15.88, 18.40) |
| Control | 15.09 (13.71, 16.47) | Control | 16.64 (15.30, 17.97) | ||||
| 1st month | Experimental | 15.51 (14.25, 16.78) | 1st month | Experimental | 17.19 (15.94, 18.44) | ||
| Control | 15.00 (13.66, 16.34) | Control | 16.58 (15.26, 17.90) | ||||
| 2nd month | Experimental | 15.51 (14.25, 16.78) | 2nd month | Experimental | 17.19 (15.94, 18.44) | ||
| Control | 15.00 (13.66, 16.34) | Control | 16.58 (15.26, 17.90) | ||||
| 3rd month | Experimental | 16.11 (14.98, 17.24) | 3rd month | Experimental | 17.27 (16.09, 18.45) | ||
| Control | 14.91 (13.71, 16.11) | Control | 16.33 (15.09, 17.58) | ||||
| Post-intervention | Experimental | 16.68 (15.62, 17.73) | Post-intervention | Experimental | 17.89 (16.82, 18.97) | ||
| Control | 14.73 (13.61, 15.84) | Control | 15.91 (14.77, 17.05) |
| Comparison on Amount of PA | Mean Difference (95% CI) | p-Value |
|---|---|---|
| Experimental-Control | 357.77 (148.90, 566.65) | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hidrus, A.; Kueh, Y.C.; Norsaádah, B.; Chang, Y.-K.; Hung, T.-M.; Naing, N.N.; Kuan, G. Effects of Brain Breaks Videos on the Motives for the Physical Activity of Malaysians with Type-2 Diabetes Mellitus. Int. J. Environ. Res. Public Health 2020, 17, 2507. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072507
Hidrus A, Kueh YC, Norsaádah B, Chang Y-K, Hung T-M, Naing NN, Kuan G. Effects of Brain Breaks Videos on the Motives for the Physical Activity of Malaysians with Type-2 Diabetes Mellitus. International Journal of Environmental Research and Public Health. 2020; 17(7):2507. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072507
Chicago/Turabian StyleHidrus, Aizuddin, Yee Cheng Kueh, Bachok Norsaádah, Yu-Kai Chang, Tsung-Min Hung, Nyi Nyi Naing, and Garry Kuan. 2020. "Effects of Brain Breaks Videos on the Motives for the Physical Activity of Malaysians with Type-2 Diabetes Mellitus" International Journal of Environmental Research and Public Health 17, no. 7: 2507. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072507