Effectiveness of Educational Interventions on Adherence to Lifestyle Modifications Among Hypertensive Patients: An Integrative Review



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
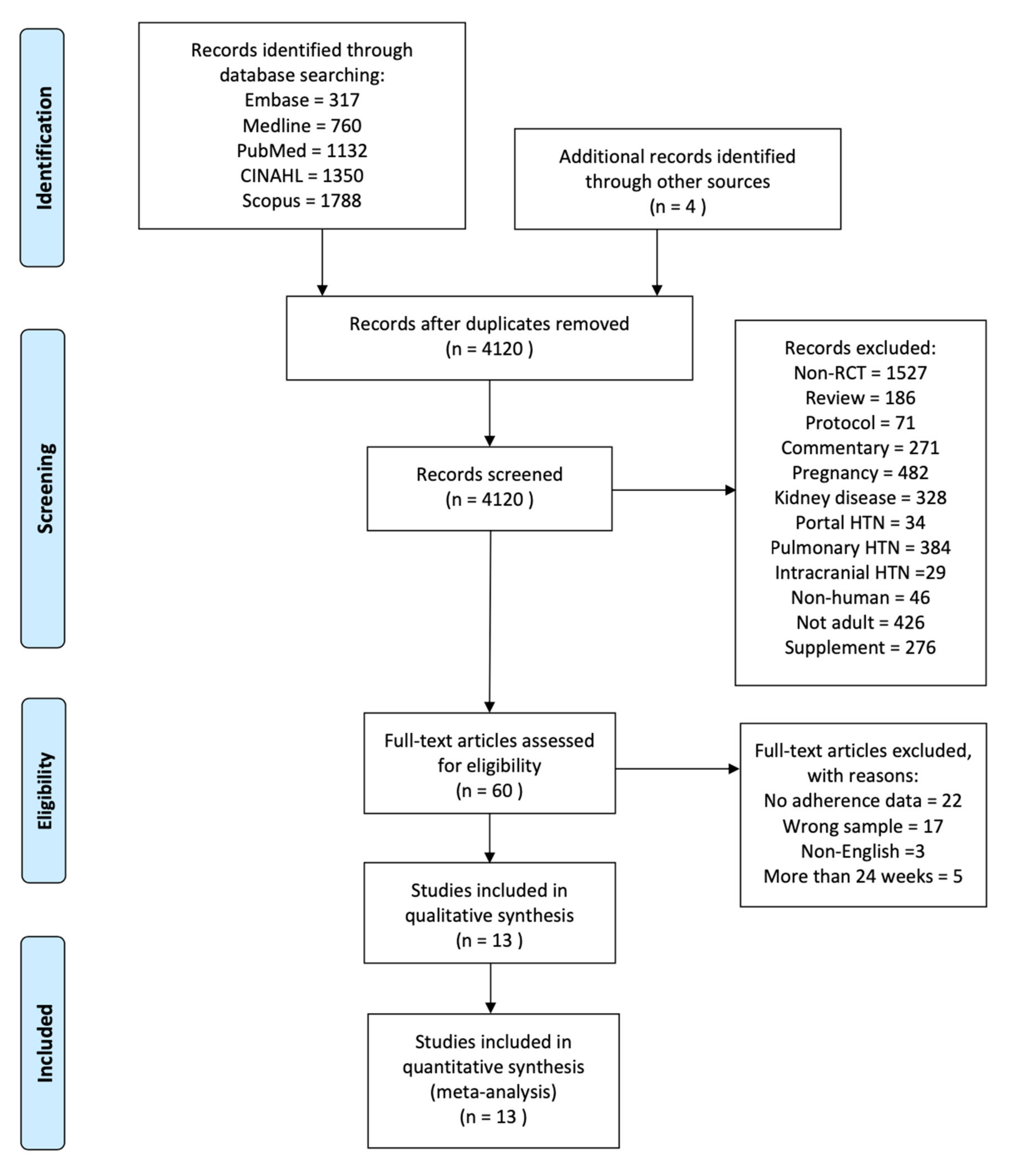
2.1. Search Strategy
| Participants | Hypertensive adults |
| Interventions | Educational interventions |
| Comparisons | Standard care |
| Outcomes | Adherence to lifestyle modifications, BP |
| Study design | RCT |
2.2. Eligible Criteria and Quality Assessment
2.3. Data Synthesis and Meta-Analysis
3. Results
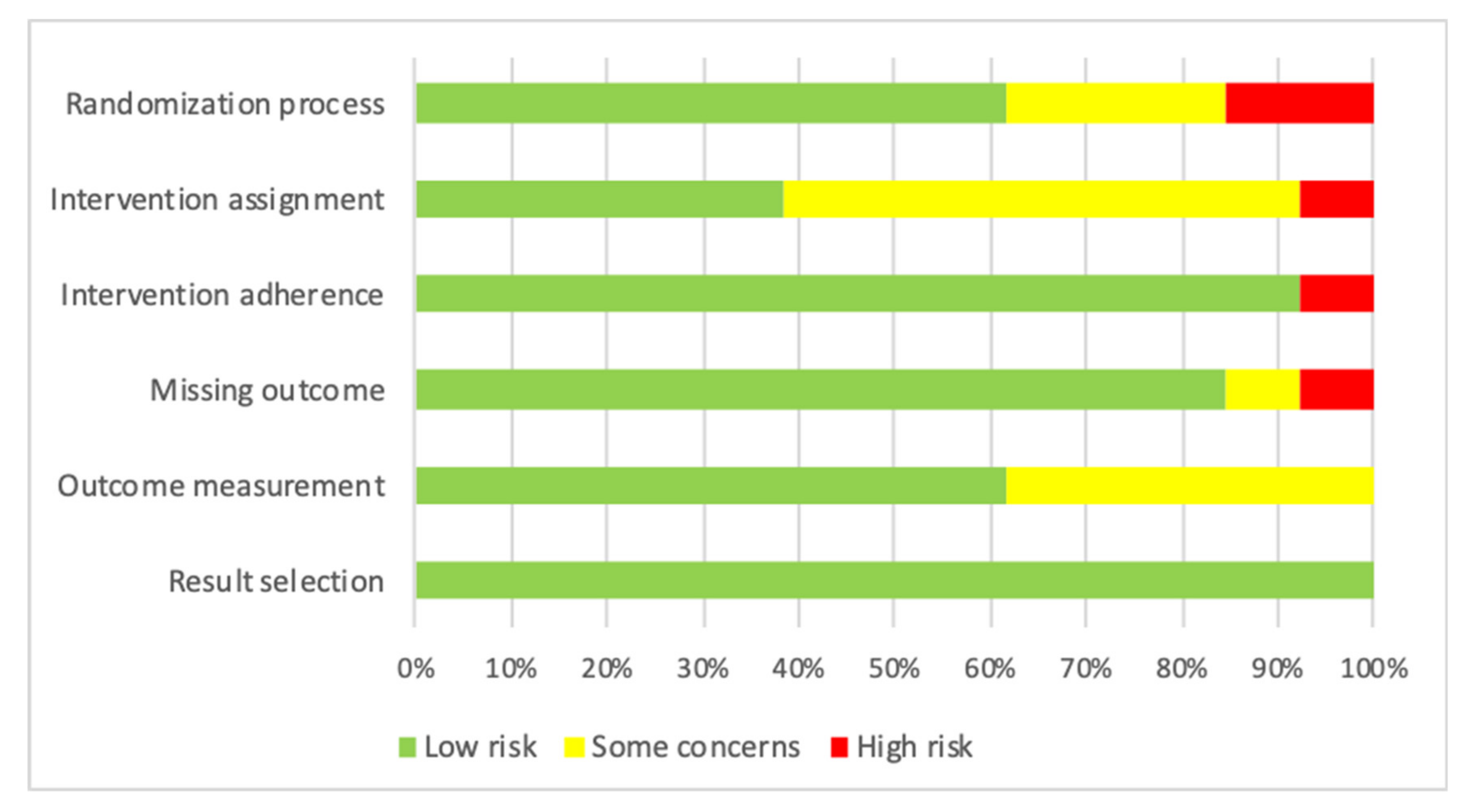
3.1. Quality Assessment
3.2. Characteristics of Studies
3.3. Characteristics of Educational Interventions
3.3.1. Delivery Mode and Dosage
3.3.2. Theoretical Framework
3.3.3. Supportive Methods
3.4. Meta-Analysis Results
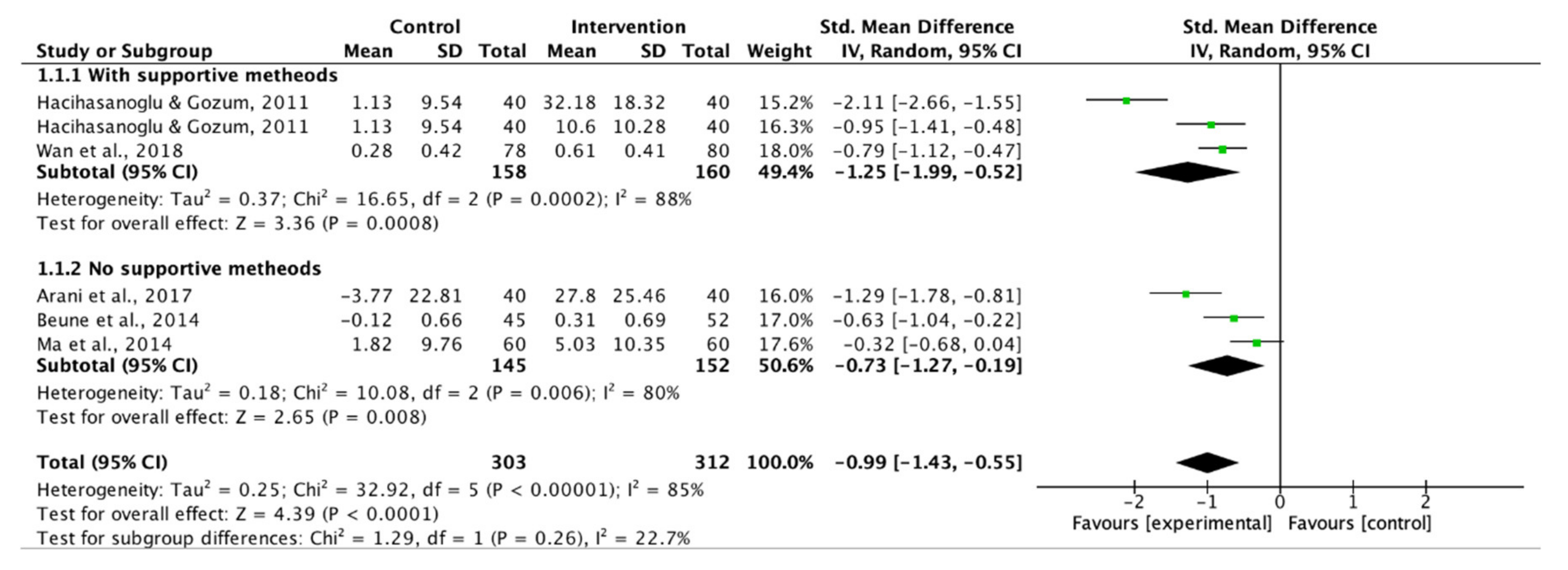
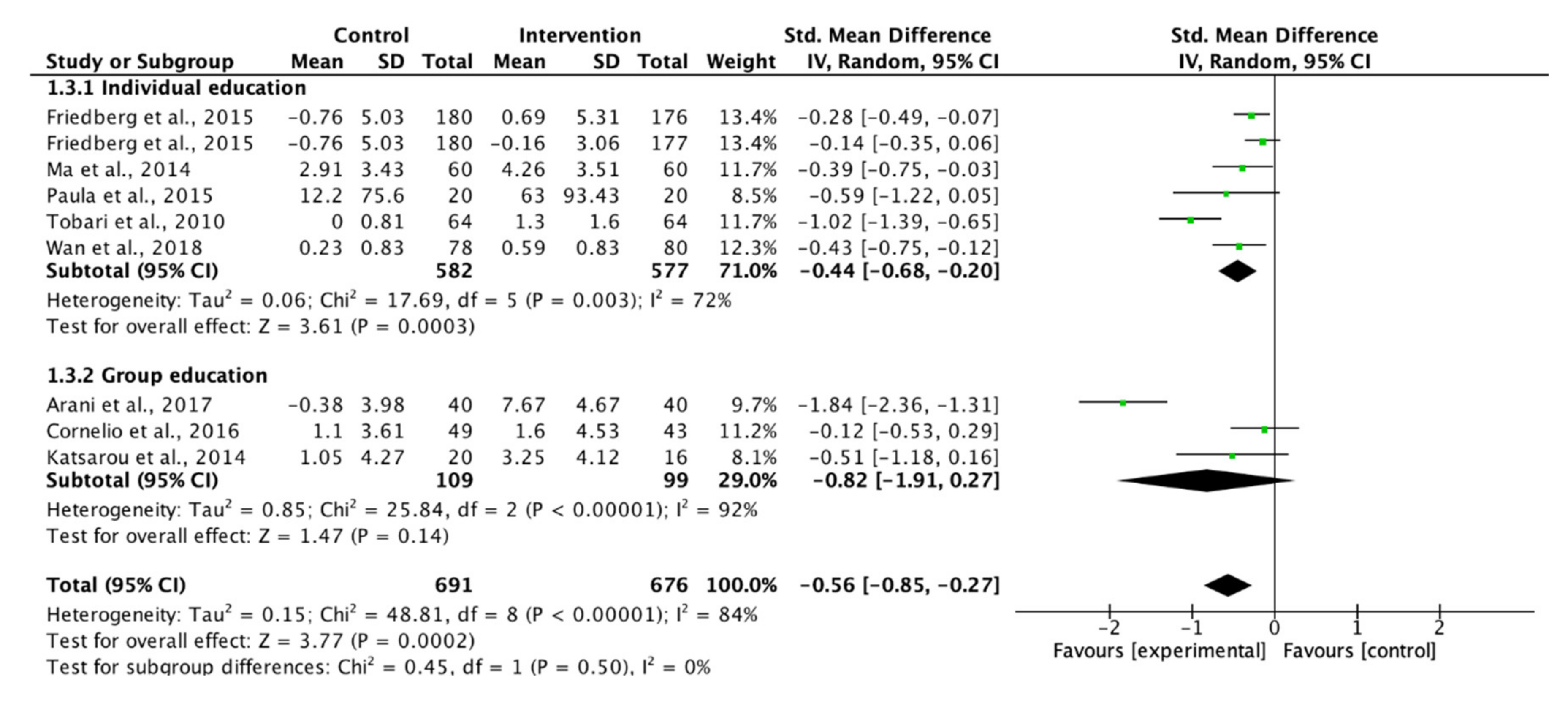
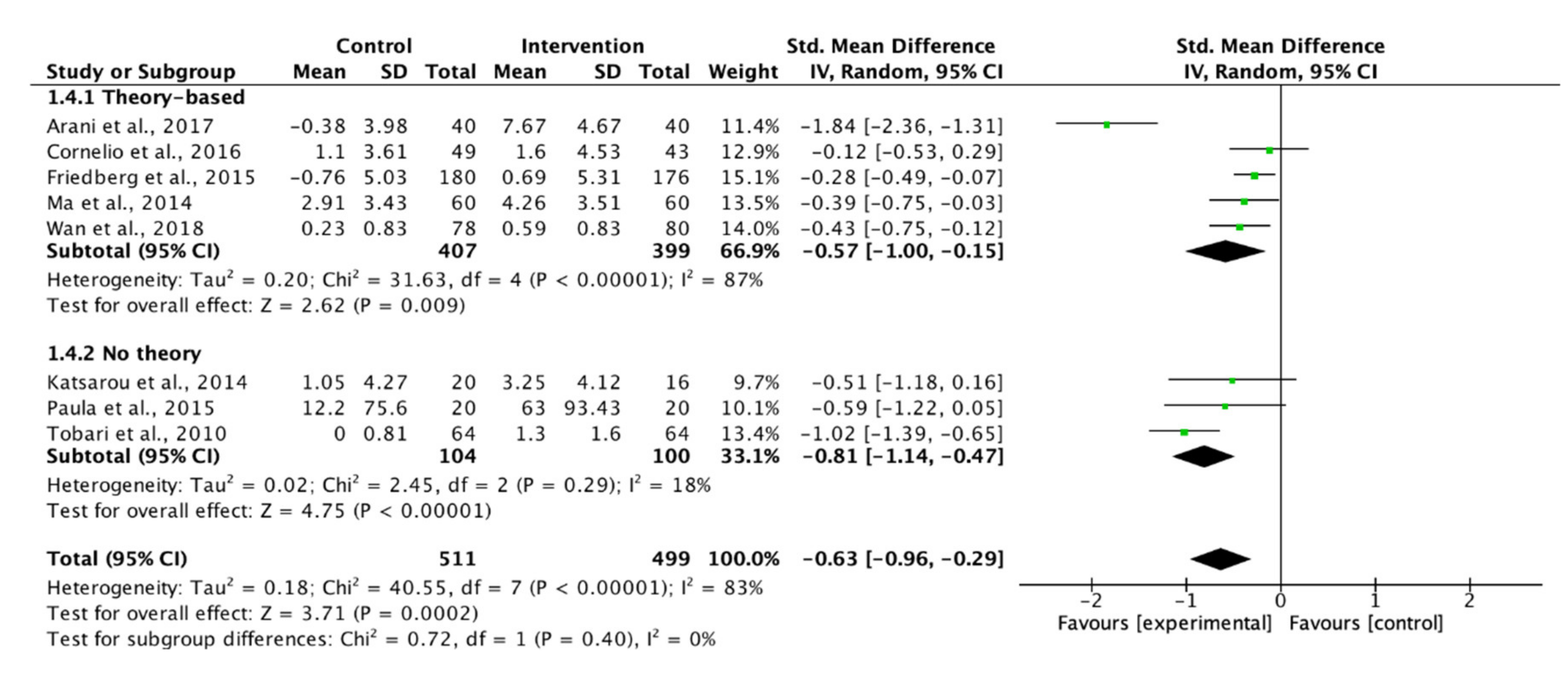
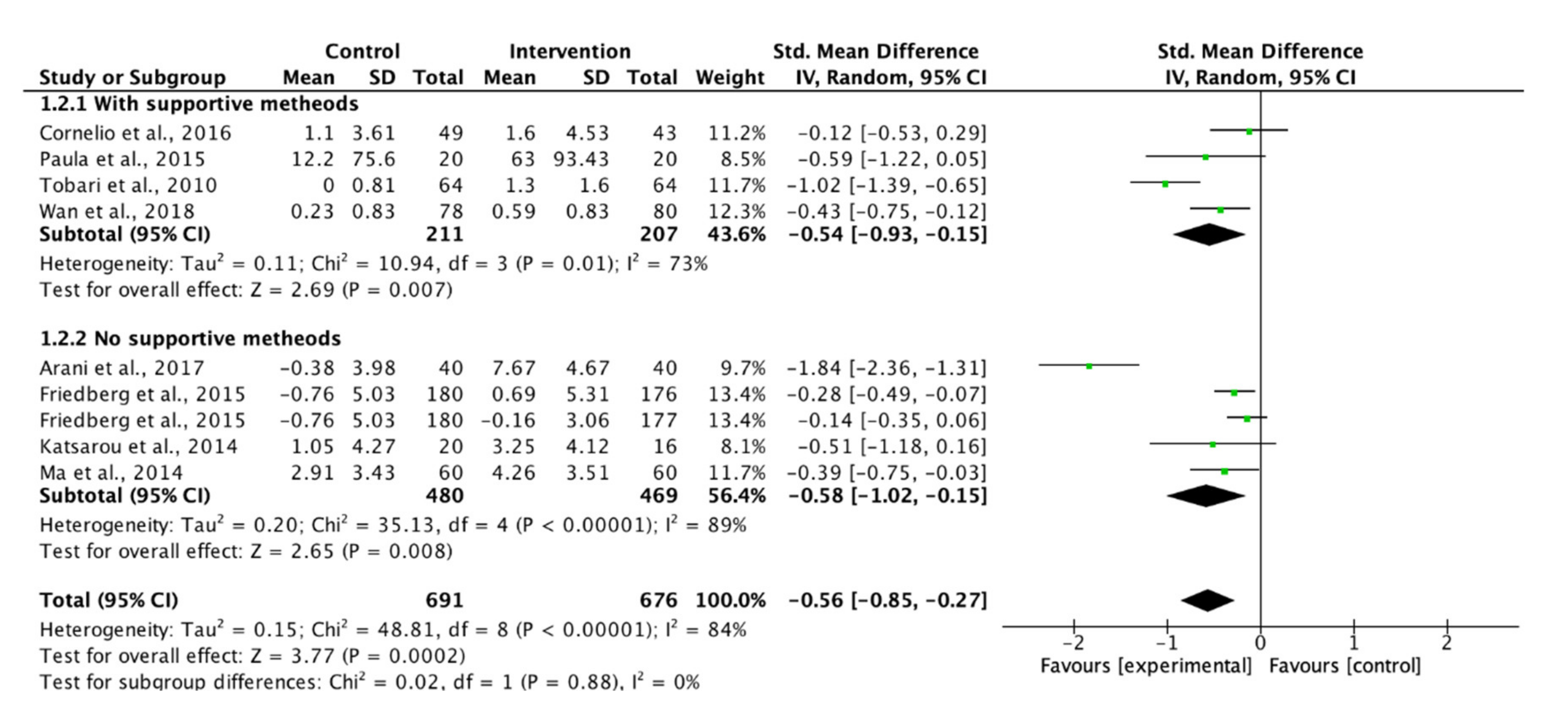
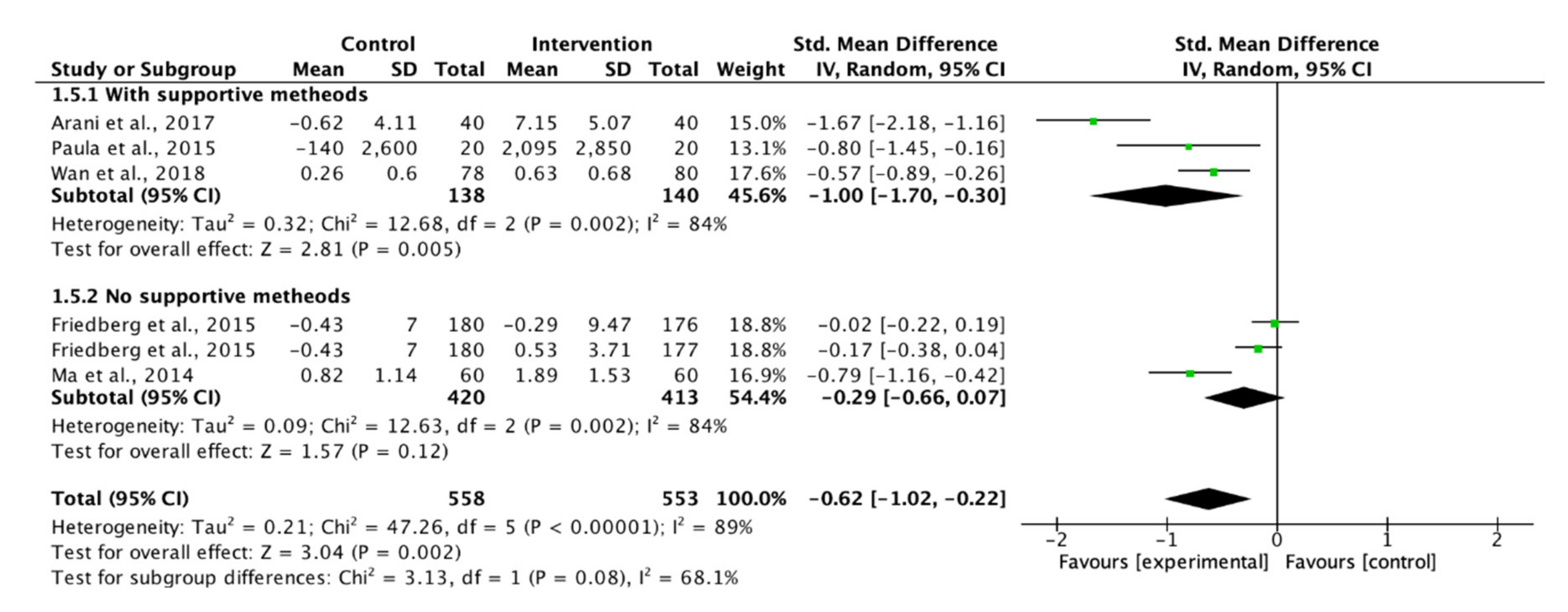
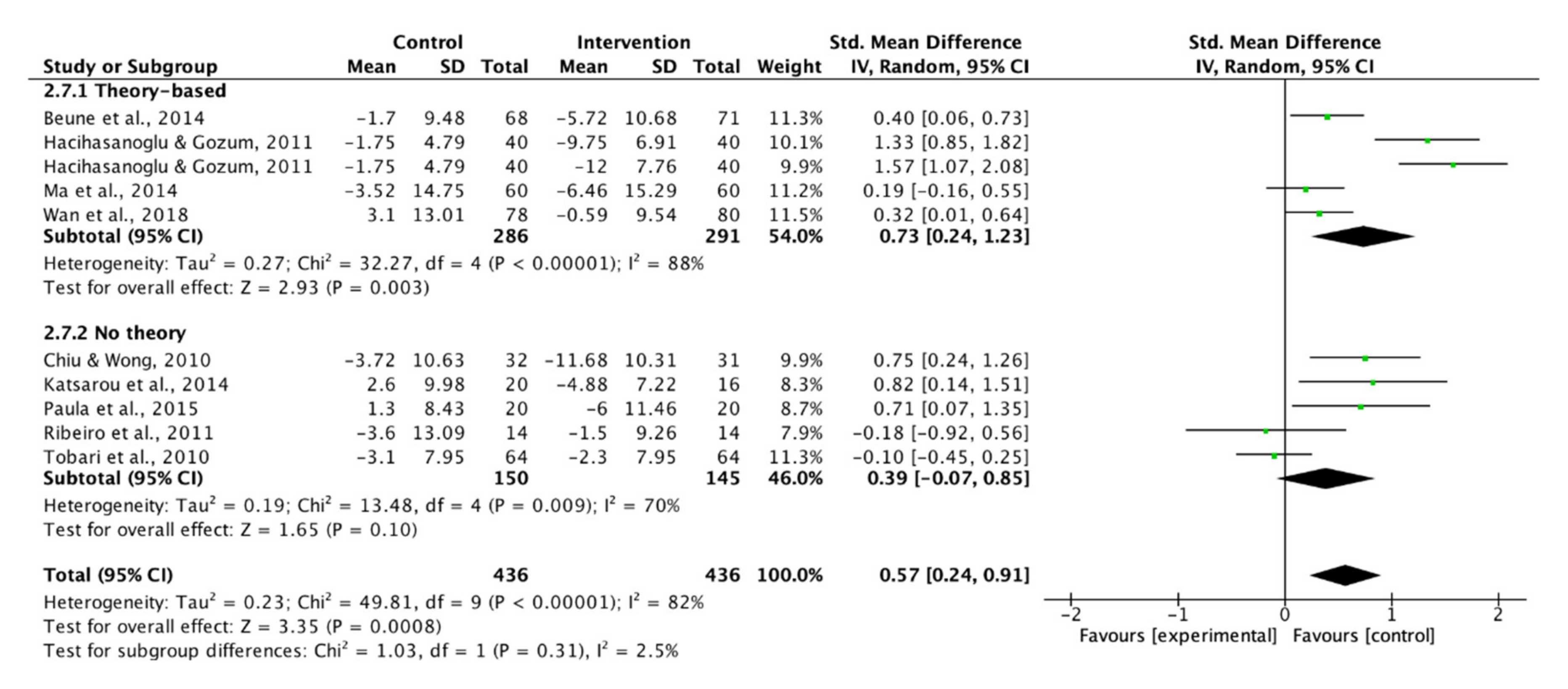
3.4.1. Adherence to Lifestyle Modifications
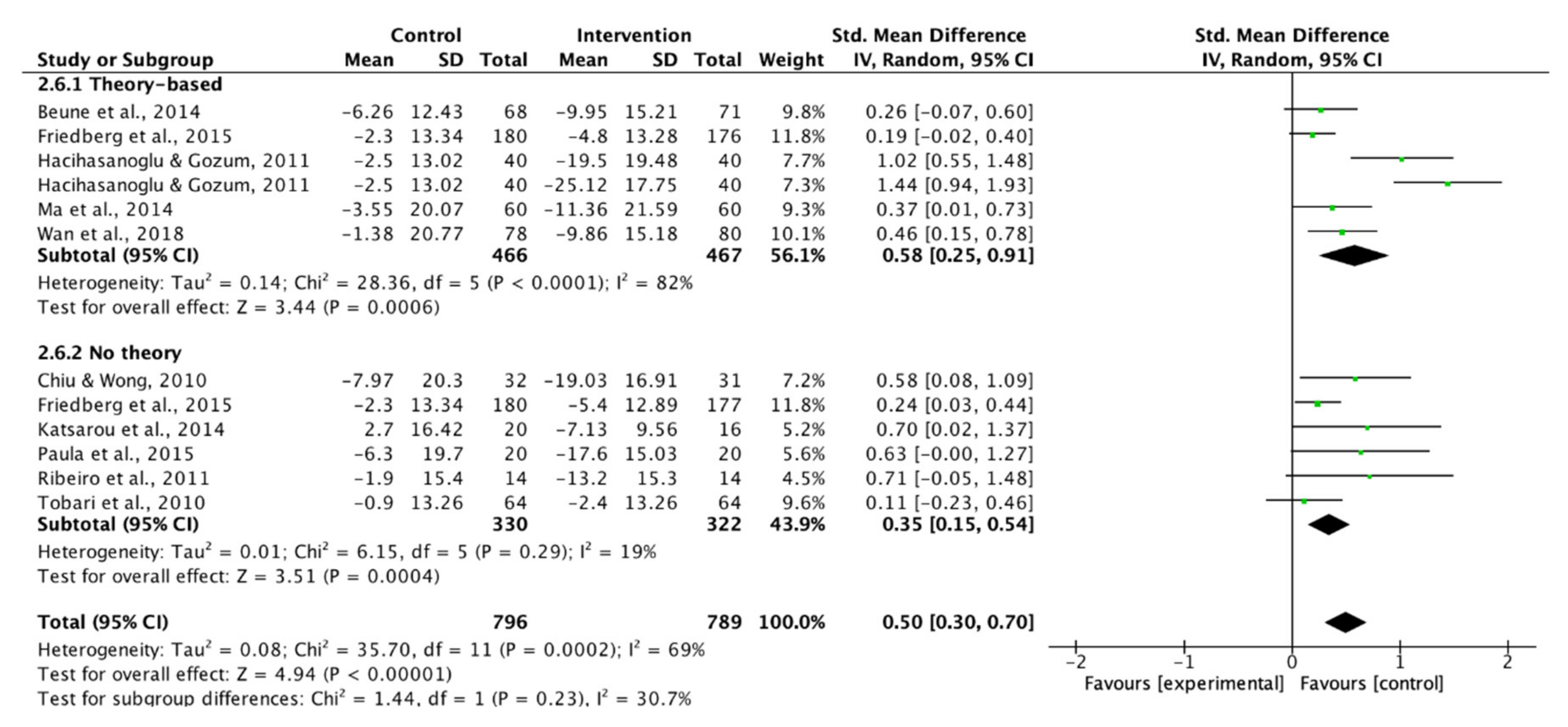
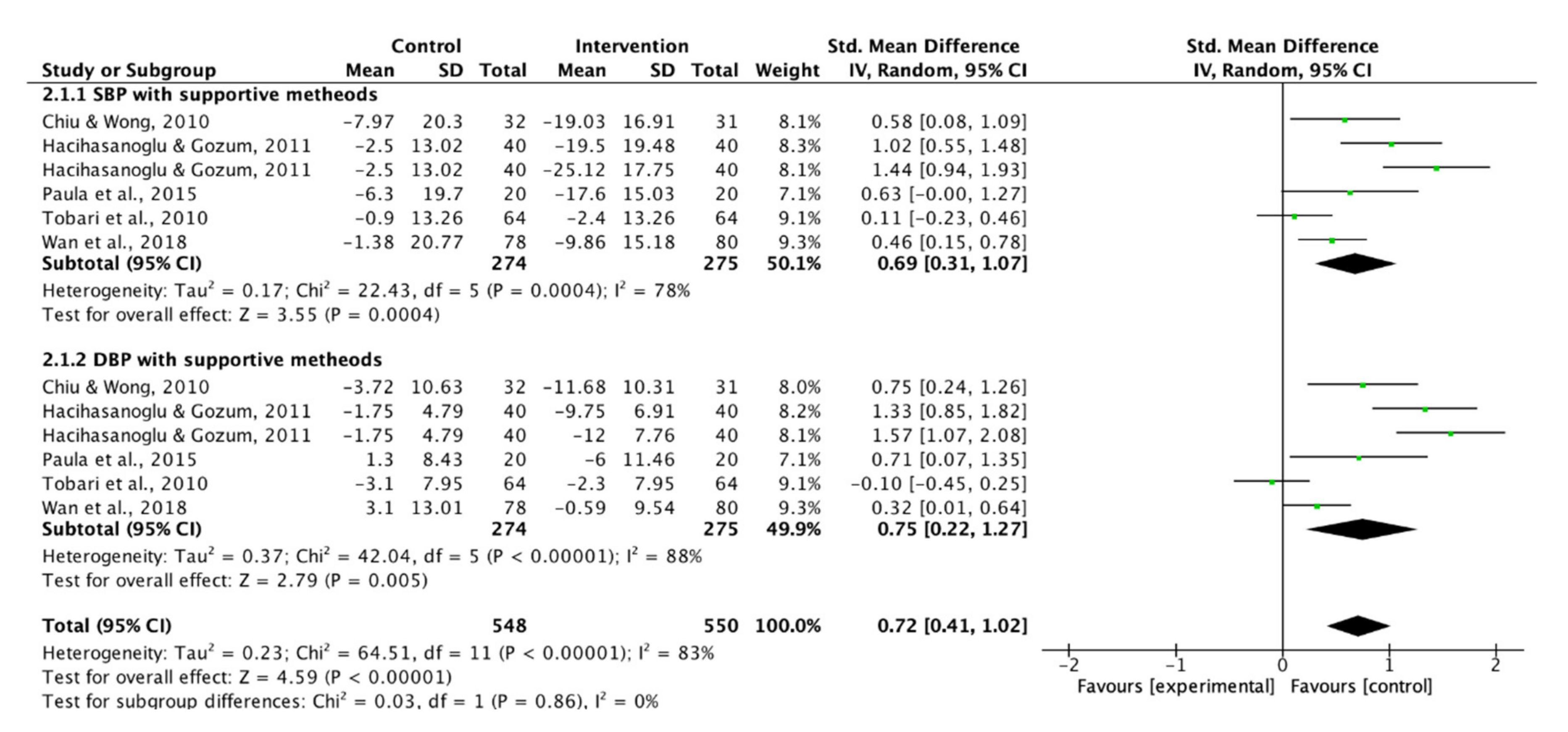
3.4.2. Blood Pressure Control
4. Discussion
4.1. Delivery Mode
4.2. Use of Theoretical Framework
4.3. Use of Supportive Methods
4.4. Limitations
5. Implications
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Availabe online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 20 January 2020).
- World Health Organization. Hypertension. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 20 January 2020).
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration. Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef] [Green Version]
- NCD Risk Factor Collaboration. Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: An analysis of 123 nationally representative surveys. Lancet 2019, 394, 639–651. [Google Scholar] [CrossRef] [Green Version]
- Posadzki, P.; Cramer, H.; Kuzdzal, A.; Lee, M.S.; Ernst, E. Yoga for hypertension: A systematic review of randomized clinical trials. Complement. Ther. Med. 2014, 22, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Mahtani, K.R.; Beinortas, T.; Bauza, K.; Nunan, D. Device-Guided Breathing for Hypertension: A Summary Evidence Review. Curr. Hypertens. Rep. 2016, 18, 33. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Liu, L.S.; Wu, Z.S.; Wang, J.G.; Wang, W.; Bao, Y.J.; Cai, J.; Chen, L.Y.; Chen, W.W.; Chu, S.L.; Feng, Y.Q.; et al. 2018 Chinese Guidelines for Prevention and Treatment of Hypertension-A report of the Revision Committee of Chinese Guidelines for Prevention and Treatment of Hypertension. J. Geriatr. Cardiol. 2019, 16, 182–241. [Google Scholar] [CrossRef]
- Umemura, S.; Arima, H.; Arima, S.; Asayama, K.; Dohi, Y.; Hirooka, Y.; Horio, T.; Hoshide, S.; Ikeda, S.; Ishimitsu, T.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens. Res. 2019, 42, 1235–1481. [Google Scholar] [CrossRef]
- Lee, H.Y.; Shin, J.; Kim, G.H.; Park, S.; Ihm, S.H.; Kim, H.C.; Kim, K.I.; Kim, J.H.; Lee, J.H.; Park, J.M.; et al. 2018 Korean Society of Hypertension Guidelines for the management of hypertension: Part II-diagnosis and treatment of hypertension. Clin. Hypertens. 2019, 25, 20. [Google Scholar] [CrossRef]
- Burnier, M.; Egan, B.M. Adherence in Hypertension. Circ. Res. 2019, 124, 1124–1140. [Google Scholar] [CrossRef]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. Available online: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf (accessed on 20 January 2020).
- Selçuk, K.T.; Çevik, C.; Mercan, Y.; Koca, H. Hypertensive patients’ adherence to pharmacological and non-pharmacological treatment methods, in Turkey. Int. J. Community Med. Public Health 2017, 4, 2648–2657. [Google Scholar] [CrossRef] [Green Version]
- Fang, J.; Moore, L.; Loustalot, F.; Yang, Q.; Ayala, C. Reporting of adherence to healthy lifestyle behaviors among hypertensive adults in the 50 states and the District of Columbia, 2013. J. Am. Soc. Hypertens. 2016, 10, 252–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glynn, L.G.; Murphy, A.W.; Smith, S.M.; Schroeder, K.; Fahey, T. Interventions used to improve control of blood pressure in patients with hypertension. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Conn, V.S.; Ruppar, T.M.; Chase, J.A.; Enriquez, M.; Cooper, P.S. Interventions to Improve Medication Adherence in Hypertensive Patients: Systematic Review and Meta-Analysis. Curr. Hypertens. Rep. 2015, 17, 94. [Google Scholar] [CrossRef]
- Morrissey, E.C.; Durand, H.; Nieuwlaat, R.; Navarro, T.; Haynes, R.B.; Walsh, J.C.; Molloy, G.J. Effectiveness and content analysis of interventions to enhance medication adherence and blood pressure control in hypertension: A systematic review and meta-analysis. Psychol. Health 2017, 32, 1195–1232. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V. Interpreting Estimates of Treatment Effects. Pharm. Ther. 2008, 33, 700–711. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Systmatic Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katsarou, A.L.; Vryonis, M.M.; Protogerou, A.D.; Alexopoulos, E.C.; Achimastos, A.; Papadogiannis, D.; Chrousos, G.P.; Darviri, C. Stress management and dietary counseling in hypertensive patients: A pilot study of additional effect. Prim. Health Care Res. Dev. 2014, 15, 38–45. [Google Scholar] [CrossRef] [PubMed]
- The World Bank Group. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519 (accessed on 20 January 2020).
- Chiu, C.W.; Wong, F.K.Y. Effects of 8 weeks sustained follow-up after a nurse consultation on hypertension: A randomised trial. Int. J. Nurs. Stud. 2010, 47, 1374–1382. [Google Scholar] [CrossRef]
- Tobari, H.; Arimoto, T.; Shimojo, N.; Yuhara, K.; Noda, H.; Yamagishi, K.; Iso, H. Physician-pharmacist cooperation program for blood pressure control in patients with hypertension: A randomized-controlled trial. Am. J. Hypertens. 2010, 23, 1144–1152. [Google Scholar] [CrossRef] [Green Version]
- Beune, E.J.; Moll van Charante, E.P.; Beem, L.; Mohrs, J.; Agyemang, C.O.; Ogedegbe, G.; Haafkens, J.A. Culturally adapted hypertension education (CAHE) to improve blood pressure control and treatment adherence in patients of African origin with uncontrolled hypertension: Cluster-randomized trial. PLoS ONE 2014, 9, e90103. [Google Scholar] [CrossRef]
- Friedberg, J.P.; Rodriguez, M.A.; Watsula, M.E.; Lin, I.; Wylie-Rosett, J.; Allegrante, J.P.; Lipsitz, S.R.; Natarajan, S. Effectiveness of a tailored behavioral intervention to improve hypertension control: Primary outcomes of a randomized controlled trial. Hypertension 2015, 65, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Hacihasanoglu, R.; Gozum, S. The effect of patient education and home monitoring on medication compliance, hypertension management, healthy lifestyle behaviours and BMI in a primary health care setting. J. Clin. Nurs. 2011, 20, 692–705. [Google Scholar] [CrossRef]
- Ribeiro, A.G.; Ribeiro, S.M.; Dias, C.M.; Ribeiro, A.Q.; Castro, F.A.; Suárez-Varela, M.M.; Cotta, R.M. Non-pharmacological treatment of hypertension in primary health care: A comparative clinical trial of two education strategies in health and nutrition. BMC Public Health 2011, 11, 637. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.; Zhou, Y.; Zhou, W.; Huang, C. Evaluation of the effect of motivational interviewing counselling on hypertension care. Patient Educ. Couns. 2014, 95, 231–237. [Google Scholar] [CrossRef]
- Paula, T.P.; Viana, L.V.; Neto, A.T.Z.; Leitão, C.B.; Gross, J.L.; Azevedo, M.J. Effects of the DASH Diet and Walking on Blood Pressure in Patients With Type 2 Diabetes and Uncontrolled Hypertension: A Randomized Controlled Trial. J. Clin. Hypertens. 2015, 17, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Cornélio, M.E.; Godin, G.; Rodrigues, R.C.M.; de Freitas Agondi, R.; Alexandre, N.M.C.; Gallani, M.-C.B.J. Effect of a behavioral intervention of the SALdável program to reduce salt intake among hypertensive women: A randomized controlled pilot study. Eur. J. Cardiovasc. Nurs. 2016, 15, e85–e94. [Google Scholar] [CrossRef] [PubMed]
- Arani, M.D.; Taghadosi, M.; Gilasi, H.R. The effect of education based on BASNEF model on lifestyle in patients with hypertension. Iran. Red Crescent Med. J. 2017, 19. [Google Scholar] [CrossRef] [Green Version]
- Wan, L.-H.; Zhang, X.-P.; You, L.-M.; Ruan, H.-F.; Chen, S.-X. The Efficacy of a Comprehensive Reminder System to Improve Health Behaviors and Blood Pressure Control in Hypertensive Ischemic Stroke Patients: A Randomized Controlled Trial. J. Cardiovasc. Nurs. 2018, 33, 509–517. [Google Scholar] [CrossRef]
- Ayodapo, A.O.; Olukokun, T.A.V. Lifestyle counselling and behavioural change: Role among adult hypertensives in a rural tertiary institution. S. Afr. Fam. Pract. 2019, 61, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Korhonen, M.J.; Pentti, J.; Hartikainen, J.; Ilomaki, J.; Setoguchi, S.; Liew, D.; Kivimaki, M.; Vahtera, J. Lifestyle Changes in Relation to Initiation of Antihypertensive and Lipid-Lowering Medication: A Cohort Study. J. Am. Heart Assoc. 2020, 9, e014168. [Google Scholar] [CrossRef]
- Maimaris, W.; Paty, J.; Perel, P.; Legido-Quigley, H.; Balabanova, D.; Nieuwlaat, R.; McKee, M. The influence of health systems on hypertension awareness, treatment, and control: A systematic literature review. PLoS Med. 2013, 10, e1001490. [Google Scholar] [CrossRef] [Green Version]
- International Council of Nurses. Nursing Definitions. Available online: https://www.icn.ch/nursing-policy/nursing-definitions (accessed on 16 February 2020).
- Yip, B.H.K.; Lee, E.K.P.; Sit, R.W.S.; Wong, C.; Li, X.; Wong, E.L.Y.; Wong, M.C.S.; Chung, R.Y.N.; Chung, V.C.H.; Kung, K.; et al. Nurse-led hypertension management was well accepted and non-inferior to physician consultation in a Chinese population: A randomized controlled trial. Sci. Rep. 2018, 8, 10302. [Google Scholar] [CrossRef] [Green Version]
- Olsen, M.H.; Angell, S.Y.; Asma, S.; Boutouyrie, P.; Burger, D.; Chirinos, J.A.; Damasceno, A.; Delles, C.; Gimenez-Roqueplo, A.-P.; Hering, D.; et al. A call to action and a lifecourse strategy to address the global burden of raised blood pressure on current and future generations: The Lancet Commission on hypertension. Lancet 2016, 388, 2665–2712. [Google Scholar] [CrossRef]
- World Health Organization. Enhancing the Role of Community Health Nursing for Universal Health Coverage: Human Resources for Health Observer Series No.18. Available online: https://apps.who.int/iris/bitstream/handle/10665/255047/9789241511896-eng.pdf (accessed on 18 February 2020).
- da Silva, A.T.M.; Mantovani, M.d.; Castanho Moreira, R.; Perez Arthur, J.; de Souza, R.M. Nursing case management for people with hypertension in primary health care: A randomized controlled trial. Res. Nurs. Health 2019. [Google Scholar] [CrossRef]
- Xu, R.; Xie, X.; Li, S.; Chen, X.; Wang, S.; Hu, C.; Lv, X. Interventions to improve medication adherence among Chinese patients with hypertension: A systematic review and meta-analysis of randomized controlled trails. Int. J. Pharm. Pract. 2018, 26, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Vargas, G.; Cajita, M.I.; Whitehouse, E.; Han, H.R. Use of Short Messaging Service for Hypertension Management: A Systematic Review. J Cardiovasc. Nurs. 2017, 32, 260–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, M.; He, F.J.; Wang, C.; MacGregor, G.A. Twenty-Four-Hour Urinary Sodium and Potassium Excretion in China: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e012923. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Chen, S.; You, L.; Luo, Z.; Xing, C. Development and psychometric evaluation of the Treatment Adherence Questionnaire for Patients with Hypertension. J. Adv. Nurs. 2012, 68, 1402–1413. [Google Scholar] [CrossRef]
- Kim, M.T.; Hill, M.N.; Bone, L.R.; Levine, D.M. Development and Testing of the Hill-Bone Compliance to High Blood Pressure Therapy Scale. Prog. Cardiovasc. Nurs. 2000, 15, 90–96. [Google Scholar] [CrossRef]
- Perez-Escamilla, B.; Franco-Trigo, L.; Moullin, J.C.; Martinez-Martinez, F.; Garcia-Corpas, J.P. Identification of validated questionnaires to measure adherence to pharmacological antihypertensive treatments. Patient Prefer. Adherence 2015, 9, 569–578. [Google Scholar] [CrossRef] [Green Version]
- Johns Hopkins School of Nursing. Translations—Hill-Bone Scales. Available online: https://0-nursing-jhu-edu.brum.beds.ac.uk/faculty_research/research/projects/hill-bone/translation.html (accessed on 18 February 2020).










© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tam, H.L.; Wong, E.M.L.; Cheung, K. Effectiveness of Educational Interventions on Adherence to Lifestyle Modifications Among Hypertensive Patients: An Integrative Review. Int. J. Environ. Res. Public Health 2020, 17, 2513. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072513
Tam HL, Wong EML, Cheung K. Effectiveness of Educational Interventions on Adherence to Lifestyle Modifications Among Hypertensive Patients: An Integrative Review. International Journal of Environmental Research and Public Health. 2020; 17(7):2513. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072513
Chicago/Turabian StyleTam, Hon Lon, Eliza Mi Ling Wong, and Kin Cheung. 2020. "Effectiveness of Educational Interventions on Adherence to Lifestyle Modifications Among Hypertensive Patients: An Integrative Review" International Journal of Environmental Research and Public Health 17, no. 7: 2513. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072513