The Effect of Active Plus, a Computer-Tailored Physical Activity Intervention, on the Physical Activity of Older Adults with Chronic Illness(es)—A Cluster Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Population
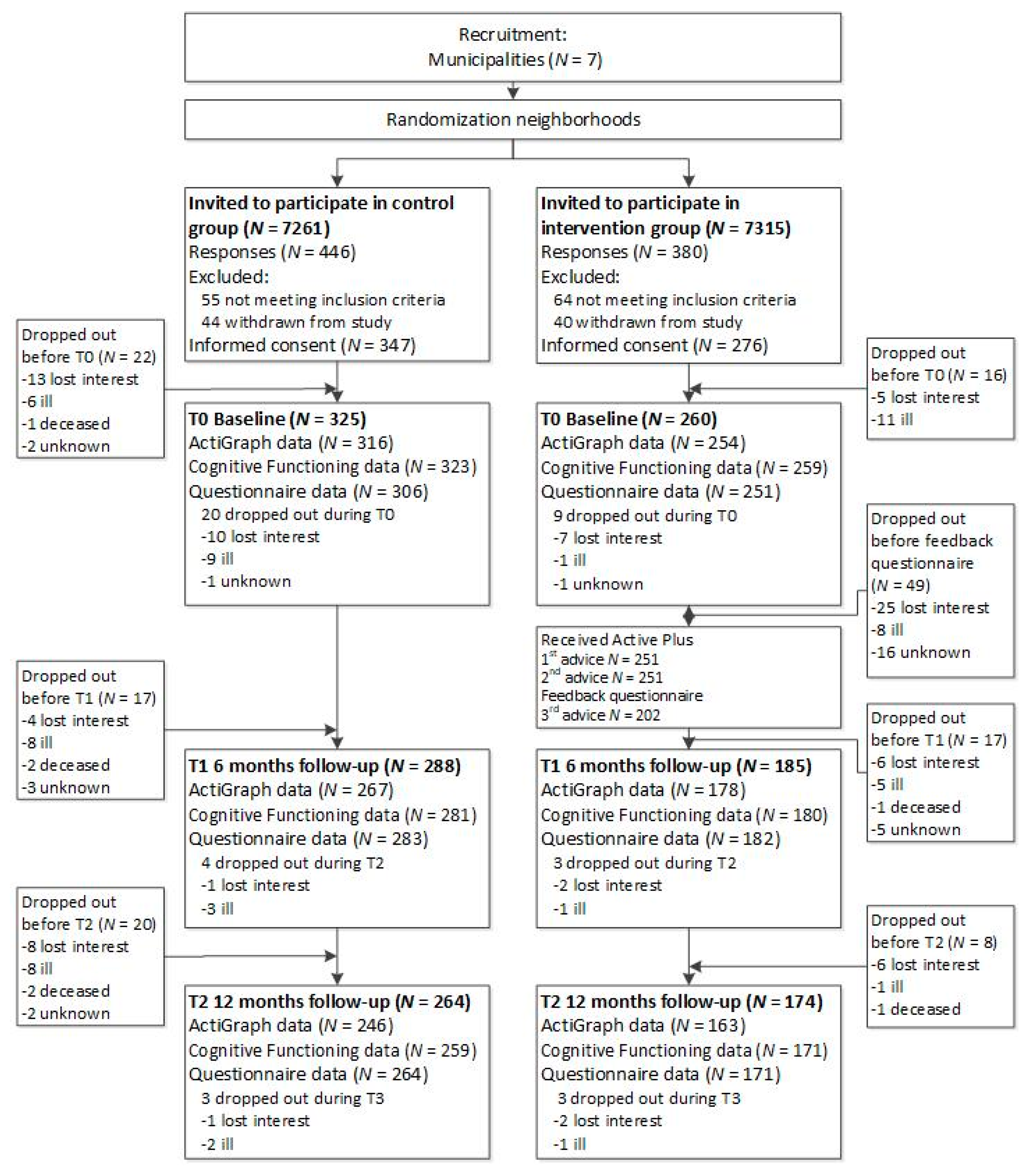
2.1.1. Procedure
2.1.2. Intervention Group
2.1.3. Waiting List Control Group
2.2. Outcomes
2.2.1. Physical Activity (PA) Outcomes
2.2.2. Other Relevant Measures
2.2.3. Sample Size and Statistical Power
2.2.4. Statistical Analyses
3. Results
3.1. Study Population
3.2. Intervention Effects
3.3. Moderation of Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Gerteis, J.; Izrael, D.; Deitz, D.; LeRoy, L.; Ricciardi, R.; Miller, T.; Basu, J. Multiple Chronic Conditions Chartbook. Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014. [Google Scholar]
- Fuller, B.G.; Stewart Williams, J.A.; Byles, J.E. Active living-the perception of older people with chronic conditions. Chronic Illn. 2010, 6, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Voss, M.W.; Carr, L.J.; Clark, R.; Weng, T. Revenge of the “sit” II: Does lifestyle impact neuronal and cognitive health through distinct mechanisms associated with sedentary behavior and physical activity? Ment. Health Phys. Act. 2014, 7, 9–24. [Google Scholar] [CrossRef]
- Marcus, B.H.; Williams, D.M.; Dubbert, P.M.; Sallis, J.F.; King, A.C.; Yancey, A.K.; Franklin, B.A.; Buchner, D.; Daniels, S.R.; Claytor, R.P. What we know and what we need to know: A scientific statement from the American Heart Association council on nutrition, physical activity, and metabolism (subcommittee on physical activity); council on cardiovascular disease in the young; and the interdis. Circulation 2006, 114, 2739–2752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devereux-Fitzgerald, A.; Powell, R.; Dewhurst, A.; French, D.P. The acceptability of physical activity interventions to older adults: A systematic review and meta-synthesis. Soc. Sci. Med. 2016, 158, 14–23. [Google Scholar] [CrossRef]
- Quiñones, A.R.; Markwardt, S.; Botoseneanu, A. Multimorbidity combinations and disability in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 823–830. [Google Scholar] [CrossRef] [Green Version]
- Salive, M.E. Multimorbidity in older adults. Epidemiol. Rev. 2013, 35, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Jindai, K.; Nielson, C.M.; Vorderstrasse, B.A.; Quiñones, A.R. Multimorbidity and functional limitations among adults 65 or older, NHANES 2005–2012. Prev. Chronic Dis. 2016, 13, E151. [Google Scholar] [CrossRef] [Green Version]
- Gill, T.M.; Gahbauer, E.A.; Han, L.; Allore, H.G. Trajectories of disability in the last year of life. N. Engl. J. Med. 2010, 362, 1173–1180. [Google Scholar] [CrossRef] [Green Version]
- De Vries, N.M.; Van Ravensberg, C.D.; Hobbelen, J.S.M.; Olde Rikkert, M.G.M.; Staal, J.B.; Nijhuis-van der Sanden, M.W.G. Effects of physical exercise therapy on mobility, physical functioning, physical activity and quality of life in community-dwelling older adults with impaired mobility, physical disability and/or multi-morbidity: A meta-analysis. Ageing Res. Rev. 2012, 11, 136–149. [Google Scholar] [CrossRef]
- Tak, E.; Kuiper, R.; Chorus, A.; Hopman-Rock, M. Prevention of onset and progression of basic ADL disability by physical activity in community dwelling older adults: A meta-analysis. Ageing Res. Rev. 2013, 12, 329–338. [Google Scholar] [CrossRef]
- De Hond, A.; Bakx, P.; Versteegh, M. Can time heal all wounds? An empirical assessment of adaptation to functional limitations in an older population. Soc. Sci. Med. 2019, 222, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Stevinson, C.; Lawlor, D.A.; Fox, K.R. Exercise interventions for cancer patients: Systematic review of controlled trials. Cancer Causes Control 2004, 15, 1035–1056. [Google Scholar] [CrossRef] [PubMed]
- Zanuso, S.; Jimenez, A.; Pugliese, G.; Corigliano, G.; Balducci, S. Exercise for the management of type 2 diabetes: A review of the evidence. Acta Diabetol. 2010, 47, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, R.S.; Brown, A.; Ebrahim, S.; Jolliffe, J.; Noorani, H.; Rees, K.; Skidmore, B.; Stone, J.A.; Thompson, D.R.; Oldridge, N. Exercise-based rehabilitation for patients with coronary heart disease: Systematic review and meta-analysis of randomized controlled trials. Am. J. Med. 2004, 116, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef]
- Bullard, T.; Ji, M.; An, R.; Trinh, L.; MacKenzie, M.; Mullen, S.P. A systematic review and meta-analysis of adherence to physical activity interventions among three chronic conditions: Cancer, cardiovascular disease, and diabetes. BMC Public Health 2019, 19, 636. [Google Scholar] [CrossRef] [Green Version]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U.; Alkandari, J.R.; Bauman, A.E.; Blair, S.N.; Brownson, R.C.; et al. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Chase, J.A.D. Interventions to increase physical activity among older adults: A meta-analysis. Gerontologist 2015, 55, 706–718. [Google Scholar] [CrossRef] [Green Version]
- Amagasa, S.; Machida, M.; Fukushima, N.; Kikuchi, H.; Takamiya, T.; Odagiri, Y.; Inoue, S. Is objectively measured light-intensity physical activity associated with health outcomes after adjustment for moderate-to-vigorous physical activity in adults? A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 65. [Google Scholar] [CrossRef]
- Kerr, J.; Marshall, S.J.; Patterson, R.E.; Marinac, C.R.; Natarajan, L.; Rosenberg, D.; Wasilenko, K.; Crist, K. Objectively measured physical activity is related to cognitive function in older adults. J. Am. Geriatr. Soc. 2013, 61, 1927–1931. [Google Scholar] [CrossRef] [Green Version]
- Johnson, L.G.; Butson, M.L.; Polman, R.C.; Raj, I.S.; Borkoles, E.; Scott, D.; Aitken, D.; Jones, G. Light physical activity is positively associated with cognitive performance in older community dwelling adults. J. Sci. Med. Sport 2016, 19, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Beddhu, S.; Wei, G.; Marcus, R.L.; Chonchol, M.; Greene, T. Light-intensity physical activities and mortality in the United States general population and CKD subpopulation. Clin. J. Am. Soc. Nephrol. 2015, 10, 1145–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amagasa, S.; Fukushima, N.; Kikuchi, H.; Takamiya, T.; Oka, K.; Inoue, S. Light and sporadic physical activity overlooked by current guidelines makes older women more active than older men. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vries, N.M.; Van Ravensberg, C.D.; Hobbelen, J.S.M.; Van Der Wees, P.J.; Olde Rikkert, M.G.M.; Staal, J.B.; Nijhuis-Van Der Sanden, M.W.G. The Coach2Move approach: Development and acceptability of an individually tailored physical therapy strategy to increase activity levels in older adults with mobility problems. J. Geriatr. Phys. Ther. 2015, 38, 169–182. [Google Scholar] [CrossRef] [Green Version]
- Jette, A.M.; Lachman, M.; Giorgetti, M.M.; Assmann, S.F.; Harris, B.A.; Levenson, C.; Wernick, M.; Krebs, D. Exercise—It’s never too late: The strong-for-life program. Am. J. Public Health 1999, 89, 66–72. [Google Scholar] [CrossRef] [Green Version]
- Pahor, M.; Blair, S.N.; Espeland, M.; Fielding, R.; Gill, T.M.; Guralnik, J.M.; Hadley, E.C.; King, A.C.; Kritchevsky, S.B.; Maraldi, C.; et al. Effects of a physical activity intervention on measures of physical performance: Results of the lifestyle interventions and independence for elders pilot (LIFE-P) study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 1157–1165. [Google Scholar]
- Marcus, B.H.; Nigg, C.R.; Riebe, D.; Forsyth, L.H. Interactive communication strategies: Implications for population-based physical-activity promotion. Am. J. Prev. Med. 2000, 19, 121–126. [Google Scholar] [CrossRef]
- Duijts, S.F.A.; Van Beurden, M.; Oldenburg, H.S.A.; Hunter, M.S.; Kieffer, J.M.; Stuiver, M.M.; Gerritsma, M.A.; Menke-Pluymers, M.B.E.; Plaisier, P.W.; Rijna, H.; et al. Efficacy of cognitive behavioral therapy and physical exercise in alleviating treatment-induced menopausal symptoms in patients with breast cancer: Results of a randomized, controlled, multicenter trial. J. Clin. Oncol. 2012, 30, 4124–4133. [Google Scholar] [CrossRef]
- Gary, R.A.; Cress, M.E.; Higgins, M.K.; Smith, A.L.; Dunbar, S.B. Combined aerobic and resistance exercise program improves task performance in patients with heart failure. Arch. Phys. Med. Rehabil. 2011, 92, 1371–1381. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.F.; Pei, D.; Chi, M.J.; Jeng, C. An investigation and comparison of the effectiveness of different exercise programmes in improving glucose metabolism and pancreatic β cell function of type 2 diabetes patients. Int. J. Clin. Pract. 2015, 69, 1159–1170. [Google Scholar] [CrossRef]
- Peels, D.A.; Van Stralen, M.M.; Bolman, C.; Golsteijn, R.H.J.; De Vries, H.; Mudde, A.N.; Lechner, L. Development of web-based computer-tailored advice to promote physical activity among people older than 50 years. J. Med. Internet Res. 2012, 14, e39. [Google Scholar] [CrossRef] [Green Version]
- Van Stralen, M.M.; Kok, G.; De Vries, H.; Mudde, A.N.; Bolman, C.; Lechner, L. The Active plus protocol: Systematic development of two theory- and evidence-based tailored physical activity interventions for the over-fifties. BMC Public Health 2008, 8, 399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boekhout, J.M.; Peels, D.A.; Berendsen, B.A.J.; Bolman, C.A.W.; Lechner, L. An eHealth intervention to promote physical activity and social network of single, chronically impaired older adults: Adaptation of an existing intervention using intervention mapping. JMIR Res. Protoc. 2017, 6, e230. [Google Scholar] [CrossRef] [PubMed]
- Peels, D.A.; Bolman, C.; Golsteijn, R.H.J.; De Vries, H.; Mudde, A.N.; Van Stralen, M.M.; Lechner, L. Long-term efficacy of a printed or a Web-based tailored physical activity intervention among older adults. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peels, D.A.; Van Stralen, M.M.; Bolman, C.; Golsteijn, R.H.J.; De Vries, H.; Mudde, A.N.; Lechner, L. The differentiated effectiveness of a printed versus a Web-based tailored physical activity intervention among adults aged over 50. Health Educ. Res. 2014, 29, 870–882. [Google Scholar] [CrossRef] [Green Version]
- Boekhout, J.M.; Berendsen, B.A.J.; Peels, D.A.; Bolman, C.A.W.; Lechner, L. Evaluation of a computer-tailored healthy ageing intervention to promote physical activity among single older adults with a chronic disease. Int. J. Environ. Res. Public Health 2018, 15, 346. [Google Scholar] [CrossRef] [Green Version]
- Shephard, R.J. Limits to the measurement of habitual physical activity by questionnaires. Br. J. Sports Med. 2003, 37, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Skender, S.; Ose, J.; Chang-Claude, J.; Paskow, M.; Brühmann, B.; Siegel, E.M.; Steindorf, K.; Ulrich, C.M. Accelerometry and physical activity questionnaires—A systematic review. BMC Public Health 2016, 16, 515. [Google Scholar] [CrossRef] [Green Version]
- Bassett, D.R.; Troiano, R.P.; Mcclain, J.J.; Wolff, D.L. Accelerometer-based physical activity: Total volume per day and standardized measures. Med. Sci. Sports Exerc. 2015, 47, 833–838. [Google Scholar] [CrossRef]
- Harris, T.J.; Owen, C.G.; Victor, C.R.; Adams, R.; Ekelund, U.; Cook, D.G. A comparison of questionnaire, accelerometer, and pedometer: Measures in older people. Med. Sci. Sports Exerc. 2009, 41, 1392–1402. [Google Scholar] [CrossRef]
- Warren, J.M.; Ekelund, U.; Besson, H.; Mezzani, A.; Geladas, N.; Vanhees, L. Assessment of physical activity—A review of methodologies with reference to epidemiological research: A report of the exercise physiology section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Fishman, E.; Böcker, L.; Helbich, M. Adult active transport in The Netherlands: An analysis of its contribution to physical activity requirements. PLoS ONE 2015, 10, e0121871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falck, R.S.; McDonald, S.M.; Beets, M.W.; Brazendale, K.; Liu-Ambrose, T. Measurement of physical activity in older adult interventions: A systematic review. Br. J. Sports Med. 2016, 50, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Volders, E.; Bolman, C.A.W.; De Groot, R.H.M.; Lechner, L. The effect of Active Plus, a computer-tailored physical activity intervention, on cognitive functioning of elderly people with chronic illness(es)—Study protocol for a randomized controlled trial. BMC Public Health 2019, 19, 1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haahr, M. RANDOM.ORG: True Random Number Service. Available online: https://random.org (accessed on 15 January 2018).
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Weinstein, N.D. The precaution adoption process. Health Psychol. 1988, 7, 355–386. [Google Scholar] [CrossRef]
- De Vries, H.; Mesters, I.; Van’t Riet, J.; Willems, K.; Reubsaet, A. Motives of Belgian adolescents for using sunscreen: The role of action plans. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1360–1366. [Google Scholar] [CrossRef] [Green Version]
- Vohs, K.D.; Baumeister, R.F. Handbook of Self-Regulation: Research, Theory, and Applications, 3rd ed.; (Hardcover); The Guilford Press: New York, NY, USA, 2016; ISBN 1-57230-991-1. [Google Scholar]
- Gorman, E.; Hanson, H.M.; Yang, P.H.; Khan, K.M.; Liu-Ambrose, T.; Ashe, M.C. Accelerometry analysis of physical activity and sedentary behavior in older adults: A systematic review and data analysis. Eur. Rev. Aging Phys. Act. 2014, 11, 35–49. [Google Scholar] [CrossRef] [Green Version]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practical considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Choi, L.; Ward, S.C.; Schnelle, J.F.; Buchowski, M.S. Assessment of wear/nonwear time classification algorithms for triaxial accelerometer. Med. Sci. Sports Exerc. 2012, 44, 2009–2016. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. J. Sci. Med. Sport 2011, 14, 411–416. [Google Scholar] [CrossRef]
- Aguilar-Farías, N.; Brown, W.J.; Peeters, G.M.E.E. ActiGraph GT3X+ cut-points for identifying sedentary behaviour in older adults in free-living environments. J. Sci. Med. Sport 2014, 17, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Wendel-Vos, G.C.W.; Schuit, A.J.; Saris, W.H.; Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef] [Green Version]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, L.M.; Singleton, J.F. What do we mean by older adult and physical activity? Reviewing the use of these terms in recent research. Act. Adapt. Aging 2017, 41, 22–46. [Google Scholar] [CrossRef]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.H.; Zhao, Y.; Yau, K.K.W.; Xiang, L. How to analyze longitudinal multilevel physical activity data with many zeros? Prev. Med. (Baltim.) 2010, 51, 476–481. [Google Scholar] [CrossRef]
- Baldwin, S.A.; Fellingham, G.W.; Baldwin, A.S. Statistical models for multilevel skewed physical activity data in health research and behavioral medicine. Health Psychol. 2016, 35, 552–562. [Google Scholar] [CrossRef]
- Chakraborty, H.; Gu, H. A Mixed Model Approach for Intent-To-Treat Analysis in Longitudinal Clinical Trials with Missing Values; RTI International: Research Triangle Park, NC, USA, 2009. [Google Scholar]
- Twisk, J.W.R. Applied Multilevel Analysis: A Practical Guide for Medical Researchers; Cambridge University Press: Cambridge, UK, 2006; ISBN 9780511610806. [Google Scholar]
- R Core Team: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: http://www.R-project.org/ (accessed on 19 February 2020).
- Conn, V.S.; Hafdahl, A.R.; Brown, S.A.; Brown, L.M. Meta-analysis of patient education interventions to increase physical activity among chronically ill adults. Patient Educ. Couns. 2008, 70, 157–172. [Google Scholar] [CrossRef] [Green Version]
- Van Der Mispel, C.; Poppe, L.; Crombez, G.; Verloigne, M.; De Bourdeaudhuij, I. A self-regulation-based eHealth intervention to promote a healthy lifestyle: Investigating user and website characteristics related to attrition. J. Med. Internet Res. 2017, 19, e241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritterband, L.M.; Thorndike, F.P.; Cox, D.J.; Kovatchev, B.P.; Gonder-Frederick, L.A. A behavior change model for internet interventions. Ann. Behav. Med. 2009, 38, 18–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wentzel, J.; Van der Vaart, R.; Bohlmeijer, E.T.; Van Gemert-Pijnen, J.E.W.C. Mixing online and face-to-face therapy: How to benefit from blended care in mental health care. JMIR Ment. Health 2016, 3, e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehra, S.; Visser, B.; Dadema, T.; van den Helder, J.; Engelbert, R.H.; Weijs, P.J.; Kröse, B.J. Translating behavior change principles into a blended exercise intervention for older adults: Design study. JMIR Res. Protoc. 2018, 7, e117. [Google Scholar] [CrossRef]
- Kloek, C.J.J.; Van Dongen, J.M.; De Bakker, D.H.; Bossen, D.; Dekker, J.; Veenhof, C. Cost-effectiveness of a blended physiotherapy intervention compared to usual physiotherapy in patients with hip and/or knee osteoarthritis: A cluster randomized controlled trial. BMC Public Health 2018, 18, 1082. [Google Scholar] [CrossRef]
- Wagner, A.L.; Keusch, F.; Yan, T.; Clarke, P.J. The impact of weather on summer and winter exercise behaviors. J. Sport Health Sci. 2019, 8, 39–45. [Google Scholar] [CrossRef]
- Volksgezondheidenzorg.Info Chronische Aandoeningen en Multimorbiditeit|Cijfers & Context|Huidige Situatie. Available online: https://www.volksgezondheidenzorg.info/onderwerp/chronische-ziekten-en-multimorbiditeit/cijfers-context/huidige-situatie#node-prevalentie-multimorbiditeit-naar-aantal-chronische-aandoeningen (accessed on 19 February 2020).
- CBS StatLine—Leefstijl en (Preventief) Gezondheidsonderzoek; Persoonskenmerken. Available online: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/83021NED/table?ts=1522312658353 (accessed on 19 February 2020).
- Eysenbach, G. The law of attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef]
- Chen, S.Y.; Feng, Z.; Yi, X. A general introduction to adjustment for multiple comparisons. J. Thorac. Dis. 2017, 9, 1725–1729. [Google Scholar] [CrossRef] [Green Version]
- Peels, D.A.; De Vries, H.; Bolman, C.; Golsteijn, R.H.J.; Van Stralen, M.M.; Mudde, A.N.; Lechner, L. Differences in the use and appreciation of a web-based or printed computer-tailored physical activity intervention for people aged over 50 years. Health Educ. Res. 2013, 28, 715–731. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Control Group | Intervention Group | p-Value | |
|---|---|---|---|
| (N = 325) | (N = 260) | ||
| Demographic characteristics | |||
| Age in years, mean (SD) | 74.46 (6.22) | 74.20 (6.60) | 0.62 |
| Gender, N (%) | 0.59 | ||
| Male | 164 (50.5%) | 138 (53.1%) | |
| Female | 161 (49.5%) | 122 (46.9%) | |
| Marital status, N (%) | 0.09 | ||
| Living single | 50 (16.6%) | 56 (22.6%) | |
| Living together | 252 (83.4%) | 192 (77.4%) | |
| Education, N (%) | 0.54 | ||
| Low | 151 (50.3%) | 127 (52.3%) | |
| Middle | 60 (20.0%) | 54 (22.2%) | |
| High | 89 (29.7%) | 62 (25.5%) | |
| Health-related characteristics | |||
| BMI, median (IQR) ꝉ | 26.9 (24.1–29.4) | 26.9 (24.4–29.8) | 0.35 |
| Degree of impairment, N (%) | 0.39 | ||
| Little impaired | 34 (11.1%) | 29 (11.6%) | |
| Medium impaired | 134 (43.8%) | 123 (49.0%) | |
| Very impaired | 138 (45.1%) | 99 (39.4%) | |
| Objective PA characteristics | |||
| LPA, mean min/wk (SD) | 2486 (641) | 2494 (674) | 0.88 |
| MVPA, median min/wk (IQR) ꝉ | 145 (57–290) | 142 (61–261) | 0.70 |
| Self-reported PA characteristics | |||
| Household activities | |||
| Number of OACI performed, N (%) | 265 (87.7%) | 223 (90.7%) | 0.35 |
| MVPA, median min/wk (IQR) ꝉ | 690 (360–1050) | 660 (330–1170) | 0.88 |
| Walking | |||
| Number of OACI performed, N (%) | 209 (69.9%) | 175 (70.3%) | 0.99 |
| MVPA, median min/wk (IQR) ꝉ | 180 (90–360) | 210 (90–360) | 0.99 |
| Cycling | |||
| Number of OACI performed, N (%) | 150 (50.2%) | 114 (45.8%) | 0.35 |
| MVPA, median min/wk (IQR) ꝉ | 180 (76.3–420) | 150 (90–360) | 0.64 |
| Gardening | |||
| Number of OACI performed, N (%) | 155 (51.8%) | 122 (49.0%) | 0.56 |
| MVPA, median min/wk (IQR) ꝉ | 180 (100–360) | 180 (92.5–360) | 0.61 |
| Odd-jobs | |||
| Number of OACI performed, N (%) | 100 (33.4%) | 87 (34.9%) | 0.78 |
| MVPA, median min/wk (IQR) ꝉ | 150 (60–480) | 180 (67.5–405) | 0.99 |
| Sports activities | |||
| Number of OACI performed, N (%) | 152 (50.8%) | 134 (53.8%) | 0.54 |
| MVPA, median min/wk (IQR) ꝉ | 150 (90–300) | 140 (75–262.5) | 0.67 |
| Measurement | Control Group | Intervention Group | |||
|---|---|---|---|---|---|
| N | Mean (SD) | N | Mean (SD) | ||
| Objective PA | |||||
| LPA min/wk | Baseline | 315 | 2486 (641) | 254 | 2494 (674) |
| 6 months | 267 | 2374 (610) | 178 | 2389 (595) | |
| 12 months | 246 | 2414 (641) | 164 | 2455 (585) | |
| MVPA min/wk | Baseline | 315 | 210 (206) | 254 | 193 (181) |
| 6 months | 267 | 191 (176) | 178 | 204 (184) | |
| 12 months | 246 | 206 (197) | 164 | 200 (206) | |
| Self-reported PA | |||||
| Household activities min/wk | Baseline | 306 | 763 (808) | 251 | 753 (715) |
| 6 months | 270 | 672 (663) | 177 | 747 (637) | |
| 12 months | 263 | 648 (701) | 171 | 719 (638) | |
| Walking min/wk | Baseline | 306 | 212 (346) | 251 | 187 (252) |
| 6 months | 270 | 193 (315) | 177 | 248 (340) | |
| 12 months | 263 | 185 (279) | 171 | 216 (257) | |
| Cycling min/wk | Baseline | 306 | 163 (349) | 251 | 137 (308) |
| 6 months | 270 | 87 (155) | 177 | 142 (266) | |
| 12 months | 263 | 135 (241) | 171 | 155 (270) | |
| Gardening min/wk | Baseline | 306 | 141 (241) | 251 | 152 (286) |
| 6 months | 270 | 80 (251) | 177 | 110 (253) | |
| 12 months | 263 | 149 (323) | 171 | 186 (317) | |
| Odd-jobs min/wk | Baseline | 306 | 130 (350) | 251 | 112 (266) |
| 6 months | 270 | 124 (308) | 177 | 120 (291) | |
| 12 months | 263 | 100 (312) | 171 | 113 (266) | |
| Sports activities min/wk | Baseline | 306 | 115 (197) | 251 | 119 (209) |
| 6 months | 270 | 113 (171) | 177 | 149 (237) | |
| 12 months | 263 | 109 (171) | 171 | 131 (211) | |
| Effect After 6 Months | Effect After 12 Months | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Coeff. | SE | 95% CI | p | Coeff. | SE | 95% CI | p | |
| Objective PA | |||||||||
| LPA min/wk | 529 | −18.47 | 44.95 | −106.6; 69.6 | 0.68 | 2.25 | 46.32 | −88.53; 93.02 | 0.96 |
| MVPA min/wk 1 | 529 | 0.04 | 0.03 | −0.02; 0.10 | 0.20 | −0.00 | 0.03 | −0.06; 0.06 | 0.93 |
| Self-reported PA | |||||||||
| Household activities | |||||||||
| Likelihood to perform 2 | 533 | 0.13 | 0.60 | −1.65; 1.81 | 0.83 | 0.12 | 0.58 | −2.09; 1.56 | 0.84 |
| MVPA min/wk 3 | 505 | 0.10 | 0.08 | −0.30; 0.56 | 0.16 | 0.13 | 0.08 | −0.18; 0.57 | 0.08 |
| Walking | |||||||||
| Likelihood to perform 2 | 533 | 0.68 | 0.40 | 0.01; 1.48 | 0.09 | 0.84 | 0.40 | 0.27; 1.62 | 0.04ꝉ |
| MVPA min/wk 3 | 457 | 0.16 | 0.09 | −0.23; 0.66 | 0.08 | 0.15 | 0.09 | −0.19; 0.54 | 0.09 |
| Cycling | |||||||||
| Likelihood to perform 2 | 533 | 1.12 | 0.44 | 0.28; 1.93 | 0.01 | 0.57 | 0.45 | −0.25; 1.43 | 0.20 |
| MVPA min/wk 3 | 312 | 0.34 | 0.12 | −0.10; 1.02 | 0.005 | 0.28 | 0.12 | −0.13; 0.86 | 0.02 |
| Gardening | |||||||||
| Likelihood to perform 2 | 533 | 0.77 | 0.38 | 0.09; 1.41 | 0.04 | 0.36 | 0.37 | −0.23; 1.15 | 0.34 |
| MVPA min/wk 3 | 328 | −0.11 | 0.13 | −0.65; 0.45 | 0.40 | 0.05 | 0.11 | −0.39; 0.61 | 0.67 |
| Odd-jobs | |||||||||
| Likelihood to perform2 | 533 | 0.14 | 0.38 | −0.49; 0.88 | 0.72 | 0.16 | 0.39 | −0.57; 0.92 | 0.67 |
| MVPA min/wk 3 | 267 | 0.08 | 0.15 | −0.53; 0.64 | 0.60 | 0.20 | 0.15 | −0.39; 0.85 | 0.19 |
| Sports activities | |||||||||
| Likelihood to perform 2 | 533 | 0.38 | 0.39 | −0.18; 1.04 | 0.32 | 0.34 | 0.39 | −0.27; 1.01 | 0.38 |
| MVPA min/wk 3 | 360 | 0.04 | 0.09 | −0.43; 0.64 | 0.62 | 0.09 | 0.09 | −0.44; 0.66 | 0.33 |
| Subgroup | Effect After 6 Months | Effect After 12 Months | ||||||
|---|---|---|---|---|---|---|---|---|
| N | Coeff. | SE | p | Coeff. | SE | p | ||
| Objective PA | ||||||||
| LPA min/wk | BMI <30 kg/ m2 | 410 | −43.04 | 50.23 | 0.39 | −40.91 | 51.82 | 0.43 |
| BMI ≥30 kg/ m2 | 119 | 74.88 | 99.44 | 0.45 | 169.18 | 101.74 | 0.096 | |
| Self-reported PA | ||||||||
| Likelihood to perform walking 1 | Little impaired | 53 | −2.26 | 1.67 | 0.18 | 12.07 | 418.04 | 0.98 |
| Medium/very impaired | 480 | 0.87 | 0.42 | 0.04 ꝉ | 0.81 | 0.42 | 0.054 | |
| Likelihood to perform odd-jobs 1 | <80 years | 420 | −0.04 | 0.41 | 0.92 | −0.16 | 0.42 | 0.70 |
| ≥80 years | 113 | 1.35 | 1.09 | 0.21 | 2.98 | 1.26 | 0.02 | |
| MVPA min/wk of household activities 2 | Low education | 257 | 0.11 | 0.11 | 0.32 | 0.13 | 0.11 | 0.24 |
| Middle education | 106 | 0.44 | 0.17 | 0.01 | 0.22 | 0.17 | 0.21 | |
| High education | 142 | −0.14 | 0.14 | 0.31 | 0.07 | 0.14 | 0.62 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volders, E.; Bolman, C.A.W.; de Groot, R.H.M.; Verboon, P.; Lechner, L. The Effect of Active Plus, a Computer-Tailored Physical Activity Intervention, on the Physical Activity of Older Adults with Chronic Illness(es)—A Cluster Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 2590. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072590
Volders E, Bolman CAW, de Groot RHM, Verboon P, Lechner L. The Effect of Active Plus, a Computer-Tailored Physical Activity Intervention, on the Physical Activity of Older Adults with Chronic Illness(es)—A Cluster Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(7):2590. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072590
Chicago/Turabian StyleVolders, Esmee, Catherine A. W. Bolman, Renate H. M. de Groot, Peter Verboon, and Lilian Lechner. 2020. "The Effect of Active Plus, a Computer-Tailored Physical Activity Intervention, on the Physical Activity of Older Adults with Chronic Illness(es)—A Cluster Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 7: 2590. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072590