Housing Conditions, Neighborhood Physical Environment, and Secondhand Smoke Exposure at Home: Evidence from Chinese Rural-to-Urban Migrant Workers


Abstract
:1. Introduction
1.1. Poor Housing Conditions and Secondhand Smoke Exposure at Home
1.2. Poor Neighborhood Physical Environments and Secondhand Smoke Exposure at Home
2. Materials and Methods
2.1. Sample and Data Collection
2.2. Variable
2.3. Statistical Analyses
3. Results
3.1. Secondhand Smoke Exposure
3.2. Housing Conditions and Neighborhood Physical Environments
3.3. Results from Logistic Regression Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gerberding, J.L. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; Publications and Reports of the Surgeon General; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2006.
- Heiss, C.; Amabile, N.; Lee, A.C.; Real, W.M.; Schick, S.F.; Lao, D.; Wong, M.L.; Jahn, S.; Angeli, F.S.; Minasi, P.; et al. Brief Secondhand Smoke Exposure Depresses Endothelial Progenitor Cells Activity and Endothelial Function. Sustained Vascular Injury and Blunted Nitric Oxide Production. J. Am. Coll. Cardiol. 2008, 51, 1760–1771. [Google Scholar] [CrossRef] [PubMed]
- Barnoya, J.; Glantz, S.A. Cardiovascular effects of secondhand smoke: Nearly as large as smoking. Circulation 2005, 111, 2684–2698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannino, D.M.; Moorman, J.E.; Kingsley, B.; Rose, D.; Repace, J. Health Effects Related to Environmental Tobacco Smoke Exposure in Children in the United States. Arch. Pediatrics Adolesc. Med. 2001, 155, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brownson, R.C.; Eriksen, M.P.; Davis, R.M.; Warner, K.E. ENVIRONMENTAL TOBACCO SMOKE: Health Effects and Policies to Reduce Exposure. Annu. Rev. Public Health 1997, 18, 163–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Deusen, A.; Hyland, A.; Travers, M.J.; Wang, C.; Higbee, C.; King, B.A.; Alford, T.; Cummings, K.M. Secondhand smoke and particulate matter exposure in the home. Nicotine Tob. Res. 2009, 11, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Homa, D.; Neff, L.; King, B.; Caraballo, R.; Bunnell, R.; Babb, S.; Garrett, B.; Sosnoff, C.; Wang, L. Vital Signs: Disparities in Nonsmokers’ Exposure to Secondhand Smoke. Morb. Mortal. Wkly. Rep. 2015, 64, 103–108. [Google Scholar]
- Rosen, L.J.; Myers, V.; Winickoff, J.P.; Kott, J. Effectiveness of Interventions to Reduce Tobacco Smoke Pollution in Homes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2015, 12, 16043–16059. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.; Wang, L.; Lu, B.; Ferketich, A.K. Secondhand Smoke Exposure, Indoor Smoking Bans and Smoking-Related Knowledge in China. Int. J. Environ. Res. Public Health 2014, 11, 12835–12847. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.; Mph, Z.Z.; Song, X.; Xu, Y.; Wu, W. Household Smoking Restrictions Related to Secondhand Smoke Exposure in Guangdong, China : A Population Representative Survey. Nicotine Tob. Res. 2014, 16, 390–396. [Google Scholar] [CrossRef]
- Nichter, M.; Padmajam, S.; Nichter, M.; Sairu, P.; Aswathy, S.; Mini, G.K.; Bindu, V.C.; Pradeepkumar, A.S.; Thankappan, K.R. Developing a smoke free homes initiative in Kerala, India. BMC Public Health 2015, 15, 480. [Google Scholar] [CrossRef] [Green Version]
- Abdullah, A.S.; Hua, F.; Xia, X.; Hurlburt, S.; Ng, P.; MacLeod, W.; Siegel, M.; Griffiths, S.; Zhang, Z. Second-hand smoke exposure and household smoking bans in Chinese families: A qualitative study. Health Soc. Care Community 2012, 20, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Song, H.; Wang, T.; Wang, T.; Yang, H.; Gong, J.; Shen, Y.; Dai, W.; Zhou, J.; Zhu, S.; et al. Determinants of tobacco smoking among rural-to-urban migrant workers: A cross-sectional survey in Shanghai. BMC Public Health 2015, 15, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Y.; Allen, R.; Sun, T. Spatial mismatch in Beijing, China: Implications of job accessibility for Chinese low-wage workers. Habitat Int. 2014, 44, 202–210. [Google Scholar] [CrossRef]
- Guo, M.; Wang, Z. Migrant Housing in Urban China: Based on Residential Segregation and Social Exclusion Theory. Open J. Bus. Manag. 2015, 03, 281–286. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics of China. China Statistical Year Book; China Statistics Press: Beijing, China, 2018.
- Zheng, Y.; Ji, Y.; Dong, H.; Chang, C. The prevalence of smoking, second-hand smoke exposure, and knowledge of the health hazards of smoking among internal migrants in 12 provinces in China: A cross-sectional analysis. BMC Public Health 2018, 18, 655. [Google Scholar] [CrossRef]
- Gong, X.; Luo, X.; Ling, L. Prevalence and associated factors of secondhand smoke exposure among internal chinese migrant women of reproductive age: Evidence from China’s labor-force dynamic survey. Int. J. Environ. Res. Public Health 2016, 13, 371. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Liu, H.; Zhang, L. Spatiotemporal Detection and Analysis of Urban Villages in Mega City Regions of China Using High-Resolution Remotely Sensed Imagery. IEEE Trans. Geosci. Remote Sens. 2015, 53, 3639–3657. [Google Scholar] [CrossRef]
- Wang, Y.P.; Wang, Y.; Wu, J. Housing migrant workers in rapidly urbanizing regions: A study of the Chinese model in Shenzhen. House Stud. 2010, 25, 83–100. [Google Scholar] [CrossRef]
- Wu, W. Migrant housing in urban China: Choices and constraints. Urban Aff. Rev. 2002, 38, 90–119. [Google Scholar] [CrossRef]
- Zhu, P.; Zhao, S.; Wang, L.; Al Yammahi, S. Residential segregation and commuting patterns of migrant workers in China. Transp. Res. Part D Transp. Environ. 2017, 52, 586–599. [Google Scholar] [CrossRef]
- Cutler, D.M.; Glaeser, E.L.; Vigdor, J.L.; Journal, S.; June, N.; Cutler, D.M.; Glaeser, E.L.; Vigdor, J.L. The Rise and Decline of the American Ghetto. J. Political Econ. 1999, 107, 455–506. [Google Scholar] [CrossRef]
- Shertzer, A.; Walsh, R.P.; Logan, J.R. Segregation and neighborhood change in northern cities: New historical GIS data from 1900–1930. Hist. Methods 2016, 49, 187–197. [Google Scholar] [CrossRef] [PubMed]
- King, B.A.; Travers, M.J.; Cummings, K.M.; Mahoney, M.C.; Hyland, A.J. Secondhand smoke transfer in multiunit housing. Nicotine Tob. Res. 2010, 12, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- King, B.A.; Babb, S.D.; Tynan, M.A.; Gerzoff, R.B. National and state estimates of secondhand smoke infiltration among U.S. multiunit housing residents. Nicotine Tob. Res. 2013, 15, 1316–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarvis, M.J.; Strachan, D.P.; Feyerabend, C. Determinants of passive smoking in children in Edinburgh, Scotland. Am. J. Public Health 1992, 82, 1225–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, S.K.; Wai-Chung Lai, L.; Ho, D.C.W.; Chau, K.W.; Lo-Kuen Lam, C.; Hung-Fai Ng, C. Sick building syndrome and perceived indoor environmental quality: A survey of apartment buildings in Hong Kong. Habitat Int. 2009, 33, 463–471. [Google Scholar] [CrossRef]
- Ganz, M.L. The relationship between external threats and smoking in Central Harlem. Am. J. Public Health 2000, 90, 367–371. [Google Scholar]
- Cui, X.; Rockett, I.R.H.; Yang, T.; Cao, R. Work stress, life stress, and smoking among rural-urban migrant workers in China. BMC Public Health 2012, 12, 979. [Google Scholar] [CrossRef] [Green Version]
- Holmes, L.M.; Llamas, J.D.; Smith, D.; Ling, P.M. Drifting Tobacco Smoke Exposure among Young Adults in Multiunit Housing. J. Community Health 2019. [Google Scholar] [CrossRef]
- Frazer, K.; Callinan, J.E.; Mchugh, J.; van Baarsel, S.; Clarke, A.; Doherty, K.; Kelleher, C. Legislative smoking bans for reducing harms from secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst. Rev. 2016, 2, CD005992. Available online: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD005992.pub3/abstract (accessed on 11 March 2020). [CrossRef]
- Latkin, C.A.; Tseng, T.Y.; Davey-Rothwell, M.; Kennedy, R.D.; Moran, M.B.; Czaplicki, L.; Edwards, C.; Falade-Nwulia, O.; Chander, G.; Knowlton, A.R. The Relationship between Neighborhood Disorder, Social Networks, and Indoor Cigarette Smoking among Impoverished Inner-City Residents. J. Urban Health 2017, 94, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Ma, P.; Businelle, M.S.; Balis, D.S.; Kendzor, D.E. The influence of perceived neighborhood disorder on smoking cessation among urban safety net hospital patients. Drug Alcohol Depend. 2015, 156, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Holmes, L.M.; Marcelli, E.A. Neighborhood Social Cohesion and Smoking among Legal and Unauthorized Brazilian Migrants in Metropolitan Boston. J. Urban Health 2014, 91, 1175–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miles, R. Neighborhood disorder and smoking: Findings of a European urban survey. Soc. Sci. Med. 2006, 63, 2464–2475. [Google Scholar] [CrossRef]
- Patterson, J.M.; Eberly, L.E.; Ding, Y.; Hargreaves, M. Associations of smoking prevalence with individual and area level social cohesion. J. Epidemiol. Community Health 2004, 58, 692–697. [Google Scholar] [CrossRef]
- Heckathorn, D.D. Respondent-Driven Sampling: A New Approach to the Study of Hidden Populations. Soc. Probl. 1997, 44, 174–199. [Google Scholar] [CrossRef]
- Qiu, P.; Yang, Y.; Ma, X.; Liu, Q.; Wu, F.; Yuan, P.; Caine, E. Respondent-driven sampling to recruit in-country migrant workers in China: A methodological assessment. Scand. J. Public Health 2012, 40, 92–101. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, X.; Qiu, P.Y.; Ma, X.; Chou, C.P. Integrating spatial technology into studying the generational differences of migrants’ health protection status in urban China. Int. J. Equity Health 2015, 1, 14–27. [Google Scholar] [CrossRef] [Green Version]
- Rhew, I.C.; Vander Stoep, A.; Kearney, A.; Smith, N.L.; Dunbar, M.D. Validation of the Normalized Difference Vegetation Index as a Measure of Neighborhood Greenness. Ann. Epidemiol. 2011, 21, 946–952. [Google Scholar] [CrossRef] [Green Version]
- Rouse, R.W.H.; Haas, J.A.W.; Deering, D.W. Monitoring Vegetation Systems in the Great Plains with ERTS; NASA: Washington, DC, USA, 1974.
- Fong, K.C.; Hart, J.E.; James, P. A Review of Epidemiologic Studies on Greenness and Health: Updated Literature Through 2017. Curr. Environ. Health Rep. 2018, 5, 77–87. [Google Scholar] [CrossRef] [Green Version]
- Mavoa, S.; Witten, K.; McCreanor, T.; O’Sullivan, D. GIS based destination accessibility via public transit and walking in Auckland, New Zealand. J. Transp. Geogr. 2012, 20, 15–22. [Google Scholar] [CrossRef]
- Veitch, J.; Carver, A.; Salmon, J.; Abbott, G.; Ball, K.; Crawford, D.; Cleland, V.; Timperio, A. What predicts children’s active transport and independent mobility in disadvantaged neighborhoods? Heal. Place 2017, 44, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.K.; Borana, S.L. MODIS derived NDVI based time series analysis of vegetation in the Jodhpur area. Int. Arch. Photogramm. Remote Sens. Spat. Inf. Sci. ISPRS Arch. 2019, 42, 535–539. [Google Scholar]
- Kulldorff, M.; Huang, L.; Konty, K. A scan statistic for continuous data based on the normal probability model. Int. J. Health Geogr. 2009, 8, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, P.; Berg, C.; Kegler, M.; Fu, W.; Wang, J.; Zhou, X.; Liu, D.; Fu, H. Smoke-Free Homes and Home Exposure to Secondhand Smoke in Shanghai, China. Int. J. Environ. Res. Public Health 2014, 11, 12015–12028. [Google Scholar] [CrossRef] [PubMed]
- Yao, T.; Sung, H.Y.; Mao, Z.; Hu, T.; Max, W. Secondhand smoke exposure at home in rural China. Cancer Causes Control 2012, 23 (Suppl. S1), 109–115. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | All Respondents | Non-Smoking Respondents | ||
|---|---|---|---|---|
| n | Percentage | n | Percentage | |
| Gender | ||||
| Male | 948 | 51.13 | 418 | 33.41 |
| Female | 906 | 48.87 | 833 | 66.59 |
| Age 1 | 1854 | 41.92 (13.09) | 1251 | 41.68 (13.09) |
| Marital status | ||||
| Married | 1438 | 77.56 | 1003 | 80.18 |
| Not in a marital union | 416 | 22.44 | 248 | 19.82 |
| Education 1 | 1854 | 3.02 (1.11) | 1251 | 3.02 (1.13) |
| Occupation | ||||
| Construction industry | 346 | 18.66 | 152 | 12.15 |
| Manufacturing industry | 246 | 13.27 | 195 | 15.59 |
| Service industry | 1127 | 60.79 | 807 | 64.51 |
| Other categories | 135 | 7.28 | 97 | 7.75 |
| Annual income (log) 1 | 1854 | 4.52 (0.29) | 1251 | 4.48 (0.29) |
| Perceived harmfulness of secondhand smoke (SHS) | ||||
| No | 268 | 14.46 | 164 | 13.11 |
| Yes | 1586 | 85.54 | 1087 | 86.89 |
| Living with child(ren) | ||||
| No | 1571 | 84.74 | 1038 | 82.97 |
| Yes | 283 | 15.26 | 213 | 17.03 |
| Housing type | ||||
| Storied commercial building | 1166 | 62.89 | 853 | 68.19 |
| Unusual housing type | 688 | 37.11 | 398 | 31.81 |
| Number of people sharing one bedroom | ||||
| ≤2 people in one bedroom | 1318 | 71.09 | 928 | 74.18 |
| ≥3 people in one bedroom | 536 | 28.91 | 323 | 25.82 |
| Availability of facilities | ||||
| Availability of facilities | 1046 | 56.42 | 770 | 61.55 |
| Lack of facilities | 808 | 43.58 | 481 | 38.45 |
| Perceived neighborhood hygiene problem 1 | 1854 | 2.40 (0.87) | 1251 | 2.41 (0.88) |
| Perceived neighborhood noise problem 1 | 1854 | 2.88 (0.99) | 1251 | 2.86 (0.99) |
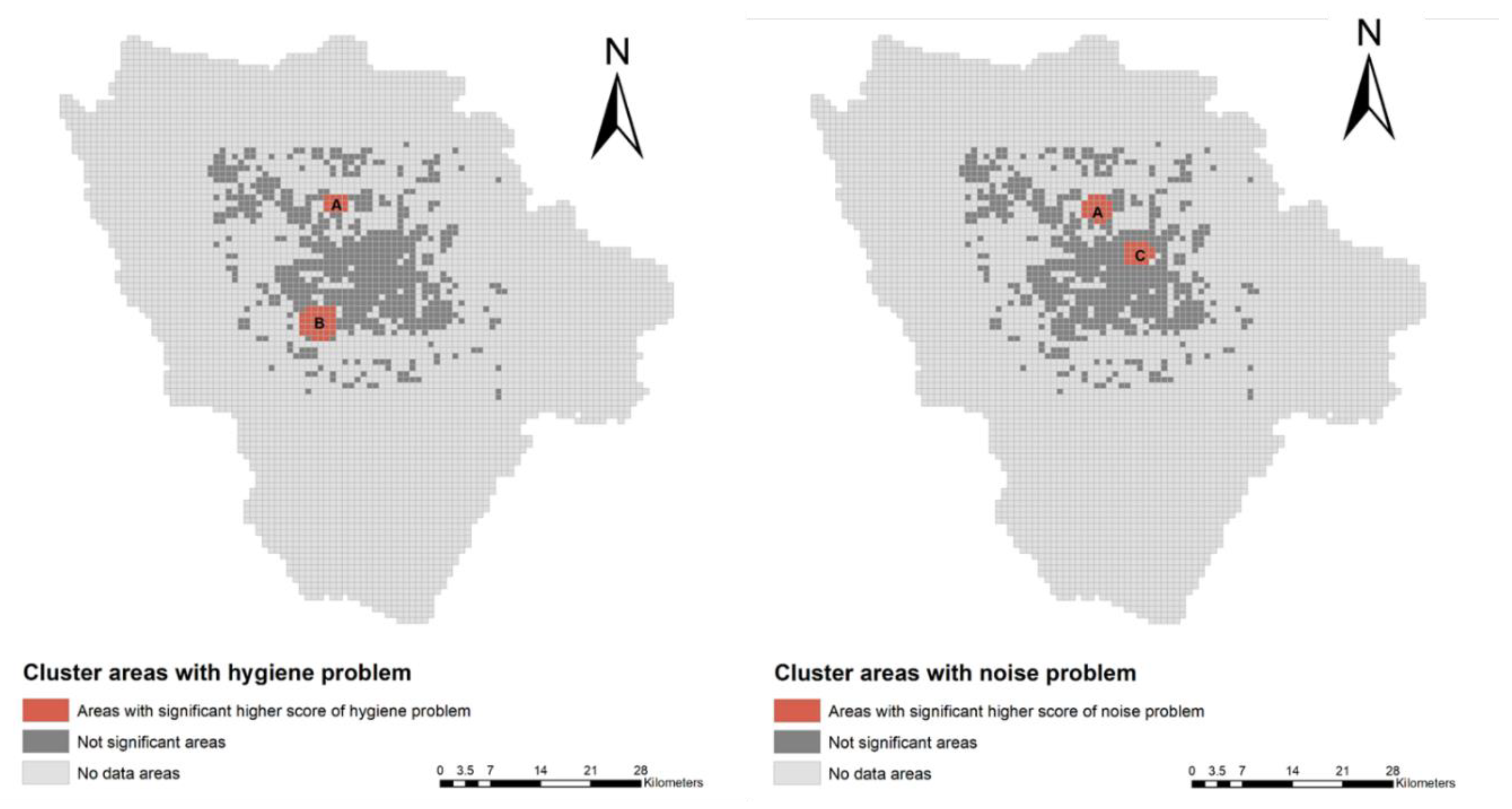
| Living in poor hygiene cluster areas | ||||
| Yes | 191 | 10.30 | 114 | 9.11 |
| No | 1663 | 89.70 | 1137 | 90.89 |
| Living in high-level noise areas | ||||
| Yes | 175 | 9.44 | 111 | 8.87 |
| No | 1679 | 90.56 | 1140 | 91.13 |
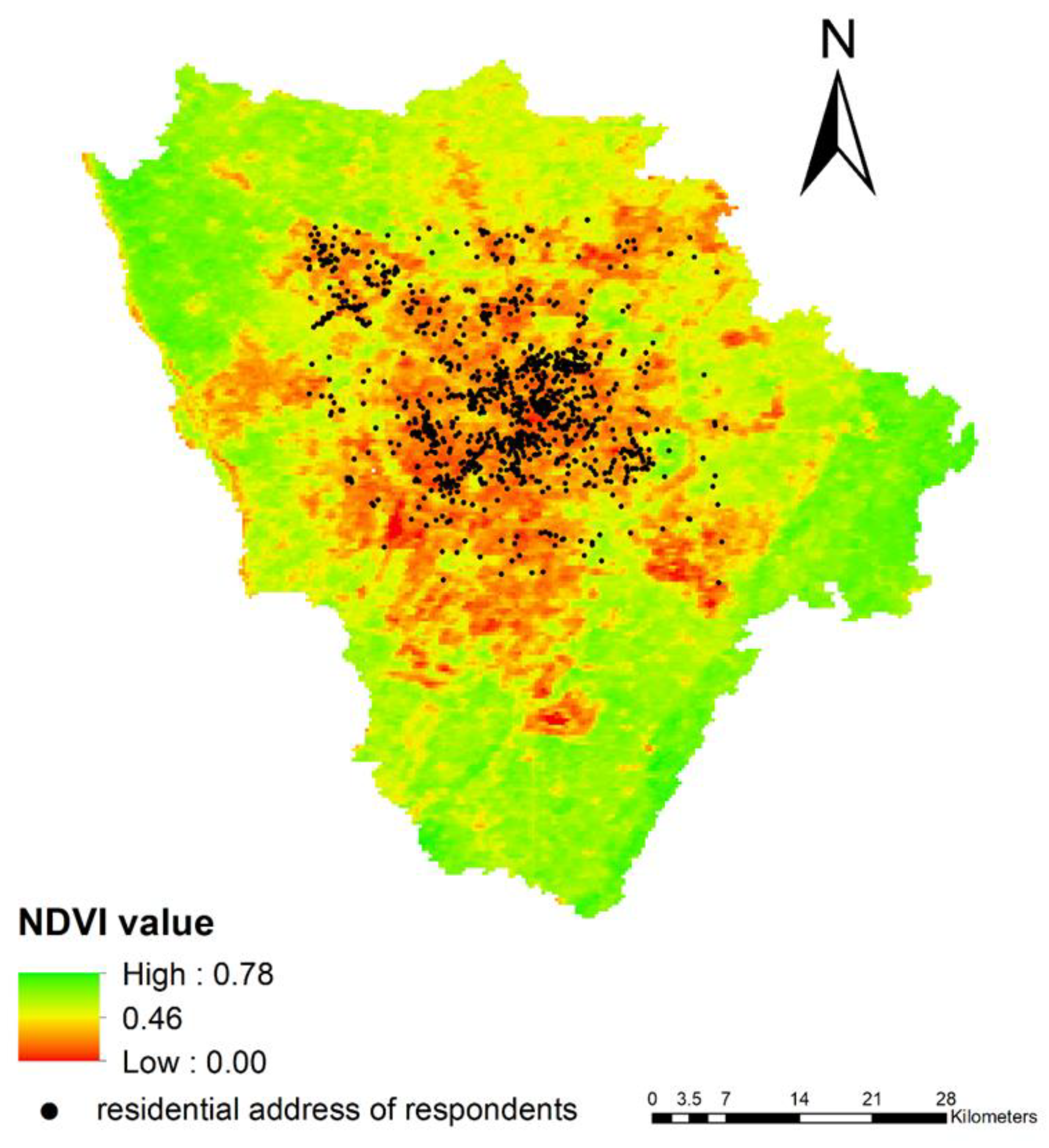
| Neighborhood greenness | ||||
| Mean Normalized Difference Vegetation Index ≤ 0.3 | 833 | 44.93 | 554 | 44.28 |
| Mean Normalized Difference Vegetation Index > 0.3 | 1021 | 55.07 | 697 | 55.72 |
| SHS exposure at home | ||||
| Never | - | - | 682 | 54.52 |
| 1–3 days per week | - | - | 109 | 8.71 |
| 4–6 days per week | 37 | 2.96 | ||
| Every day | 423 | 33.81 | ||
| Variables | OR | 95% C.I. Low | 95% C.I. High |
|---|---|---|---|
| Housing conditions | |||
| Unusual housing type | 2.09 | 1.66 | 2.63 |
| ≥3 people in one bedroom | 2.13 | 1.67 | 2.71 |
| Lack of facilities | 1.67 | 1.34 | 2.08 |
| Perceived neighborhood physical environment problems | |||
| Perceived neighborhood hygiene problem | 1.23 | 1.09 | 1.40 |
| Perceived neighborhood noise problem | 1.17 | 1.05 | 1.31 |
| Neighborhood physical environment based on scan statistics | |||
| Not living in poor hygiene cluster areas | 0.48 | 0.33 | 0.69 |
| Not living in high-level noise cluster areas | 0.35 | 0.24 | 0.51 |
| Neighborhood greenness based on sensor data | |||
| Neighborhood mean NDVI value > 0.3 | 0.78 | 0.62 | 0.96 |
| Variables | OR | 95% C.I. Low | 95% C.I. High |
|---|---|---|---|
| Housing conditions | |||
| Unusual housing type | 1.77 | 1.35 | 2.33 |
| ≥3 people in one bedroom | 1.77 | 1.35 | 2.32 |
| Lack of facilities | 1.37 | 1.06 | 1.77 |
| Perceived neighborhood physical environment problems | |||
| Perceived neighborhood hygiene problem | 1.23 | 1.08 | 1.41 |
| Perceived neighborhood noise problem | 1.17 | 1.04 | 1.31 |
| Neighborhood physical environment based on scan statistics | |||
| Not living in poor hygiene cluster areas | 0.54 | 0.36 | 0.81 |
| Not living in high-level noise cluster areas | 0.50 | 0.31 | 0.80 |
| Neighborhood greenness based on sensor data | |||
| Neighborhood mean NDVI value > 0.3 | 0.89 | 0.70 | 1.12 |
| Variables | OR | 95% C.I. Low | 95% C.I. High |
|---|---|---|---|
| Housing conditions | |||
| Unusual housing type | 1.68 | 1.22 | 2.31 |
| ≥3 people in one bedroom | 1.73 | 1.26 | 2.38 |
| Lack of facilities | 0.95 | 0.70 | 1.29 |
| Perceived neighborhood physical environment problems | |||
| Perceived neighborhood hygiene problem | 1.17 | 1.02 | 1.34 |
| Perceived neighborhood noise problem | 1.13 | 1.01 | 1.27 |
| Neighborhood greenness based on sensor data | |||
| Neighborhood mean NDVI value > 0.3 | 0.92 | 0.72 | 1.17 |
| Variables | OR | 95% C.I. Low | 95% C.I. High |
|---|---|---|---|
| Housing conditions | |||
| Unusual housing type | 1.64 | 1.19 | 2.27 |
| ≥3 people in one bedroom | 1.72 | 1.30 | 2.28 |
| Lack of facilities | 0.89 | 0.65 | 1.21 |
| Neighborhood physical environment based on scan statistics | |||
| Not living in poor hygiene cluster areas | 0.62 | 0.41 | 0.95 |
| Not living in high-level noise cluster areas | 0.58 | 0.36 | 0.93 |
| Neighborhood greenness based on sensor data | |||
| Neighborhood mean NDVI value > 0.3 | 0.91 | 0.71 | 1.15 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, C.; Yang, Y.; Xu, X.; Ma, X. Housing Conditions, Neighborhood Physical Environment, and Secondhand Smoke Exposure at Home: Evidence from Chinese Rural-to-Urban Migrant Workers. Int. J. Environ. Res. Public Health 2020, 17, 2629. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082629
Xiao C, Yang Y, Xu X, Ma X. Housing Conditions, Neighborhood Physical Environment, and Secondhand Smoke Exposure at Home: Evidence from Chinese Rural-to-Urban Migrant Workers. International Journal of Environmental Research and Public Health. 2020; 17(8):2629. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082629
Chicago/Turabian StyleXiao, Chenghan, Yang Yang, Xiaohe Xu, and Xiao Ma. 2020. "Housing Conditions, Neighborhood Physical Environment, and Secondhand Smoke Exposure at Home: Evidence from Chinese Rural-to-Urban Migrant Workers" International Journal of Environmental Research and Public Health 17, no. 8: 2629. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082629