The Effect of Maternal Depression on Infant Attachment: A Systematic Review

 ,
, 
 ,
,
Abstract
:1. Introduction
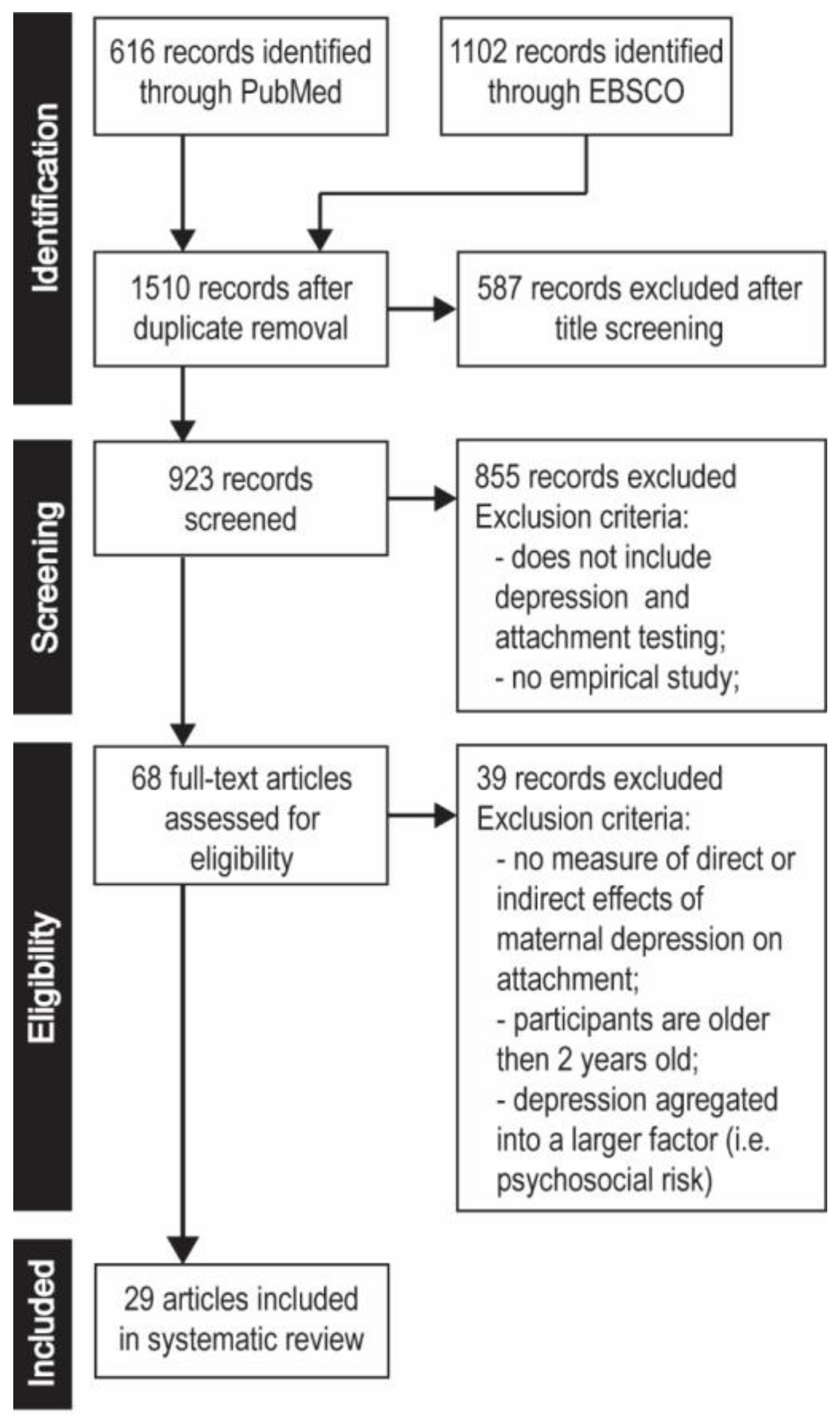
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Research Strategy and Data Extraction
2.3. Risk of Bias Assessment
2.4. Quality Assessment
- (a)
- Sample size: an adequate minimum sample size was regarded as 30 participants in each compared group;
- (b)
- Representative of study population: representative and adequate study sample (should vary in demographic characteristics);
- (c)
- Low attrition: below 30% of the initial sample;
- (d)
- Validated measuring methods: standardized with given validity and reliability; proper adaptation if the measurement method was conducted in a different country than its origin;
- (e)
- Coding experience: the authors possessed training and experience in assessing attachment;
- (f)
- Statistical analysis: appropriately described and correct;
- (g)
- Assessment procedure: double-blind procedure in the attachment assessment;
- (h)
- Conclusions which were consistent with results;
- (i)
- Aim of the study: direct/indirect assessment of the influence of depression on attachment style.
3. Results
3.1. The Influence of Major Depression on Attachment Style
3.2. The Influence of Prenatal Depression on Attachment Style
3.3. The Influence of Postnatal Depression on Attachment Style
3.3.1. High-Risk Groups
3.3.2. Type of Measurement and Timeframe of the Examination of Depression
3.3.3. Studies Conducted on Representative and Large Groups
3.4. Factors that Modify Depression—Attachment Link
3.4.1. Demographic Factors
3.4.2. Psychological Factors
3.4.3. Gynaecological-Obstetrics Factors
3.4.4. Infant Factors
3.4.5. Social Support and Single Parenting
3.4.6. Parenting and Emotional Availability
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kessler, R.C.; Bromet, E.J. The Epidemiology of Depression across Cultures. Annu. Rev. Public Health 2013, 34, 119–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Wu, X.; Lai, W.; Long, E.; Zhang, X.; Li, W.; Zhu, Y.; Chen, C.; Zhong, X.; Liu, Z.; et al. Prevalence of depression and depressive symptoms among outpatients: A systematic review and meta-analysis. BMJ Open 2017, 7, e017173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brummelte, S.; Galea, L.A.M. Postpartum depression: Etiology, treatment and consequences for maternal care. Horm. Behav. 2016, 77, 153–166. [Google Scholar] [CrossRef] [PubMed]
- van de Loo, K.F.E.; Vlenterie, R.; Nikkels, S.J.; Merkus, P.J.F.M.; Roukema, J.; Verhaak, C.M.; Roeleveld, N.; van Gelder, M.M.H.J. Depression and anxiety during pregnancy: The influence of maternal characteristics. Birth 2018, 45, 478–489. [Google Scholar] [CrossRef]
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef]
- Stuart-Parrigon, K.; Stuart, S. Perinatal Depression: An Update and Overview. Curr. Psychiatry Rep. 2014, 16, 467–476. [Google Scholar] [CrossRef] [Green Version]
- Wisner, K.L.; Moses-Kolko, E.L.; Sit, D.K.Y. Postpartum depression: A disorder in search of a definition. Arch. Womens Ment. Health 2010, 13, 37–40. [Google Scholar] [CrossRef]
- O’Hara, M.W.; McCabe, J.E. Postpartum Depression: Current Status and Future Directions. Annu. Rev. Clin. Psychol. 2013, 9, 379–407. [Google Scholar] [CrossRef]
- Banti, S.; Mauri, M.; Oppo, A.; Borri, C.; Rambelli, C.; Ramacciotti, D.; Montagnani, M.S.; Camilleri, V.; Cortopassi, S.; Rucci, P.; et al. From the third month of pregnancy to 1 year postpartum. Prevalence, incidence, recurrence, and new onset of depression. Results from the Perinatal Depression–Research & Screening Unit study. Compr. Psychiatry 2011, 52, 343–351. [Google Scholar]
- Gavin, N.I.; Gaynes, B.N.; Lohr, K.N.; Meltzer-Brody, S.; Gartlehner, G.; Swinson, T. Perinatal Depression: A Systematic Review of Prevalence and Incidence. Obstet. Gynecol. 2005, 106, 1071–1083. [Google Scholar] [CrossRef]
- Gelaye, B.; Rondon, M.B.; Araya, R.; Williams, M.A. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry 2016, 3, 973–982. [Google Scholar] [CrossRef] [Green Version]
- Guo, N.; Robakis, T.; Miller, C.; Butwick, A. Prevalence of Depression among Women of Reproductive Age in the United States. Obstet. Gynecol. 2018, 131, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Dubber, S.; Reck, C.; Müller, M.; Gawlik, S. Postpartum bonding: The role of perinatal depression, anxiety and maternal–fetal bonding during pregnancy. Arch. Womens Ment. Health 2015, 18, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.R.; O’Hara, M.W.; Stuart, S.; Gorman, L.L.; Larsen, K.E.; Coy, K.C. Effective treatment for postpartum depression is not sufficient to improve the developing mother–child relationship. Dev. Psychopathol. 2007, 19, 585–602. [Google Scholar] [CrossRef]
- O’Higgins, M.; Roberts, I.S.J.; Glover, V.; Taylor, A. Mother-child bonding at 1 year; associations with symptoms of postnatal depression and bonding in the first few weeks. Arch. Womens Ment. Health 2013, 16, 381–389. [Google Scholar] [CrossRef]
- Perry, D.F.; Ettinger, A.K.; Mendelson, T.; Le, H.-N. Prenatal depression predicts postpartum maternal attachment in low-income Latina mothers with infants. Infant Behav. Dev. 2011, 34, 339–350. [Google Scholar] [CrossRef]
- Nonnenmacher, N.; Noe, D.; Ehrenthal, J.C.; Reck, C. Postpartum bonding: The impact of maternal depression and adult attachment style. Arch. Womens Ment. Health 2016, 19, 927–935. [Google Scholar] [CrossRef]
- Klier, C.M. Mother–infant bonding disorders in patients with postnatal depression: The Postpartum Bonding Questionnaire in clinical practice. Arch. Womens Ment. Health 2006, 9, 289–291. [Google Scholar] [CrossRef]
- Tronick, E.; Reck, C. Infants of Depressed Mothers. Harv. Rev. Psychiatry 2009, 17, 147–156. [Google Scholar] [CrossRef]
- Brennan, P.A.; Hammen, C.; Andersen, M.J.; Bor, W.; Najman, J.M.; Williams, G.M. Chronicity, severity, and timing of maternal depressive symptoms: Relationships with child outcomes at age 5. Dev. Psychol. 2000, 36, 759–766. [Google Scholar] [CrossRef]
- Trapolini, T.; McMahon, C.A.; Ungerer, J.A. The effect of maternal depression and marital adjustment on young children’s internalizing and externalizing behaviour problems. Child Care Health Dev. 2007, 33, 794–803. [Google Scholar] [CrossRef] [PubMed]
- Murray, L.; Arteche, A.; Fearon, P.; Halligan, S.; Croudace, T.; Cooper, P. The effects of maternal postnatal depression and child sex on academic performance at age 16 years: A developmental approach: PND & child cognitive and academic outcomes. J. Child Psychol. Psychiatry 2010, 51, 1150–1159. [Google Scholar] [PubMed]
- Feldman, R.; Granat, A.; Pariente, C.; Kanety, H.; Kuint, J.; Gilboa-Schechtman, E. Maternal Depression and Anxiety Across the Postpartum Year and Infant Social Engagement, Fear Regulation, and Stress Reactivity. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 919–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granat, A.; Gadassi, R.; Gilboa-Schechtman, E.; Feldman, R. Maternal depression and anxiety, social synchrony, and infant regulation of negative and positive emotions. Emotion 2017, 17, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.Ś.; Garrity-Rokous, F.E.; Chazan-Cohen, R.; Little, C.; Briggs-Gowan, M.J. Maternal Depression and Comorbidity: Predicting Early Parenting, Attachment Security, and Toddler Social-Emotional Problems and Competencies. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 18–26. [Google Scholar] [CrossRef]
- Conroy, S.; Marks, M.N.; Schacht, R.; Davies, H.A.; Moran, P. The impact of maternal depression and personality disorder on early infant care. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 285–292. [Google Scholar] [CrossRef]
- Conroy, S.; Pariante, C.M.; Marks, M.N.; Davies, H.A.; Farrelly, S.; Schacht, R.; Moran, P. Maternal Psychopathology and Infant Development at 18 Months: The Impact of Maternal Personality Disorder and Depression. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 51–61. [Google Scholar] [CrossRef]
- Wang, Y.; Dix, T. Patterns of depressive parenting: Why they occur and their role in early developmental risk. J. Fam. Psychol. 2013, 27, 884–895. [Google Scholar] [CrossRef]
- Kingston, D.; Tough, S.; Whitfield, H. Prenatal and Postpartum Maternal Psychological Distress and Infant Development: A Systematic Review. Child Psychiatry Hum. Dev. 2012, 43, 683–714. [Google Scholar] [CrossRef]
- Letourneau, N.L.; Dennis, C.-L.; Cosic, N.; Linder, J. The effect of perinatal depression treatment for mothers on parenting and child development: A systematic review. Depress. Anxiety 2017, 34, 928–966. [Google Scholar] [CrossRef]
- Schore, A.N. Effects of a secure attachment relationship on right brain development, affect regulation, and infant mental health. Infant Ment. Health J. 2001, 22, 7–66. [Google Scholar] [CrossRef]
- Eiden, R.D.; Edwards, E.P.; Leonard, K.E. Mother–infant and father–infant attachment among alcoholic families. Dev. Psychopathol. 2002, 14, 253–278. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vu-Ngoc, H.; Elawady, S.S.; Mehyar, G.M.; Abdelhamid, A.H.; Mattar, O.M.; Halhouli, O.; Vuong, N.L.; Ali, C.D.M.; Hassan, U.H.; Kien, N.D.; et al. Quality of flow diagram in systematic review and/or meta-analysis. PLoS ONE 2018, 13, e0195955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyons-Ruth, K.; Connell, D.B.; Grunebaum, H.U.; Botein, S. Infants at Social Risk: Maternal Depression and Family Support Services as Mediators of Infant Development and Security of Attachment. Child Dev. 1990, 61, 85–98. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons Ltd: Chichester, UK, 2011; ISBN 978-0-470-05796-4. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Green, S., Eds.; John Wiley & Sons Ltd: Chichester, UK, 2011; pp. 8.1–8.53. ISBN 978-0-470-05796-4. [Google Scholar]
- Kjaergard, L.L.; Villumsen, J.; Gluud, C. Reported Methodologic Quality and Discrepancies between Large and Small Randomized Trials in Meta-Analyses. Ann. Intern. Med. 2001, 135, 982–989. [Google Scholar] [CrossRef]
- Gratz, K.L.; Kiel, E.J.; Latzman, R.D.; Elkin, T.D.; Moore, S.A.; Tull, M.T. Meternal Borderline Personality Pathology and Infant Emotion Regulation: Examining Emotion-Related Difficulties and Infant Attachment. J. Personal. Disord. 2014, 28, 52–69. [Google Scholar] [CrossRef]
- Gravener, J.A.; Rogosch, F.A.; Oshri, A.; Narayan, A.J.; Cicchetti, D.; Toth, S.L. The Relations among Maternal Depressive Disorder, Maternal Expressed Emotion, and Toddler Behavior Problems and Attachment. J. Abnorm. Child Psychol. 2012, 40, 803–813. [Google Scholar] [CrossRef] [Green Version]
- Laurent, H.K.; Ablow, J.C. The missing link: Mothers’ neural response to infant cry related to infant attachment behaviors. Infant Behav. Dev. 2012, 35, 761–772. [Google Scholar] [CrossRef] [Green Version]
- Ludmer, J.A.; Gonzalez, A.; Kennedy, J.; Masellis, M.; Meinz, P.; Atkinson, L. Association between maternal childhood maltreatment and mother-infant attachment disorganization: Moderation by maternal oxytocin receptor gene and cortisol secretion. Horm. Behav. 2018, 102, 23–33. [Google Scholar] [CrossRef]
- Lyons-Ruth, K.; Zoll, D.; Connell, D.; Grunebaum, H.U. The depressed mother and her one-year-old infant: Environment, interaction, attachment, and infant development. New Dir. Child Adolesc. Dev. 1986, 1986, 61–82. [Google Scholar] [CrossRef] [PubMed]
- Hayes, L.J.; Goodman, S.H.; Carlson, E. Maternal antenatal depression and infant disorganized attachment at 12 months. Attach. Hum. Dev. 2013, 15, 133–153. [Google Scholar] [CrossRef] [PubMed]
- Murray, L. The Impact of Postnatal Depression on Infant Development. J. Child Psychol. Psychiatry 1992, 33, 543–561. [Google Scholar] [CrossRef] [PubMed]
- Tharner, A.; Luijk, M.P.C.M.; van IJzendoorn, M.H.; Bakermans-Kranenburg, M.J.; Jaddoe, V.W.V.; Hofman, A.; Verhulst, F.C.; Tiemeier, H. Maternal lifetime history of depression and depressive symptoms in the prenatal and early postnatal period do not predict infant–mother attachment quality in a large, population-based Dutch cohort study. Attach. Hum. Dev. 2012, 14, 63–81. [Google Scholar] [CrossRef]
- Smith-Nielsen, J.; Tharner, A.; Steele, H.; Cordes, K.; Mehlhase, H.; Vaever, M.S. Postpartum depression and infant-mother attachment security at one year: The impact of co-morbid maternal personality disorders. Infant Behav. Dev. 2016, 44, 148–158. [Google Scholar] [CrossRef]
- Toth, S.L.; Rogosch, F.A.; Sturge-Apple, M.; Cicchetti, D. Maternal Depression, Children’s Attachment Security, and Representational Development: An Organizational Perspective. Child Dev. 2009, 80, 192–208. [Google Scholar] [CrossRef] [Green Version]
- McMahon, C.A.; Barnett, B.; Kowalenko, N.M.; Tennant, C.C. Maternal attachment state of mind moderates the impact of postnatal depression on infant attachment. J. Child Psychol. Psychiatry 2006, 47, 660–669. [Google Scholar] [CrossRef]
- Tomlinson, M.; Cooper, P.; Murray, L. The Mother-Infant Relationship and Infant Attachment in a South African Peri-Urban Settlement. Child Dev. 2005, 76, 1044–1054. [Google Scholar] [CrossRef]
- Righetti-Veltema, M.; Bousquet, A.; Manzano, J. Impact of postpartum depressive symptoms on mother and her 18-month-old infant. Eur. Child Adolesc. Psychiatry 2003, 12, 75–83. [Google Scholar] [CrossRef]
- Cicchetti, D.; Rogosch, F.A.; Toth, S.L. Maternal depressive disorder and contextual risk: Contributions to the development of attachment insecurity and behavior problems in toddlerhood. Dev. Psychopathol. 1998, 10, 283–300. [Google Scholar] [CrossRef]
- Bigelow, A.E.; Beebe, B.; Power, M.; Stafford, A.-L.; Ewing, J.; Egleson, A.; Kaminer, T. Longitudinal relations among maternal depressive symptoms, maternal mind-mindedness, and infant attachment behavior. Infant Behav. Dev. 2018, 51, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Measelle, J.R.; Ablow, J.C. Contributions of early adversity to pro-inflammatory phenotype in infancy: The buffer provided by attachment security. Attach. Hum. Dev. 2018, 20, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Beeghly, M.; Partridge, T.; Tronick, E.; Muzik, M.; Rahimian Mashhadi, M.; Boeve, J.L.; Irwin, J.L. Associations between early maternal depressive symptom trajectories and toddlers’ felt security at 18 months: Are boys and girls at differential risk? Infant Ment. Health J. 2017, 38, 53–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Falco, S.; Emer, A.; Martini, L.; Rigo, P.; Pruner, S.; Venuti, P. Predictors of mother-child interaction quality and child attachment security in at-risk families. Front. Psychol. 2014, 5, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehler, K.; Wendrich, D.; Kissgen, R.; Roth, B.; Oberthuer, A.; Pillekamp, F.; Kribs, A. Mothers seeing their VLBW infants within 3 h after birth are more likely to establish a secure attachment behavior: evidence of a sensitive period with preterm infants? J. Perinatol. 2011, 31, 404–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, K.; Sarkar, P.; Glover, V.; O’Connor, T.G. Maternal Prenatal Cortisol and Infant Cognitive Development: Moderation by Infant–Mother Attachment. Biol. Psychiatry 2010, 67, 1026–1032. [Google Scholar] [CrossRef] [Green Version]
- Zaslow, M.; Bronte-Tinkew, J.; Capps, R.; Horowitz, A.; Moore, K.A.; Weinstein, D. Food Security During Infancy: Implications for Attachment and Mental Proficiency in Toddlerhood. Matern. Child Health J. 2009, 13, 66–80. [Google Scholar] [CrossRef]
- Tarabulsy, G.M.; Bernier, A.; Provost, M.A.; Maranda, J.; Larose, S.; Moss, E.; Larose, M.; Tessier, R. Another Look Inside the Gap: Ecological Contributions to the Transmission of Attachment in a Sample of Adolescent Mother-Infant Dyads. Dev. Psychol. 2005, 41, 212–224. [Google Scholar] [CrossRef]
- Sagi, A.; Koren-Karie, N.; Gini, M.; Ziv, Y.; Joels, T. Shedding Further Light on the Effects of Various Types and Quality of Early Child Care on Infant-Mother Attachment Relationship: The Haifa Study of Early Child Care. Child Dev. 2002, 73, 1166–1186. [Google Scholar] [CrossRef]
- Edhborg, M.; Lundh, W.; Seimyr, L.; Widström, A.-M. The long-term impact of postnatal depressed mood on mother-child interaction: A preliminary study. J. Reprod. Infant Psychol. 2001, 19, 61–71. [Google Scholar] [CrossRef]
- Hughes, P.; Turton, P.; Hopper, E.; McGauley, G.A.; Fonagy, P. Disorganised Attachment Behaviour among Infants Born Subsequent to Stillbirth. J. Child Psychol. Psychiatry 2001, 42, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Clarke-Stewart, K.A.; Vandell, D.L.; McCartney, K.; Owen, M.T.; Booth, C. Effects of Parental Separation and Divorce on Very Young Children. J. Fam. Psychol. 2000, 14, 304–326. [Google Scholar] [CrossRef] [PubMed]
- Donovan, W.L.; Leavitt, L.A. Maternal Self-Efficacy and Infant Attachment: Integrating Physiology, Perceptions, and Behavior. Child Dev. 1989, 60, 460. [Google Scholar] [CrossRef] [PubMed]
- Fihrer, I.; McMahon, C. Maternal state of mind regarding attachment, maternal depression and children’s family drawings in the early school years. Attach. Hum. Dev. 2009, 11, 537–556. [Google Scholar] [CrossRef]
- Fathi, F.; Mohammad-Alizadeh-Charandabi, S.; Mirghafourvand, M. Maternal self-efficacy, postpartum depression, and their relationship with functional status in Iranian mothers. Women Health 2018, 58, 188–203. [Google Scholar] [CrossRef]
- Gibbs, B.G.; Forste, R.; Lybbert, E. Breastfeeding, Parenting, and Infant Attachment Behaviors. Matern. Child Health J. 2018, 22, 579–588. [Google Scholar] [CrossRef]
- Weaver, J.M.; Schofield, T.J.; Papp, L.M. Breastfeeding duration predicts greater maternal sensitivity over the next decade. Dev. Psychol. 2018, 54, 220–227. [Google Scholar] [CrossRef]
- Britton, J.R.; Britton, H.L.; Gronwaldt, V. Breastfeeding, Sensitivity, and Attachment. Pediatrics 2006, 118, e1436–e1443. [Google Scholar] [CrossRef] [Green Version]
- Dias, C.C.; Figueiredo, B. Breastfeeding and depression: A systematic review of the literature. J. Affect. Disord. 2015, 171, 142–154. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, L.; Paglia, A.; Coolbear, J.; Niccols, A.; Parker, K.C.H.; Guger, S. Attachment security A meta-analysis of maternal mental health correlates. Clin. Psychol. Rev. 2000, 20, 1019–1040. [Google Scholar] [CrossRef]
- Barnes, J.; Theule, J. Maternal depression and infant attachment security: A meta-analysis. Infant Ment. Health J. 2019, 40, 817–834. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.; Gaffan, E.A. Effects of Early Maternal Depression on Patterns of Infant–Mother Attachment: A Meta-analytic Investigation. J. Child Psychol. Psychiatry 2000, 41, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Van Ijzendoorn, M.H.; Schuengel, C.; Bakermans–Kranenburg, M.J. Disorganized attachment in early childhood: Meta-analysis of precursors, concomitants, and sequelae. Dev. Psychopathol. 1999, 11, 225–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, R.A.; Vianello, M.; Hasselman, F.; Adams, B.G.; Adams, R.B.; Alper, S.; Aveyard, M.; Axt, J.; Babalola, M.T.; Bahník, Š.; et al. Many Labs 2: Investigating Variation in Replicability across Sample and Setting. Assoc. Psychol. Sci. 2018, 1, 443–490. [Google Scholar] [CrossRef]


{kind=link}
| Study (Year), Country Study Design. | Main Objectives/ Research Questions | Participant Details/ Sample Size N; M Mother’s Age (Standard Deviation, SD) | Attachment and Depression Measurement: Name of a Tool and the Time When Administered (in Trimester if Prenatally or Months if Postnatally) | Results | Study Quality Score |
|---|---|---|---|---|---|
| [47] (2016), Denmark longitudinal study | To examine the role of personality disorders in the association between maternal postpartum depression and infant–mother attachment in a low-risk sample. | Mothers with personality disorders (PD) and mothers from low-risk sample. N = 80; (M age = 30.5, SD = 4.12) | SSP: 13 months; PSE: 2 months; EPDS: 2 months | Postpartum depression was associated with attachment insecurity only if the mother also had a personality disorder diagnosis. Infants of depressed mothers without co-morbid personality disorders did not differ from infants of mothers with no psychopathology. These results suggest that co-existing personality disorders may be crucial in understanding how postpartum depression impacts on parenting and infant social-emotional development.. |  5 5Low attrition rate, validated methods, clear statistical analysis and direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. Inadequate sample size and no representative group of mothers from low-risk sample. |
| [44] (2013), USA longitudinal study | To examine associations between maternal antenatal depression and infant disorganization at 12 months. A secondary aim was to test the roles of maternal postpartum depression and maternal parenting quality as potential moderators of this association. | Only mothers with at least one major depressive episode before pregnancy. N = 79; (M age = 30.3; SD = 5.4) | SSP: 12 months; BDI-II: 1st and 2nd trimester; 6 and 12 months; SCID-I/P: 1st trimester | Attachment disorganization was strongly correlated with antenatal depression. Maternal parenting quality moderated this association, as exposure to higher levels of maternal depressive symptoms during pregnancy was only associated with higher rates of infant disorganized attachment when maternal parenting at three months was less optimal. No significant effects were found for postpartum depression. |  4 4Adequate sample size, validated methods, clear methodology and statistical analysis, direct measurement of depression-attachment influence. No information about attrition rate, double-blind procedure or coder experience, no representative high-risk study population. |
| [46] (2012), Netherlands longitudinal study | To examine the effects of maternal history of depressive disorder and the effects of depressive symptoms during pregnancy and early postpartum period on attachment insecurity. | A varied and representative sample with socio-economic diversity. N = 627; (M age = 32; SD = NA) | SSP: 14 months; BSI: 2nd trimester and 2 months; EPDS: 2months; CIDI: 3rd trimester | Insecure and disorganized attachment patterns were not related to maternal lifetime diagnosis of depression regardless of its severity. Higher maternal BSI depression score during pregnancy and BSI/EPDS score during postpartum period were not related to infant-mother attachment insecurity or disorganization at 14 months. |  9 9Adequate and representative sample size, low attrition rate, validated methods, clear statistical analysis and direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. |
| [40] (2011), USA prospective cross sectional | To examine associations between maternal depression and maternal expressed emotion (self-criticism, child-criticism), child internalizing and externalizing behaviors, and attachment insecurity. | Mothers with major depression with at least high-school education and good or very good socio-economic status. N = 198; (M age = 31.7; SD = 4.68) | SSP: 20 months; BDI: 20 months; DIS-III-R: 20 months | The depressed and nondepressed groups differed significantly regarding the main study variables, with depressed mothers evidencing higher child-criticism and self-criticism and having toddlers with higher levels of internalizing symptoms, externalizing symptoms, and attachment insecurity. Results revealed that children of mothers with higher self-criticism had a significantly higher probability of being classified as insecurely attached. However, child-criticism was not a significant mediator of the association between maternal depression and child attachment insecurity. |  8 8Adequate sample size, validated methods, clear statistical analysis and direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. No information about attrition rate, no representative low-risk study population. |
| [48] (2009), USA longitudinal study | To examine the impact of maternal depression on attachment security and on the representation of the parents by the child. | Mothers with major depression with at least high-school education and good or very good socio-economic status. N = 131; (M age = NA; SD = NA) | SSP: 20 and 36 months; BDI: 20, 36 and 48 months; DIS-III-R: 20 months | At 20 and 36 months, the distribution of attachment classifications differed significantly between the depressed and nondepressed groups. Lower rates of secure and higher rates of disorganized attachment were found for the depressed group. |  7 7Adequate and representative sample size, validated methods, clear statistical analysis and direct measurement of depression-attachment influence, used double-blind procedure by experienced coders. High attrition rate. |
| [49] (2006), Australia longitudinal study | To explore whether a mother’s own state of mind regarding attachment moderated the association between postpartum depression and insecure mother–child attachment. | A varied and representative sample with socio-economic diversity. N = 111; (M age = 31.4; SD = 4.2) | SSP: 15 months; CIDI: 4 and 12 months; CES-D: 4, 12 and 15 months | Mothers diagnosed as depressed were more likely to have an insecure state of mind regarding attachment. Infants of chronically depressed mothers were more likely to be insecurely attached. However, the relationship between maternal depression and child attachment was moderated by maternal attachment state of mind. When mothers were depressed and also had an insecure state of mind, their children were highly likely to be insecurely attached. |  9 9Adequate and representative sample size, low attrition rate, validated methods, clear statistical analysis and direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. |
| [50] (2005), South Africa longitudinal study | To evaluate how early disturbances in mother-infant interactions might be related to infant attachment problems. To examine the effect of wider contextual influences on infant attachment, including the mother’s experience of depression (both at 2 and at 18 months), the degree of support she received from her partner and others, and socio-economic status. | Mothers from a high-risk (low income) group. N = 147; (M age = 26.8; SD = NA) | SSP: 18 months; SCID: 2 and 18 months | Mothers with postpartum depression at two months were more likely to have children who were insecurely attached. Mothers who were less sensitive, more often intrusive, coercive (maternal intrusiveness), and displayed more maternal remoteness at two months postpartum were more likely to have insecurely attached children. Mothers who were less sensitive, highly intrusive-coercive at 18 months of a child’s life also were more likely to have insecurely attached children. Mothers of secure children were more likely to report that they felt supported by their partner than insecure ones. Unwanted pregnancy, unwanted baby, maternal depression at 18 months, remote-disengaged behavior at 18 months were not related to the style of infant attachment. |  7 7Adequate sample size, low attrition rate, validated methods, clear statistical analysis and direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. No representative group of mothers from a high-risk sample. |
| [51] (2003), Switzerland longitudinal study | To examine the effect of postpartum depression on the mother–child relationship. | Mothers with postpartum depression and control group. N = 70; (M age = 29; SD = NA) | SSP: 18 months; Diagnostic interview: last trimester; 3 and 19 months; EPDS: 3 and 18 months | Infants of non-depressed mothers were more likely to be securely attached to their mother. Mild or moderate depressive symptomatology, as detected at three months postpartum, had an impact 15 months later on the child’s development and on mother-child interaction, despite the fact that most mothers no longer presented depressive symptoms at 18 months. Boys were shown to be more resistant than girls. |  5 5Adequate sample size with high attrition rate. Validated methods, clear methodology and statistical analysis and direct measurement of depression-attachment influence. No information about coders experience or double-blind procedure. No clear information if study population is representative. |
| [25] (2001), USA longitudinal study | To examine relations between maternal depression (in pure and comorbid forms) and mother–infant interactions, infant attachment, and toddler social-emotional problems and competencies. | A varied and representative sample with socio-economic diversity. N = 69; (M age = 31.9; SD = 4.88) | SSP: 14 months; SCID-NP: 4 and 14 months; CES-D: prenatally and 4 and 14 and 30 months | A history of depression and other disorders increased risk for infant insecure attachment. Higher incidence of insecure attachment was observed in infants of the comorbid group as compared with infants of the pure depression group and no-psychopathology group, but no differences between the pure depression and no-psychopathology groups were found. |  5 5Representative but inadequate sample size with high attrition rate. Validated methods, clear methodology and statistical analysis, direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. |
| [52](1998), USA longitudinal study | To examine the direct influences of maternal depression on child development, as well as the role of contextual risks that may be particularly heightened in families with depressed parents. | Mothers with at least high-school education and good or very good socio-economic status in relationships with the child’s father. N = 156; (M age = 31.8; SD = 4.57) | AQS: NA; BDI: NA; DIS-III-R: NA | Toddlers with depressed mothers expressed significantly more insecure attachments than did toddlers with non-disordered mothers, and this difference was not accounted for by contextual risk. |  5 5Adequate sample size with low attrition rate, validated methods, clear methodology and statistical analysis, direct measurement of depression-attachment influence. No information about double-blind procedure or code experience, no representative low-risk study population. |
| [45] (1992), UK longitudinal study | To compare the cognitive, social and emotional development of infants of mothers with main depression and/or postpartum depression with that of infants of non-depressed mothers. To assess the impact of the style of interpersonal contact associated with depression (rather than depressive symptoms) on attachment style. | Mothers of healthy borne children with major depression episode and healthy control group. N = 111; (M age = 28; SD = 4.3) | SSP: 18 months; EPDS: 6 and 12 months; SPI: 3 month; SADS-L: 3 and 18 months | Infants whose mothers had been depressed in the postnatal period were significantly more likely to be insecurely attached to their mothers at 18 months than infants of non-depressed mothers. No difference in outcome was found between infants whose mothers had their first episode of depression following childbirth and those who had previous as well as postpartum depression. The duration, severity of the depression and current maternal depression was unrelated to infant outcome. Women who had previous but not postpartum depression were not significantly more likely to have infants who were insecure than women with no history of depression. |  3 3Representative, albeit inadequate, sample size with low attrition rate, validated methods, and direct measurement of depression-attachment influence. Clear methodology but vague statistical analysis and conclusion are not consistent. No information about coder experience or double-blind procedure. |
| Study (Year), Country Study Design | Main Objectives/ Research Questions | Participant Details/ Sample Size N; M Mother’s Age (Standard Deviation, SD) | Attachment and Depression Measurement: Name of a Tool and the Time When Administered (in Trimester if Prenatally or Months if Postnatally) | Results | Study Quality Score |
|---|---|---|---|---|---|
| [53] (2018), USA longitudinal study | To investigate the relationships between maternal depression risk and mind-mindedness on infant attachment behavior at one year. | A varied and representative sample with socio-economic diversity. N = 87; (M age = 29.4; SD = 6.5) | SSP: 12 months; CES-D: 6 weeks and 4 and 12 months | Maternal depression risk decreased over the infants’ first year, with the sharpest decline between 6 weeks and 4 months. Mothers at risk of depression when infants were 6 weeks showed less appropriate mind-mindedness at 4 months. The degree of disorganized attachment behavior by the infants at one year was positively associated with the risk of maternal depression at 6 weeks, and negatively associated with maternal appropriate mind-mindedness at 4 months. |  5 5Representative but not adequate sample size with high attrition rate, validated methods, clear methodology and statistical analysis, direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. |
| [42] (2018), Canada prospective cross-sectional | To examine the influence of maternal oxytocin receptor (OXTR, rs53576) genotype and cortisol secretion as moderators of the relation between maternal childhood maltreatment history and disorganized mother–infant attachment. | Mothers from low-risk sample, mainly high-educated sample. N = 314 (M age = 32.9; SD = 4.5) | SSP: 17 months; BDI: 16 months | Marital status, employment, age, breast feeding status, self-reported ethnicity, depression, parenting stress and sensitivity, family income, number of siblings and hours per week in out of home care was not associated with attachment disorganization scores. Only infant sex was related to disorganization, insofar that males had higher disorganization scores than females. Maltreatment history more strongly predicted mother-infant attachment disorganization score and disorganized classification for mothers with more plasticity alleles of OXTR (G) and for mothers with higher SSP cortisol secretion, relative to mothers with fewer plasticity alleles and lower SSP cortisol secretion. |  4 4Adequate sample size with no information about attrition rate. Validated methods, used a double-blind procedure, clear methodology and statistical analysis. No representative low-risk sample and no direct measurement of depression-attachment influence. |
| [54] (2018), USA longitudinal study | To examine the association between multiple forms of early adversity—socioeconomic status disadvantage, familial stress, maternal depression, and security of attachment—and individual differences in a composite measure of pro-inflammatory cytokines and the acute phase protein CRP (C Reactive Protein). | Mothers from psychosocial and/or socio-demographic high-risk groups. N = 49; (M age = 24; SD = 4.7) | SSP: 17 months; CES-D: 5 and 17 months | Higher levels of depressive symptoms and insecure attachment are significantly associated with higher inflammatory load score (ILS). No significant association between maternal depressive symptoms and elevated infant ILS was observed for securely attached infants, whereas insecurely attached infants showed high levels of ILS at high levels of maternal depressive symptoms. Securely attached infants had the least amount of salivary inflammation, regardless of mothers’ levels of depression. Regions of significance analysis indicated that starting at sub-clinical levels of maternal depressive symptoms, infants classified as insecure had significantly higher ILS than all other infants. |  2 2No adequate sample size form high-risk group of mothers with no information about attrition rate. Validated methods, double-blind procedure by experienced coders, clear methodology and statistical analysis but with indirect measurement of depression-attachment influence. |
| [55] (2016), USA longitudinal study | To determine whether the sex of an infant influences early vulnerability to maternal psychosocial risk, as indexed by trajectories of maternal depressive symptoms across the first 18 months’ postpartum, and toddlers’ attachment security at 18 months of age. | African American mothers from heterogeneous socio-economic backgrounds. N = 182; (M age = 29.5; SD = 4.37) | SSP: 18 months; CES-D: 2 and 3 and 6 and 12 and 18 months | Toddlers’ attachment security was significantly and negatively correlated with maternal depressive symptoms at 2, 3 and 6 months, marginally associated with symptoms at 12 months, but not associated with maternal depressive symptoms at 18 months. Boys’ attachment security was significantly and negatively associated with maternal depressive symptoms during the first postpartum year (at 2, 3, 6, and 12 months). Girls’ attachment security was not significantly associated with maternal depressive symptoms at any time of measurement. |  8 8Adequate sample size, low attrition rate, validated methods, clear statistical analysis and direct measurement of depression-attachment influence; double-blind procedure used by experienced coders. Representative African American population. |
| [56] (2014), Italy longitudinal study | To examine the predictors of mother–child interaction quality and child attachment security in a sample of first-time mothers with psychosocial and/or socio-demographic risk factors. | Mothers from psychosocial and/or socio-demographic high-risk groups. N = 40; (M age = 27.3; SD = 6.56) | AQS: 18 months; SCL-90-R: 3 months; EPDS: 3 and 6 months | Attachment security was not significantly associated with young maternal age, single parenting, psychopathological symptoms or low family socio-economic status. When groups were divided according to risk factors (socio-demographic only, psychosocial only, both factors) only socio-demographic factors were significantly associated with attachment security. Postpartum depression showed no association with either mother–child emotional availability or child attachment security. |  1 1No representative and no adequate sample size, with no direct measurement of depression-attachment influence. Unclear methodology and statistical analysis. Validated methods, SSP procedure performed by experienced coders but no information about double-blind procedure. Low attrition rate. |
| [39] (2014), USA prospective cross-sectional study | To examine the extent to which maternal borderline personality pathology and related emotional dysfunction (including emotion regulation difficulties and emotional intensity/reactivity) are connected with infant emotional regulation difficulties. To examine the moderating role of mother–infant attachment in the relations between maternal borderline personality pathology and related emotional dysfunction and infant emotional regulation. | Mothers with borderline personality disorder. N = 101; (M age = 28.7; SD = 5.6) | SSP: between 12 and 23 months; DASS: 12 months | High scores in the depression subscale of DASS correlated positively with a high symptomatology of the borderline personality (BP). No link was found between depressive symptoms and attachment classification. Results suggest that it may be the emotional dysfunction associated with BP, rather than the presence of clinically relevant BP pathology per se, that places infants of mothers with BP pathology at risk of negative outcomes. |  3 3No adequate sample size for high-risk group of mothers with low attrition rate. Validated methods, double-blind procedure used by experienced coders, clear methodology and statistical analysis but indirect measurement of depression-attachment influence. |
| [57] (2011), Germany longitudinal study | To examine the effect of the time of first meeting between mother and very low birth weight (VLBW) newborn on the establishment of a secure attachment behavior; to indicate the role of maternal depression, social support and pregnancy history. | Mothers of very low birth weight (VLBW) newborns. N = 52; (M age = 31.2; SD = 5.1) | SSP: 12-18 months c.a. (corrected age); ADS-L: 0 and 3 and 12 months c.a. | Not seeing child within 30 min to 3 h after birth and first born child were identified as the best predictors for insecure attachment behavior. Maternal factors including age of the mother, degree of depression at three time points, social support, social status of mother and father, and pregnancy history did not significantly differ between children with secure and insecure attachment. |  5 5No representative or adequate sample size with good attrition rate. Validated methods, used double-blind procedure, clear methodology and statistical analysis, direct measurement of depression-attachment influence. No information about SSP coder experience. |
| [58] (2010), UK longitudinal study | To determine whether prenatal cortisol exposure predicts infant cognitive development and to evaluate how infant–parent relationship moderates this effect. | A varied and representative sample with socio-economic diversity. N = 125; (M age =36.6; SD=4.1) | SSP: 17 months; EPDS: 17 months | Cortisol level during pregnancy and postnatal depression were not associated with infant attachment style. Securely attached children had mothers who reported lower levels of postnatal state anxiety. |  5 5Adequate and representative sample size, validated methods, clear statistical analysis, double-blind procedure used by experienced coders. High attrition rate and indirect measurement of depression-attachment influence. |
| [59] (2009), USA longitudinal study | To examine the associations between household food security (access to sufficient, safe, and nutritious food) during infancy and attachment and mental proficiency in toddlerhood. | A varied and representative sample with socio-economic diversity. N = 7894; (M age =27.3; SD=13.1) | TAS-45: 24 months; CES-D: 9 months | Food insecurity has no significant direct association with being insecurely attached. Instead, food insecurity works indirectly through depression and parenting practices to influence insecure attachment. Attachment insecurity is positively associated with depression. |  7 7Adequate and representative sample size, low attrition rate, validated methods, clear statistical analysis and direct measurement of depression-attachment influence. No information about double-blind procedure and coders experience. |
| [60] (2005), Canada longitudinal study | To replicate the finding that a significant association exists between maternal state of mind, maternal sensitivity, and infant attachment security, but also that maternal sensitivity only partially mediates the association between maternal state of mind and infant attachment. The second objective was to consider whether paths to infant attachment security may exist that do not originate with maternal state of mind. | Adolescent mothers up to 19 years old. N = 64; (M age = 17.4; SD = 1.5) | AQS: 15 and 18 months; CES-D: 6 months | Significant (but weak) associations were documented between maternal attachment state of mind and maternal sensitivity, as well as between maternal sensitivity and infant security. Association between maternal sensitivity and attachment security remained significant even when other variables were statistically controlled. A marginal link was observed between maternal depression and infant attachment security. Furthermore, there was no association between depression and maternal sensitivity. |  5 5Adequate sample size with no information about attrition rate. Validated methods used by experienced coders, clear methodology and statistical analysis and direct measurement of depression-attachment influence. No information about double-blind procedure and no representative group of adolescent mothers. |
| [61] (2002), Israel longitudinal study | To predict attachment classifications from: (a) relevant control variables (socio-economic status, marital relation, knowledge of infant development), (b) a maternal variable (sensitivity or depression) or child variable (gender or temperament), (c) a childcare variable (type of care at 12 months, amount of nonmaternal care, age of entry into nonmaternal care, stability of care, different types of care, and infant–adult ratio), and (d) the interaction between the two selected (mother/child and child-care) variables. | Jewish mothers of healthy children with socio-economic diversity. N = 758; (M age = 29.2; SD = 4.78) | SSP: 12 months; DACL: 6 and 12 months; BDI: 6 months | Center-care adversely increased the likelihood of infants developing insecure attachment to their mothers as compared to infants who were either in maternal care, individual non-parental care with a relative, individual nonparental care with a paid caregiver, or family day-care. Mothers found to be more sensitive were more likely to have securely attached infants regardless of care type (maternal, family, nanny etc.). Maternal depression, child’s gender, temperament, age (in weeks) when nonmaternal care was introduced, length of extra care (3–12 months), stability of care were not found to be significant predictors of attachment security/insecurity. |  9 9Adequate and representative sample size, low attrition rate, validated methods, clear statistical analysis and direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. |
| [62] (2001), Sweden longitudinal study | To explore the long-term impact of depressive symptomatology on mother–child interaction and on infant attachment to mothers. | No adequate information about studied sample. N = 45; (M age = NA, SD = NA) | PCERA: 15 and 18 months; EPDS: 2 months | Children of mothers with high EPDS scores were less curious and focused on free play situations than children of low EPDS scorers. Even if the proportion of insecurely attached children did not differ between high and low EPDS groups, those children who had mothers in the high-scoring group were more likely to show restricted levels of joy in their secure attachment behaviours. |  4 4No adequate sample size with high attrition rate. Validated methods, clear methodology and statistical analysis, direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. No clear information whether study population is representative. |
| [63] (2001), UK longitudinal study | To determine whether experience of loss may lead to unresolved state of mind in a mother, and whether this is associated with increasing rates of disorganization of infant attachment patterns among infants born subsequent to stillbirth. To determine whether disorganized infant attachment could be predicted by maternal symptoms of depression or anxiety, by social disadvantage, by additional experience of miscarriage or termination of pregnancy, or by whether or not the mother had seen and held her stillborn infant and had held a funeral for the infant. | Mothers who have experienced a stillbirth (after 18 month of gestation) before their current pregnancy and a control group. N = 106; (M age = 19.9; SD = 5.4) | SSP: 12 months; EPDS: 3rd trimester and 6 weeks; BDI: 26 weeks and 12 months | Infants next-born after a stillbirth were significantly more likely to have disorganized attachment style than control infants. Maternal depression was not associated with child attachment style. |  7 7Adequate and representative sample size, validated methods, clear statistical analysis and direct measurement of depression-attachment influence, double-blind procedure used by experienced coders. High attrition rate. |
| [64] (2000), USA longitudinal study | To explore the effects of marital separation and divorce on psychological development of children in the first 3 years of life. To examine the consequences of marital separation on children’s functioning immediately after separation and to assess whether maternal background before and after marital separation may affect studied variables. | A varied and representative sample with socio-economic diversity. N = 340; (M age = 26.3; SD = NA) | SSP: 15 and 36 months; AQS: 24 months; CES-D: 1 and 6 and 15 and 24 and 36 months | Children in 2-parent families performed better than children in 1-parent families on assessments of cognitive and social abilities, problem behavior, attachment security, and behavior with mother. However, controlling for maternal education and family income reduced these differences, and associations with separated-intact marital status were non-significant. Hence, child psychological development was not affected by parental separation per se; it was related to maternal income, education, ethnicity, child- rearing beliefs, depressive symptoms, and behavior. Maternal depression increased behavioral problems of the child, but did not affect the security of attachment style. |  8 8Adequate and representative sample size, low attrition rate, validated methods, clear statistical analysis and direct measurement of depression-attachment influence, SSP procedure performed by experienced coders. No information about double-blind procedure. |
| [35] (1990), USA Intervention longitudinal study | To assess whether a family in high-risk circumstances (combined effects of poverty, maternal depression, and caretaking inadequacy) could benefit from family support services. | Mothers from a high-risk (low income) group and controls. N = 76; (M age = 24.06, SD = NA) | SSP: 12 months; CES-D: 12 and 18 months | The negative effects of social risk status were more pervasive in regard to infant attachment security than in regard to mental development, with the unsupported high-risk group as a whole differing significantly both from the supported high-risk group. Unsupported high-risk infants had a very high rate of insecure-disorganized attachment, 60%, compared to 29% for high-risk infants supported by family services and 28% for community infants. |  5 5Representative but not adequate sample size with no information about attrition rate. Validated methods, double-blind procedure used by experienced coders, clear methodology and statistical analysis, no direct measurement of depression-attachment influence. |
| [65] (1989), USA longitudinal study | To examine the predictors of mother–child interaction quality and child attachment security in a sample of first-time mothers with psychosocial and/or socio-demographic risk factors. | Married mothers. N = 40; (M age = 27.3; SD = 6.56) | SSP: 16 and 40 months; BDI: 5 and 16 months | Insecure infant attachment at 16 months was associated with maternal perception of overcontrol, depressed mood state, and aversive conditioning to impending cries in a laboratory task at the 5-month period. Mothers of insecurely-attached infants were more depressed at 5 (but not 16) months than mothers of securely attached infants. |  6 6No adequate sample size with low attrition rate. Validated methods, clear methodology and statistical analysis, direct measurement of depression-attachment influence, double-blind procedure by experienced coders used. No clear information whether study population was representative. |
| [43] (1986), USA prospective cross sectional | To examine whether maternal depression is a risk factor for infant development, as well as for childhood psychopathology, and whether maternal depression affect the security of attachment at twelve months of age in a low-income sample. | Mothers from high-risk (low income) group. N = 56; (M age = NA; SD = NA) | SSP: 12 months; CES-D: 0–9 month and 18 months | Depressed and non-depressed mothers did not differ in incidence of insecure infant attachment, nor did the maternal depression scores correlate with infant reunion behaviors in the strange situation, including infant avoidance or resistance at reunion. Mothers reporting mild to moderate depression were more likely to have securely attached infants, while mothers reporting severe depression were more likely to have infants showing unstable avoidant attachment. More surprisingly, mothers reporting the least frequent depressive symptoms were more likely to have avoidant infants. |  5 5Adequate sample size with no information about attrition rate. Validated methods, used double-blind procedure, clear methodology and statistical analysis, direct measurement of depression-attachment influence. No clear information if SSP coders have some experience. No representative high-risk population. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Śliwerski, A.; Kossakowska, K.; Jarecka, K.; Świtalska, J.; Bielawska-Batorowicz, E. The Effect of Maternal Depression on Infant Attachment: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2675. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082675
Śliwerski A, Kossakowska K, Jarecka K, Świtalska J, Bielawska-Batorowicz E. The Effect of Maternal Depression on Infant Attachment: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(8):2675. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082675
Chicago/Turabian StyleŚliwerski, Andrzej, Karolina Kossakowska, Karolina Jarecka, Julita Świtalska, and Eleonora Bielawska-Batorowicz. 2020. "The Effect of Maternal Depression on Infant Attachment: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 8: 2675. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082675