Risk Factors for Upper Limb Injury in Tennis Players: A Systematic Review

 ,
,  and
and 
Abstract
:1. Introduction
2. Experimental Section
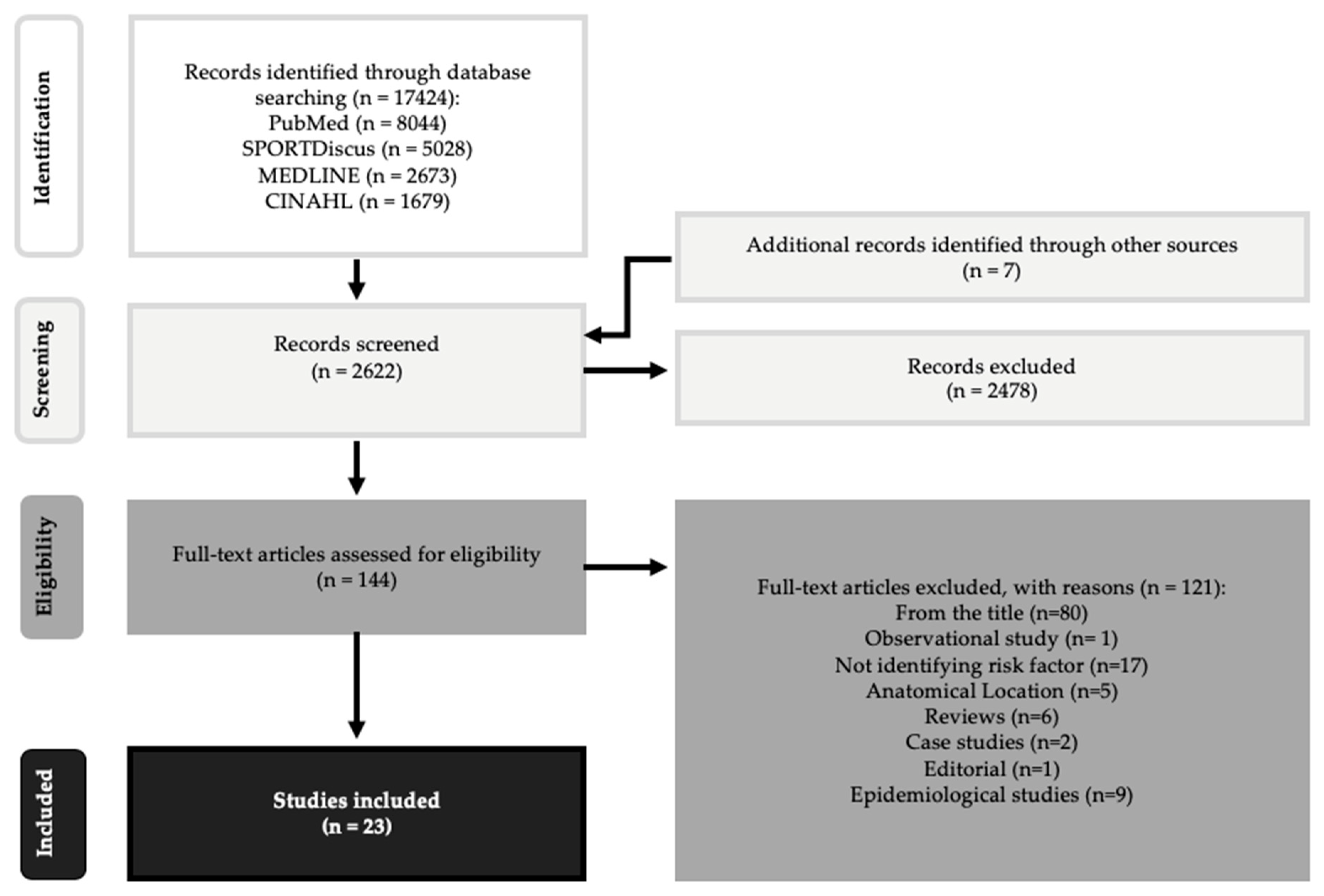
2.1. Study Selection
2.2. Data Extraction
3. Results
Key Findings—Risk Factors
4. Discussion
4.1. Prolonged Tennis (Exposure to Tennis)
4.2. Dyskinesia
4.3. Shoulder Rotational Properties
4.4. Technique and Skill Level
4.5. Racquet Properties
4.6. Previous Injury
4.7. Age
4.8. Surface
5. Limitations, Strength, and Practical Applications
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pluim, B.M.; Staal, J.B.; Windler, G.E.; Jayanthi, N. Tennis injuries: Occurrence, aetiology, and prevention. Br. J. Sports Med. 2006, 40, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; Safran, M. Tennis injuries. Med. Sport Sci. 2005, 48, 120–137. [Google Scholar] [PubMed] [Green Version]
- Kibler, B. Evaluation of sports demands as a diagnostic tool in shoulder disorders. In The Shoulder: A Balance of Mobility and Stability; Fa, M., Fu, F.H., Hawkins, R.T., Eds.; AAOS: Rosemont, IL, USA, 1993; pp. 379–399. [Google Scholar]
- McCurdie, I.; Smith, S.; Bell, P.H.; Batt, M.E. Tennis injury data from The Championships, Wimbledon, from 2003 to 2012. Br. J. Sports Med. 2017, 51, 607–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, R.T.; Gracitelli, G.C.; Saccol, M.F.; Frota De Souza Laurino, C.; Silva, A.C.; Braga-Silva, J.L. Shoulder strength profile in elite junior tennis players: Horizontal adduction and abduction isokinetic evaluation. Br. J. Sports Med. 2006, 40, 513–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrams, G.D.; Renstrom, P.A.; Safran, M.R. Epidemiology of musculoskeletal injury in the tennis player. Br. J. Sports Med. 2012, 46, 492–498. [Google Scholar] [CrossRef]
- Kibler, W.B.; Sciascia, A.; Thomas, S.J. Glenohumeral internal rotation deficit: Pathogenesis and response to acute throwing. Sports Med. Arthrosc. Rev. 2012, 20, 34–38. [Google Scholar] [CrossRef]
- Kibler, W.B.; Ludewig, P.M.; McClure, P.W.; Michener, L.A.; Bak, K.; Sciascia, A.D. Clinical implications of scapular dyskinesis in shoulder injury: The 2013 consensus statement from the ‘scapular summit’. Br. J. Sports Med. 2013, 47, 877–885. [Google Scholar] [CrossRef] [Green Version]
- Sell, K.; Hainline, B.; Yorio, M.; Kovacs, M. Injury trend analysis from the us open tennis championships between 1994 and 2009. Br. J. Sports Med. 2014, 48, 546–551. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, M.; Ellenbecker, T.; Kibler, W.; Al, E. Demographic data and injury trends in American national junior tennis players. J. Strength Cond. Res. 2012, 26, S52. [Google Scholar]
- Safran, R. Biomechanics of tennis strokes and its association with tennis injuries. Am. J. Med Sci. 2003, 5, 276–284. [Google Scholar]
- Lynall, R.C.; Kerr, Z.Y.; Djoko, A.; Pluim, B.M.; Hainline, B.; Dompier, T.P. Epidemiology of National Collegiate Athletic Association men’s and women’s tennis injuries, 2009/2010–2014/2015. Br. J. Sports Med. 2016, 50, 1211–1216. [Google Scholar] [CrossRef] [PubMed]
- Hjelm, N.; Werner, S.; Renstrom, P. Injury profile in junior tennis players: A prospective two year study. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Jayanthi, N.A.; O’Boyle, J.; Durazo-Arvizu, R.A. Risk factors for medical withdrawals in United States Tennis Association junior national tennis tournaments: A descriptive epidemiologic study. Sports Health 2009, 1, 231–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, M.S. Applied physiology of tennis performance. Br. J. Sports Med. 2006, 40, 381–385. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Oxford Centre for Evidence-Based Medicine. Available online: http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/ (accessed on 1 March 2020).
- Kenny, S.J.; Whittaker, J.L.; Emery, C.A. Risk factors for musculoskeletal injury in preprofessional dancers: A systematic review. Br. J. Sports Med. 2016, 50, 997–1003. [Google Scholar] [CrossRef]
- Martin, C.; Kulpa, R.; Ezanno, F.; Delamarche, P.; Bideau, B. Influence of playing a prolonged tennis match on shoulder internal range of motion. Am. J. Sports Med. 2016, 44, 2147–2151. [Google Scholar] [CrossRef]
- Martin, C.; Kulpa, R.; Ropars, M.; Delamarche, P.; Bideau, B. Identification of temporal pathomechanical factors during the tennis serve. Med. Sci. Sports Exerc. 2013, 45, 2113–2119. [Google Scholar] [CrossRef] [Green Version]
- Cools, A.M.; Johansson, F.R.; Cambier, D.C.; Velde, A.V.; Palmans, T.; Witvrouw, E.E. Descriptive profile of scapulothoracic position, strength and flexibility variables in adolescent elite tennis players. Br. J. Sports Med. 2010, 44, 678–684. [Google Scholar] [CrossRef] [Green Version]
- Kibler, W.B.; Chandler, T.J. Range of motion in junior tennis players participating in an injury risk modification program. J. Sci. Med. Sport 2003, 6, 51–62. [Google Scholar] [CrossRef]
- Hennig, E.M. Influence of racket properties on injuries and performance in tennis. Exerc. Sport Sci. Rev. 2007, 35, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Tagliafico, A.S.; Ameri, P.; Michaud, J.; Derchi, L.E.; Sormani, M.P.; Martinoli, C. Wrist injuries in nonprofessional tennis players: Relationships with different grips. Am. J. Sports Med. 2009, 37, 760–767. [Google Scholar] [CrossRef] [PubMed]
- Rogowski, I.; Creveaux, T.; Chèze, L.; Macé, P.; Dumas, R. Effects of the racket polar moment of inertia on dominant upper limb joint moments during tennis serve. PLoS ONE 2014, 9, e104785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cools, A.M.; Palmans, T.; Johansson, F.R. Age-related, sport-specific adaptions of the shoulder girdle in elite adolescent tennis players. J. Athl. Train. 2014, 49, 647–653. [Google Scholar] [CrossRef] [Green Version]
- Moore-Reed, S.D.; Kibler, W.B.; Myers, N.L.; Smith, B.J. Acute changes in passive glenohumeral rotation following tennis play exposure in elite female players. Int. J. Sports Phys. Ther. 2016, 11, 230–236. [Google Scholar]
- Martin, C.; Bideau, B.; Delamarche, P.; Kulpa, R. Influence of a Prolonged Tennis Match Play on Serve Biomechanics. PLoS ONE 2016, 11, e0159979. [Google Scholar] [CrossRef] [Green Version]
- Rich, R.L.; Struminger, A.H.; Tucker, W.S.; Munkasy, B.A.; Joyner, A.B.; Buckley, T.A. Scapular upward-rotation deficits after acute fatigue in tennis players. J. Athl. Train. 2016, 51, 474–479. [Google Scholar] [CrossRef] [Green Version]
- Maquirriain, J.; Ghisi, J.P.; Amato, S. Is tennis a predisposing factor for degenerative shoulder disease? A controlled study in former elite players. Br. J. Sports Med. 2006, 40, 447–450. [Google Scholar] [CrossRef] [Green Version]
- Hatch Iii, G.F.; Pink, M.M.; Mohr, K.J.; Sethi, P.M.; Jobe, F.W. The effect of tennis racket grip size on forearm muscle firing patterns. Am. J. Sports Med. 2006, 34, 1977–1983. [Google Scholar] [CrossRef]
- Lädermann, A.; Chagué, S.; Kolo, F.C.; Charbonnier, C. Kinematics of the shoulder joint in tennis players. J. Sci. Med. Sport 2016, 19, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.; Bideau, B.; Ropars, M.; Delamarche, P.; Kulpa, R. Upper limb joint kinetic analysis during tennis serve: Assessment of competitive level on efficiency and injury risks. Scand. J. Med. Sci. Sports 2014, 24, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Rogowski, I.; Creveaux, T.; Chèze, L.; Dumas, R. Scapulothoracic kinematics during tennis forehand drive. Sports Biomech. 2014, 13, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Saccol, M.F.; Gracitelli, G.C.; da Silva, R.T.; Laurino, C.F.D.S.; Fleury, A.M.; Andrade, M.D.S.; da Silva, A.C. Shoulder functional ratio in elite junior tennis players. Phys. Ther. Sport 2010, 11, 8–11. [Google Scholar] [CrossRef]
- Silva, R.T.; Hartmann, L.G.; De Souza Laurino, C.F.; Biló, J.P.R. Clinical and ultrasonographic correlation between scapular dyskinesia and subacromial space measurement among junior elite tennis players. Br. J. Sports Med. 2010, 44, 407–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warner, J.J.; Micheli, L.J.; Arslanian, L.E.; Kennedy, J.; Kennedy, R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome. A study using Moire topographic analysis. Clin. Orthop. Relat. Res. 1992, 285, 191–199. [Google Scholar]
- Kibler, W.B.; McMullen, J. Scapular dyskinesis and its relation to shoulder pain. J. Am. Acad. Orthop. Surg. 2003, 11, 142–151. [Google Scholar] [CrossRef] [Green Version]
- Burn, M.B.; McCulloch, P.C.; Lintner, D.M.; Liberman, S.R.; Harris, J.D. Prevalence of scapular dyskinesis in overhead and nonoverhead athletes: A systematic review. Orthop. J. Sports Med. 2016, 4, 2325967115627608. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Pérez, V.; Moreside, J.; Barbado, D.; Vera-Garcia, F.J. Comparison of shoulder rotation range of motion in professional tennis players with and without history of shoulder pain. Man. Ther. 2015, 20, 313–318. [Google Scholar] [CrossRef]
- De Smedt, T.; De Jong, A.; Van Leemput, W.; Lieven, D.; Van Glabbeek, F. Lateral epicondylitis in tennis: Update on aetiology, biomechanics and treatment. Br. J. Sports Med. 2007, 41, 816–819. [Google Scholar] [CrossRef]
- Hennig, E.M.; Rosenbaum, D.; Milani, T.L. Transfer of tennis racket vibrations onto the human forearm. Med. Sci. Sports Exerc. 1992, 24, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Rettig, A.C. Wrist problems in the tennis player. Med. Sci. Sports Exerc. 1994, 26, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Krosshaug, T. Understanding injury mechanisms: A key component of preventing injuries in sport. Br. J. Sports Med. 2005, 39, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; Chandler, T.J.; Livingston, B.P.; Roetert, E.P. Shoulder range of motion in elite tennis players: Effect of age and years of tournament play. Am. J. Sports Med. 1996, 24, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Vad, V.B.; Gebeh, A.; Dines, D.; Altchek, D.; Norris, B. Hip and shoulder internal rotation range of motion deficits in professional tennis players. J. Sci. Med. Sport 2003, 6, 71–75. [Google Scholar] [CrossRef]
- Girard, O.; Eicher, F.; Fourchet, F.; Micallef, J.P.; Millet, G.P. Effects of the playing surface on plantar pressures and potential injuries in tennis. Br. J. Sports Med. 2007, 41, 733–738. [Google Scholar] [CrossRef] [Green Version]
- Maquirriain, J. The interaction between the tennis court and the player: How does surface affect leg stiffness? Sports Biomech. 2013, 12, 48–53. [Google Scholar] [CrossRef]
- Okholm Kryger, K.; Dor, F.; Guillaume, M.; Haida, A.; Noirez, P.; Montalvan, B.; Toussaint, J.F. Medical reasons behind player departures from male and female professional tennis competitions. Am. J. Sports Med. 2015, 43, 34–40. [Google Scholar] [CrossRef]


{kind=link}
| Pubmed | Sportdiskus | Medline | Cinahl | ||
|---|---|---|---|---|---|
| Age AND tennis | Exclusion criteria search | 758 | 1498 | 752 | 447 |
| Inclusion criteria search | 477 | 448 | 98 | 74 | |
| Tennis Injuries | Exclusion criteria search | 2242 | 598 | 118 | 92 |
| Inclusion criteria search | 1087 | 143 | 6 | 9 | |
| Muscle AND tennis | Exclusion criteria search | 839 | 889 | 683 | 330 |
| Inclusion criteria search | 504 | 233 | 64 | 49 | |
| Elbow injuries AND tennis | Exclusion criteria search | 1613 | 141 | 70 | 113 |
| Inclusion criteria search | 787 | 28 | 1 | 9 | |
| Shoulder Kinetics OR kinematics AND tennis | Exclusion criteria search | 348 | 329 | 145 | 132 |
| Inclusion criteria search | 237 | 65 | 23 | 30 | |
| Kinematics AND tennis | Exclusion criteria search | 344 | 257 | 95 | 78 |
| Inclusion criteria search | 233 | 90 | 38 | 34 | |
| Kinetics AND tennis | Exclusion criteria search | 157 | 369 | 156 | 41 |
| Inclusion criteria search | 124 | 63 | 8 | 13 | |
| Injury risk AND Tennis | Exclusion criteria search | 283 | 103 | 77 | 49 |
| Inclusion criteria search | 190 | 21 | 7 | 9 | |
| Shoulder Injury AND tennis | Exclusion criteria search | 258 | 134 | 41 | 67 |
| Inclusion criteria search | 153 | 17 | 2 | 5 | |
| Overuse Injury AND tennis | Exclusion criteria search | 233 | 139 | 61 | 42 |
| Inclusion criteria search | 114 | 22 | 2 | 7 | |
| Risk factors AND tennis | Exclusion criteria search | 221 | 69 | 117 | 67 |
| Inclusion criteria search | 151 | 11 | 8 | 9 | |
| Shoulder Rotation AND tennis | Exclusion criteria search | 118 | 102 | 65 | 42 |
| Inclusion criteria search | 83 | 14 | 8 | 8 | |
| Wrist Injuries AND tennis | Exclusion criteria search | 91 | 55 | 39 | 27 |
| Inclusion criteria search | 41 | 7 | 0 | 3 | |
| Glenohumeral AND tennis | Exclusion criteria search | 45 | 68 | 45 | 31 |
| Inclusion criteria search | 30 | 8 | 1 | 2 | |
| Asymmetry AND tennis | Exclusion criteria search | 60 | 60 | 43 | 15 |
| Inclusion criteria search | 45 | 19 | 7 | 7 | |
| Scapular AND tennis | Exclusion criteria search | 49 | 36 | 49 | 28 |
| Inclusion criteria search | 33 | 6 | 5 | 7 | |
| Scapula AND tennis | Exclusion criteria search | 48 | 28 | 44 | 31 |
| Inclusion criteria search | 30 | 5 | 3 | 5 | |
| Shoulder Kinematics AND tennis | Exclusion criteria search | 107 | 12 | 6 | 5 |
| Inclusion criteria search | 76 | 4 | 0 | 2 | |
| Overhead Injuries AND tennis | Exclusion criteria search | 68 | 20 | 13 | 16 |
| Inclusion criteria search | 49 | 7 | 3 | 5 | |
| Training loads AND tennis | Exclusion criteria search | 26 | 74 | 8 | 4 |
| Inclusion criteria search | 23 | 22 | 5 | 0 | |
| Kinetic Chain AND tennis | Exclusion criteria search | 30 | 26 | 20 | 11 |
| Inclusion criteria search | 27 | 8 | 5 | 3 | |
| Dyskinesis AND Tennis | Exclusion criteria search | 48 | 7 | 11 | 4 |
| Inclusion criteria search | 40 | 3 | 3 | 1 | |
| Dyskinesia AND Tennis | Exclusion criteria search | 40 | 1 | 8 | 1 |
| Inclusion criteria search | 34 | 0 | 0 | 0 | |
| Shoulder Kinetics AND Tennis | Exclusion criteria search | 18 | 13 | 7 | 6 |
| Inclusion criteria search | 15 | 2 | 0 | 1 |
| Study | Type of Study | Participants | Sample Size | Risk Factor Examined |
|---|---|---|---|---|
| [22] | Cross-sectional study | Competitive junior tennis players | N = 35, (M = 19, F = 16) | Scapulothoracic position, muscle strength, flexibility |
| [27] | Cross-sectional study | Competitive adult tennis players | N = 59, (M = 31, F = 28) | Age-related shoulder/scapular adaptions |
| [32] | Controlled laboratory study | Collegiate tennis players | N = 16’ (Μ) | Racket grip size |
| [24] | Cross-sectional study | Competitive adult tennis players | N = 55, (Μ) | Racket properties |
| [13] | Prospective 2-year study | Competitive junior tennis players | N = 55, (M = 35, F = 20) | Previous injury |
| [23] | Laboratory-based study | Competitive junior tennis players | N = 51, (M = 29, F = 22) | Flexibility and range of motion |
| [33] | Laboratory study | Ex-professional senior tennis players | N = 10, (M = 9, F = 1) | Glenohumeral instability and shoulder impingement |
| [21] | Cross-sectional study | Professional and competitive tennis players | N = 18, (M = 18) | Skills and technique |
| [34] | Laboratory-based study | Competitive adult tennis players | N = 20, (M = 20) | Skill, technique kinetic chain, and previous injury |
| [29] | Laboratory-based study | Competitive adult tennis players | N= 8, (M = 8) | Effect of prolonged tennis to shoulder muscle fatigue |
| [20] | Laboratory-based study | Competitive adult tennis players | N= 8, (M = 8) | Effect of prolonged tennis to shoulder range of motion |
| [31] | Cross-sectional controlled study | Competitive senior tennis players | N = 18, (M = 17, F = 1) | Prolonged tennis may affect shoulder articular cartilage |
| [28] | Cohort study | Professional tennis players | N = 79, (F = 79) | Effect of prolonged tennis on glenohumeral rotation |
| [30] | Randomized controlled clinical trial | Collegiate tennis players | N = 20, (M = 20) | Influence of fatigue on scapular kinematics |
| [35] | Laboratory-based study | Competitive adult tennis players | N = 8, (M = 8) | Scapulothoracic kinematics |
| [26] | Laboratory-based study | Competitive adult tennis players | N = 8, (M = 8) | Racket polar moment of inertia |
| [36] | Cross-sectional study | Competitive junior tennis players | N = 40, (M = 26, F = 14) | Shoulder rotational muscle imbalances |
| [37] | Cross-sectional study | Competitive junior tennis players | N = 53, (M = 31, F = 22) | Correlation between scapular dyskinesia and subacromial space |
| [25] | Cross-sectional study | Competitive adult tennis players | N = 400, (M = 323, F = 77) | Racket grip |
| Studies | Clear Description of the Hypothesis, Objectives | Outcomes Clearly Described in the Introduction or Methods Section | Clear Description of the Patient’s Characteristics | Clear Description of Intervention of Interest | Clear Description of the Distribution of Principal Confounders | Clear Description of Study Findings | Estimates of the Random Variability in the Data for the Outcomes | Measurement of Adverse Events | Description of Patient’s Characteristics that were Lost to Follow-Up | Report of Probability Values | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [22] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [27] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [32] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 6/10 |
| [24] | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1/10 |
| [13] | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 6/10 |
| [23] | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 4/10 |
| [33] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 6/10 |
| [21] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [34] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [29] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [20] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 6/10 |
| [31] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [28] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [30] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [35] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [26] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [36] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [37] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| [25] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 7/10 |
| Studies | Were the Subjects Asked to Participate in the Study Representative of the Entire Population from which they were Recruited? | Were Those Subjects who were Prepared to Participate Representative of the Entire Population from which they were Recruited? | Were the Stuff, Places, and Facilities where the Patients were Treated Representative of the Treatment the Majority of Patients Received? | Score |
|---|---|---|---|---|
| [22] | 0 | 1 | 1 | 2/3 |
| [27] | 0 | 1 | 1 | 2/3 |
| [32] | 0 | 1 | 1 | 2/3 |
| [24] | 0 | 1 | 1 | 2/3 |
| [13] | 0 | 1 | 1 | 2/3 |
| [23] | 0 | 1 | 1 | 2/3 |
| [33] | 1 | 1 | 1 | 3/3 |
| [21] | 1 | 1 | 1 | 3/3 |
| [34] | 1 | 1 | 1 | 3/3 |
| [29] | 1 | 1 | 1 | 3/3 |
| [20] | 0 | 1 | 1 | 2/3 |
| [31] | 0 | 1 | 1 | 2/3 |
| [28] | 0 | 1 | 1 | 2/3 |
| [30] | 0 | 1 | 1 | 2/3 |
| [35] | 1 | 1 | 1 | 3/3 |
| [26] | 1 | 1 | 1 | 3/3 |
| [36] | 0 | 1 | 1 | 2/3 |
| [37] | 1 | 1 | 1 | 3/3 |
| [25] | 0 | 1 | 1 | 2/3 |
| Studies | Was an Attempt Made to Blind Study Subjects to the Intervention they had Received | Was an Attempt Made to Blind those Measuring the Main Outcomes of the Intervention | If any of the Results of the Study were Based on “Data Dredging”, was this Made Clear? | In Trials/Cohort Studies, do the Analyses Adjust for Different Lengths of Follow-Up of Patients, or in Case Control Studies, is the Time Period between the Intervention and Outcome the Same for Cases and Controls | Were the Statistical Tests Used to Assess the Main Outcomes Appropriate | Was Compliance with the Intervention/s Reliable? | Were the Main Outcome Measures Used Accurate (Valid and Reliable)? |
|---|---|---|---|---|---|---|---|
| [22] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [27] | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| [32] | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| [24] | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| [13] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [23] | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| [33] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [21] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [34] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [29] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [20] | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| [31] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [28] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [30] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [35] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [26] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [36] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [37] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| [25] | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| Studies | Were the Patients in Different Intervention Groups or were the Cases and Control Recruited from the Same Population | Were Study Subjects in Different Intervention Groups (Trials and Cohort Studies) or were the Cases and Controls Recruited over the Same Period | Were Study Subjects Randomized to Intervention Groups | Was the Randomized Intervention Assignment Concealed from Both Patients and Health Care Staff until Recruitment was Complete and Irrevocable? | Was there Adequate Adjustment for Confounding in the Analysis from which the Main Findings were Drawn? | Were Losses of Patients to Follow-Up Taken into Account |
|---|---|---|---|---|---|---|
| [22] | 0 | 0 | 0 | 0 | 0 | 0 |
| [27] | 0 | 0 | 0 | 0 | 0 | 0 |
| [32] | 0 | 0 | 0 | 0 | 0 | 0 |
| [24] | 0 | 0 | 0 | 0 | 0 | 0 |
| [13] | 0 | 0 | 0 | 0 | 0 | 0 |
| [23] | 0 | 0 | 0 | 0 | 0 | 0 |
| [33] | 0 | 0 | 0 | 0 | 0 | 0 |
| [21] | 0 | 0 | 0 | 0 | 0 | 0 |
| [34] | 0 | 0 | 0 | 0 | 0 | 0 |
| [29] | 0 | 0 | 0 | 0 | 0 | 0 |
| [20] | 0 | 0 | 0 | 0 | 0 | 0 |
| [31] | 0 | 0 | 0 | 0 | 0 | 0 |
| [28] | 0 | 0 | 0 | 0 | 0 | 0 |
| [30] | 1 | 0 | 1 | 1 | 0 | 0 |
| [35] | 0 | 0 | 0 | 0 | 0 | 0 |
| [26] | 0 | 0 | 0 | 0 | 0 | 0 |
| [36] | 0 | 0 | 0 | 0 | 0 | 0 |
| [37] | 0 | 0 | 0 | 0 | 0 | 0 |
| [25] | 0 | 0 | 0 | 0 | 0 | 0 |
| Studies | Level of Evidence | Level 1 | Level 2 | Level 3 | ||||
|---|---|---|---|---|---|---|---|---|
| Risk Factor | RCT Study | Cohort Study | Cross-Sectional Study | Laboratory Study | Prospective Study | Studies | ||
| [22] | Scapulothoracic position | 12 (26) | 1 | |||||
| [22] | Muscle strength | 12 (26) | 1 | |||||
| [22] | Shoulder flexibility | 12 (26) | 2 | |||||
| [23] | 8 (26) | |||||||
| [27] | Age-related shoulder/scapular adaptions | 11 (26) | 1 | |||||
| [32] | Racquet grip size | 10 (26) | 1 | |||||
| [24] | Racquet properties | 5 (26) | 1 | |||||
| [13] | Prolonged tennis | 11 (26) | 5 | |||||
| [29] | Effect of prolonged tennis to shoulder muscle fatigue | 13 (26) | ||||||
| [20] | Effect of prolonged tennis to shoulder range of motion | 10 (26) | ||||||
| [31] | Prolonged tennis may affect shoulder articular cartilage | 12 (26) | ||||||
| [28] | Effect of prolonged tennis on glenohumeral rotation | 14 (26) | ||||||
| [13] | Previous injury | 11 (26) | 2 | |||||
| [34] | 13 (26) | |||||||
| [23] | Range of motion | 8 (26) | 1 | |||||
| [33] | Glenohumeral instability | 12 (26) | 1 | |||||
| [21] | Skills | 13 (26) | 2 | |||||
| [34] | 13 (26) | |||||||
| [21] | Technique | 13 (26) | 2 | |||||
| [34] | 13 (26) | |||||||
| [34] | Kinetic chain | 13 (26) | 1 | |||||
| [30] | Influence of fatigue on scapular kinematics | 12 (26) | 1 | |||||
| [35] | Scapulothoracic kinematics | 13 (26) | 1 | |||||
| [26] | Racquet polar moment of inertia | 13 (26) | 1 | |||||
| [36] | Shoulder rotational muscle imbalances | 12 (26) | 1 | |||||
| [37] | Correlation between scapular dyskinesia and Subacromial space | 13 (26) | 1 | |||||
| [25] | Racquet grip | 12 (26) | 1 | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kekelekis, A.; Nikolaidis, P.T.; Moore, I.S.; Rosemann, T.; Knechtle, B. Risk Factors for Upper Limb Injury in Tennis Players: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2744. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082744
Kekelekis A, Nikolaidis PT, Moore IS, Rosemann T, Knechtle B. Risk Factors for Upper Limb Injury in Tennis Players: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(8):2744. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082744
Chicago/Turabian StyleKekelekis, Afxentios, Pantelis Theodoros Nikolaidis, Isabel Sarah Moore, Thomas Rosemann, and Beat Knechtle. 2020. "Risk Factors for Upper Limb Injury in Tennis Players: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 8: 2744. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082744