Effectiveness of Motivational Interviewing in Regard to Activities of Daily Living and Motivation for Rehabilitation among Stroke Patients


Abstract
:1. Introduction
2. Materials and Methods
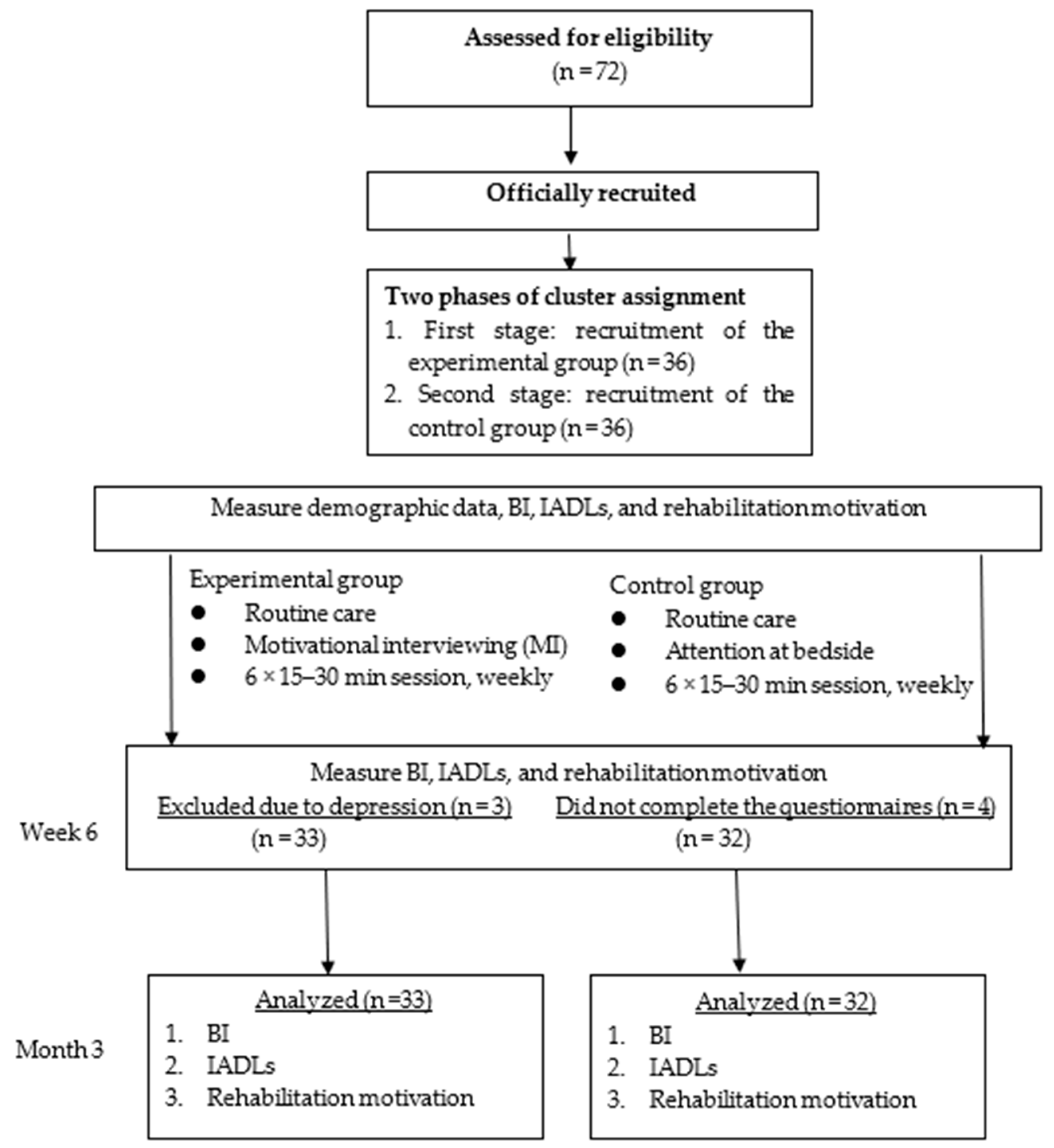
2.1. Study Design
2.2. Participants
2.3. Interventions
2.4. Measurement
2.5. Data Collection
2.6. Statistical Analyses
3. Results
3.1. Basic Demographic Attributes
3.2. Changes in Activities of Daily Living (Barthel Index, BI, and Instrumental Activities of Daily Living, IADLs) of Stroke Patients After the Motivational Interviewing (MI) Intervention
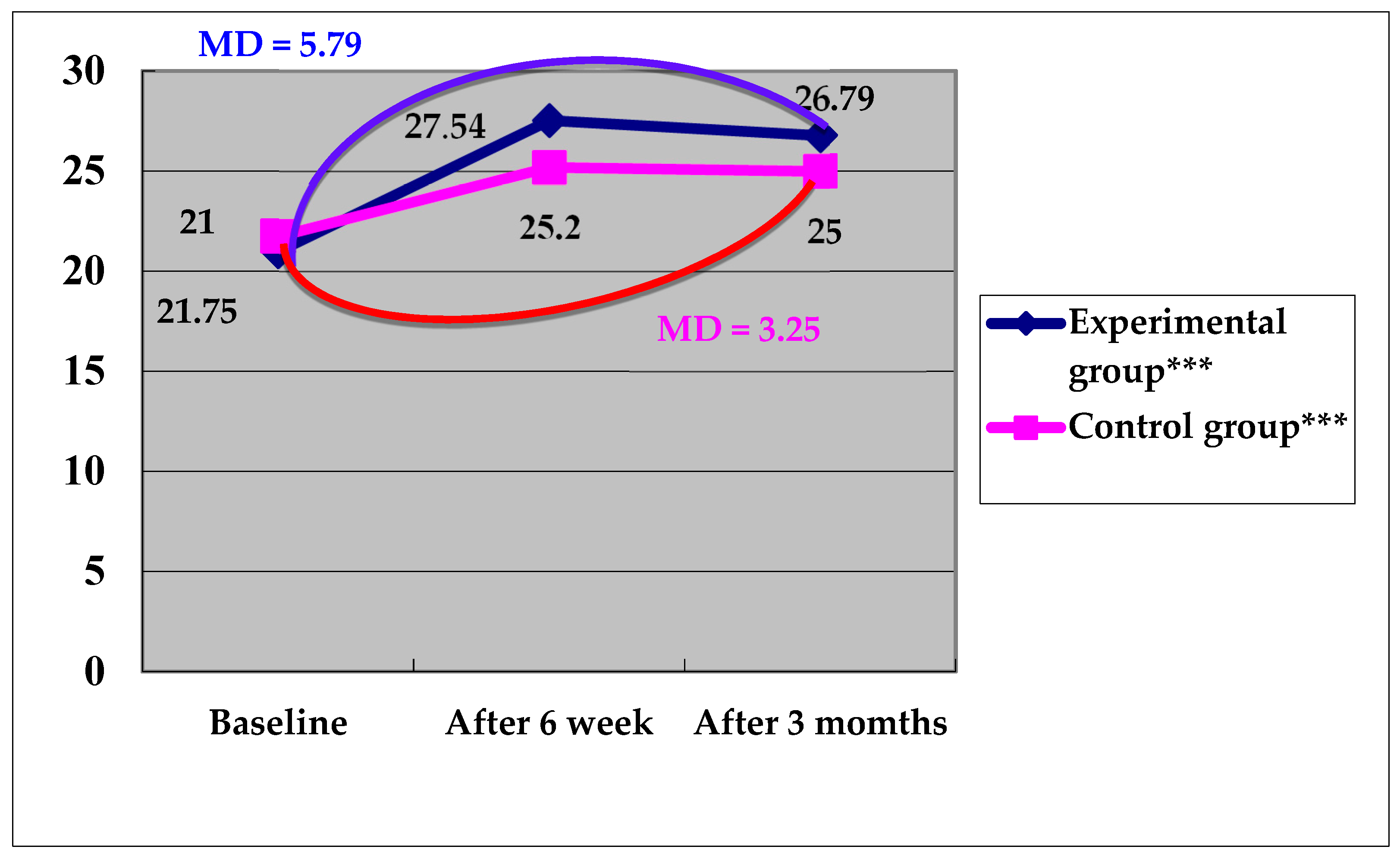
3.3. Changes in Rehabilitation Motivation of Stroke Patients after the MI Intervention
4. Discussion.
4.1. Comparison of Differences in Activities of Daily Living (BI and IADLs) between the Experimental and Control Groups
4.2. Comparison of Motivation for Rehabilitation Between the Experimental and Control Groups
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Khan, N.I.; Chaku, S.; Goehl, C.; Endris, L.; Mueller-Luckey, G.; Siddiqui, F.M. Novel algorithm to help identify stroke mimics. J. Stroke Cerebrovasc. Dis. 2018, 27, 703–708. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Stroke, Cerebrovascular accident. Available online: http://www.emro.who.int/health-topics/stroke-cerebrovascular-accident/index.html (accessed on 24 March 2020).
- Musa, K.I.; Keegan, T.J. The change of Barthel Index scores from the time of discharge until 3-month post-discharge among acute stroke patients in Malaysia: A random intercept model. PLoS ONE 2018, 13, e0208594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blomgren, C.; Samuelsson, H.; Blomstrand, C.; Jern, C.; Jood, K.; Claesson, L. Long-term performance of instrumental activities of daily living in young and middle-aged stroke survivors—Impact of cognitive dysfunction, emotional problems and fatigue. PLoS ONE 2019, 14, e0216822. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Zeng, N.; Wang, C.; Sun, L.; Thomas, G.A.; Wang, H. Effects of mind-body exercises for mood and functional capabilities in patients with stroke: An analytical review of randomized controlled trials. Int. J. Environ. Res. Public. Health 2018, 15, 721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, H.K.; Lee, S.J. The effect of a movie-based nursing intervention program on rehabilitation motivation and depression in stroke patients. J. Korean Acad. Nurs. 2017, 47, 345–356. [Google Scholar] [CrossRef] [Green Version]
- Kawada, S.; Goto, R. Relationship between psychophysiological factors and prognosis for activities of daily living in patients with stroke in a recovery rehabilitation unit: a preliminary study. J. Phys. Ther. Sci. 2017, 29, 2206–2209. [Google Scholar] [CrossRef] [Green Version]
- Rapolienė, J.; Endzelytė, E.; Jasevičienė, I.; Savickas, R. Stroke patients motivation influence on the effectiveness of occupational therapy. Rehabil. Res. Pract. 2018, 2018, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Miller, W.R.; Rose, G.S. Motivational interviewing and decisional balance: contrasting responses to client ambivalence. Behav. Cogn. Psychother. 2015, 43, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Prior, P.L.; Suskin, N. Exercise for stroke prevention. Stroke Vasc. Neurol. 2018, 3, 59–68. [Google Scholar] [CrossRef]
- Derakhshanrad, S.A.; Piven, E. Modification of the persian version of hermans achievement motivation questionnaire to develop an adapted scale for measuring motivation of post-stroke survivors in Iran. Iran. J. Neurol. 2016, 15, 189–194. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods. 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Byers, A.M.; Lamanna, L.; Rosenberg, A. The effect of motivational interviewing after ischemic stroke on patient knowledge and patient satisfaction with care: a pilot study. J. Neurosci. Nurs. 2010, 42, 312–322. [Google Scholar] [CrossRef]
- Yeh, H.F.; Shao, J.H. Exploring the relationship between heart failure symptom and diet self-efficiency old age patient as an example. Hungkuang. Acad. Rev. 2015, 75, 1–11. [Google Scholar]
- Ahluwalia, J.S.; Okuyemi, K.; Nollen, N.; Choi, W.S.; Kaur, H.; Pulvers, K.; Mayo, M.S. The effects of nicotine gum and counseling among African American light smokers: a 2 × 2 factorial design. Addiction 2006, 101, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Redding, C.A.; Evers, K.E. The transtheoretical model and stages of change. Health Behav. Theory Res. Pract. 2015, 125–148. [Google Scholar]
- DiClemente, C.C.; Corno, C.M.; Graydon, M.M.; Wiprovnick, A.E.; Knoblach, D.J. Motivational interviewing, enhancement, and brief interventions over the last decade: a review of reviews of efficacy and effectiveness. Psychol. Addict. Behav. 2017, 31, 862–887. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Vanclay, F.; Cooper, B. Predicting discharge status at commencement of stroke rehabilitation. Stroke 1989, 20, 766–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, H.; Chen, Y.; Mau, L.; Shiao, S.; Liu, H.; Huang, M. An evaluation of the reliability and validity of the Chinese-version OARS multidimensional functional assessment questionnaire. Chin. J. Public Health 1997, 16, 119–132. [Google Scholar]
- Litman, T.J. An analysis of the sociologic factors affecting the rehabilitation of physically handicapped patients. Arch. Phys. Med. Rehabil. 1964, 45, 9–16. [Google Scholar] [PubMed]
- Cheng, D.; Qu, Z.; Huang, J.; Xiao, Y.; Luo, H.; Wang, J. Motivational interviewing for improving recovery after stroke. Cochrane Database Syst. Rev. 2015, 6, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Tshiswaka, D.I.; Seals, S.; Raghavan, P. Correlates of physical function among stroke survivors: an examination of the 2015 BRFSS. Public Health 2018, 155, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.Y.; Ke, C.W.; Kuan, T.S.; Yang, H.C.; Tsai, C.L.; Kuo, L.C. Impacts of sensation, perception, and motor abilities of the Ipsilesional upper limb on hand functions in unilateral stroke: quantifications from biomechanical and functional perspectives. PM&R 2018, 10, 146–153. [Google Scholar]
- Wu, Y.C.; Shao, C.W.; Hsieh, W.Y.; Li, W.C.; Chen, S.Y. Correlation between the concordance and functional performance of upper extremity in daily life after hemiparetic stroke- a pilot study. Formosan. J. Phys. Ther. 2018, 43, 164–165. [Google Scholar]
- Danzl, M.M.; Etter, N.M.; Andreatta, R.D.; Kitzman, P.H. Facilitating neurorehabilitation through principles of engagement. J. Allied. Health 2012, 41, 35–41. [Google Scholar]
- Anstiss, T. Motivational interviewing in primary care. J. Clin. Psychol. Med. Sett. 2009, 16, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.C.; McMahon, B.T. Motivational interviewing and rehabilitation counseling practice. Rehabil. Couns. Bull. 2004, 47, 152–161. [Google Scholar] [CrossRef]
- Balaam, M.; Rennick Egglestone, S.; Fitzpatrick, G.; Rodden, T.; Hughes, A.-M.; Wilkinson, A.; Nind, T.; Axelrod, L.; Harris, E.; Ricketts, I. Motivating mobility: designing for lived motivation in stroke rehabilitation. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Vancouver, BC, Canada, 7–12 May 2011; pp. 3073–3082. [Google Scholar]
- Chin, J.M.; Cheng, C.C.; Yu, W.P.; Chen, S.C. Nursing care experience for an adolescent with stroke. J. Nurs. 2016, 27, 285–295. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Total (N = 65) | Experimental Group (N = 33) | Control Group (N = 32) | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | x2 | p | |
| Sex | 0.23 | 0.639 | ||||||
| Male | 47 | 72.3 | 23 | 69.7 | 24 | 75.0 | ||
| Female | 18 | 27.7 | 10 | 30.3 | 8 | 25.0 | ||
| Marital status | 0.13 | 0.727 | ||||||
| Unmarried/widowed/divorced | 17 | 26.2 | 8 | 24.2 | 9 | 28.1 | ||
| Married/cohabiting/separated | 48 | 73.8 | 25 | 75.8 | 23 | 71.9 | ||
| Living situation | 2.05 | 0.157 | ||||||
| Solitary | 5 | 7.7 | 1 | 3.0 | 4 | 12.5 | ||
| With others | 60 | 92.3 | 32 | 97.0 | 28 | 87.5 | ||
| Religion | 1.97 | 0.168 | ||||||
| No | 15 | 23.1 | 10 | 30.3 | 5 | 15.6 | ||
| Yes | 50 | 76.9 | 23 | 69.7 | 27 | 84.4 | ||
| Level of education | 12.45 | 0.060 | ||||||
| Junior high school/under junior high school | 37 | 56.9 | 25 | 75.8 | 12 | 37.5 | ||
| High school (vocational) | 15 | 23.1 | 5 | 15.2 | 10 | 31.3 | ||
| College or above | 13 | 20.0 | 3 | 9.1 | 10 | 31.3 | ||
| Working situation | 1.06 | 0.312 | ||||||
| No | 56 | 86.2 | 27 | 81.8 | 29 | 90.6 | ||
| Yes | 9 | 13.8 | 6 | 18.2 | 3 | 9.4 | ||
| Economic conditions | ||||||||
| Main source of income | 2.09 | 0.470 | ||||||
| Children/spouse/brothers or sisters/parent/other | 34 | 52.3 | 19 | 57.6 | 15 | 46.9 | ||
| Pension/government grants | 16 | 24.6 | 6 | 18.2 | 10 | 31.3 | ||
| Work | 15 | 23.1 | 8 | 24.2 | 7 | 21.9 | ||
| Adequacy of the cost of living | 6.60 | 0.776 | ||||||
| Sufficient and more than/roughly enough | 31 | 47.7 | 11 | 33.3 | 20 | 62.5 | ||
| Inadequate | 32 | 49.2 | 20 | 60.6 | 12 | 37.5 | ||
| Very inadequate | 2 | 3.1 | 2 | 6.1 | 0 | 0 | ||
| Smoking history | 0.02 | 0.892 | ||||||
| Non-smoker | 36 | 55.4 | 18 | 5.4 | 18 | 56.3 | ||
| Smoker | 29 | 44.6 | 15 | 45.5 | 14 | 43.7 | 0.38 | 0.544 |
| Type of stroke | ||||||||
| Blockage/ischemic stroke | 33 | 50.8 | 18 | 54.5 | 15 | 46.9 | ||
| Hemorrhagic stroke | 32 | 49.2 | 15 | 45.5 | 17 | 53.1 | ||
| Stroke area | 9.35 | 0.543 | ||||||
| Anterior cerebral artery | 12 | 18.5 | 7 | 21.2 | 5 | 15.6 | ||
| Middle cerebral artery | 21 | 32.3 | 12 | 36.4 | 9 | 28.1 | ||
| Posterior cerebral artery | 8 | 12.3 | 6 | 18.2 | 2 | 6.3 | ||
| Basal ganglia | 10 | 15.4 | 2 | 6.1 | 8 | 25.0 | ||
| Thalamus | 2 | 3.1 | 1 | 3.0 | 1 | 3.1 | ||
| Intracranial hemorrhage | 8 | 12.3 | 2 | 6.1 | 6 | 18.8 | ||
| Brain stem | 4 | 6.2 | 3 | 9.1 | 1 | 3.1 | ||
| Hemi paralysis | 0.12 | 0.731 | ||||||
| Left side | 44 | 67.7 | 23 | 69.7 | 21 | 65.6 | ||
| Right side | 21 | 32.3 | 10 | 30.3 | 11 | 34.4 | ||
| Risk factors for stroke | 0.83 | 0.569 | ||||||
| No | 4 | 6.2 | 2 | 6.1 | 2 | 6.3 | ||
| Hypertension | 32 | 49.2 | 17 | 51.5 | 15 | 46.9 | ||
| Diabetes | 3 | 4.6 | 2 | 6.1 | 1 | 3.1 | ||
| Heart disease | 4 | 6.2 | 2 | 6.1 | 2 | 6.3 | ||
| Cardiovascular disease and diabetes | 19 | 29.2 | 9 | 27.3 | 10 | 31.3 | ||
| Hypertension and heart disease | 3 | 4.6 | 1 | 3.0 | 2 | 6.3 | ||
| Mean | SD | Mean | SD | Mean | SD | t | p | |
| Age | 61.46 | 13.88 | 61.61 | 14.71 | 61.31 | 2.60 | 0.09 | 0.933 |
| Number of people living together | 3.37 | 2.53 | 4.12 | 2.76 | 2.60 | 2.05 | 2.53 | 0.360 |
| Number of diseases | 2.79 | 1.10 | 2.33 | 0.89 | 3.19 | 1.26 | −3.39 | 0.052 |
| Items | Mean (SD) | MD | F | p | |||
|---|---|---|---|---|---|---|---|
| Time 1 | Time 2 | Time 3 | T2 − T1 | T3 − T1 | |||
| Experimental group (N = 33) | |||||||
| BI | 32.66 (16.66) | 51.20 (20.67) | 59.38 (23.51) | 18.59 * | 26.72 * | 42.90 | <0.001 *** |
| IADLs | 4.38 (3.21) | 6.84 (3.82) | 7.56 (3.78) | 2.47 * | 3.19b * | 22.88 | <0.001 *** |
| Motivation for rehabilitation | 21.00 (3.74) | 27.54 (2.59) | 26.79 (4.17) | 6.55 * | 5.79 * | 54.60 | <0.001 *** |
| Control group (N = 32) | |||||||
| BI | 40.45 (17.96) | 58.03 (21.50) | 63.15 (26.63) | 17.58 * | 22.70 * | 30.85 | <0.001 *** |
| IADLs | 5.24 (2.70) | 8.48 (3.95) | 9.39 (5.03) | 3.24 * | 4.15 * | 18.10 | <0.001 *** |
| Motivation for rehabilitation | 21.75 (3.02) | 25.20 (4.18) | 25.00 (3.72) | 3.45 * | 3.25 * | 16.24 | <0.001 *** |
| Parameter | Estimate (B) | S.E. | Wald x2 | p-Value |
|---|---|---|---|---|
| BI | ||||
| Intercept | 32.66 | 2.90 | 126.99 | <0.001 *** |
| Group | −7.80 | 4.23 | 3.40 | 0.070 |
| Time 2 (T2) | 17.58 | 3.00 | 38.43 | <0.001 *** |
| Time 3 (T3) | 22.70 | 3.52 | 57.65 | <0.001 *** |
| Group*Time (T2) | 1.02 | 3.61 | 0.08 | 0.782 |
| Group*Time (T3) | 4.02 | 5.08 | 6.26 | 0.436 |
| IADLs c | ||||
| Intercept | 4.37 | 0.56 | 61.35 | <0.001 *** |
| Group | −0.87 | 0.72 | 1.43 | 0.231 |
| Time 2 (T2) | 3.24 | 0.54 | 20.81 | <0.001 *** |
| Time 3 (T3) | 4.15 | 0.57 | 31.01 | <0.001 *** |
| Group*Time (T2) | −0.77 | 0.78 | 0.97 | 0.324 |
| Group*Time (T3) | −0.96 | 0.98 | 0.97 | 0.325 |
| Motivation for rehabilitation | ||||
| Intercept | 21.75 | 0.52 | 1717.79 | <0.001 *** |
| Group | −0.75 | 0.83 | 0.82 | 0.372 |
| Time 2 (T2) | 3.45 | 0.60 | 33.43 | <0.001 *** |
| Time 3 (T3) | 3.25 | 0.71 | 20.72 | <0.001 *** |
| Group*Time (T2) | 3.10 | 0.83 | 14.03 | <0.001 *** |
| Group*Time (T3) | 2.54 | 1.09 | 5.38 | 0.026 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-M.; Lee, H.-L.; Yang, F.-C.; Chiu, Y.-W.; Chao, S.-Y. Effectiveness of Motivational Interviewing in Regard to Activities of Daily Living and Motivation for Rehabilitation among Stroke Patients. Int. J. Environ. Res. Public Health 2020, 17, 2755. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082755
Chen H-M, Lee H-L, Yang F-C, Chiu Y-W, Chao S-Y. Effectiveness of Motivational Interviewing in Regard to Activities of Daily Living and Motivation for Rehabilitation among Stroke Patients. International Journal of Environmental Research and Public Health. 2020; 17(8):2755. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082755
Chicago/Turabian StyleChen, Hsiao-Mei, Hsiao-Lu Lee, Fu-Chi Yang, Yi-Wen Chiu, and Shu-Yuan Chao. 2020. "Effectiveness of Motivational Interviewing in Regard to Activities of Daily Living and Motivation for Rehabilitation among Stroke Patients" International Journal of Environmental Research and Public Health 17, no. 8: 2755. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082755