Lifetime Costs of Surviving Cancer—A Queensland Study (COS-Q): Protocol of a Large Healthcare Data Linkage Study

 ,
, 
Abstract
:1. Introduction
- (1)
- To quantify lifetime health service use by cancer patients from the date of diagnosis.
- (2)
- To identify factors associated with high and low health service use.
- (3)
- To estimate lifetime health service use and cost by cancer type from the date of diagnosis using economic modeling.
- (4)
- To identify opportunities for improvement for future health service delivery.
2. Materials and Methods
2.1. Study Cohort
2.2. Ethical Approval and Consent to Participate
2.3. Data Collection
- (1)
- Queensland Cancer Register (QCR)
- (2)
- Queensland Hospital Admitted Patient Data Collection (QHAPDC)
- (3)
- Emergency Department Information System (EDIS)
- (4)
- Healthcare Purchasing & System Performance data (HPSP), HHS Funding Models: National Hospital Cost Data Collection (NHCDC), Patient Activity Weighting (PAWS/ GenWAU)
- (5)
- Medicare Benefits Schedule (MBS)
- (6)
- Pharmaceutical Benefit Schedule (PBS)
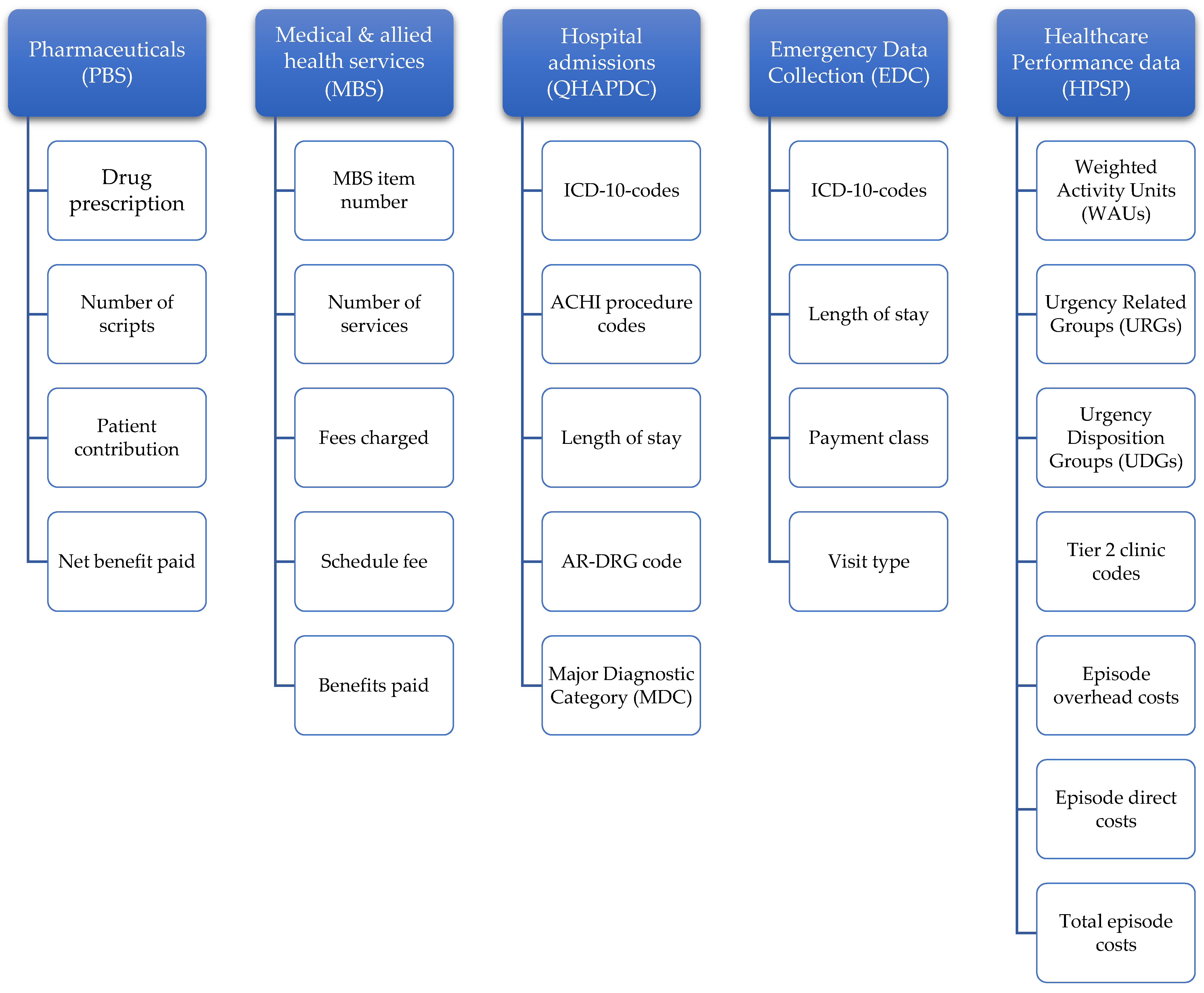
2.4. Data Items Collected
2.5. Data Linkage Process
- SSB formats QCR cohort as required by AIHW. All identifying information to be included to allow AIHW to identify cases. A new, random ID is attached to each case patient, e.g., ‘CASE00000001’.
- QHAPDC & EDIS data are linked by SSB and episode IDs of all patient cohort records are transferred to HPSP.
- Extracted data by HPSP will be transferred back to SSB for matching back to linked records.
- SSB will complete extraction of all Queensland data (including QCR data), and transfer this to a Secure Unified Research Environment (SURE) administered by the Sax Institute in Sydney, Australia.
- SSB transfers cohort file to AIHW using secure file transfer service.
2.6. Data Storage
2.7. Analyses
2.7.1. For Aims 1–2: Analysis of Linked Healthcare Records Over Time
2.7.2. For aim 3: Economic Modeling Estimating Lifetime Outcomes of Surviving Cancer (Based on Findings from Aims 1–2)
2.7.3. For Aims 4: Identifying Opportunities of Improvement for Future Health Service Delivery
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Database | Purpose | Timeframe for Data Extraction | Linkage Variables * | Research Variables |
|---|---|---|---|---|
| Queensland Cancer Registry (QCR) | To identify the initial cohort of cancer patients diagnosed in Queensland | 1 January 1997–31 December 2015 as it becomes available | - Surname - Given names - Sex - Date of birth - Address - Suburb - Postcode - Facility identifier - UR number - Date of diagnosis | - Age at diagnosis - Month/Year of birth - Statistical Area Level 2 - Occupation - Country of Birth - Indigenous Status - Marital Status - Age at death - Cause of Death - Site Code in ICD-O-3 (International Classification of Diseases for Oncology, 3rd Edition) - Morphology in ICD-O-3 (International Classification of Diseases for Oncology, 3rd Edition) - Differentiation - Behavior code (status) - Date of Diagnosis - Basis of Diagnosis - Laterality - Suburb (where patient was living at when diagnosed) - Postcode (where patient was living at when diagnosed) If Breast Tumor: - Tumor Size - Number of Nodes - Number of Positive Nodes If Melanoma Tumor: - Clark’s Level - Thickness - Ulceration |
| Queensland Hospital Admitted Patient Data Collection (QHAPDC) | To capture hospitalizations of cancer survivors over time | 1 January 2002–31 December 2016 for public facilities 1 July 2007–31 December 2016 for private facilities | - Patient identifier (UR number) - Facility identifier - Surname - First given name - Second given name - Third given name - Sex - Date of birth - Postcode | (a) Socio-economic variables: - Sex - Postcode - Estimated date of birth flag - Single year of age capped at 85+years - Marital status - Indigenous status (Flag Indigenous/non-Indigenous) - Facility HHS (hospital and health service) - Patient HHS (hospital and health service) - ARIA (Accessibility and Remoteness Index of Australia) - SEIFA (Socio-Economic Index For Areas based on the index of relative advantage and disadvantage) - Statistical Locality Area (SLA) of usual residence - Type of usual accommodation (for mental health episodes only) - Employment status (for mental health episodes only) - Pension status (for mental health episodes only) (b) Episode of care variables: - Admission date (MMYYYY) - Separation date (MMYYYY) - Mode of separation - Length of stay in days * (capped at 500+days)) - Admission ward - Standard ward code - Standard unit - Principal diagnosis (International Classification of Diseases code) - Additional diagnoses (International Classification of Diseases codes) (all) - External causes (International Classification of Diseases codes) - Morphology (International Classification of Diseases codes) - Length of stay in intensive care unit - Psych days (length of stay in a psychiatric unit in days) - Procedures (Australian Classification of Health Interventions codes) (all) - Block codes for procedures (Australian Classification of Health Interventions procedure block codes) - Procedure dates (MMYYYY) - AR-DRG codes (Australian Refined Diagnosis Related Groups) - MDC code (Major Diagnostic Category) (c) Other information: - Facility type - Elective patient status - Source of referral/transfer - Care type - Planned same day (Y/N) - Hospital insurance status - Funding source - First admission for psychiatric treatment - Referral for further care (for psychiatric patients) - Previous specialized non-admitted treatment (for psychiatric patients) (Y/N) - Mental health phase of care type - First admission for palliative care treatment (Y/N) - Previous specialized non-admitted palliative care treatment (Y/N) (d) Telehealth variables (public hospitals only): (available approx. 1 September 2012) - Admitted patient telehealth activity - Start date * - Start time - End date * - End time - Provider type - Telehealth event type * We would like to receive length of stay in days which will be required to inform distributions of transition probabilities in the economic models; if length of stay variables are capped at 30+ days this would underestimate the burden on health services and hence overall cost. Similarly, it is important to use the duration of telehealth activities for translation to healthcare costs, i.e., the day-month-year format would be more suitable. |
| Emergency Department Information System (EDIS) | To capture emergency admissions of cancer survivors over time | 1 January 2009–31 December 2016 | - Surname - First given name - Second given name - Third given name - Sex - Date of birth - Patient usual residence—address - Patient usual residence—suburb - Patient usual residence—postcode - DVA file number - Medicare number - Facility identifier - Hospital UR number - Presentation date | - Sex - Estimated date of birth indicator - Patient country of birth - Patient indigenous status - Presentation datetime - Triage category - Triage datetime - Arrival transport mode - Visit type - Payment class - Service commencement datetime - Principal diagnosis (International Classification of Diseases code) - Episode end status - Episode end datetime |
| Healthcare Purchasing & System Performance data (HPSP), HHS Funding Models: National Hospital Cost data (NHCDC) & Patient Activity Weighting (PAWS)/(GenWAU) | To capture healthcare funding related to healthcare records | 1 July 2012–31 December 2016 | - For inpatients: Episode ID, including Year, facility ID and facility unique ID - For ED patients: Year, facility ID, hospital UR number, presentation date (supplied by Statistical Services Branch, Queensland Health) | - Weighted Activity Units (WAUs) - Urgency Related Groups (URGs) - Urgency Disposition Groups (UDGs) - Tier 2 clinic codes - Total episode costs - Overhead costs - Direct costs |
| Medicare Benefits Schedule (MBS) | To estimate healthcare usage for non-hospital events (e.g., GP, specialist services) | 1 January 1997–31 December 2016 as it becomes available | - Person identification number (assigned by the state/territory) - Surname - First given name - Second given name - Third given name - Sex - Date of birth - Patient postcode | - Date of service - Date of referral - MBS item number - MBS item description - MBS item category - Broad type of service - Hospital indicator - Bill type - Number of services - Fee charged - Schedule fee - Benefit paid - Servicing provider registered specialty |
| Pharmaceutical Benefit Schedule (PBS) | To estimate healthcare usage as per pharmaceuticals consumed | 1 May 2002–31 December 2016 as it becomes available | - Person identification number (assigned by the state/territory) - Surname - First given name - Second given name - Third given name - Sex - Date of birth - Patient postcode | - Date of supply - Date of prescribing - PBS item number - Drug name - Form and strength - ATC code - Patient category - Form category - Number of scripts - Patient contribution - Net benefit - Prescriber major specialty |
References
- Rowland, J.; Yabroff, R. Cancer Survivorship. In The Cancer Atlas, 3rd ed.; Jemal, A.T.L., Soerjomataram, I.F.B., Eds.; American Cancer Society: Atlanta, GA, USA, 2019; pp. 66–67. [Google Scholar]
- American Cancer Society. Cancer Treatment & Survivorship Facts & Figures 2019–2021; American Cancer Society: Atlanta, GA, USA, 2019. [Google Scholar]
- Cancer Council Victoria. Australians Living with and Beyond Cancer in 2040. Available online: https://www.cancervic.org.au/research/registry-statistics/statistics-data/cancer-prevalence-in-2040.html (accessed on 5 April 2020).
- Denlinger, C.S.; Carlson, R.W.; Are, M.; Baker, K.S.; Davis, E.; Edge, S.B.; Friedman, D.L.; Goldman, M.; Jones, L.; King, A.; et al. Survivorship: Introduction and definition. Clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2014, 12, 34–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marzorati, C.; Riva, S.; Pravettoni, G. Who Is a Cancer Survivor? A Systematic Review of Published Definitions. J. Cancer Educ. 2017, 32, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Cancer in Australia: Actual incidence data from 1982 to 2013 and mortality data from 1982 to 2014 with projections to 2017. Asia Pac. J. Clin. Oncol. 2018, 14, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, K.; Lines, L.M.; Lee, D.W.; Korn, J.R.; Earle, C.C.; Menzin, J. Lifetime and treatment-phase costs associated with colorectal cancer: Evidence from SEER-Medicare data. Clin. Gastroenterol. Hepatol. 2009, 7, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Ananda, S.; Kosmider, S.; Tran, B.; Field, K.; Jones, I.; Skinner, I.; Guerrieri, M.; Chapman, M.; Gibbs, P. The rapidly escalating cost of treating colorectal cancer in Australia. Asia Pac. J. Clin. Oncol. 2016, 12, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Inotai, A.; Abonyi-Toth, Z.; Rokszin, G.; Voko, Z. Occurrence, Survival and Annual Cost of Colorectal-, Breast-, Prostate-and Lung Cancer in Hungary. Value Health 2014, 17, A553. [Google Scholar] [CrossRef] [Green Version]
- Gordon, L.G.; Rowell, D. Health system costs of skin cancer and cost-effectiveness of skin cancer prevention and screening: A systematic review. Eur. J. Cancer Prev. 2015, 24, 141–149. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Health system expenditure on cancer and other neoplasms in Australia: 2008–2009; Cancer Series No. 81. Cat. No. 78; AIHW: Canberra, Australia, 2013. [Google Scholar]
- Valdivieso, M.; Kujawa, A.M.; Jones, T.; Baker, L.H. Cancer survivors in the United States: A review of the literature and a call to action. Int. J. Med. Sci. 2012, 9, 163–173. [Google Scholar] [CrossRef] [Green Version]
- Naughton, M.J.; Weaver, K.E. Physical and mental health among cancer survivors: Considerations for long-term care and quality of life. N. C. Med. J. 2014, 75, 283–286. [Google Scholar] [CrossRef]
- Harrington, C.B.; Hansen, J.A.; Moskowitz, M.; Todd, B.L.; Feuerstein, M. It’s not over when it’s over: Long-term symptoms in cancer survivors—A systematic review. Int. J. Psychiatry Med. 2010, 40, 163–181. [Google Scholar] [CrossRef]
- Carneiro Teixeira, J.F.; Maia-Lemos, P.D.S.; Cypriano, M.D.S.; Pellegrini Pisani, L. Obesity in Survivors of Childhood Cancer: A Review. Pediatr. Endocrinol. Rev. 2017, 15, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Gawade, P.L.; Hudson, M.M.; Kaste, S.C.; Neglia, J.P.; Constine, L.S.; Robison, L.L.; Ness, K.K. A systematic review of dental late effects in survivors of childhood cancer. Pediatr. Blood Cancer 2014, 61, 407–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gawade, P.L.; Hudson, M.M.; Kaste, S.C.; Neglia, J.P.; Wasilewski-Masker, K.; Constine, L.S.; Robison, L.L.; Ness, K.K. A systematic review of selected musculoskeletal late effects in survivors of childhood cancer. Curr. Pediatr. Rev. 2014, 10, 249–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michel, G.; Vetsch, J. Screening for psychological late effects in childhood, adolescent and young adult cancer survivors: A systematic review. Curr. Opin. Oncol. 2015, 27, 297–305. [Google Scholar] [CrossRef]
- O’Sullivan, D. Late effects of chemotherapeutic agents on renal function in childhood cancer survivors: A review of the literature. Ir. J. Med. Sci. 2017, 186, 49–55. [Google Scholar] [CrossRef]
- Overbeek, A.; van den Berg, M.H.; van Leeuwen, F.E.; Kaspers, G.J.; Lambalk, C.B.; van Dulmen-den Broeder, E. Chemotherapy-related late adverse effects on ovarian function in female survivors of childhood and young adult cancer: A systematic review. Cancer Treat. Rev. 2017, 53, 10–24. [Google Scholar] [CrossRef] [PubMed]
- van Deuren, S.; Boonstra, A.; van Dulmen-den Broeder, E.; Blijlevens, N.; Knoop, H.; Loonen, J. Severe fatigue after treatment for childhood cancer. Cochrane Database Syst. Rev. 2020, 3, CD012681. [Google Scholar] [CrossRef] [PubMed]
- Duckett, S.; Willcox, S. The Australian Health Care System; Oxford University Press: Melbourne, Australia, 2015. [Google Scholar]
- Gordon, L.G.; Merollini, K.M.D.; Lowe, A.; Chan, R.J. A Systematic Review of Financial Toxicity Among Cancer Survivors: We Can’t Pay the Co-Pay. Patient 2017, 10, 295–309. [Google Scholar] [CrossRef] [Green Version]
- Zafar, S.Y. Financial Toxicity of Cancer Care: It’s Time to Intervene. J. Natl. Cancer Inst. 2016, 108, djv370. [Google Scholar] [CrossRef] [Green Version]
- Callander, E.; Bates, N.; Lindsay, D.; Larkins, S.; Topp, S.M.; Cunningham, J.; Sabesan, S.; Garvey, G. Long-term out of pocket expenditure of people with cancer: Comparing health service cost and use for indigenous and non-indigenous people with cancer in Australia. Int. J. Equity Health 2019, 18, 32. [Google Scholar] [CrossRef] [Green Version]
- Gordon, L.G.; Elliott, T.M.; Olsen, C.M.; Pandeya, N.; Whiteman, D.C.; Study, Q.S. Patient out-of-pocket medical expenses over 2 years among Queenslanders with and without a major cancer. Aust. J. Prim. Health 2018, 24, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Newton, J.C.; Johnson, C.E.; Hohnen, H.; Bulsara, M.; Ives, A.; McKiernan, S.; Platt, V.; McConigley, R.; Slavova-Azmanova, N.S.; Saunders, C. Out-of-pocket expenses experienced by rural Western Australians diagnosed with cancer. Support. Care Cancer 2018, 26, 3543–3552. [Google Scholar] [CrossRef] [PubMed]
- Ekwueme, D.U.; Zhao, J.; Rim, S.H.; de Moor, J.S.; Zheng, Z.; Khushalani, J.S.; Han, X.; Kent, E.E.; Yabroff, K.R. Annual Out-of-Pocket Expenditures and Financial Hardship Among Cancer Survivors Aged 18-64 Years-United States, 2011–2016. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 494–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buttner, M.; Konig, H.H.; Lobner, M.; Briest, S.; Konnopka, A.; Dietz, A.; Riedel-Heller, S.; Singer, S. Out-of-pocket-payments and the financial burden of 502 cancer patients of working age in Germany: Results from a longitudinal study. Support. Care Cancer 2019, 27, 2221–2228. [Google Scholar] [CrossRef] [PubMed]
- Fitch, M.; Longo, C.J. Exploring the impact of out-of-pocket costs on the quality of life of Canadian cancer patients. J. Psychosoc. Oncol. 2018, 36, 582–596. [Google Scholar] [CrossRef]
- Russell, H.; Bernhardt, M.B. Bending the Cost Curve in Childhood Cancer. Curr. Hematol. Malig. Rep. 2016, 11, 295–302. [Google Scholar] [CrossRef]
- Cohn, R.J.; Goodenough, B.; Foreman, T.; Suneson, J. Hidden financial costs in treatment for childhood cancer: An Australian study of lifestyle implications for families absorbing out-of-pocket expenses. J. Pediatr. Hematol. Oncol. 2003, 25, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Heath, J.A.; Lintuuran, R.M.; Rigguto, G.; Tokatlian, N.; McCarthy, M. Childhood cancer: Its impact and financial costs for Australian families. Pediatr. Hematol. Oncol. 2006, 23, 439–448. [Google Scholar] [CrossRef]
- Warner, E.L.; Kirchhoff, A.C.; Nam, G.E.; Fluchel, M. Financial Burden of Pediatric Cancer for Patients and Their Families. J. Oncol. Pract. 2014, 11, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Rativa Velandia, M.; Carreno Moreno, S.P. Family Economic Burden Associated to Caring for Children with Cancer. Investig. Educ. Enferm. 2018, 36, e07. [Google Scholar] [CrossRef]
- Sneha, L.M.; Sai, J.; Ashwini, S.; Ramaswamy, S.; Rajan, M.; Scott, J.X. Financial Burden Faced by Families due to Out-of-pocket Expenses during the Treatment of their Cancer Children: An Indian Perspective. Indian J. Med. Paediatr. Oncol. 2017, 38, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Goldsbury, D.E.; Yap, S.; Weber, M.F.; Veerman, L.; Rankin, N.; Banks, E.; Canfell, K.; O’Connell, D.L. Health services costs for cancer care in Australia: Estimates from the 45 and Up Study. PLoS ONE 2018, 13, e0201552. [Google Scholar] [CrossRef]
- Bates, N.; Callander, E.; Lindsay, D.; Watt, K. CancerCostMod: A model of the healthcare expenditure, patient resource use, and patient co-payment costs for Australian cancer patients. Health Econ. Rev. 2018, 8, 28. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.S.; Rutten, F.F.; van Ineveld, B.M.; Redekop, W.K.; Hakkaart-van Roijen, L. Comparing methodologies for the cost estimation of hospital services. Eur. J. Health Econ. 2009, 10, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Barber, J.A.; Thompson, S.G. Analysis of cost data in randomized trials: An application of the non-parametric bootstrap. Stat. Med. 2000, 19, 3219–3236. [Google Scholar] [CrossRef]
- Liao, M.; Li, Y.; Kianifard, F.; Obi, E.; Arcona, S. Cluster analysis and its application to healthcare claims data: A study of end-stage renal disease patients who initiated hemodialysis. BMC Nephrol. 2016, 17, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lê Cook, B.; Manning, W.G. Thinking beyond the mean: A practical guide for using quantile regression methods for health services research. Shanghai Arch. Psychiatry 2013, 25, 55–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deb, P.; Norton, E.C. Modeling Health Care Expenditures and Use. Ann. Rev. Public Health 2018, 39, 489–505. [Google Scholar] [CrossRef] [Green Version]
- Bojke, L.; Manca, A.; Asaria, M.; Mahon, R.; Ren, S.; Palmer, S. How to Appropriately Extrapolate Costs and Utilities in Cost-Effectiveness Analysis. Pharmacoeconomics 2017, 35, 767–776. [Google Scholar] [CrossRef]
- Briggs, A.H.; Weinstein, M.C.; Fenwick, E.A.; Karnon, J.; Sculpher, M.J.; Paltiel, A.D.; Force, I.-S.M.G.R.P.T. Model parameter estimation and uncertainty: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force—6. Value Health 2012, 15, 835–842. [Google Scholar] [CrossRef] [Green Version]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)—Explanation and elaboration: A report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health 2013, 16, 231–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limwattananon, S. Handling uncertainty of the economic evaluation result: Sensitivity analysis. J. Med. Assoc. Thai. 2008, 91, S59–S65. [Google Scholar] [PubMed]
- Briggs, A.H. Statistical approaches to handling uncertainty in health economic evaluation. Eur. J. Gastroenterol. Hepatol. 2004, 16, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Badgery-Parker, T.; Pearson, S.A.; Chalmers, K.; Brett, J.; Scott, I.A.; Dunn, S.; Onley, N.; Elshaug, A.G. Low-value care in Australian public hospitals: Prevalence and trends over time. BMJ Qual. Saf. 2019, 28, 205–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, N.; Callander, E.; Lindsay, D.; Watt, K. Labour force participation and the cost of lost productivity due to cancer in Australia. BMC Public Health 2018, 18, 375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanly, P.; Ceilleachair, A.O.; Skally, M.; O’Leary, E.; Kapur, K.; Fitzpatrick, P.; Staines, A.; Sharp, L. How much does it cost to care for survivors of colorectal cancer? Caregiver’s time, travel and out-of-pocket costs. Support. Care Cancer 2013, 21, 2583–2592. [Google Scholar] [CrossRef]
- de Oliveira, C.; Pataky, R.; Bremner, K.E.; Rangrej, J.; Chan, K.K.; Cheung, W.Y.; Hoch, J.S.; Peacock, S.; Krahn, M.D. Phase-specific and lifetime costs of cancer care in Ontario, Canada. BMC Cancer 2016, 16, 809. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira, C.; Weir, S.; Rangrej, J.; Krahn, M.D.; Mittmann, N.; Hoch, J.S.; Chan, K.K.W.; Peacock, S. The economic burden of cancer care in Canada: A population-based cost study. CMAJ Open 2018, 6, E1–E10. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira, C.; Bremner, K.E.; Liu, N.; Greenberg, M.L.; Nathan, P.C.; McBride, M.L.; Krahn, M.D. Costs of cancer care in children and adolescents in Ontario, Canada. Pediatr. Blood Cancer 2017, 64. [Google Scholar] [CrossRef]
- Luengo-Fernandez, R.; Leal, J.; Gray, A.; Sullivan, R. Economic burden of cancer across the European Union: A population-based cost analysis. Lancet Oncol. 2013, 14, 1165–1174. [Google Scholar] [CrossRef]
- Sam, D.; Cheung, W.Y. A population-level comparison of cancer-related and non-cancer-related health care costs using publicly available provincial administrative data. Curr. Oncol. 2019, 26, 94–97. [Google Scholar] [CrossRef] [Green Version]
- Avritscher, E.B.; Cooksley, C.D.; Grossman, H.B.; Sabichi, A.L.; Hamblin, L.; Dinney, C.P.; Elting, L.S. Clinical model of lifetime cost of treating bladder cancer and associated complications. Urology 2006, 68, 549–553. [Google Scholar] [CrossRef]
- Barrows, C.E.; Belle, J.M.; Fleishman, A.; Lubitz, C.C.; James, B.C. Financial burden of thyroid cancer in the United States: An estimate of economic and psychological hardship among thyroid cancer survivors. Surgery 2020, 167, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Bermejo de Las Heras, B.; Cortes Ramon, Y.C.J.; Galve Calvo, E.; de la Haba Rodriguez, J.; Garcia Mata, J.; Moreno Anton, F.; Pelaez Fernandez, I.; Rodriguez-Lescure, A.; Rodriguez Sanchez, C.A.; Ruiz-Borrego, M.; et al. The economic burden of metastatic breast cancer in Spain. Eur. J. Hosp. Pharm. 2020, 27, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Corral, J.; Castells, X.; Molins, E.; Chiarello, P.; Borras, J.M.; Cots, F. Long-term costs of colorectal cancer treatment in Spain. BMC Health Serv. Res. 2016, 16, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Ortega, L.; Gonzalez-Dominguez, A.; Borras, J.M.; Oliva-Moreno, J.; Gonzalez-Haba, E.; Menjon, S.; Perez, P.; Vicente, D.; Cordero, L.; Jimenez, M.; et al. The economic burden of disease of epithelial ovarian cancer in Spain: The OvarCost study. Eur. J. Health Econ. 2019, 20, 135–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsey, S.D.; Berry, K.; Etzioni, R. Lifetime cancer-attributable cost of care for long term survivors of colorectal cancer. Am. J. Gastroenterol. 2002, 97, 440–445. [Google Scholar] [CrossRef]
- Schernberg, A.; Sagaon-Teyssier, L.; Schwarzinger, M.; Group, E.S. Clinical and economic burden of head and neck cancer: A nationwide retrospective cohort study from France. Clin. Outcomes Res. 2019, 11, 441–451. [Google Scholar] [CrossRef] [Green Version]
- You, C.H.; Kang, S.; Kwon, Y.D. The Economic Burden of Breast Cancer Survivors in Korea: A Descriptive Study Using a 26-Month Micro-Costing Cohort Approach. Asian Pac. J. Cancer Prev. 2019, 20, 2131–2137. [Google Scholar] [CrossRef] [Green Version]
- Jonsson, B. Cost of Cancer: Healthcare Expenditures and Economic Impact. Recent Results Cancer Res. 2019, 213, 7–23. [Google Scholar] [CrossRef]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merollini, K.M.D.; Gordon, L.G.; Aitken, J.F.; Kimlin, M.G. Lifetime Costs of Surviving Cancer—A Queensland Study (COS-Q): Protocol of a Large Healthcare Data Linkage Study. Int. J. Environ. Res. Public Health 2020, 17, 2831. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082831
Merollini KMD, Gordon LG, Aitken JF, Kimlin MG. Lifetime Costs of Surviving Cancer—A Queensland Study (COS-Q): Protocol of a Large Healthcare Data Linkage Study. International Journal of Environmental Research and Public Health. 2020; 17(8):2831. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082831
Chicago/Turabian StyleMerollini, Katharina M. D., Louisa G. Gordon, Joanne F. Aitken, and Michael G. Kimlin. 2020. "Lifetime Costs of Surviving Cancer—A Queensland Study (COS-Q): Protocol of a Large Healthcare Data Linkage Study" International Journal of Environmental Research and Public Health 17, no. 8: 2831. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082831