A Visual Scan Analysis Protocol for Postural Assessment at School in Young Students

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
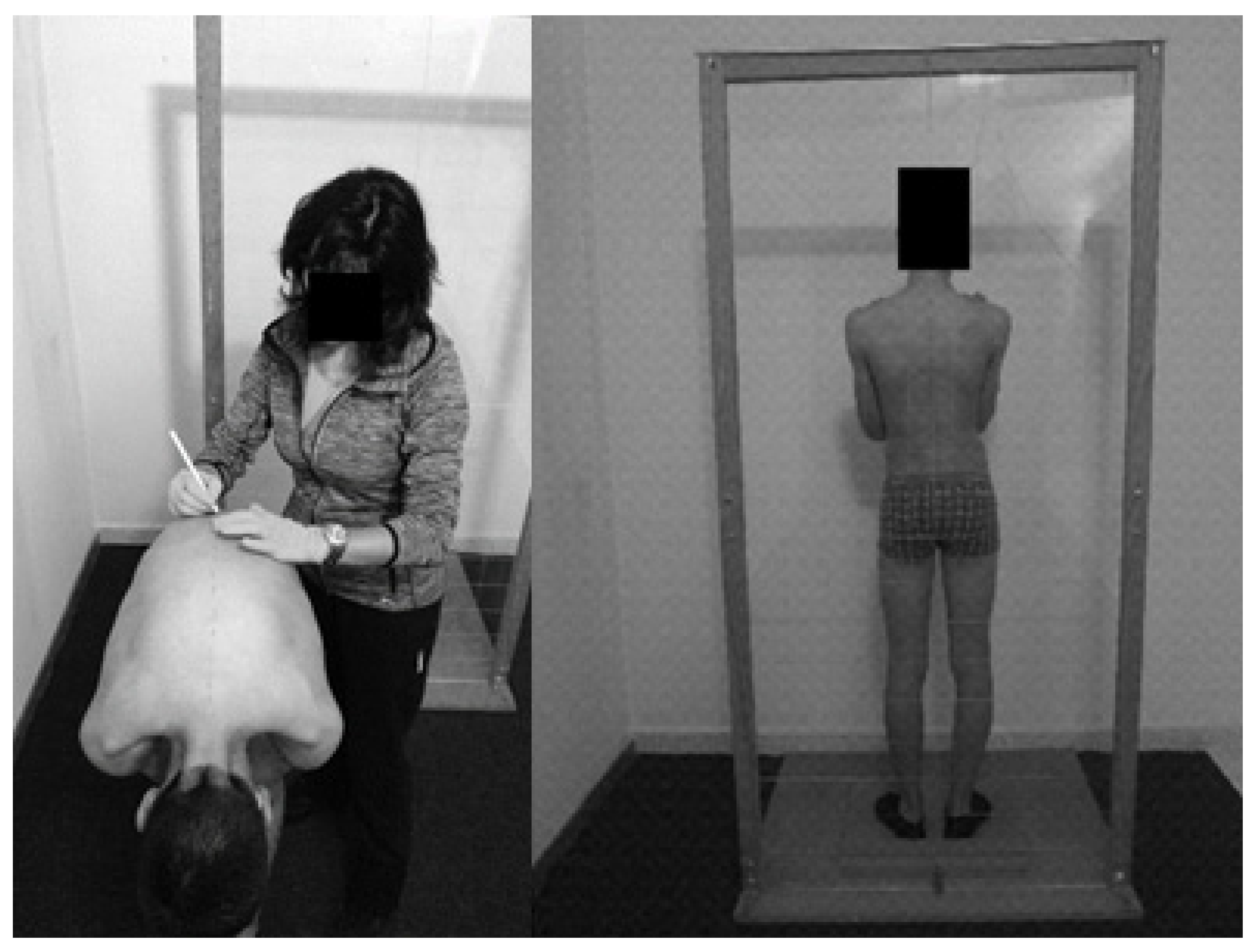
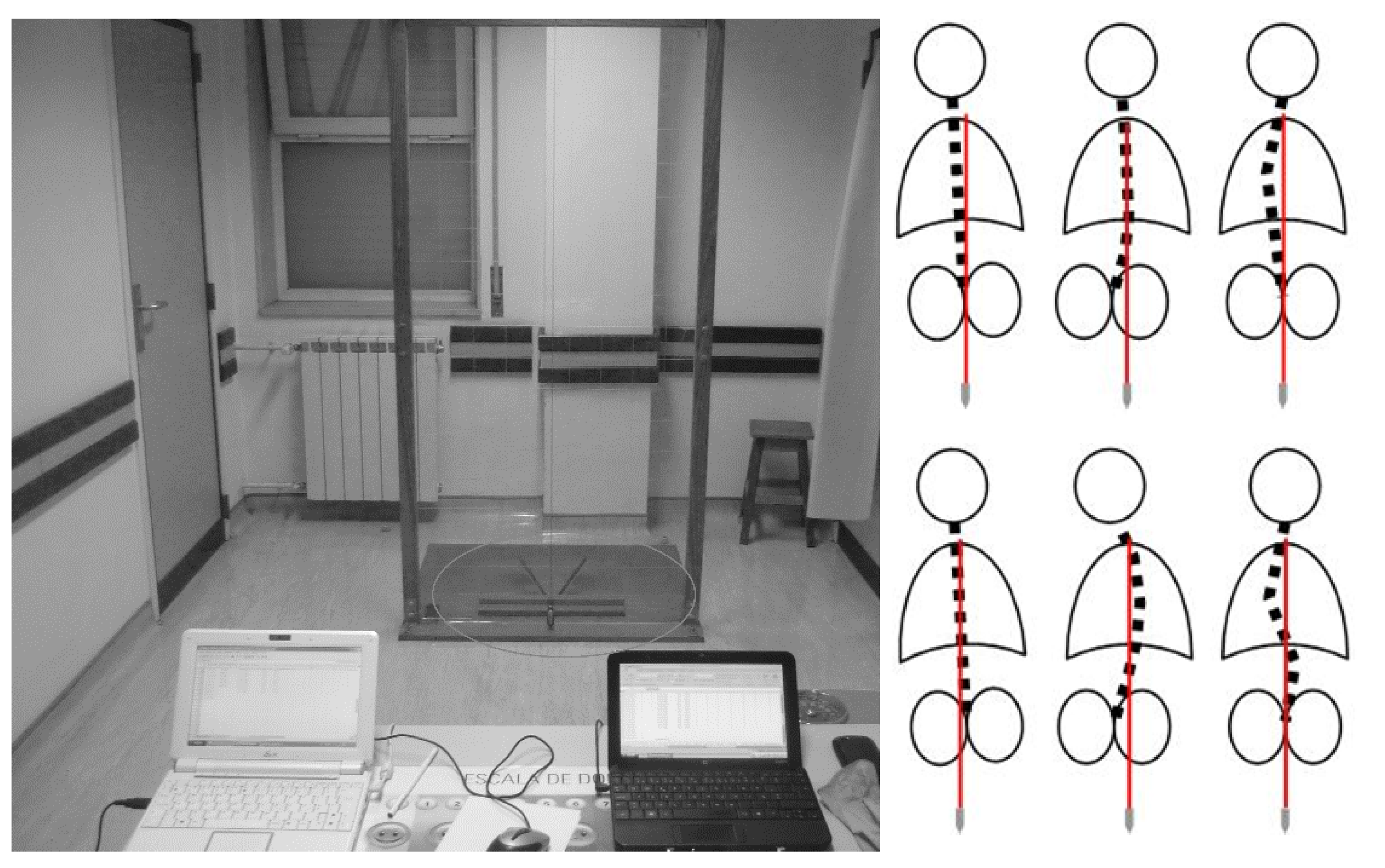
2.2. Visual Scan Method (Field Test)
2.3. X-ray Method (Clinical Test)
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Trigueros, R.; García-Tascón, M.; Gallardo, A.M.; Alías, A.; Aguilar-Parra, J.M. The influence of the teacher’s prosocial skills on the mind wandering, creative intelligence, emotions, and academic performance of secondary students in the area of physical education classes. Int. J. Environ. Res. Public Health 2020, 17, 1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallis, J.F.; McKenzie, T.L.; Beets, M.W.; Beighle, A.; Erwin, H.; Lee, S. Physical education’s role in public health: Steps forward and backward over 20 years and HOPE for the future. Res. Q. Exerc. Sport 2012, 83, 125–135. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, T.L. The preparation of physical educators: A public health perspective. Quest 2007, 59, 345–357. [Google Scholar] [CrossRef]
- Adamczewska, K.; Wiernicka, M.; Malchrowicz-Mośko, E.; Małecka, J.; Lewandowski, J. The angle of trunk rotation in school children: A study from an idiopathic scoliosis screening. Prevalence and optimal age screening value. Int. J. Environ. Res. Public Health 2019, 16, 3426. [Google Scholar] [CrossRef] [Green Version]
- Leonard, A.; Sabina, M. The body posture and its imbalances in children and adolescents. Sci. Mov. Health 2014, 14, 354–359. [Google Scholar]
- Gangnet, N.; Pomero, V.; Dumas, R.; Skalli, W.; Vital, J.M. Variability of the spine and pelvis location with respect to the gravity line: A three-dimensional stereoradiographic study using a force platform. Surg. Radiol. Anat. 2003, 25, 424–433. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Theory and Practical Applications; Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Haddad, J.M.; Rietdyk, S.; Claxton, L.J.; Huber, J. Task-dependent postural control throughout the lifespan. Exerc. Sport Sci. Rev. 2013, 41, 123. [Google Scholar] [CrossRef] [Green Version]
- Calvo-Muñoz, I.; Gómez-Conesa, A.; Sánchez-Meca, J. Prevalence of low back pain in children and adolescents: A meta-analysis. BMC Pediatr. 2013, 13, 14. [Google Scholar] [CrossRef] [Green Version]
- Théroux, J.; Le May, S.; Fortin, C.; Labelle, H. Prevalence and management of back pain in adolescent idiopathic scoliosis patients: A retrospective study. Pain Res. Manag. 2015, 20, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Shehab, D.K.; Al-Jarallah, K.F. Nonspecific low-back pain in Kuwaiti children and adolescents: Associated factors. J. Adolesc. Health 2005, 36, 32–35. [Google Scholar] [CrossRef]
- Watson, K.D.; Papageorgiou, A.C.; Jones, G.T.; Taylor, S.; Symmons, D.P.; Silman, A.J.; Macfarlane, G.J. Low back pain in schoolchildren: Occurrence and characteristics. Pain 2002, 97, 87–92. [Google Scholar] [CrossRef]
- Lowe, T.; Edgar, M.; Margulies, J.; Miller, N.; Raso, V.; Reinker, K.; Rivard, C.H. Etiology of idiopathic scoliosis: Current trends in research. J. Bone Jt. Surg. Am. 2000, 82, 1157–1168. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, H.N.; Barbosa, T.M. The effects of backpack carriage on gait kinematics and kinetics of schoolchildren. Sci. Rep. 2019, 9, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, J.P.; Marques, M.C.; Neiva, H.P.; Esteves, D.; Alonso-Martínez, A.M.; Izquierdo, M.; Ramirez-Campillo, R.; Alvarez, C.; Marinho, D.A. Effects of backpacks on ground reaction forces in children of different ages when walking, running, and jumping. Int. J. Environ. Res. Public Health 2019, 16, 5154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breen, R.; Pyper, S.; Rusk, Y.; Dockrell, S. An investigation of children’s posture and discomfort during computer use. Ergonomics 2007, 50, 1582–1592. [Google Scholar] [CrossRef] [PubMed]
- Dunk, N.M.; Chung, Y.Y.; Compton, D.S.; Callaghan, J.P. The reliability of quantifying upright standing postures as a baseline diagnostic clinical tool. J. Manip. Physiol. Ther. 2004, 27, 91–96. [Google Scholar] [CrossRef]
- Kilinç, F.; Yaman, H.; Atay, E. Investigation of the effects of intensive one-sided and double-sided training drills on the postures of basketball playing children. J. Phys. Ther. Sci. 2009, 21, 23–28. [Google Scholar] [CrossRef] [Green Version]
- Day, G.A.; McPhee, I.B.; Tuffley, J.; Tomlinson, F.; Chaseling, R.; Kellie, S.; Torode, I.; Sherwood, M.; Cutbush, K.; Geddes, A.J.; et al. Idiopathic scoliosis and pineal lesions in Australian children. J. Orthop. Surg. 2007, 15, 327–333. [Google Scholar] [CrossRef] [Green Version]
- Petermann, X.B.; Meereis, E.C.W. Postural body: A systematic review about assessment methods. Man. Ther. Posturol. Rehab. J. 2016, 14, 1–9. [Google Scholar]
- Gracey, P.; Gentaz, R. Trastornos Posturales del eje Corporal. In Manual de Rehabilitación de la Columna Vertebral, 2nd ed.; Liebenson, C., Ed.; Editorial Paidotribo: Barcelona, Spain, 2003; pp. 409–423. [Google Scholar]
- Jeon, K.; Kim, D.I. The association between low body weight and scoliosis among Korean Elementary school students. Int. J. Environ. Res. Public Health 2018, 15, 2613. [Google Scholar] [CrossRef] [Green Version]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Furlanetto, T.S.; Candotti, C.T.; Comerlato, T.; Loss, J.F. Validating a postural evaluation method developed using a Digital Image-based Postural Assessment (DIPA) software. Comput. Methods Programs Biomed. 2012, 108, 203–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, J.; Baraliakos, X.; Golder, W.; Hermann, K.G.; Listing, J.; Brandt, J.; Rudwaleit, M.; Zuehlsdorf, S.; Bollow, M.; Sieper, J.; et al. Analysing chronic spinal changes in ankylosing spondylitis: A systematic comparison of conventional X-rays with magnetic resonance imaging using established and new scoring systems. Ann. Rheum. Dis. 2004, 63, 1046–1055. [Google Scholar] [CrossRef]
- Knott, P.; Pappo, E.; Cameron, M.; de Mauroy, J.C.; Rivard, C.; Kotwicki, T.; Zaina, F.; Wynne, J.; Stikeleather, L.; Bettany-Saltikov, J.; et al. SOSORT 2012 consensus paper: Reducing X-ray exposure in pediatric patients with scoliosis. Scoliosis 2014, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; O’Sullivan, P.; Straker, L. Classification of sagittal thoraco-lumbo-pelvic alignment of the adolescent spine in standing and its relationship to low back pain. Spine 2008, 33, 2101–2107. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, E.A.G.; Duarte, M.; Maldonado, E.P.; Burke, T.N.; Marques, A.P. Postural assessment software (PAS/SAPO): Validation and reliabiliy. Clinics 2010, 65, 675–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piątek, E.; Kuczyński, M.; Ostrowska, B. The effects of active self-correction on postural control in girls with adolescent idiopathic scoliosis: The role of an additional mental task. Int. J. Environ. Res. Public Health 2020, 17, 1640. [Google Scholar] [CrossRef] [Green Version]
- Lafond, D.; Descarreaux, M.; Normandm, M.C.; Harrison, D.E. Postural development in school children: A cross-sectional study. Chiropr. Osteopat. 2007, 15, 1. [Google Scholar] [CrossRef] [Green Version]
- Alves, M.E.; Carneiro, D.N.; Alves, J.; Forte, P.; Duarte, J.A. A noninvasive tool for postural assessment in young students at school: Validation, sensibility, specificity and accuracy. Motricidade 2019, 15, 75–76. [Google Scholar]
- Adobor, R.D.; Rimeslatten, S.; Steen, H.; Brox, J.I. School screening and point prevalence of adolescent idiopathic scoliosis in 4000 Norwegian children aged 12 years. Scoliosis 2011, 6, 23. [Google Scholar] [CrossRef] [Green Version]
- Penha, P.J.; João, S.M.A.; Casarotto, R.A.; Amino, C.J.; Penteado, D.C. Postural assessment of girls between 7 and 10 years of age. Clinics 2005, 60, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, Y.; Mathur, A.K.; Blunt, B.A.; Glüer, C.C.; Will, A.S.; Fuerst, T.P.; Jergas, M.D.; Andriano, K.N.; Cummings, S.R.; Genant, H.K. Dual X-ray absorptiometry quality control: Comparison of visual examination and process-control charts. J. Bone Min. Res. 1996, 11, 626–637. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Postural Diagnosis | Field Test | X-ray |
|---|---|---|
| Alignment | 9 (11.1%) | 10 (12.3%) |
| Misalignment | 72 (88.9%) | 71 (87.7%) |
| X-ray | ||||
|---|---|---|---|---|
| Misalignment | Alignment | Total | ||
| Field test | Alignment | 2 | 70 | 72 |
| Misalignment | 8 | 1 | 9 | |
| Total | 10 | 71 | 81 | |
| Scoliosis Level | Field Test | X-ray |
|---|---|---|
| Non-accentuated | 34 (47.20%) | 32 (44.40%) |
| Scoliosis | 38 (52.80%) | 40 (55.60%) |
| X-ray | ||||
|---|---|---|---|---|
| Non-accentuated | Scoliosis | Total | ||
| Field test | Non-accentuated | 31 | 3 | 34 |
| Scoliosis | 1 | 37 | 38 | |
| Total | 32 | 40 | 81 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alves, M.E.; Marinho, D.A.; Carneiro, D.N.; Alves, J.; Forte, P.; Nevill, A.M.; Morais, J.E. A Visual Scan Analysis Protocol for Postural Assessment at School in Young Students. Int. J. Environ. Res. Public Health 2020, 17, 2915. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082915
Alves ME, Marinho DA, Carneiro DN, Alves J, Forte P, Nevill AM, Morais JE. A Visual Scan Analysis Protocol for Postural Assessment at School in Young Students. International Journal of Environmental Research and Public Health. 2020; 17(8):2915. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082915
Chicago/Turabian StyleAlves, Maria E., Daniel A. Marinho, Duarte N. Carneiro, Jorge Alves, Pedro Forte, Alan M. Nevill, and Jorge E. Morais. 2020. "A Visual Scan Analysis Protocol for Postural Assessment at School in Young Students" International Journal of Environmental Research and Public Health 17, no. 8: 2915. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17082915