Effects of Lifting Method, Safety Shoe Type, and Lifting Frequency on Maximum Acceptable Weight of Lift, Physiological Responses, and Safety Shoes Discomfort Rating



Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Measurement and Instrumentation
2.3.1. Anthropogenic Measurements
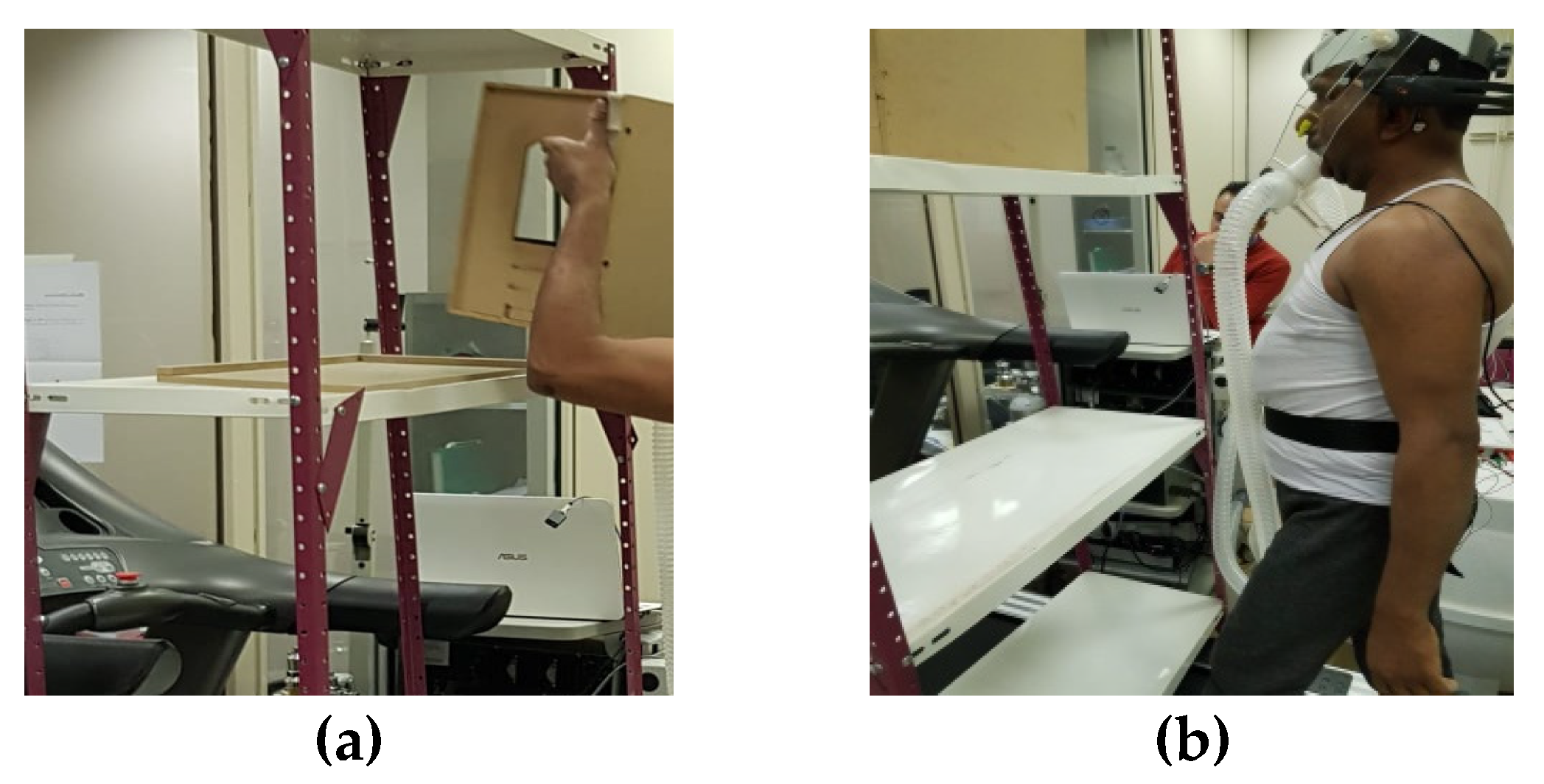
2.3.2. Maximum Acceptable Weight of Lift (MAWL)
2.3.3. Respiration Responses
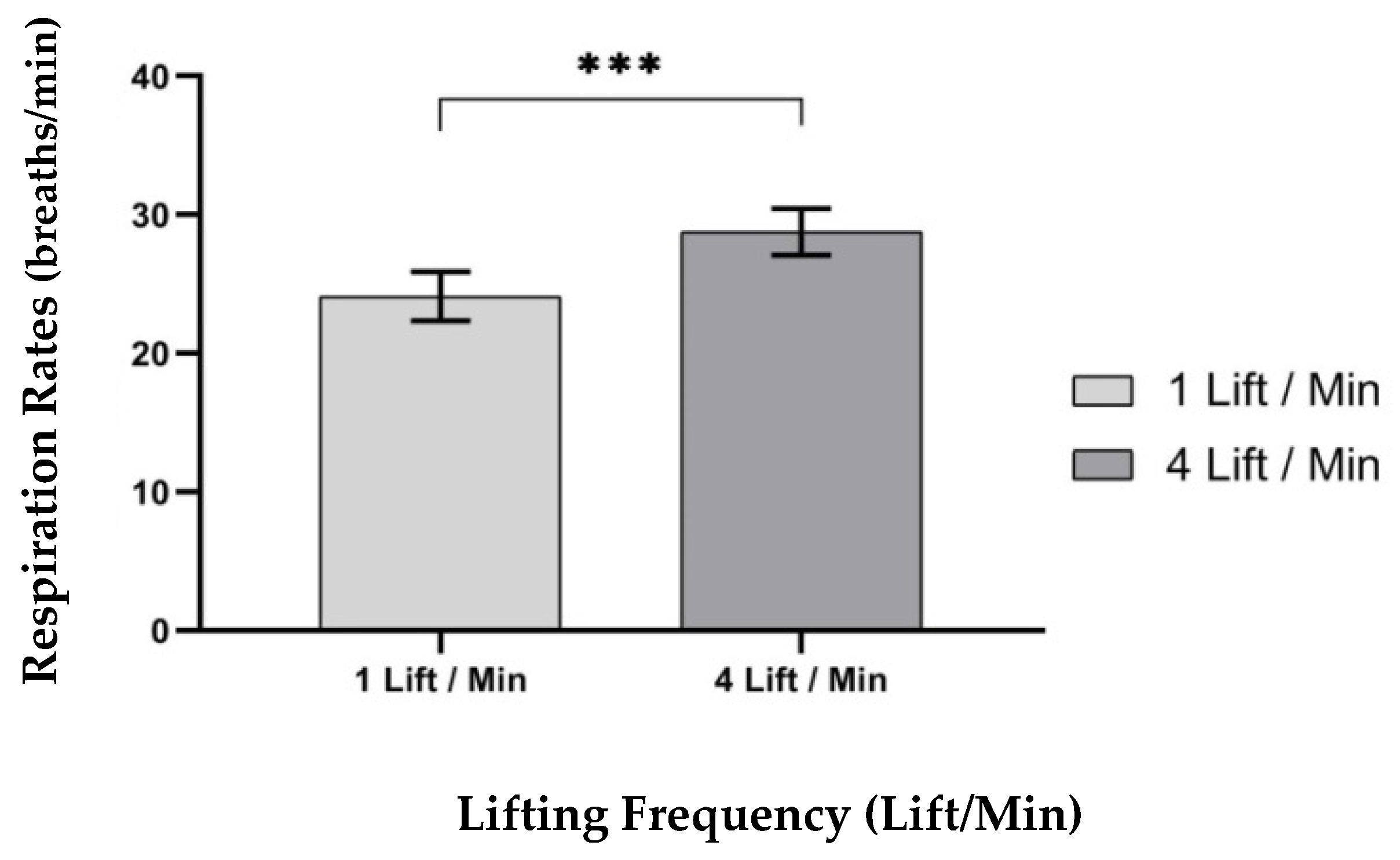
- Respiration Rates (RR (breaths/min)): The respiration rate was the number of breaths taken in 1 min, measured as the number of times the participants’ chest rose in one min.
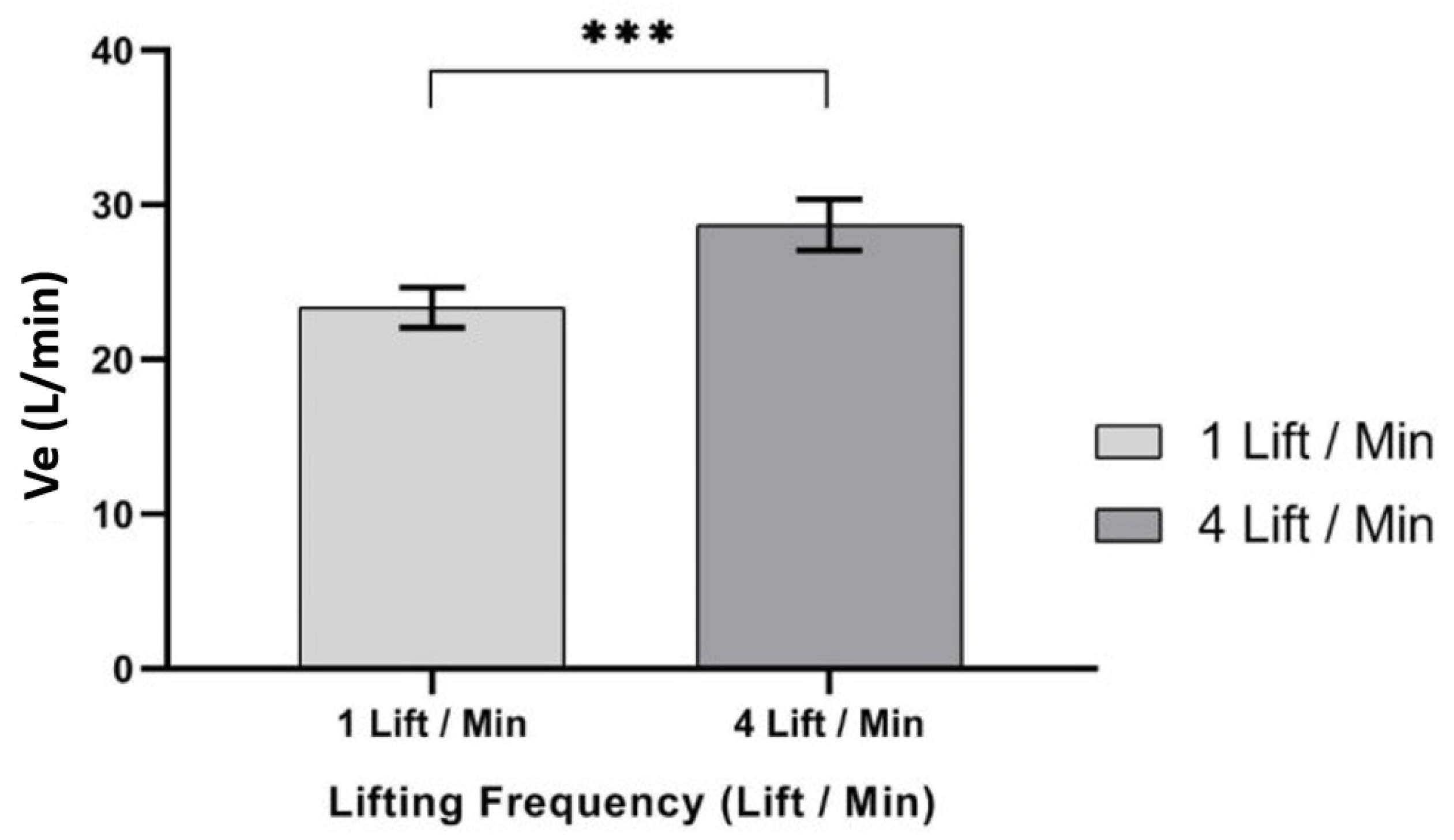
- Minute Ventilation (Ve (L/min)): It was measured as the volume of air a person can exhale in liters during a breathing process, in one min.
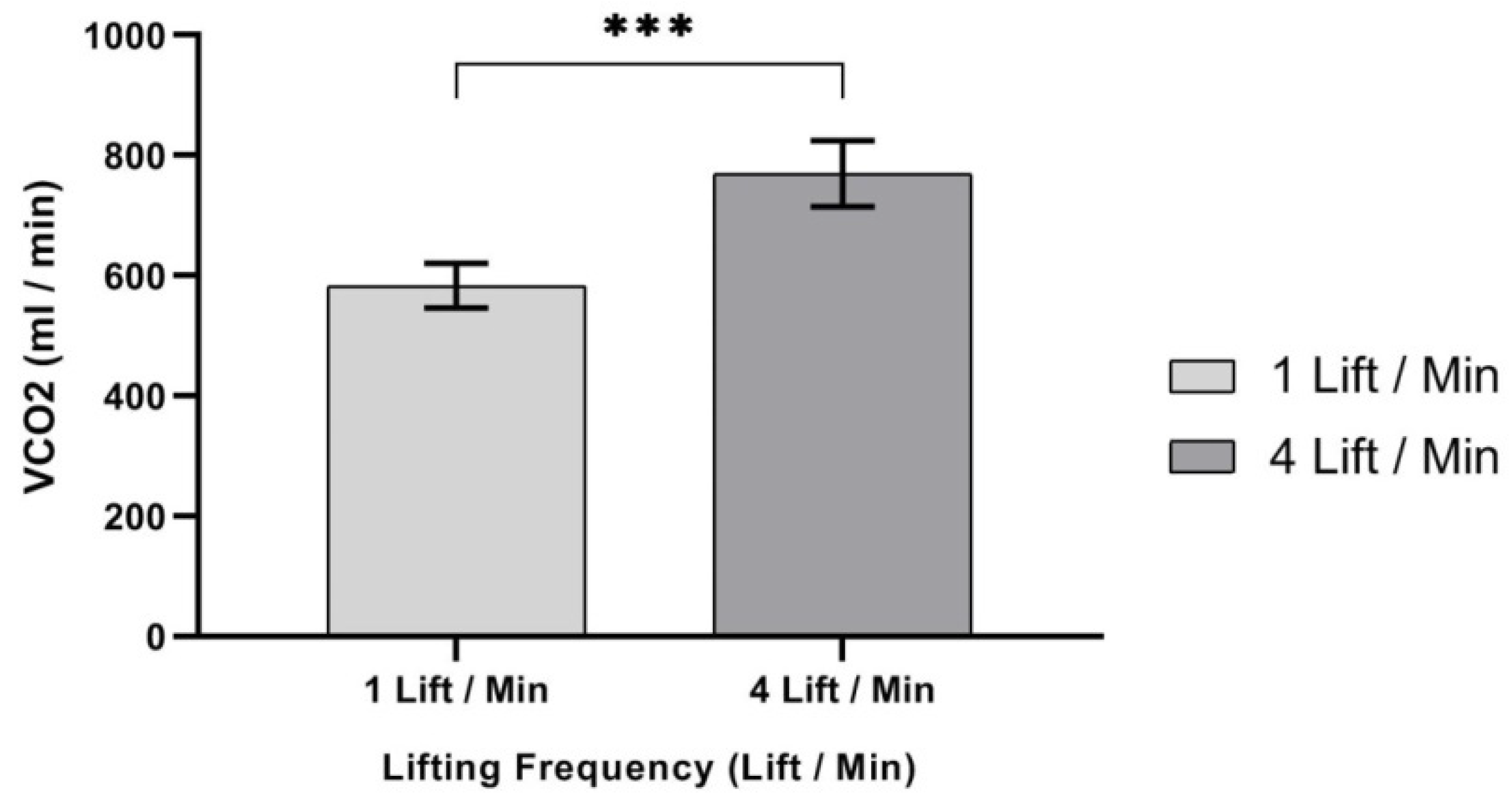
- CO2 production (VCO2 (mL/min)): It was measured as the volume of carbon dioxide that a person breathed out after transporting oxygen through the body.
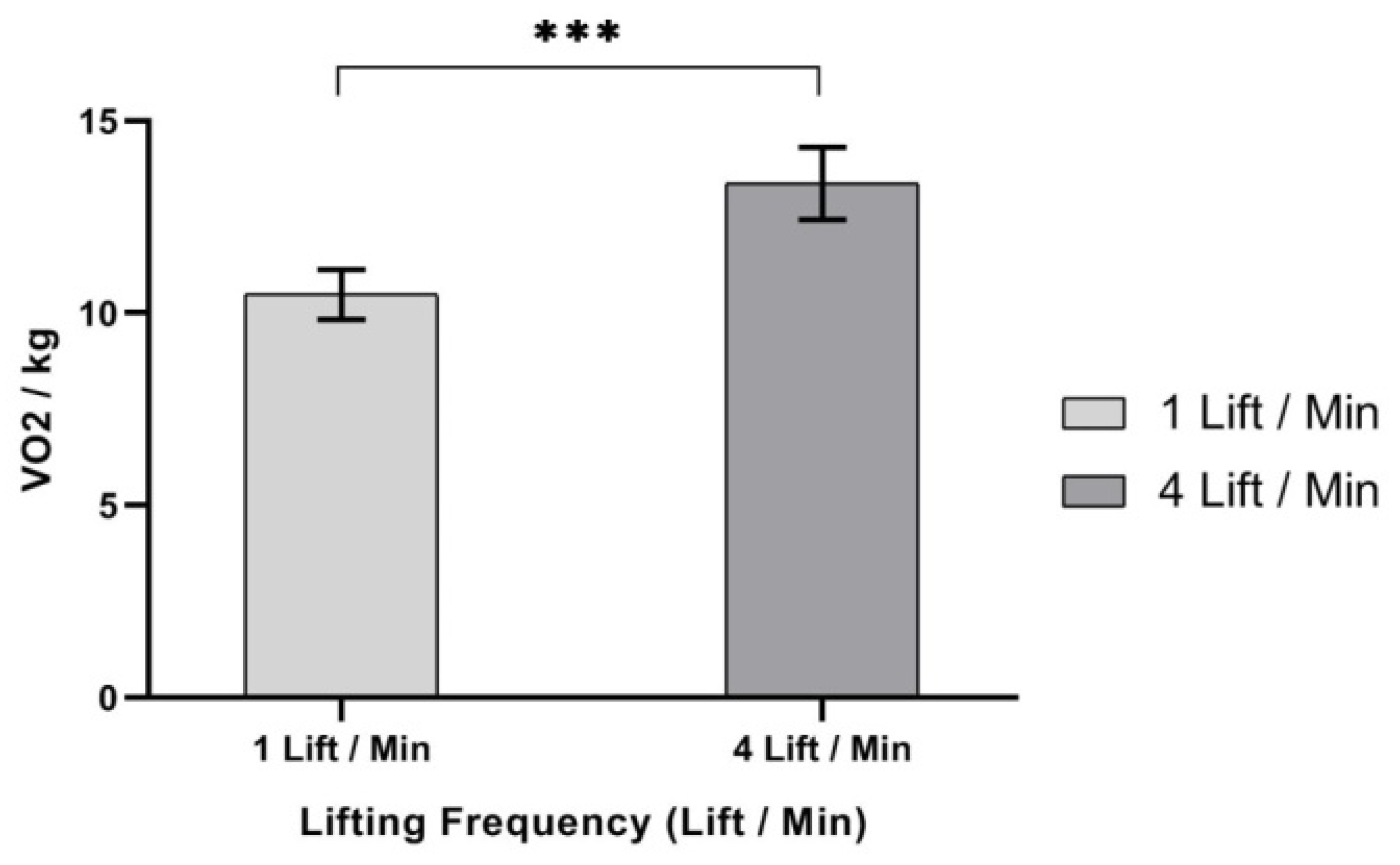
- Oxygen Uptake/body mass (VO2/kg): It was measured as the amount of oxygen consumption a person can utilize during the breathing process in one min, per person’s body mass.
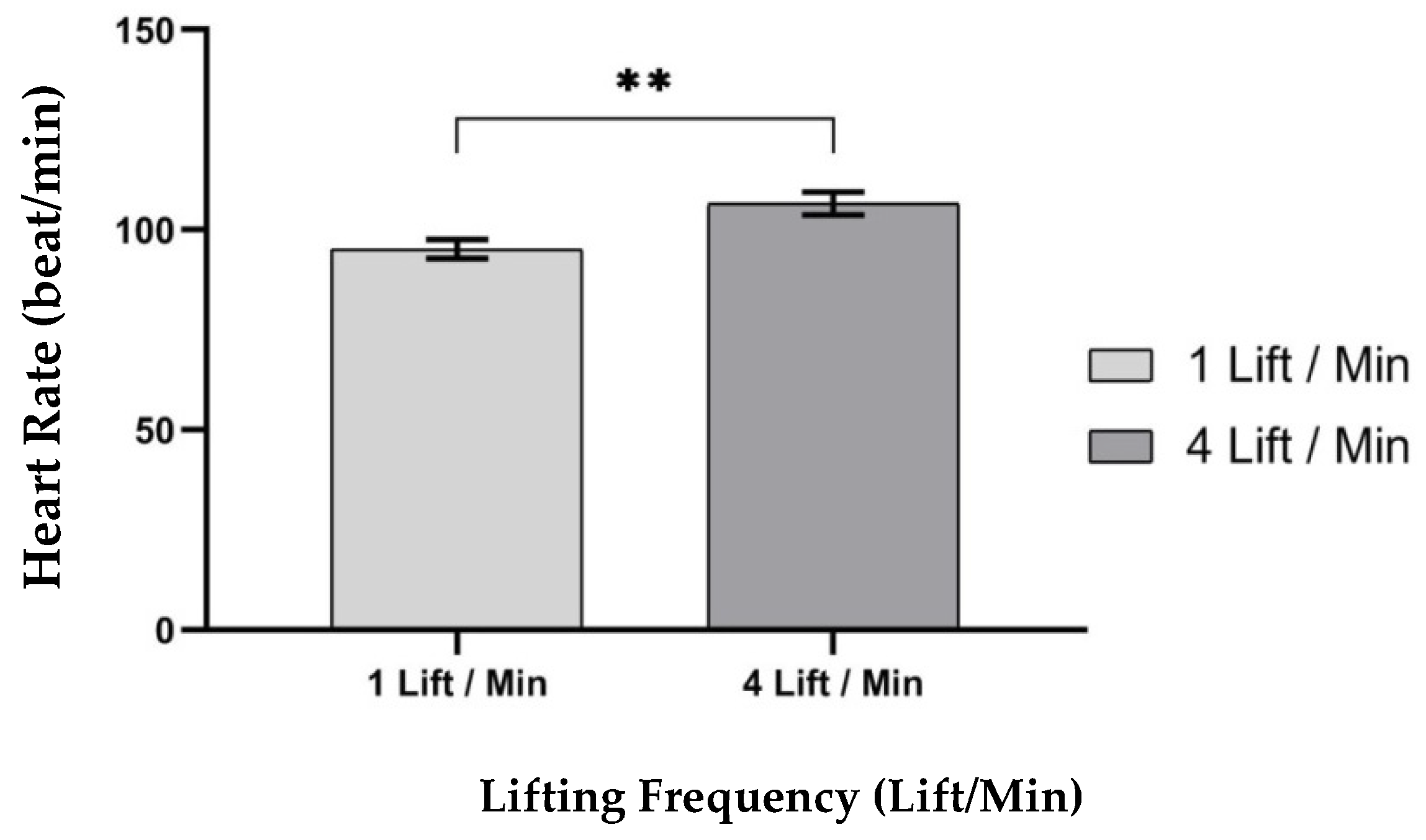
2.3.4. Heart Rates (beats/min)
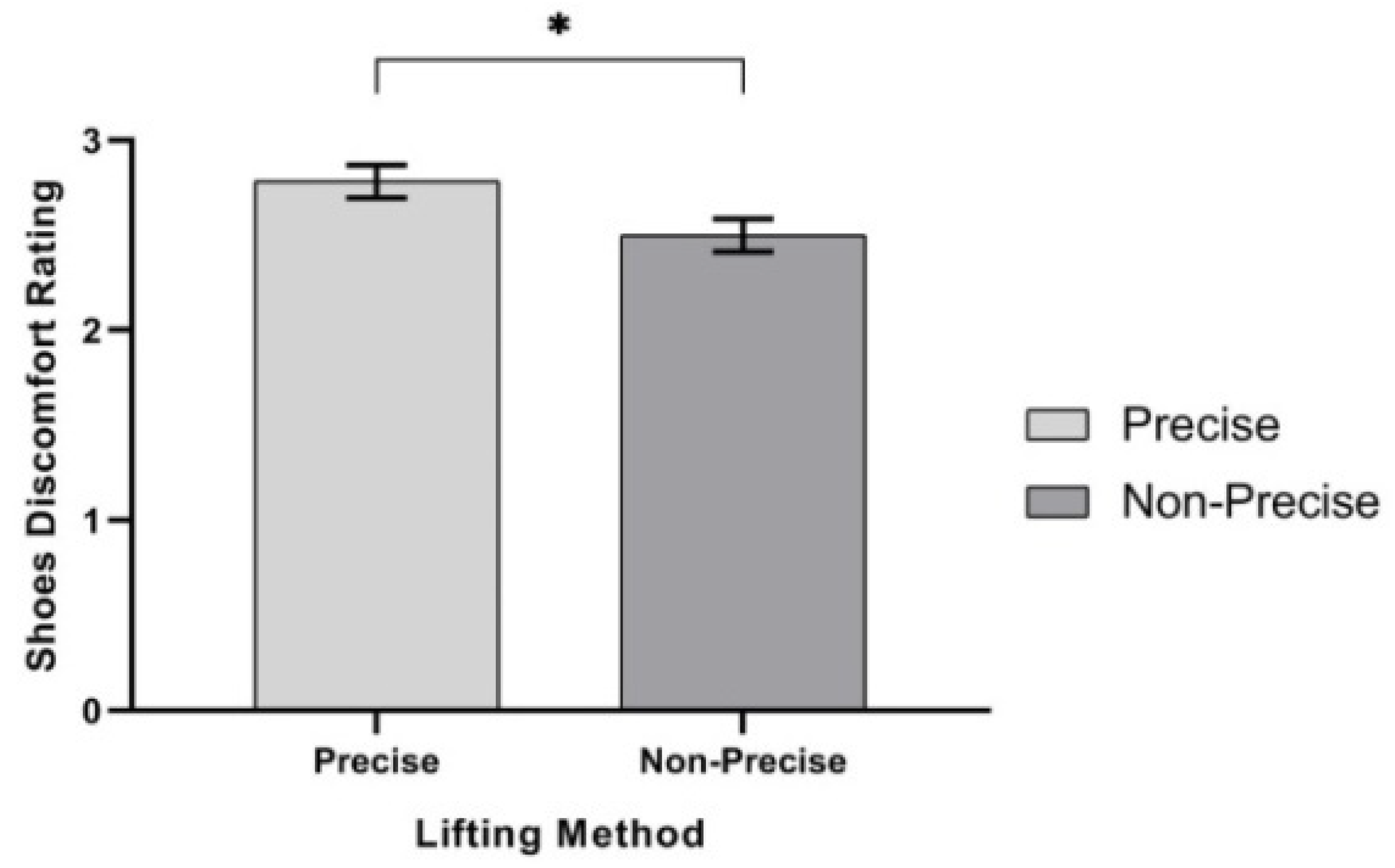
2.3.5. Safety Shoes Discomfort Rating (SSDR)
2.4. Experimental Variables
2.4.1. Lifting Method
2.4.2. Lifting Frequency
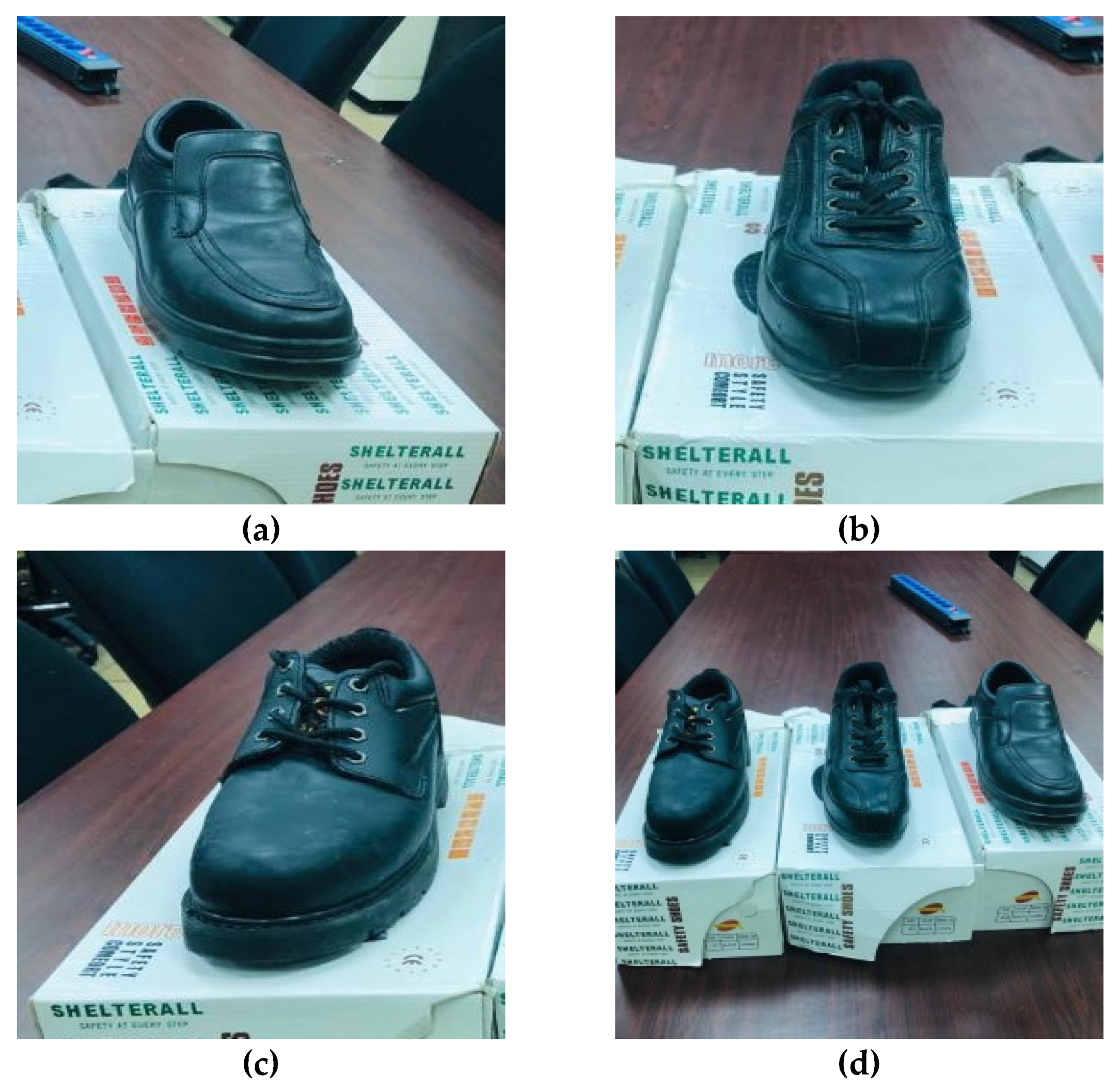
2.4.3. Safety Shoe Types
2.5. Experimental Design
2.6. Experimental Procedures
3. Results
3.1. MAWL
3.2. Resperation Responses
3.2.1. Respiration Rates
3.2.2. Minute Ventilation (Ve (L/min))
3.2.3. VCO2 (mL/min)
3.2.4. VO2/kg
3.3. Heart Rate
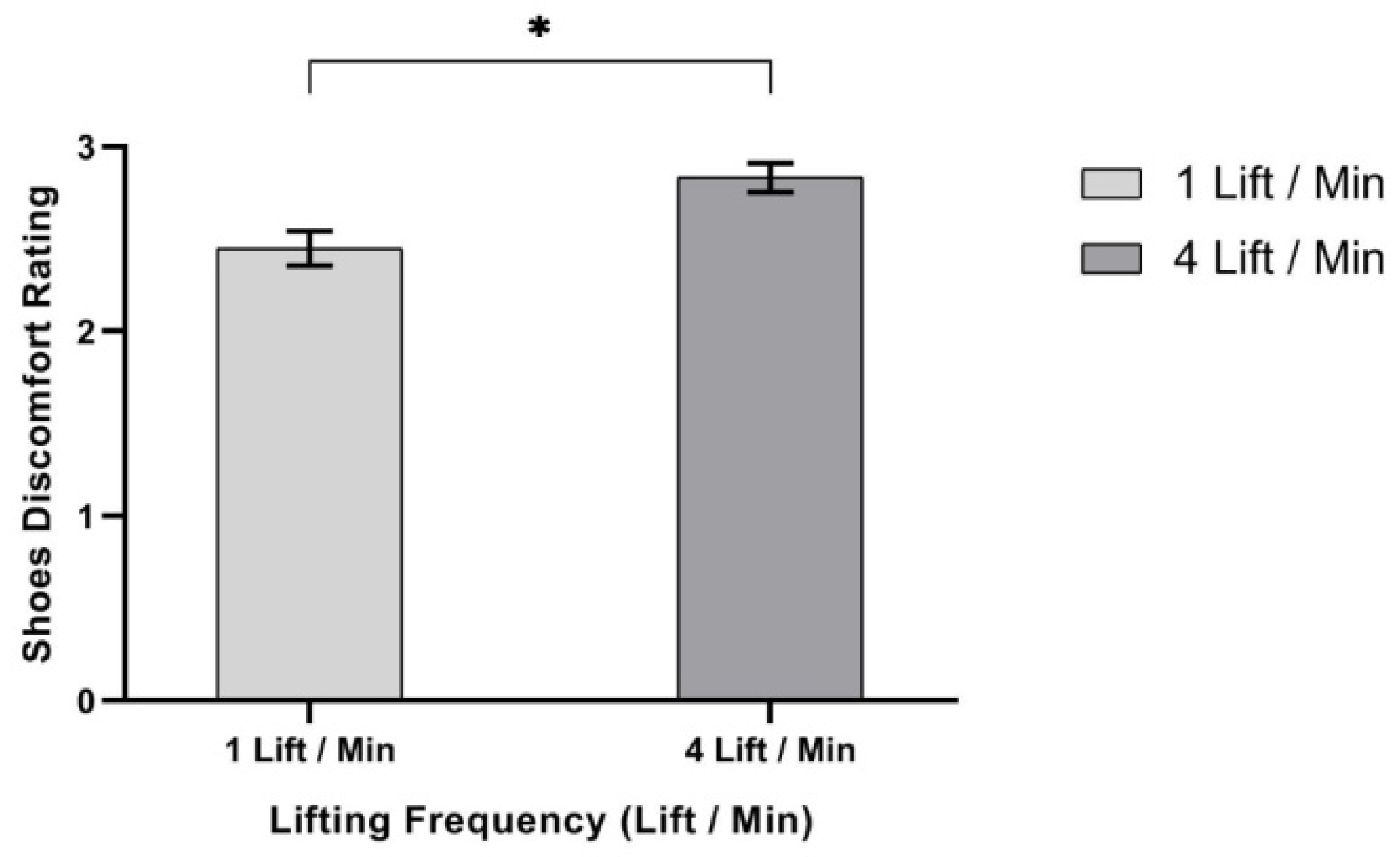
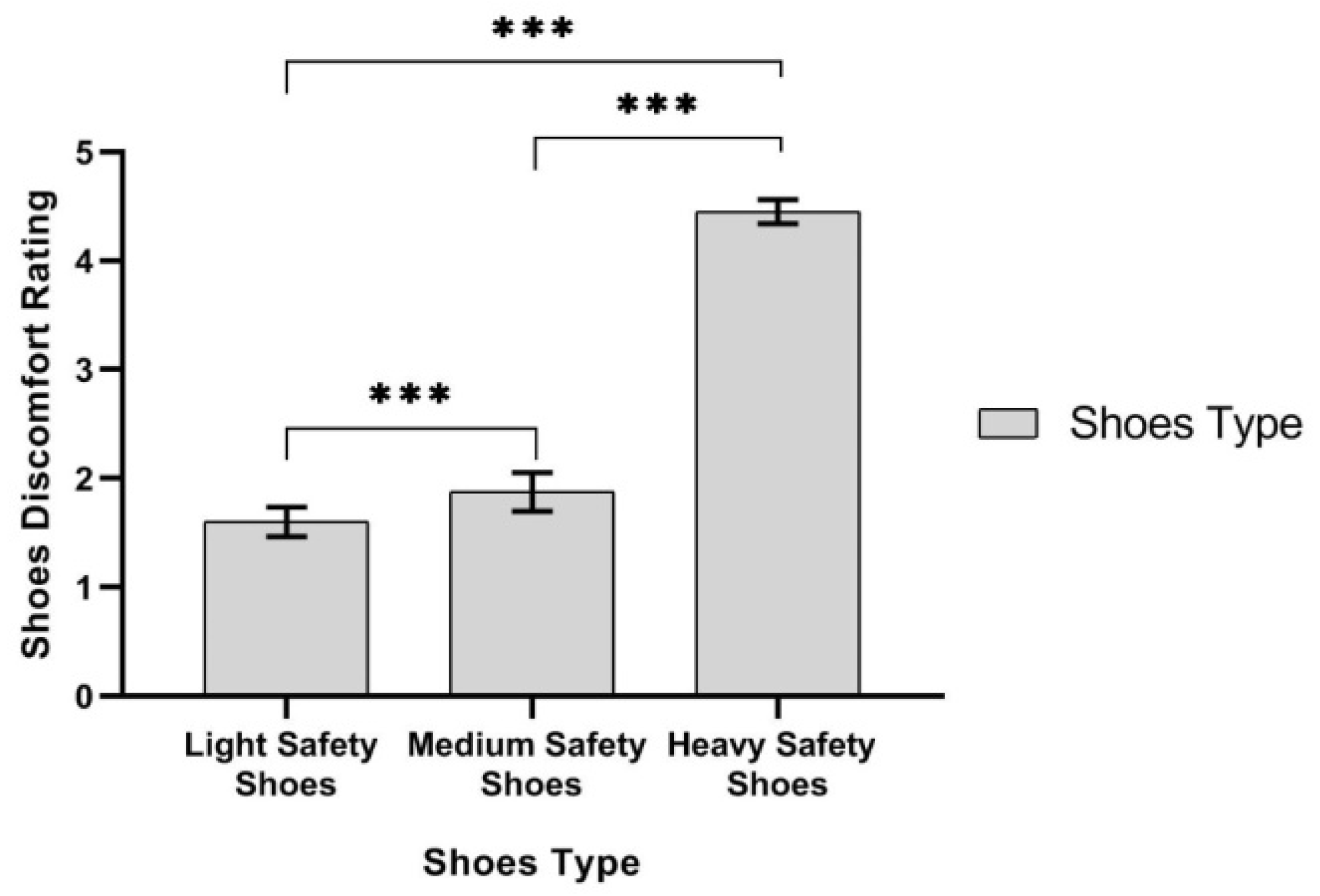
3.4. Safety Shoes Discomfort Rating (SSDR)
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fredericks, T.K.; Kumar, A.R.; Karim, S. An ergonomic evaluation of a manual metal pouring operation. Int. J. Ind. Ergon. 2008, 38, 182–192. [Google Scholar] [CrossRef]
- Triano, J. Manual Material Handling to Prevent Back Injury. Spine-Health. 2006. Available online: https://www.spine-health.com/wellness/ergonomics/manual-material-handling-prevent-back-injury (accessed on 10 October 2019).
- Turner, A.J.; Swain, J.C.; Mcwhirter, K.L.; Knight, A.C.; Carruth, D.W.; Chander, H. Impact of occupational footwear and workload on lower extremity muscular exertion. Int. J. Exerc. Sci. 2018, 11, 331–341. [Google Scholar]
- Li, K.W.; Wen-Sheng, C. Isometric arm strength and subjective rating of upper limb fatigue in two-handed carrying tasks. PLoS ONE 2015, 10, e0119550. [Google Scholar] [CrossRef] [PubMed]
- Ochsmann, E.; Noll, U.; Ellegast, R.; Hermanns, I.; Kraus, T. Influence of different safety shoes on gait and plantar pressure: A standardized examination of workers in the automotive industry. J. Occup. Health 2016, 58, 404–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, K.G.; Marras, W.S.; Heaney, C.A.; Waters, T.R.; Gupta, P. The impact of mental processing and pacing on spine loading 2002 volvo award in biomechanics. Spine 2002, 27, 2645–2653. Available online: https://pdfs.semanticscholar.org/abab/15313dc7f5685ecd7c8ba3af99e2b7d3cb87.pdf (accessed on 22 May 2019). [CrossRef]
- Shahu, R.S. The NIOSH lifting equation for manual lifting and its applications. J. Ergon. 2016, 6. [Google Scholar] [CrossRef]
- United States Department of Labor. Million Nonfatal Workplace Injuries and Illnesses Resulted in Days Away from Work in 2017: The Economics Daily: U.S. Bureau of Labor Statistics; Bureau of Labor Statistics—Government Agency: Washington, DC, USA, 2018.
- Li, K.W.; Yu, R.; Gao, Y.; Maikala, R.V.; Tsai, H. Physiological and perceptual responses in male Chinese workers performing combined manual materials handling tasks. Int. J. Ind. Ergon. 2009, 39, 422–427. [Google Scholar] [CrossRef]
- The National Institute for Occupational Safety and Health (NIOSH). Ergonomic Guidelines for Manual Material Handling; NIOSH: Cincinnati, OH, USA, 2007. [CrossRef]
- Calzavara, M.; Glock, C.H.; Grosse, E.H.; Persona, A.; Sgarbossa, F. Analysis of economic and ergonomic performance measures of different rack layouts in an order picking warehouse. Comput. Ind. Eng. 2017, 111, 527–536. [Google Scholar] [CrossRef]
- Erdem, M.; Boran, F.E.; Akay, D. Classification of risks of occupational low back disorders with support vector machines. Hum. Factor Ergon. Manuf. 2016, 26, 550–558. [Google Scholar] [CrossRef]
- Harari, Y.; Riemer, R.; Bechar, A. Factors determining workers’ pace while conducting continuous sequential lifting, carrying, and lowering tasks. Appl. Ergon. 2018, 67, 61–70. [Google Scholar] [CrossRef]
- Nordander, C.; Hansson, G.; Ohlsson, K.; Arvidsson, I.; Balogh, I.; Strömberg, U.; Rittner, R.; Skerfving, S. Exposure–response relationships for work-related neck and shoulder musculoskeletal disorders—Analyses of pooled uniform data sets. Appl. Ergon. 2016, 55, 70–84. [Google Scholar] [CrossRef] [PubMed]
- European Agency for Safety and Health at Work. OSH in Figures: Work-Related Musculoskeletal Disorders in the EU-Facts and Figures; European Agency for Safety and Health at Work: Bilbao, Spain, 2010. [Google Scholar] [CrossRef]
- Chaffin, D.B. Manual materials handling and the biomechanical basis for prevention of low-back pain in industry—An overview. Am. Ind. Hyg. Assoc. J. 1987, 48, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Chaffin, D.B.; Park, K.S. A longitudinal study of low-back pain as associated with occupational weight lifting factors. Am. Ind. Hyg. Assoc. J. 1973, 34, 513–525. [Google Scholar] [CrossRef] [PubMed]
- Christie, C.J.; Wolfe, A. Impact of ceiling restriction and lifting barriers on selected physiological and perceptual responses. Work 2011, 38, 225–234. [Google Scholar] [CrossRef]
- Gallagher, S.; Christopher, A.; Hamrick, K.M.; Cornelius, M.R. The effects of restricted workspace on lumbar spine loading. Occup. Ergon. 2001, 2, 201–213. [Google Scholar]
- Waters, T.R.; Putz-Anderson, V.; Garg, A.; Fine, L.J. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993, 36, 749–776. [Google Scholar] [CrossRef]
- Mozrall, J.R.; Drury, C.G.; Sharit, J.; Cerny, F. The effects of whole-body restriction on task performance. Ergonomics 2000, 43, 1805–1823. [Google Scholar] [CrossRef]
- Mital, A.; Wang, L. Effects on load handling of restricted and unrestricted shelf opening clearances. Ergonomics 1989, 32, 39–49. [Google Scholar] [CrossRef]
- Ayoub, M.M.; Mital, A.; Bakken, G.M.; Asfour, S.S.; Bethea, N.J. Development of strength and capacity norms for manual materials handling activities: The state of the art. Hum. Factors 1980, 22, 271–283. [Google Scholar] [CrossRef]
- Mital, A.; Fard, H.F. Psychophysical and physiological responses to lifting symmetrical and asymmetrical loads symmetrically and asymmetrically. Ergonomics 1986, 29, 1263–1272. [Google Scholar] [CrossRef]
- Ayoub, M.M.; Betliea, N.J.; Asfour, S.; Calisto, G.; Grasley, C. Review of the Strength and Capacity Data for Manual Material Handling Activities; Tech. Report; Institute for Biotechnology, Texas Tech University: Lubbock, TX, USA, 1980. [Google Scholar]
- Dempsey, P.G.; Ayoub, M.M. The role of power in predicting lifting capacity. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, Philadelphia, PA, USA, 2–6 September 1996; Volume 40, pp. 609–613. [Google Scholar] [CrossRef]
- Snook, S.H.; Ciriello, V.M. Maximum Weights and Work Loads Acceptable to Female Workers. Occup. Health Nurs. 1974, 22, 11–20. [Google Scholar] [PubMed]
- Wheeler, D.L.; Graves, J.E.; Miller, G.J.; Connor, P.O.; MacMillan, M. Functional assessment for prediction of lifting capacity. Spine 1994, 19, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.; Saxena, U. Effects of lifting frequency and technique on physical fatigue with special reference to psychophysical methodology and metabolic rate. Am. Ind. Hyg. Assoc. J. 1979, 40, 894–903. [Google Scholar] [CrossRef] [PubMed]
- Harbin, G.L.; Shenoy, C.; Garcia, A.; Olson, J.C. Shoulder injury reduction with pos-offer testing. Work 2011, 39, 113–123. [Google Scholar] [CrossRef] [Green Version]
- Snook, S.H.; Campanelli, R.A.; Hart, J.W. A study of three preventive approaches to low back injury. J. Occup. Med. 1978, 20, 478–481. [Google Scholar] [CrossRef]
- Herrin, G.D.; Jaraiedi, M.; Anderson, C.K. Prediction of overexertion injuries using biomechanical and psychophysical models. Am. Ind. Hyg. Assoc. J. 1986, 47, 322–330. [Google Scholar] [CrossRef]
- Chaffin, D.B.; Herrin, G.D.; Keyserling, W.M. Preemployment strength testing: An updated position. J. Occup. Med. 1978, 20, 403–408. [Google Scholar]
- Poulsen, E. Prediction of maximum loads in lifting from measurement of back muscle strength. Prog. Phys. Ther. 1970, 1, 146–149. [Google Scholar]
- Pinder, A.D.J.; Boocock, M.G. Prediction of the maximum acceptable weight of lift from the frequency of lift. Int. J. Ind. Ergon. 2014, 44, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Knipfer, E.R. Predictive Models for the Maximum Acceptable Weight of Lift. Ph.D. Thesis, Texas Tech University, Lubbock, TX, USA, 1974. [Google Scholar]
- McHugh, C.; Gibson, L. Pre-placement screenings: An exploratory study of their use in a sample of New South Wales workplaces. Work 2011, 40, 187–194. [Google Scholar] [CrossRef]
- Al-Ashaik, R.A.; Ramadan, M.Z.; Al-Saleh, K.S.; Khalaf, T.M. Effect of safety shoes type, lifting frequency, and ambient temperature on subject’s MAWL and physiological responses. Int. J. Ind. Ergon. 2015, 50, 43–51. [Google Scholar] [CrossRef]
- Ciriello, V.M.; Snook, S.H.; Hughes, G.J. Further studies of psychophysically determined maximum acceptable weights and forces. Hum. Factors 1993, 35, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, M.M.; Dryden, R.D.; Knipfer, R.E. Psychophysical based models for the prediction of lifting capacity of the industrial worker. SAE Trans. 1976, 85, 276–286. [Google Scholar] [CrossRef]
- Snook, S.H.; Ciriello, V.M. The design of manual handling tasks: Revised tables of maximum acceptable weights and forces. Ergonomics 1991, 34, 1197–1213. [Google Scholar] [CrossRef] [PubMed]
- Wu, S. Maximum acceptable weights for asymmetric lifting of Chinese females. Appl. Ergon. 2003, 34, 215–224. [Google Scholar] [CrossRef]
- Lee, T. Psychophysically determined asymmetrical lifting capabilities for different frequencies and containers. Ind. Health 2005, 43, 337–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maiti, R.; Ray, G.G. Determination of maximum acceptable weight of lift by adult indian female workers. Int. J. Ind. Ergon. 2004, 34, 483–495. [Google Scholar] [CrossRef]
- Singh, N.; Belokar, R.M.; Walia, R.S. Physiological evaluation of manual lifting tasks on Indian male workers. Int. J. Eng. Adv. Tech. 2012, 2, 8–16. [Google Scholar]
- Fox, R.R.; Smith, J.L. A psychophysical study of high-frequency arm lifting. Int. J. Ind. Ergon. 2014, 44, 238–245. [Google Scholar] [CrossRef]
- Dempsey, P. A critical review of biomechanical, epidemiological, physiological and psychophysical criteria for designing manual materials handling tasks. Ergonomics 1998, 41, 73–88. [Google Scholar] [CrossRef]
- Hamilton, B.J.; Richard, B.C. A work physiology study of the relative effects of pace and weight in a carton handling task. AIIE Trans. 1969, 1, 106–110. [Google Scholar] [CrossRef]
- Garg, A.; Chaffin, D.; Herrin, G.D. Prediction of metabolic rates for manual materials handling jobs. Am. Ind. Hyg. Assoc. J. 1978, 39, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Jbrgensen, K.; Poulsen, E. Physiological problems in repetitive lifting with special reference to tolerance limits to the maximum lifting frequency. Ergonomics 1974, 17, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Asfour, S.S. Energy Cost Prediction Models for Manual Lifting and Lowering Tasks. Ph.D. Thesis, Texas Tech University, Lubbock, TX, USA, 1980. Available online: https://ttu-ir.tdl.org/handle/2346/17402 (accessed on 17 June 2017).
- Simpson, K.M.; Bridget, J.M.; Steele, J.R. Effect of load mass on posture, heart rate and subjective responses of recreational female hikers to prolonged load carriage. Appl. Ergon. 2011, 42, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Lorenzi-Filho, G.; Dajani, H.R.; Leung, R.S.T.; Floras, J.S.; Bradley, T.D. Entrainment of blood pressure and heart rate oscillations by periodic breathing. Am. J. Respir. Crit Care Med. 1999, 159, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Ghaleb, A.M.; Ramadan, M.Z.; Badwelan, A.; Saad Aljaloud, K. Effect of ambient oxygen content, safety shoe type, and lifting frequency on subject’s MAWL and physiological responses. Int. J. Environ. Res. Public Health 2019, 16, 4172. [Google Scholar] [CrossRef] [Green Version]
- Ramadan, M.Z.; Ghaleb, A.M.; Ragab, A.E. Using electroencephalography (EEG) power responses to investigate the effects of ambient oxygen content, safety shoe type, and lifting frequency on the worker’s activities. BioMed Res. Int. 2020, 2020, 7956037. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- NASA. Anthropometric Source Book, Volume I. Anthropometry for Designers; Anthropology Research Project Staff, NASA Reference Publication 1024; NASA: Houston, TX, USA, 1978.
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- Ramadan, M.Z. Effects of Task and Environment-Related Variables on Individuals’ Lifting Capabilities While Wearing Protective Clothing. Ph.D. Thesis, West Virgiba University, Morgantown, WV, USA, 1988. [Google Scholar]
- Hafez, H.A.; Ayoub, M.M. A psychophysical study of manual lifting in hot environments. Int. J. Ind. Ergon. 1991, 7, 303–309. [Google Scholar] [CrossRef]
- Chen, F.; Aghazadeh, F.; Lee, K.S. Prediction of the maximum acceptable weight of symmetrical and asymmetrical lift using direct estimation method. Ergonomics 1992, 35, 755–768. [Google Scholar] [CrossRef]
- Mital, A. Maximum weights of lift acceptable to male and female industrial workers for extended work shifts. Ergonomics 1984, 27, 1115–1126. [Google Scholar] [CrossRef]
- Treadmill. Available online: http://www.olympiafitnessplanet.com/commercial-treadmill.html (accessed on 10 October 2016).
- Mills, K.; Peter, B.; Vicenzino, B. Identifying clinically meaningful tools for measuring comfort perception of footwear. Med. Sci. Sport Exerc. 2010, 42, 1966–1971. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.C.; Hong, W.H.; Chiu, M.C. Comparisons with subjective and objective indexes of lifting risk among different combinations of lifting weight and frequency. J. Ambient Intell. Humaniz. Compt. 2018. [Google Scholar] [CrossRef]
- Alabdullatif, A. Impact of Lighting on Human Biomechanical Response During Lifting in Confined Spaces. Ph.D. Thesis, University of Cincinnati, Cincinnati, OH, USA, 2016. [Google Scholar]
- Stambolian, D.B. Biomechanical Analysis of Accurately and Carefully Placing an Aerospace Avionics Box in Restricted Space. Ph.D. Thesis, University of Miami, Coral Gables, FL, USA, 2018. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurement | Light Safety Shoes | Medium Safety Shoes | Heavy Safety Shoes |
|---|---|---|---|
| Upper | Full Leather with Double Density PU Sole | Genuine Full Leather with Double Density PU Sole | Waxy Full Grain Leather |
| Linings | Cambrele | Cambrele | Cambrele Woven |
| Tongue | … | Padded | Padded |
| Lacing | … | Through 4 Pairs Eyelets | Through 4 Pairs Eyelets |
| Collar | Padded | Padded | Padded |
| Toe Caps | Steel | Steel (Toe Cap) | Steel (Toe Cap) |
| Sole | Rubber | Polyurethane Molded | Polyurethane |
| Innersole | Full Sock | Full Sock | Full Sock |
| Cut | Low Cut | Low Cut | High Cut |
| Additional | … | … | Steel Plate |
| Weight | 0.9 kg | 1.05 kg | 1.45 kg |
| Source | SS | DF | MS | F-Value | p-Value | Partial Eta Squared |
|---|---|---|---|---|---|---|
| LM | 134.408 | 1 | 134.408 | 189.357 | 0.000 | 0.955 |
| Error | 6.388 | 9 | 0.710 | |||
| LF | 222.496 | 1 | 222.496 | 284.832 | 0.000 | 0.969 |
| Error | 7.030 | 9 | 0.781 | |||
| ST | 6.912 | 2 | 3.456 | 4.170 | 0.032 | 0.317 |
| Error | 14.918 | 18 | 0.829 |
| Source | SS | DF | MS | F-Value | p-Value | Partial Eta Squared |
|---|---|---|---|---|---|---|
| LF | 649.605 | 1 | 649.605 | 43.530 | 0.000 | 0.829 |
| Error | 134.310 | 9 | 14.923 |
| Source | SS | DF | MS | F-Value | p-Value | Partial Eta Squared |
|---|---|---|---|---|---|---|
| LF | 853.653 | 1 | 853.653 | 67.861 | 0.000 | 0.883 |
| Error | 113.215 | 9 | 12.579 |
| Source (Variables) | SS | DF | MS | F-Value | p-Value | Partial Eta Squared |
|---|---|---|---|---|---|---|
| LF | 1041731.907 | 1 | 1041731.907 | 60.375 | 0.000 | 0.870 |
| Error | 155289.517 | 9 | 17254.391 |
| Source (Variables) | SS | DF | MS | F-Value | p-Value | Partial Eta Squared |
|---|---|---|---|---|---|---|
| LF | 250.765 | 1 | 250.765 | 52.163 | 0.000 | 0.853 |
| Error | 43.266 | 9 | 4.807 |
| Source | SS | DF | MS | F-Value | p-Value | Partial Eta Squared |
|---|---|---|---|---|---|---|
| LF | 3514.622 | 1 | 3514.622 | 16.664 | 0.004 | 0.676 |
| Error | 1687.280 | 8 | 210.910 |
| Source | SS | DF | MS | F-Value | p-Value | Partial Eta Squared |
|---|---|---|---|---|---|---|
| LM | 2.408 | 1 | 2.408 | 5.898 | 0.038 | 0.396 |
| Error | 3.675 | 9 | 0.408 | |||
| LF | 4.408 | 1 | 4.408 | 10.796 | 0.009 | 0.545 |
| Error | 3.675 | 9 | 0.408 | |||
| ST | 197.717 | 2 | 98.858 | 100.063 | 0.000 | 0.917 |
| Error | 17.783 | 18 | 0.988 |
| Source | Present Study | Ghaleb et al. [54] | Al Ashaik [38] | Singh et al. [45] | Ramadan [59] | Hafez [60] |
|---|---|---|---|---|---|---|
| 1 lift/min | 95.17 | 99.98 | 90.40 | 90.80 | 89.60 | 89.90 |
| 4 lifts/min | 106.58 | 119.79 | - | - | - | - |
| 5 lifts/min | - | - | 100.20 | 107.80 | 108.00 | 95.60 |
| Lifting Frequency (lift/min) | Mean Safety Shoes Discomfort Rating (SSDR) | |
|---|---|---|
| Present Study | Ghaleb et al. [54] | |
| 1 lift/min | 2.83 | 3.67 |
| 4 lifts/min | 2.50 | 3.88 |
| Safety Shoe Type | Mean Safety Shoes Discomfort Rating (SSDR) | ||
|---|---|---|---|
| Present Study at Normal Lab Temperature | Ghaleb et al. [54] | Al Ashaik et al. [38] on 5 lifts/min at 20 °C | |
| Light safety shoes | 1.60 | 4.28 | 2.43 |
| Medium safety shoes | 1.88 | 3.93 | 2.43 |
| Heavy safety shoes | 4.50 | 3.13 | 3.79 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alferdaws, F.F.; Ramadan, M.Z. Effects of Lifting Method, Safety Shoe Type, and Lifting Frequency on Maximum Acceptable Weight of Lift, Physiological Responses, and Safety Shoes Discomfort Rating. Int. J. Environ. Res. Public Health 2020, 17, 3012. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093012
Alferdaws FF, Ramadan MZ. Effects of Lifting Method, Safety Shoe Type, and Lifting Frequency on Maximum Acceptable Weight of Lift, Physiological Responses, and Safety Shoes Discomfort Rating. International Journal of Environmental Research and Public Health. 2020; 17(9):3012. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093012
Chicago/Turabian StyleAlferdaws, Fares F., and Mohamed Z. Ramadan. 2020. "Effects of Lifting Method, Safety Shoe Type, and Lifting Frequency on Maximum Acceptable Weight of Lift, Physiological Responses, and Safety Shoes Discomfort Rating" International Journal of Environmental Research and Public Health 17, no. 9: 3012. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093012