Differential Effect of Growth on Development between AGA and SGA Preterm Infants


Abstract
:1. Introduction
2. Materials and Methods
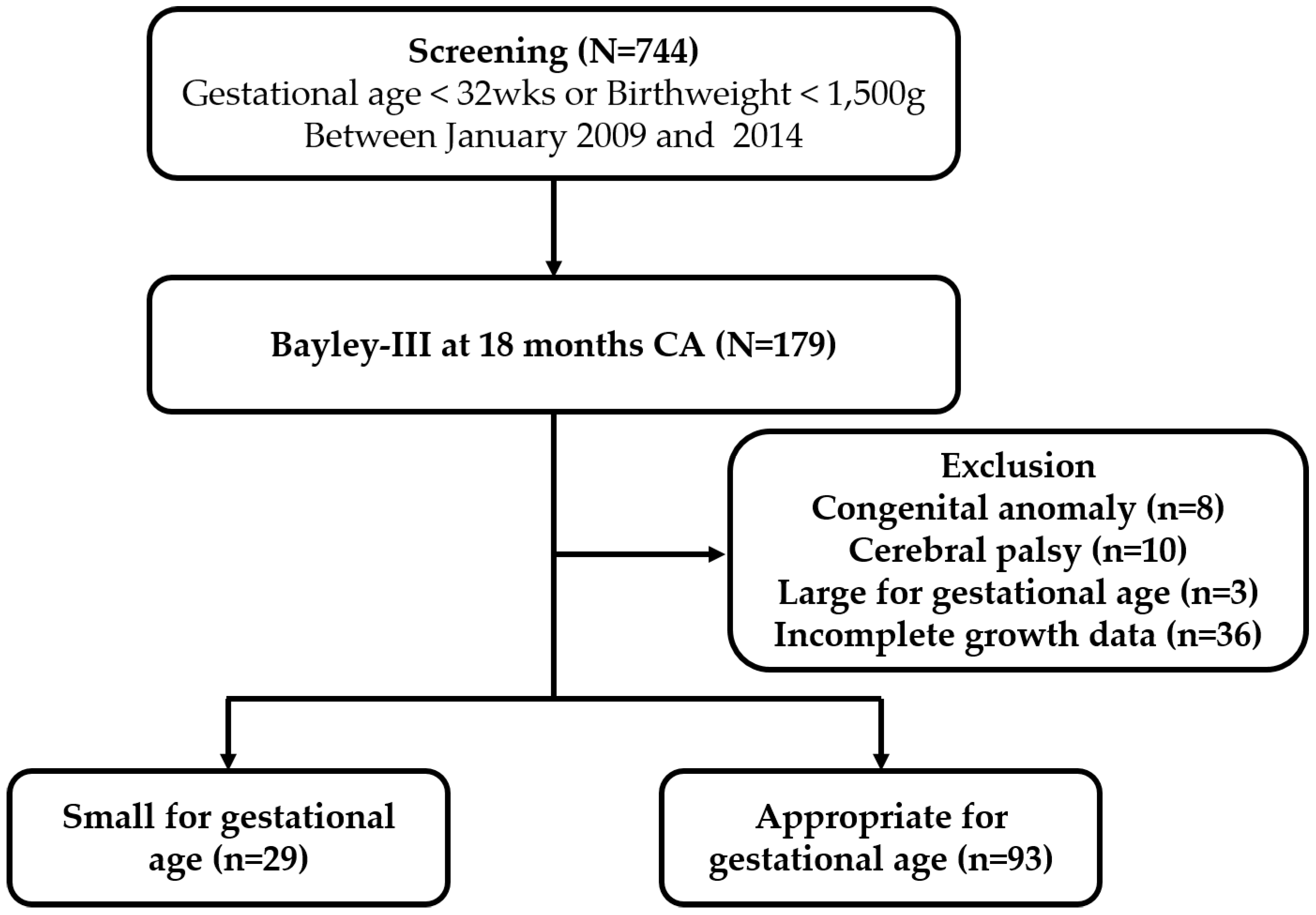
2.1. Patients and Data Collection
2.2. Statistical Analysis
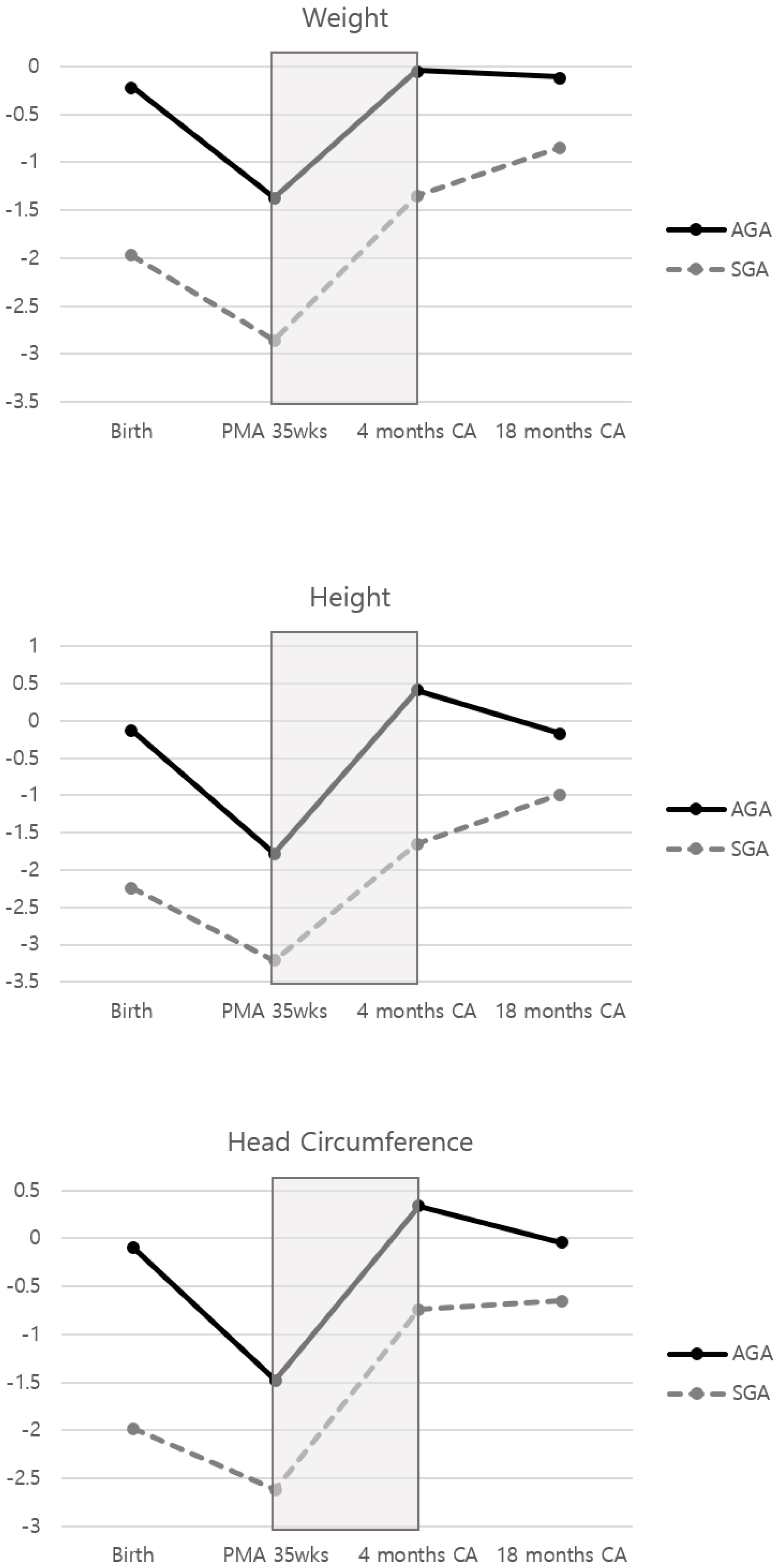
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Preterm Birth 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 19 February 2018).
- Chung, S.H.; Bae, C.W. Improvement in the survival rates of very low birth weight infants after the establishment of the Korean Neonatal Network: Comparison between the 2000s and 2010s. J. Korean Med. Sci. 2017, 32, 1228–1234. [Google Scholar] [CrossRef] [PubMed]
- De Curtis, M.; Rigo, J. Extrauterine growth restriction in very-low-birthweight infants. Acta Paediatr. 2004, 93, 1563–1568. [Google Scholar] [CrossRef] [PubMed]
- Horbar, J.D.; Ehrenkranz, R.A.; Badger, G.J.; Edwards, E.M.; Morrow, K.A.; Soll, R.F.; Buzas, J.S.; Bertino, E.; Gagliardi, L.; Bellù, R. Weight growth velocity and postnatal growth failure in infants 501 to 1500 grams: 2000–2013. Pediatrics 2015, 136, e84–e92. [Google Scholar] [CrossRef] [Green Version]
- Ramel, S.E.; Gray, H.L.; Ode, K.L.; Younge, N.; Georgieff, M.K.; Demerath, E.W. Body composition changes in preterm infants following hospital discharge: Comparison with term infants. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Westerberg, A.C.; Henriksen, C.; Ellingvåg, A.; Veierød, M.B.; Júlíusson, P.B.; Nakstad, B.; Aurvåg, A.K.; Rønnestad, A.; Grønn, M.; Iversen, P.O.; et al. First year growth among very low birth weight infants. Acta Paediatr. 2010, 99, 556–562. [Google Scholar] [CrossRef]
- Hintz, S.R.; Barnes, P.D.; Bulas, D.; Slovis, T.L.; Finer, N.N.; Wrage, L.A.; Das, A.; Tyson, J.E.; Stevenson, D.K.; Carlo, W.A.; et al. Neuroimaging and neurodevelopmental outcome in extremely preterm infants. Pediatrics 2015, 135, e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, N.A. Advanced neuroimaging and its role in predicting neurodevelopmental outcomes in very preterm infants. Semin. Perinatol. 2016, 40, 530–541. [Google Scholar] [CrossRef] [Green Version]
- Ghods, E.; Kreissl, A.; Brandstetter, S.; Fuiko, R.; Widhalm, K. Head circumference catch-up growth among preterm very low birth weight infants: Effect on neurodevelopmental outcome. J. Perinat. Med. 2011, 39, 579–586. [Google Scholar] [CrossRef]
- Neubauer, V.; Griesmaier, E.; Pehböck-Walser, N.; Pupp-Peglow, U.; Kiechl-Kohlendorfer, U. Poor postnatal head growth in very preterm infants is associated with impaired neurodevelopment outcome. Acta Paediatr. 2013, 102, 883–888. [Google Scholar] [CrossRef]
- Leppänen, M.; Lapinleimu, H.; Lind, A.; Matomäki, J.; Lehtonen, L.; Haataja, L.; Rautava, P.; PIPARI Study Group. Antenatal and postnatal growth and 5-year cognitive outcome in very preterm infants. Pediatrics 2014, 133, 63–70. [Google Scholar]
- Ranke, M.B.; Krägeloh-Mann, I.; Vollmer, B. Growth, head growth, and neurocognitive outcome in children born very preterm: Methodological aspects and selected results. Dev. Med. Child. Neurol. 2015, 57, 23–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ACOG Committee on Practice Bulletins Obstetrics. ACOG practice bulletin. Clinical management guidelines for obstetricians-gynecologists. 2004, 55 (replaces practice pattern number 6, October 1997). Management of postterm pregnancy. Obstet. Gynecol. 2004, 104, 639–646. [Google Scholar]
- University of Calgary. The Fenton Preterm Growth Chart site 2013. Available online: https://www.ucalgary.ca/fenton/2013chart (accessed on 19 February 2018).
- Tozzi, M.G.; Moscuzza, F.; Michelucci, A.; Lorenzoni, F.; Cosini, C.; Ciantelli, M.; Ghirri, P. ExtraUterine growth restriction (EUGR) in preterm Infants: Growth patterns, nutrition and epigenetic markers. A pilot study. Front. Pediatr. 2018, 6, 408. [Google Scholar] [CrossRef] [PubMed]
- Franz, A.R.; Pohlandt, F.; Bode, H.; Mihatsch, W.A.; Sander, S.; Kron, M.; Steinmacher, J. Intrauterine, early neonatal, and postdischarge growth and neurodevelopmental outcome at 5.4 years in extremely preterm infants after intensive neonatal nutritional support. Pediatrics 2009, 123, e101–e109. [Google Scholar] [CrossRef] [Green Version]
- Claas, M.; de Vries, L.; Koopman, C.; Venema, M.U.; Eijsermans, M.; Bruinse, H.; Verrijn Stuart, A.A. Postnatal growth of preterm born children ≤ 750 g at birth. Early Hum. Dev. 2011, 87, 495–507. [Google Scholar] [CrossRef]
- Raz, S.; Newman, J.B.; DeBastos, A.K.; Peters, B.N.; Batton, D.G. Postnatal growth and neuropsychological performance in preterm-birth preschoolers. Neuropsychology 2014, 28, 188. [Google Scholar] [CrossRef]
- Raghuram, K.; Yang, J.; Church, P.T.; Cieslak, Z.; Synnes, A.; Mukerji, A.; Shah, P.S.; Canadian Neonatal Network; Canadian Neonatal Follow-Up Network Investigators. Head growth trajectory and neurodevelopmental outcomes in preterm neonates. Pediatrics 2017, 140, e20170216. [Google Scholar] [CrossRef] [Green Version]
- Thompson, R.A.; Nelson, C.A. Developmental science and the media: Early brain development. Am. Psychol. 2001, 56, 5. [Google Scholar] [CrossRef]
- Ramel, S.E.; Demerath, E.W.; Gray, H.L.; Younge, N.; Boys, C.; Georgieff, M.K. The relationship of poor linear growth velocity with neonatal illness and two-year neurodevelopment in preterm infants. Neonatology 2012, 102, 19–24. [Google Scholar] [CrossRef]
- Belfort, M.B.; Rifas-Shiman, S.L.; Sullivan, T.; Collins, C.T.; McPhee, A.J.; Ryan, P.; Kleinman, K.P.; Gillman, M.W.; Gibson, R.A.; Makrides, M. Infant growth before and after term: Effects on neurodevelopment in preterm infants. Pediatrics 2011, 128, e899–e906. [Google Scholar] [CrossRef]
- Belfort, M.B.; Gillman, M.W.; Buka, S.L.; Casey, P.H.; McCormick, M.C. Preterm infant linear growth and adiposity gain: Trade-offs for later weight status and intelligence quotient. J. Pediatr. 2013, 163, 1564–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| SGA 1 (n = 29) | AGA 2 (n = 93) | p Value | |
|---|---|---|---|
| Mean (SD) or n (%) | Mean (SD) or n (%) | ||
| Gestational age, weeks day/7 | 30 4/7 (2 6/7) | 28 1/7 (2 2/7) | <0.001 |
| <26 | 3 (10.3) | 14 (15.1) | <0.001 |
| 26–28 | 5 (17.2) | 45 (48.4) | |
| 29–31 | 9 (31.0) | 31 (33.3) | |
| ≥32 | 12 (41.4) | 3 (3.2) | |
| Primiparous | 20 (69.0) | 69 (74.2) | 0.580 |
| Caesarean section | 24 (82.8) | 51 (54.8) | 0.007 |
| Multiple birth | 12 (41.4) | 51 (54.8) | 0.205 |
| Female | 15 (51.7) | 46 (49.5) | 0.832 |
| Birthweight, g | 892.7 (271.6) | 1053.2 (296.5) | 0.010 |
| Length, cm | 34.1 (3.5) | 36.0 (3.5) | 0.014 |
| Head circumference, cm | 24.9 (2.4) | 25.4 (2.5) | 0.404 |
| Maternal chorioamnionitis | 3 (10.3) | 14 (15.1) | 0.523 |
| Respiratory distress syndrome | 10 (34.5) | 49 (52.7) | 0.087 |
| Patent ductus arteriosus treatment | |||
| Medication | 10 (34.5) | 46 (49.5) | 0.050 |
| Operation | 1 (3.5) | 12 (12.9) | |
| Bronchopulmonary dysplasia | |||
| Mild | 7 (24.1) | 30 (32.6) | 0.100 |
| Moderate | 6 (20.7) | 29 (31.5) | |
| Severe | 1 (3.5) | 8 (8.7) | |
| Intraventricular hemorrhage ≥ Grade III | 1 (3.5) | 4 (4.3) | 0.840 |
| Periventricular leukomalacia | 1 (3.5) | 3 (3.2) | 0.953 |
| Necrotizing enterocolitis ≥ Stage 2 | 4 (13.8) | 10 (10.8) | 0.654 |
| Sepsis | 2 (9.5) | 16 (20.3) | 0.255 |
| Retinopathy of prematurity operation | 4 (19.1) | 34 (43.0) | 0.044 |
| Extrauterine growth retardation | 12 (41.4) | 54 (58.1) | 0.115 |
| Cognition score | |||
| Mean (SD) | 97.4 (10.8) | 99.3 (13.3) | 0.488 |
| <85 | 2 (6.9) | 7 (8.5) | 0.910 |
| Language score | |||
| Mean (SD) | 90.6 (11.9) | 97.0 (15.5) | 0.043 |
| <85 | 9 (31.0) | 21 (22.6) | 0.356 |
| Motor score | |||
| Mean (SD) | 97.1 (9.1) | 96.8 (11.8) | 0.905 |
| <85 | 2 (6.9) | 12 (12.9) | 0.376 |
| Growth Indicators | Time | Cognition | Language | Motor | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SGA (n = 29) 1 | AGA (n = 93) 2 | SGA | AGA | SGA | AGA | ||||||||
| ß | p | ß | p | ß | p | ß | p | ß | p | ß | p | ||
| Weight | Birth | 12.78 | 0.048 | 3.61 | 0.091 | 13.19 | 0.059 | 4.79 | 0.057 | 6.16 | 0.232 | 4.15 | 0.018 |
| 35 weeks | 11.61 | 0.214 | 3.99 | 0.157 | 12.75 | 0.234 | 9.19 | 0.004 | 6.32 | 0.407 | 2.15 | 0.348 | |
| 4 months CA 3 | 2.04 | 0.402 | 1.01 | 0.453 | 4.00 | 0.141 | 1.53 | 0.329 | 0.56 | 0.777 | 2.08 | 0.053 | |
| 18 months CA | 2.92 | 0.209 | 0.30 | 0.841 | 3.15 | 0.236 | −0.48 | 0.780 | 1.78 | 0.347 | 2.70 | 0.022 | |
| Length | Birth | 2.91 | 0.522 | −1.94 | 0.356 | −1.60 | 0.759 | −0.64 | 0.793 | 1.19 | 0.747 | −1.62 | 0.339 |
| 35 weeks | 1.99 | 0.772 | −2.63 | 0.292 | −0.47 | 0.953 | 1.93 | 0.507 | −0.88 | 0.874 | 0.51 | 0.803 | |
| 4 months CA | 0.90 | 0.706 | −0.23 | 0.821 | 3.52 | 0.183 | −0.85 | 0.478 | 0.00 | 0.999 | 0.42 | 0.609 | |
| 18 months CA | 2.08 | 0.304 | −0.23 | 0.867 | 1.53 | 0.511 | −0.60 | 0.706 | 0.76 | 0.646 | 1.69 | 0.124 | |
| Head Circumference | Birth | −4.27 | 0.458 | 0.36 | 0.822 | −4.41 | 0.504 | 3.75 | 0.040 | −5.27 | 0.249 | −0.62 | 0.628 |
| 35 weeks | 4.29 | 0.586 | 1.81 | 0.328 | 0.71 | 0.938 | 3.49 | 0.104 | 2.59 | 0.683 | 1.70 | 0.255 | |
| 4 months CA | 0.91 | 0.739 | 2.71 | 0.012 | 1.20 | 0.702 | 2.26 | 0.076 | −0.77 | 0.727 | 2.38 | 0.006 | |
| 18 months CA | 4.57 | 0.207 | 3.55 | 0.003 | 4.42 | 0.290 | 3.08 | 0.030 | 1.41 | 0.637 | 2.60 | 0.008 | |
| Growth Indicators | Time Period | Cognition | Language | Motor | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SGA (n = 29) 1 | AGA (n = 93) 2 | SGA | AGA | SGA | AGA | ||||||||
| ß | p | ß | p | ß | p | ß | p | ß | p | ß | p | ||
| Weight | Birth to 18 months CA 3 | 2.53 | 0.309 | −0.23 | 0.878 | 2.06 | 0.474 | −0.69 | 0.685 | 1.62 | 0.421 | 2.40 | 0.040 |
| Birth to 35 weeks | 0.68 | 0.942 | 2.68 | 0.407 | −8.12 | 0.438 | 10.90 | 0.003 | 0.81 | 0.914 | 1.68 | 0.520 | |
| 35 weeks to 4 months CA | 1.29 | 0.602 | 0.11 | 0.934 | 3.20 | 0.249 | −0.57 | 0.723 | 0.14 | 0.942 | 1.66 | 0.132 | |
| 4 months CA to 18 months CA | 0.99 | 0.674 | −1.42 | 0.438 | −0.59 | 0.829 | −3.58 | 0.092 | 1.23 | 0.514 | 0.27 | 0.855 | |
| Length | Birth to 18 months CA | 1.43 | 0.475 | 0.51 | 0.688 | 1.78 | 0.435 | −0.28 | 0.849 | 0.50 | 0.759 | 2.04 | 0.044 |
| Birth to 35 weeks | −2.56 | 0.617 | 0.06 | 0.973 | 1.76 | 0.764 | 1.51 | 0.477 | −1.99 | 0.629 | 1.49 | 0.312 | |
| 35 weeks to 4 months CA | 0.65 | 0.784 | 0.21 | 0.838 | 3.50 | 0.181 | −1.16 | 0.329 | 0.11 | 0955 | 0.33 | 0.685 | |
| 4 months CA to 18 months CA | 3.14 | 0.298 | 0.16 | 0.901 | −2.42 | 0.486 | 0.78 | 0.599 | 1.69 | 0.492 | 0.81 | 0.431 | |
| Head Circumference | Birth to 18 months CA | 5.35 | 0.102 | 2.20 | 0.027 | 5.27 | 0.164 | 0.53 | 0.653 | 3.02 | 0.263 | 1.97 | 0.040 |
| Birth to 35 weeks | 6.56 | 0.247 | 0.72 | 0.598 | 4.77 | 0.468 | −0.89 | 0.579 | 6.63 | 0.140 | 1.39 | 0.207 | |
| 35 weeks to 4 months CA | 0.38 | 0.887 | 2.62 | 0.032 | 1.08 | 0.727 | 1.30 | 0.367 | −1.04 | 0.629 | 2.26 | 0.022 | |
| 4 months CA to 18 months CA | 1.61 | 0.561 | 0.27 | 0.885 | 1.23 | 0.698 | 0.50 | 0.817 | 1.57 | 0.479 | −0.92 | 0.540 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, I.G.; Kim, E.-K.; Cho, H.; Shin, S.H.; Sohn, J.A.; Kim, H.-S. Differential Effect of Growth on Development between AGA and SGA Preterm Infants. Int. J. Environ. Res. Public Health 2020, 17, 3022. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093022
Song IG, Kim E-K, Cho H, Shin SH, Sohn JA, Kim H-S. Differential Effect of Growth on Development between AGA and SGA Preterm Infants. International Journal of Environmental Research and Public Health. 2020; 17(9):3022. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093022
Chicago/Turabian StyleSong, In Gyu, Ee-Kyung Kim, Hannah Cho, Seung Han Shin, Jin A. Sohn, and Han-Suk Kim. 2020. "Differential Effect of Growth on Development between AGA and SGA Preterm Infants" International Journal of Environmental Research and Public Health 17, no. 9: 3022. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093022