Association between Sleep Quality and Duration and Periodontal Disease among University Students: A Cross-Sectional Study

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
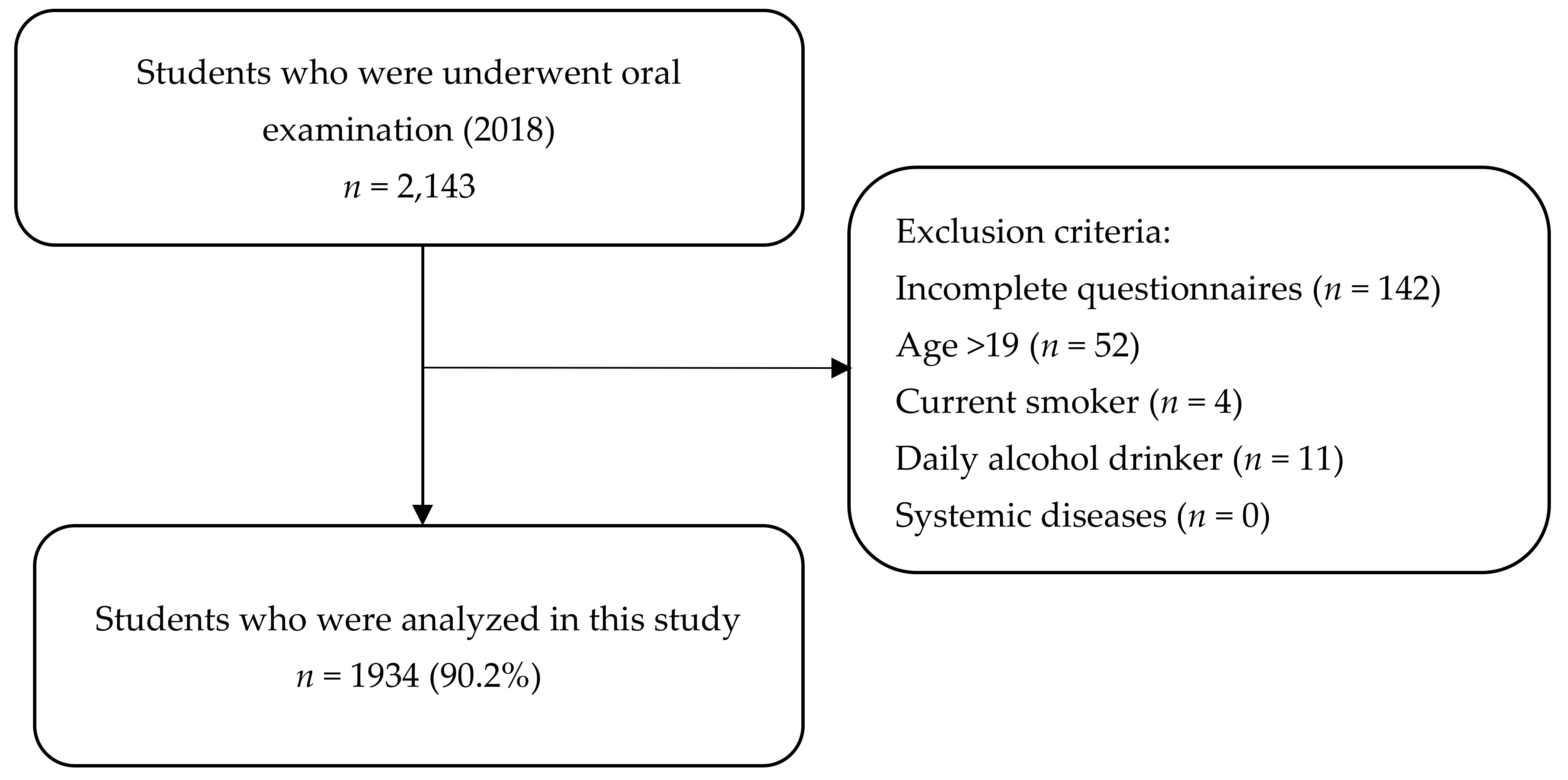
2.1. Study Participants
2.2. Ethical Procedures and Informed Consent
2.3. Self-Questionnaire
2.4. Assessment of Sleep Quality
2.5. Assessment of Stress
2.6. Oral Examination
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- National Health and Nutrition Survey 2018. Available online: https://www.mhlw.go.jp/stf/newpage_08789.html (accessed on 12 March 2010). (In Japanese).
- Qureshi, A.I.; Giles, W.H.; Croft, J.B.; Bliwise, D.L. Habitual sleep patterns and risk for stroke and coronary heart disease: A 10-year follow-up from NHANES I. Neurology 1997, 48, 904–910. [Google Scholar] [CrossRef]
- Zielinski, M.R.; Krueger, J.M. Sleep and innate immunity. Front. Biosci. (Schol. Ed.) 2011, S3, 632–642. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-Y.; Yadav, D.; Ahn, S.V.; Koh, S.-B.; Park, J.T.; Yoon, J.; Yoo, B.-S.; Lee, S.-H. A prospective study of total sleep duration and incident metabolic syndrome: The ARIRANG study. Sleep Med. 2015, 16, 1511–1515. [Google Scholar] [CrossRef] [PubMed]
- Yaggi, H.K.; Araujo, A.B.; Mckinlay, J.B. Sleep Duration as a Risk Factor for the Development of Type 2 Diabetes. Diabetes Care 2006, 29, 657–661. [Google Scholar] [CrossRef] [Green Version]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 3. [Google Scholar] [CrossRef]
- Survey on Dental Disease 2016. Available online: https://www.mhlw.go.jp/toukei/list/62-17c.html (accessed on 22 April 2020).
- Nakada, T.; Kato, T.; Numabe, Y. Effects of fatigue from sleep deprivation on experimental periodontitis in rats. J. Periodontal Res. 2014, 50, 131–137. [Google Scholar] [CrossRef]
- Karaaslan, F.; Dikilitaş, A. The association between stage-grade of periodontitis and sleep quality and oral health‒related quality of life. J. Periodontol. 2019, 90, 1133–1141. [Google Scholar] [CrossRef]
- Romandini, M.; Gioco, G.; Perfetti, G.; Deli, G.; Staderini, E.; Laforì, A. The association between periodontitis and sleep duration. J. Clin. Periodontol. 2017, 44, 490–501. [Google Scholar] [CrossRef]
- Carra, M.C.; Schmitt, A.; Thomas, F.; Danchin, N.; Pannier, B.; Bouchard, P. Sleep disorders and oral health: A cross-sectional study. Clin. Oral. Investig. 2016, 21, 975–983. [Google Scholar] [CrossRef]
- Grover, V.; Malhotra, R.; Kaur, H. Exploring association between sleep deprivation and chronic periodontitis: A pilot study. J. Indian Soc. Periodontol. 2015, 19, 304–307. [Google Scholar] [CrossRef]
- Singh, V.; Gan, J.; Liew, W.; Soe, H.K.; Nettem, S.; Nettemu, S. Association between quality of sleep and chronic periodontitis: A case–control study in Malaysian population. Dent. Res. J. (Isfahan) 2019, 16, 29–35. [Google Scholar] [CrossRef]
- Alqaderi, H.; Goodson, J.M.; Agaku, I. Association between sleep and severe periodontitis in a nationally representative adult US population. J. Periodontol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Wiener, R.C. Relationship of Routine Inadequate Sleep Duration and Periodontitis in a Nationally Representative Sample. Sleep Disord. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preišegolavičiūtė, E.; Leskauskas, D.; Adomaitienė, V. Associations of quality of sleep with lifestyle factors and profile of studies among Lithuanian students. Medicina (Kaunas) 2010, 46, 482–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesquita, G.; Reimão, R. Quality of sleep among university students: Effects of night time computer and television use. Arq. Neuropsiquiatr. 2010, 68, 720–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuta, M.; Ekuni, D.; Irie, K.; Azuma, T.; Tomofuji, T.; Ogura, T.; Morita, M. Sex Differences in Gingivitis Relate to Interaction of Oral Health Behaviors in Young People. J. Periodontol. 2011, 82, 558–565. [Google Scholar] [CrossRef]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. 2000, 97, 165–172. [Google Scholar] [CrossRef]
- Toyama, N.; Ekuni, D.; Taniguchi-Tabata, A.; Yoneda, T.; Kataoka, K.; Yokoi, A.; Uchida, Y.; Fukuhara, D.; Saho, H.; Monirul, I.M.; et al. Associations between sleep bruxism, sleep quality, and exposure to secondhand smoke in Japanese young adults: A cross-sectional study. Sleep Med. 2019, 68, 57–62. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385. [Google Scholar] [CrossRef]
- Sumi, K. Reliability and validity of the Japanese version of the Perceived Stress Scale. J. Health Psychol. Res. 2006, 19, 44–53. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Lu, W.; Bian, Q.; Wang, W.; Wu, X.; Wang, Z.; Zhao, M. Chinese version of the Perceived Stress Scale-10: A psychometric study in Chinese university students. PLoS ONE 2017, 12, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenstein, G. The Role of Bleeding upon Probing in the Diagnosis of Periodontal Disease: A Literature Review. J. Periodontol. 1984, 55, 684–688. [Google Scholar] [CrossRef]
- Greene, J.G.; Vermillion, J.R. The Simplified Oral Hygiene Index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Kawabata, Y.; Ekuni, D.; Miyai, H.; Kataoka, K.; Yamane, M.; Mizutani, S.; Irie, K.; Azuma, T.; Tomofuji, T.; Iwasaki, Y.; et al. Relationship Between Prehypertension/Hypertension and Periodontal Disease: A Prospective Cohort Study. Am. J. Hypertens. 2016, 29, 388–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purani, H.; Friedrichsen, S.; Allen, A.M. Sleep quality in cigarette smokers: Associations with smoking-related outcomes and exercise. Addict. Behav. 2019, 90, 71–76. [Google Scholar] [CrossRef]
- Ogeil, R.P.; Cheetham, A.; Mooney, A.; Allen, N.B.; Schwartz, O.; Byrne, M.L.; Simmons, J.G.; Whittle, S.; Lubman, D.I. Early adolescent drinking and cannabis use predicts later sleep-quality problems. Psychol. Addict. Behav. 2019, 33, 266–273. [Google Scholar] [CrossRef]
- Kitazawa, M.; Yoshimura, M.; Hitokoto, H.; Sato-Fujimoto, Y.; Murata, M.; Negishi, K.; Mimura, M.; Tsubota, K.; Kishimoto, T. Survey of the effects of internet usage on the happiness of Japanese university students. Health Qual. Life Outcomes 2019, 17. [Google Scholar] [CrossRef] [Green Version]
- Corrêa, C.D.C.; Oliveira, F.K.D.; Pizzamiglio, D.S.; Ortolan, E.V.P.; Weber, S.A.T. Sleep quality in medical students: A comparison across the various phases of the medical course. J. Bras. Pneumol. 2017, 43, 285–289. [Google Scholar] [CrossRef]
- Dietch, J.R.; Taylor, D.J.; Sethi, K.; Kelly, K.; Bramoweth, A.D.; Roane, B.M. Psychometric Evaluation of the PSQI in U.S. College Students. J. Clin. Sleep Med. 2016, 12, 1121–1129. [Google Scholar] [CrossRef] [Green Version]
- Ekuni, D.; Mizutani, S.; Kojima, A.; Tomofuji, T.; Irie, K.; Azuma, T.; Yoneda, T.; Furuta, M.; Eshima, N.; Iwasaki, Y.; et al. Relationship between increases in BMI and changes in periodontal status: A prospective cohort study. J. Clin. Periodontol. 2014, 41, 772–778. [Google Scholar] [CrossRef]
- Linden, G.J.; Mullally, B.H.; Freeman, R. Stress and the progression of periodontal disease. J. Clin. Periodontol. 1996, 23, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Watson, E.J.; Coates, A.M.; Kohler, M.; Banks, S. Caffeine Consumption and Sleep Quality in Australian Adults. Nutrients. 2016, 8, E479. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.F.; Cheng, S.H.; Yeh, T.L.; Shih, C.-C.; Chen, K.C.; Yang, Y.C.; Yang, Y.K. The risk factors of Internet addiction—A survey of university freshmen. Psychiatry Res. 2009, 167, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Benavente, S.B.T.; Silva, R.M.D.; Higashi, A.B.; Guido, L.D.A.; Costa, A.L.S. Influence of stress factors and socio-demographic characteristics on the sleep quality of nursing students. Rev. Esc. Enferm USP. 2014, 48, 514–520. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables (n = 1934) | n (%)Mean ± SD |
|---|---|
| Gender | |
| Male | 1058 (54.7) |
| Female | 876 (45.3) |
| Age (y) | 18.2 ± 0.4 |
| Regular dental check-up (Yes) | 572 (29.6) |
| Daily flossing (Yes) | 499 (25.8) |
| Daily tooth brushing (≥2 times) | 179 (9.2) |
| OHI-S | 0.5 ± 0.5 |
| Number of teeth present | 28.3 ± 1.4 |
| Exercise (Yes) | 1462 (75.6) |
| Sleeping duration (hour/night) | 7.1 ± 1.1 |
| PSQI Global | 4.0 ± 1.9 |
| Sleep quality | |
| Poor (PSQI ≥ 5) | 372 (19.2) |
| Good (PSQI < 5) | 1562 (80.8) |
| PSS-10 (Total) | 17.2 ± 2.5 |
| Psychological stress | |
| No stress | 87 (4.5) |
| Moderate stress | 1843 (95.2) |
| High stress | 4 (0.2) |
| Periodontal disease (Yes) | 283 (14.6) |
| Variables (n = 1934) | Periodontal Disease (n = 283) | Non-Periodontal Disease (n = 1651) | p-Value |
|---|---|---|---|
| Gender (Male) | 185 (65.4) 1 | 873 (52.8) | <0.001 3 |
| Age (y) | 18.2 ± 0.4 2 | 18.2 ± 0.4 | 0.125 4 |
| Regular dental check-up (Yes) | 82 (28.9) | 490 (29.7) | 0.811 3 |
| Flossing daily (Yes) | 61 (21.6) | 438 (26.5) | 0.077 3 |
| Daily tooth brushing (≥2 times) | 30 (10.6) | 149 (9.0) | 0.398 3 |
| OHI-S | 0.7 ± 0.7 | 0.5 ± 0.5 | <0.001 4 |
| Number of teeth present | 28.7 ± 1.41 | 28.3 ± 1.35 | <0.001 4 |
| Exercise (Yes) | 222 (78.4) | 1240 (75.1) | 0.227 3 |
| Sleeping duration (hour/night) | 7.0 ± 1.1 | 7.1 ± 1.2 | 0.283 4 |
| Sleep quality | |||
| Poor (PSQI >5) | 59 (20.8) | 313 (18.9) | 0.456 3 |
| PSQI Global | 4.1 ± 2.0 | 3.9 ± 1.9 | 0.201 5 |
| PSQI domain score | |||
| Sleep quality | 1.0 ± 0.6 | 1.0 ± 0.6 | 0.868 4 |
| Sleep latency | 0.8 ± 0.8 | 0.8 ± 0.8 | 0.145 4 |
| Sleep duration | 0.9 ± 0.8 | 0.8 ± 0.8 | 0.260 4 |
| Habitual sleep efficiency | 0.2 ± 0.5 | 0.1 ± 0.4 | 0.054 4 |
| Sleep disturbance | 0.5 ± 0.5 | 0.5 ± 0.5 | 0.213 4 |
| Medication | 0.02 ± 0.2 | 0.04 ± 0.3 | 0.133 4 |
| Daytime dysfunction | 0.7 ± 0.7 | 0.7 ± 0.7 | 0.685 4 |
| Total PSS-10 | 17.1 ± 2.6 | 17.2 ± 2.5 | 0.900 4 |
| Psychological stress | |||
| No stress | 18 (6.3) | 69 (4.2) | 0.219 3 |
| Moderate stress | 264 (93.3) | 1579 (95.6) | |
| High stress | 1 (0.4) | 3 (0.2) |
| Independent Variables | OR (95% CI) 1 | p-Value | |
|---|---|---|---|
| Gender | Female | Ref | 0.015 |
| Male | 1.42 (1.10–1.87) | ||
| Age | 1.28 (0.91–1.78) | 0.156 | |
| Regular dental check-up | Yes | Ref | 0.402 |
| No | 0.88 (0.66–1.18) | ||
| Flossing daily | Yes | Ref | 0.153 |
| No | 1.26 (0.92–1.73) | ||
| Daily tooth brushing frequency | ≥2 times | Ref | 0.904 |
| <2 times | 1.03 (0.67–1.59) | ||
| OHI-S | 2.30 (1.83–2.90) | <0.001 | |
| Exercise | Yes | Ref | 0.522 |
| No | 0.90 (0.65–1.24) | ||
| Sleep quality | Good | Ref | 0.577 |
| Poor | 1.09 (0.79–1.53) | ||
| Sleeping duration (hour/night) | 0.98 (0.87–1.10) | 0.717 | |
| Psychological stress | No stress | Ref | |
| Moderate stress | 0.63 (0.37–1.09) | 0.103 | |
| High stress | 1.20 (0.11–12.77) | 0.879 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.M.; Ekuni, D.; Toyama, N.; Taniguchi-Tabata, A.; Kataoka, K.; Uchida-Fukuhara, Y.; Fukuhara, D.; Saho, H.; Sawada, N.; Nakashima, Y.; et al. Association between Sleep Quality and Duration and Periodontal Disease among University Students: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 3034. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093034
Islam MM, Ekuni D, Toyama N, Taniguchi-Tabata A, Kataoka K, Uchida-Fukuhara Y, Fukuhara D, Saho H, Sawada N, Nakashima Y, et al. Association between Sleep Quality and Duration and Periodontal Disease among University Students: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(9):3034. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093034
Chicago/Turabian StyleIslam, Md Monirul, Daisuke Ekuni, Naoki Toyama, Ayano Taniguchi-Tabata, Kota Kataoka, Yoko Uchida-Fukuhara, Daiki Fukuhara, Hikari Saho, Nanami Sawada, Yukiho Nakashima, and et al. 2020. "Association between Sleep Quality and Duration and Periodontal Disease among University Students: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 9: 3034. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093034