Antisocial Disorders in Adolescence and Youth, According to Structural, Emotional, and Cognitive Transdiagnostic Variables: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria and Inclusion of Articles
2.2. Information Sources
2.3. Search
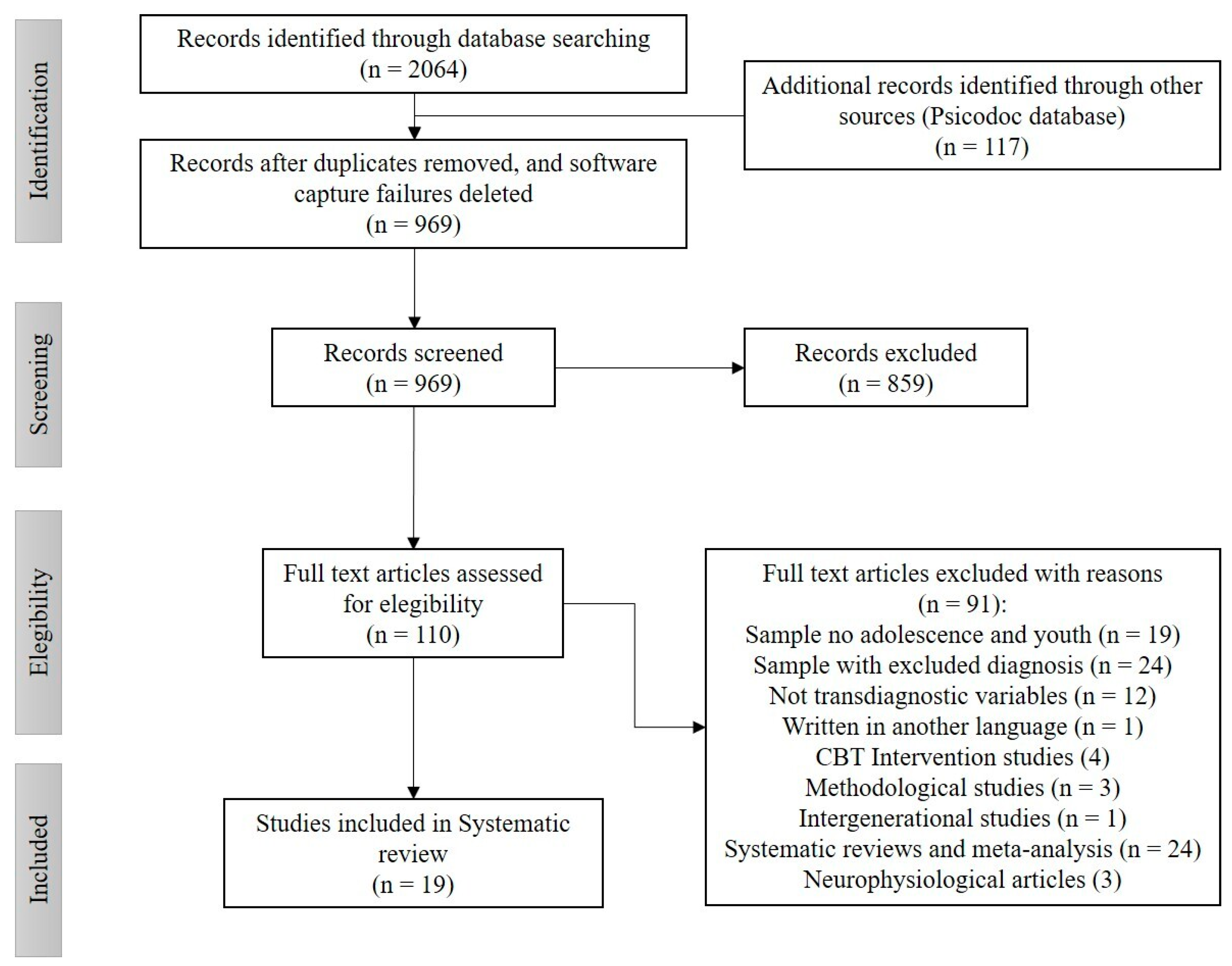
2.4. Selection of Studies
2.5. Data Extraction Process
2.6. Bias Risk
2.7. Summary of Results
3. Results
3.1. Characteristics of the Studies
3.2. Assessment of the Methodological and Theoretical Quality
3.3. Qualitative Synthesis
4. Discussion
4.1. Personality, Inhibition-Behavioral Activation and Negative Affect
4.2. Emotional Dysregulation, Motivation and Cognition
4.3. Limitations
4.4. Clinical Implications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Achenbach, T.M.; Edelbrock, C.S. Manual for the Child Behavior Checklist and Revised Child Profile; University of Vermont Department of Psychiatry: Burlington, VT, USA, 1983. [Google Scholar]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders DSM-V, 5th ed.; APA: Washington, DC, USA, 2013. [Google Scholar]
- Krueger, R.F.; Markon, K.E.; Patrick, C.J.; Iacono, W.G. Externalizing psychopathology in adulthood: A dimensional-spectrum conceptualization and its implications for DSM-V. J. Abnorm. Psychol. 2005, 114, 537–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandín, B.; Chorot, P.; Valiente, R.M. Transdiagnóstico: Nueva frontera en psicología clínica. Rev. Psicopatol. Psicol. Clín. 2012, 17, 185–203. [Google Scholar] [CrossRef] [Green Version]
- Mansell, W.; Harvey, A.; Watkins, E.; Shafran, R. Conceptual foundations of the transdiagnostic approach to CBT. J. Cogn. Psychother. 2009, 23, 6–19. [Google Scholar] [CrossRef]
- Ehrenreich-May, J.; Chu, B.C. Transdiagnostic Treatments for Children and Adolescents: Principles and Practice; Guilford Press: New York, NY, USA, 2014; pp. 3–14. [Google Scholar]
- Rector, N.A.; Man, V.; Lerman, B. The expanding Cognitive-Behavioural Therapy treatment umbrella for the anxiety disorders: Disorder-specific and transdiagnostic approaches. Can. J. Psychiat. 2014, 59, 301–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van-Wert, M.; Mishna, F.; Malti, T. A conceptual model of the relationship between maltreatment and externalizing, antisocial, and criminal behavior problems, and the intervening role of child welfare service delivery. Aggress. Violent. Behav. 2016, 29, 10–19. [Google Scholar] [CrossRef]
- Shankman, S.A.; Gorka, S.M. Psychopathology research in the RDoC era: Unanswered questions and the importance of the psychophysiological unit of analysis. Int. J. Psychophysiol. 2015, 98, 330–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casey, B.J.; Olivery, M.E.; Insel, T. A neurodevelopmental perspective on the research domain criteria (RDoC) framework. Biol. Psychiatry. 2014, 76, 350–353. [Google Scholar] [CrossRef]
- Yip, S.W.; Potenza, M.N. Application of Research Domain Criteria to childhood and adolescent impulsive and addictive disorders: Implications for treatment. Clin. Psychol. Rev. 2016, S0272–S7358, 30438-X. [Google Scholar] [CrossRef]
- Brazil, I.A.; van Dongen, J.D.M.; Maes, J.H.R.; Mars, R.B.; Baskin-Sommers, A.R. Classification and treatment of antisocial individuals: From behavior to biocognition. Neurosci. Biobehav. Rev. 2016, 91, 259–277. [Google Scholar] [CrossRef]
- Girard, J.M.; Wright, A.G.C.; Beeney, J.E.; Lazarus, S.A.; Scott, L.N.; Stepp, S.D.; Pilkonis, P.A. Interpersonal problems across levels of the psychopathology hierarchy. Compr. Psychiatry. 2017, 79, 53–69. [Google Scholar] [CrossRef]
- Sukhodolsky, D.G.; Smith, S.D.; McCauley, S.A.; Ibrahim, K.; Piasecka, J.B. Behavioral interventions for anger, irritability, and aggression in children and adolescents. J. Child Adolesc. Psychopharmacol. 2016, 26, 58–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, 4th ed.; John Wiley & Sons: West Sussex, UK, 2011. [Google Scholar]
- Perestelo-Pérez, L. Standards on how to develop and report systematic reviews in Psychology and Health. Int. J. Clin. Health Psychol. 2012, 13, 49–57. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The Second Decade: Improving Adolescent Health and Development; WHO: Washington, DC, USA, 2001; Available online: http://apps.who.int/iris/bitstream/handle/10665/64320/WHO_FRH_ADH_98.18_Rev.1.pdf (accessed on 20 April 2020).
- Sanislow, C.A.; Pine, D.S.; Quinn, K.J.; Kozak, M.J.; Garvey, M.A.; Heinssen, R.K.; Wang, P.S.E.; Cuthbert, B.N. Developing constructs for psychopathology research: Research domain criteria. J. Abnorm. Psychol. 2010, 119, 631–639. [Google Scholar] [CrossRef] [Green Version]
- Gwet, K.L. Handbook of Inter-Rater Reliability; Stataxis Publishing Company: Gaithersburg, MD, USA, 2001. [Google Scholar]
- Valentine, J.C.; Cooper, H. A systematic and transparent approach for assessing the methodological quality of intervention effectiveness research: The Study Design and Implementation Assessment Device (Study DIAD). Psychol. Methods 2008, 13, 130–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carragher, N.; Teesson, M.; Sunderland, M.; Newton, N.C.; Krueger, R.F.; Conrod, P.J.; Barrett, E.L.; Champion, K.E.; Nair, N.K.; Slade, T. The structure of adolescent psychopathology: A symptom-level analysis. Psychol. Med. 2016, 46, 981–994. [Google Scholar] [CrossRef] [PubMed]
- Castellanos-Ryan, N.; Brière, F.N.; O’Leary-Barrett, M.; Banaschewski, T.; Bokde, A.; Bromberg, U.; Büchel, C.; Flor, H.; Frouin, V.; Gallinat, J.; et al. The structure of psychopathology in adolescence and its common personality and cognitive correlates. J. Abnorm. Psychol. 2016, 125, 1039–1052. [Google Scholar] [CrossRef] [PubMed]
- Conway, C.C.; Starr, L.R.; Espejo, E.P.; Brennan, P.A.; Hammen, C. Stress responsivity and the structure of common mental disorders: Transdiagnostic internalizing and externalizing dimensions are associated with contrasting stress appraisal biases. J. Abnorm. Psychol. 2016, 125, 1079–1089. [Google Scholar] [CrossRef]
- Hamilton, J.L.; Burke, T.A.; Stange, J.P.; Kleiman, E.M.; Rubenstein, L.M.; Scopelliti, K.A.; Abramson, L.Y.; Alloy, L.B. Trait affect, emotion regulation, and the generation of negative and positive interpersonal events. Behav. Ther. 2017, 48, 435–447. [Google Scholar] [CrossRef]
- Hankin, B.L.; Davis, E.P.; Snyder, H.; Young, J.F.; Glynn, L.M.; Sandman, C.A. Temperament factors and dimensional, latent bifactor models of child psychopathology: Transdiagnostic and specific associations in two youth samples. Psychiatry Res. 2017, 252, 139–146. [Google Scholar] [CrossRef]
- Hawes, S.W.; Crane, C.A.; Henderson, C.E.; Mulvey, E.P.; Schubert, C.A.; Pardini, D.A. Codevelopment of psychopathic features and alcohol use during emerging adulthood: Disaggregating between- and within-person change. J. Abnorm. Psychol. 2015, 124, 729–739. [Google Scholar] [CrossRef]
- South, S.C.; Miller, M.L. Measuring momentary stress, affect, and cognition: Relationships with the internalizing and externalizing spectra. J. Psychopathol. Behav. Assess. 2013, 36, 93–104. [Google Scholar] [CrossRef]
- Copeland, W.E.; Brotman, M.A.; Costello, E.J. Normative irritability in youth: Developmental findings from the Great Smoky Mountains study. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 635–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadds, M.R.; Cauchi, A.J.; Wimalaweera, S.; Hawes, D.J.; Brennan, J. Outcomes, moderators, and mediators of empathic-emotion recognition training for complex conduct problems in childhood. Psychiatry Res. 2012, 199, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Jonhson, S.L.; Carver, C.S.; Joormann, J. Impulsive responses to emotion as a transdiagnostic vulnerability to internalizing and externalizing symptoms. J. Affect. Disord. 2013, 150, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Masi, G.; Muratori, P.; Manfredi, A.; Pisano, S.; Milone, A. Child behavior checklist emotional dysregulation profiles in youth with disruptive behavior disorders: Clinical correlates and treatment implications. Psychiatry Res. 2015, 225, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Mclaughlin, K.A.; Hatzenbuehler, M.L.; Mennin, D.S.; Nolen-Hoeksema, S. Emotion dysregulation and adolescent psychopathology: A prospective study. Behav. Res. Ther. 2011, 49, 544–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poon, J.A.; Turpyn, C.C.; Hansen, A.; Jacangelo, J.; Chaplin, T.M. Adolescent substance use & psychopathology: Interactive effects of cortisol reactivity and emotion regulation. Cognit. Ther. Res. 2015, 40, 368–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shea, S.E.; Coyne, L.W. Reliance on experiential avoidance in the context of relational aggression: Links to internalizing and externalizing problems and dysphoric mood among urban, minority adolescent girls. J. Contextual Behav. Sci. 2017, 6, 195–201. [Google Scholar] [CrossRef]
- Fahlgren, M.K.; Puhalla, A.A.; Sorgi, K.M.; McCloskey, M.S. Emotion processing in intermittent explosive disorder. Psychiatry Res. 2019, 273, 544–550. [Google Scholar] [CrossRef]
- Conway, C.C.; Mammen, C.; Brennan, P.A. Optimizing prediction of psychosocial and clinical outcomes with a transdiagnostic model of personality disorder. J. Pers. Disord. 2016, 30, 545–566. [Google Scholar] [CrossRef] [Green Version]
- Mclaughlin, K.A.; Aldao, A.; Wisco, B.E.; Hilt, L.M. Rumination as a transdiagnostic factor underlying transitions between internalizing symptoms and aggressive behavior in early adolescents. J. Abnorm. Psychol. 2014, 123, 13–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, A.L.; Eisner, M.; Obsuth, I.; Ribeaud, D. Situating violent ideations within the landscape of mental health: Associations between violent ideations and dimensions of mental health. Psychiatry Res. 2017, 249, 70–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du Pont, A.; Rhee, S.H.; Corley, R.P.; Hewitt, J.K.; Friedman, N.P. Rumination and executive functions: Understanding cognitive vulnerability for psychopathology. J. Affect. Disord. 2019, 256, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Eaton, N.R. The hierarchical structure of common mental disorders: Connecting multiple levels of comorbidity, bifactor models, and predictive validity. J. Abnorm. Psychol. 2015, 124, 1064–1078. [Google Scholar] [CrossRef]
- Kessler, R.C.; Petukhova, M.; Zaslavsky, A.M. The role of latent internalizing and externalizing predispositions in accounting for the development of comorbidity among common mental disorders. Curr. Opin. Psychiatry 2011, 24, 307–312. [Google Scholar] [CrossRef] [Green Version]
- Williams, T.F.; Scalco, M.D.; Simms, L.J. The construct validity of general and specific dimensions of personality pathology. Psychol. Med. 2018, 48, 834–848. [Google Scholar] [CrossRef]
- Copeland, W.E.; Angold, A.; Shanahan, L.; Costello, E.J. Longitudinal patterns of anxiety from childhood to adulthood: The Great Smoky Mountains Study. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 21–33. [Google Scholar] [CrossRef] [Green Version]
- Bell, K.M.; Naugle, A.E. Intimate partner violence theoretical considerations: Moving towards a contextual framework. Clin. Psychol. Rev. 2008, 28, 1096–1107. [Google Scholar] [CrossRef]
- Shorey, R.C.; Elmquist, J.; Zucosky, H.; Febres, J.; Brasfield, H.; Stuart, G.L. Experiential avoidance and male dating violence perpetration: An initial investigation. J. Contextual Behav. Sci. 2014, 3, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Kingston, J.; Clarke, S.; Remington, B. Experiential avoidance and problem behavior: A mediational analysis. Behav. Modif. 2010, 34, 145–163. [Google Scholar] [CrossRef]
- Kahle, S.; Utendale, W.T.; Widaman, K.F.; Hastings, P.D. Parasympathetic regulation and inhibitory control predict the development of externalizing problems in early childhood. J. Abnorm Child Psychol. 2018, 46, 237–249. [Google Scholar] [CrossRef]
- Roskam, I. Externalizing behavior from early childhood to adolescence: Prediction from inhibition, language, parenting, and attachment. Dev. Psychopathol. 2019, 31, 587–599. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, E.; Johnson, S.L. Anger in psychological disorders: Prevalence, presentation, etiology and prognostic implications. Clin. Psychol. Rev. 2016, 46, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Owen, J.M. Transdiagnostic cognitive processes in high trait anger. Clin. Psychol. Rev. 2011, 31, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Wills, T.A.; Simons, J.S.; Sussman, S.; Knight, R. Emotional self-control and dysregulation: A dual-process analysis of pathways to externalizing/internalizing symptomatology and positive well-being in younger adolescents. Drug Alcohol Depend. 2015, 163, S37–S45. [Google Scholar] [CrossRef] [Green Version]
- Verona, E.; Bresin, K. Aggression proneness: Transdiagnostic processes involving negative valence and cognitive systems. Int. J. Psychophysiol. 2015, 98, 321–329. [Google Scholar] [CrossRef]
- Modecki, K.L.; Zimmer-Gembeck, M.J.; Guerra, N. Emotion regulation, coping, and decision making: Three linked skills for preventing externalizing problems in adolescence. Child Dev. 2017, 88, 417–426. [Google Scholar] [CrossRef] [Green Version]
- Beauchaine, T.P. Future Directions in emotion dysregulation and youth psychopathology. J. Clin. Child Adolesc. Psychol. 2015, 44, 875–896. [Google Scholar] [CrossRef] [Green Version]
- Chung, S.; Zhou, Q.; Eisenberg, N.; Wolchik, S. Threat appraisals and coping responses to stressors: Links to chinese children’s behavioral problems and social competence. J. Early Adolesc. 2017, 39, 280–305. [Google Scholar] [CrossRef]
- Compas, B.E.; Jaser, S.S.; Bettis, A.H.; Watson, K.H.; Gruhn, M.A.; Dunbar, J.P.; Williams, E.; Thigpen, J.C. Coping, emotion regulation, and psychopathology in childhood and adolescence: A meta-analysis and narrative review. Psychol. Bull. 2017, 143, 939–991. [Google Scholar] [CrossRef]
- Murray, A.L.; Obsuth, I.; Eisner, M.; Ribeaud, D. Shaping aggressive personality in adolescence: Exploring cross-lagged relations between aggressive thoughts, aggressive behaviour and self-control. Pers. Individ. Differ. 2016, 97, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Persson, M.; Sturup, J.; Belfrage, H.; Kristiansson, M. Self-reported violent ideation and its link to interpersonal violence among offenders with mental disorders and general psychiatric patients. Psychiatry Res. 2018, 261, 197–203. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Databases | Descriptors |
|---|---|
| Science Direct | Transdiagnostic and antisocial |
| Proquest | Transdiagnostic and aggression |
| Health & Medical Collection | Transdiagnostic and delinquency |
| Medline | Transdiagnostic and violence |
| Nursing and Allied health database | Transdiagnostic and anger |
| PsycArticles | Transdiagnostic and psychopathy |
| PsycBooks | Transdiagnostic and antisocial personality disorder |
| Psychology Database | Transdiagnostic and conduct disorder |
| PsycInfo | Transdiagnostic and dissocial disorder |
| PsycTest | Transdiagnostic and externalizing |
| Psicodoc |
| Authors | Country | N | Age in Years M(SD) | Male and Female % | AD Assessed | Measure | Transdiagnostic Variable | Key Findings |
|---|---|---|---|---|---|---|---|---|
| Carragher et al. [21] | Australia | 2175 | 13.3 (0.48) | M = 57.4% F = 42.6% | Externalizing symptoms (behavior and hiperactivity), alcohol consumption | Strengths and Difficulties Questionnaire (SDQ), Diagnostic Interview Schedule for Children | Impulsivity, Sensation seeking | They tested a model with a general psychopathology factor. Men show more externalizing symptoms. They point out that adolescents require treatments focused on decreasing impulsivity, and sensation-seeking. |
| Castellanos-Ryan et al. [22] | Canada | 2144 | 14.39 (0.77) | M = 49% F = 51% | Conduct Disorder (CD), Attention-Deficit/Hyperactivity Disorder (ADHD), Oppositional-Defiant Disorder (ODD) | Development and Well-Being Assessment interview (DAWBA), Alcohol Use Disorders Identification Test (AUDIT), Substance Use Risk Profile Scale (SURPS), NEO Five Factor Inventory (NEO FFI), Temperament and Character Inventory (TCI), Wechsler Intelligence Scale for Children—4th edition (WISC-IV), Test Automated Battery (CANTAB), Spatial Working Memory (SWM). | Externalizing personality factor | They present a two-factor personality model composed of an externalizing, and an internalizing one. The externalizing factor is associated with substance consumption, sensation-seeking, extraversion, and attentional biases to negative valence stimuli. The general factor is characterized by high disinhibition, impulsiveness, neuroticism, low affability, and performance when measuring intelligence. |
| Conway et al. [23] | Australia | 700 | 20 (NR) | M = 48.28% F = 51.72% | Personality Pathology PD Externalizing diagnosis (substance use and disruptive behavior disorder) | Structured Clinical Interview for DSM-IV (SCID), Structured Clinical Interview for DSM-IV Axis II Personality Disorders, Version 2.0 (SCID-II), Longitudinal Interval Follow-Up Examination (LIFE), Aggression, and Delinquency subscales of the Young Adult Self Report (YASR) | Externalizing personality factor | A two-factor model appears with a higher severity factor of the personality disorder (hierarchical MT). Significant correlations between personality disorder, aggression, and negative affect as a trait (both with r = 0.46) |
| Hamilton et al. [24] | USA | 304 | 18.20 (1.39) | M = 32% F = 68% | Externalizing problems | Behavioral Inhibition System/Behavioral Activation System Scales (BIS/BAS), Sensitivity to Punishment/Sensitivity to Reward Questionnaire (SPSRQ), Positive and Negative Affect Schedule (PANAS), Responses to Positive Affect Scale (RPAS), Life Events Scale (LES) and Life Events Interview (LEI), Beck Depression Inventory (BDI). | Positive and negative trait affect and emotion regulatory | Positive and negative affect as a trait is associated with an increase in emotional regulation strategies in positive and negative interpersonal events (externalizing problems). People with high negative affect traits would be at greater risk of increasing depressive symptoms, while in low positive affect traits, they would be at greater risk of interpersonal problems (people who decrease their positive responses decrease their functional interaction with others). |
| Hankin et al. [25] | USA | 571 | 13.58 (2.37) | M = 44.5% F = 55.5% | Oppositional Defiant Disorder or Conduct Disorder (ODD/CD) | Children’s Depression Inventory (CDI), Manifest Anxiety Scale for Children (MASC), Child Behavior Checklist (CBCL/YSR), Aggression scale of the Early Adolescent Temperament Questionnaire Revised (EATQ-R), Swanson, Nolan, and Pelham scale (MTA SNAPIV), Positive and Negative Affect Scale for Children (PANAS-C). | Temperament as a dimensional and latent psychopathological factor Positive and Negative Affect. Active control (effortful control). | Latent psychopathological lability was found in the pathologies (P Factor), both in the pre-adolescent and adolescent samples. The P factor was associated with low active control and high negative affect. In internalizing problems, a high negative and low positive affect was associated with the P factor, while in the externalizing problems, only a low active control was associated. |
| Hawes et al. [26] | USA | 1170 | 14–17 | M = 100% F = 0% | Psychopathy Alcohol use | Index of Social Position (ISP), Youth Psychopathic Traits Inventory-Short Version (YPI-S), Substance Use/Abuse Inventory (Quantity and Frequency Index, QFI), Proportion of supervised time (PST) | Psychopathic trait factor (Interpersonal, Callous-Unemotional, Impulsive-Irresponsible) | Variations were found in the change rates of late adolescent and young adult offenders, in terms of alcohol use and psychopathic characteristics (social relationship problems with peers and family, assuming adult roles, increased violence, and cruelty to others), especially the year following the start of consumption. |
| South et al. [27] | USA | 78 | 20.8 (2.23) | M = 29% F = 71% | High order externalizing factor: Aggression factor and Substance use factor | Inventory of Depression and Anxiety Symptoms (IDAS), Personality-based Externalizing Scale (EXT-P) | Positive-Negative Affect. | Cognitive (Distress, Control, and Coping) and affective (Positive and Negative Affect) reactions to everyday stressors are related to the internalizing spectrum and less to the externalizing spectrum, due to its low inhibitory emotional nature. They add that externalizing measures moderate the association between Distress and negative affect. People who are high in externalizing problems and have a high sense of control over their environment decrease their negative affect response. |
| Authors | Country | N | Age in Years M(SD) | Male and Female % | AD Asessed | Measure | Transdiagnostic Variable | Key Findings |
|---|---|---|---|---|---|---|---|---|
| Copeland et al. [28] | USA | 1420 | 9 to 16 (cohort: 9, 11, 13, 16) | M = 51% F = 49% | No AD was reported. | Child and Adolescent Psychiatric Assessment (CAPA), Child and Adolescent Burden Assessment | Tonic and phasic irritability as a transdiagnostic marker | Irritability decreases with age. Irritability does not vary between genders, nor is it associated with an increased risk of disruptive problems. It had little to do with a common profile of disruptive functioning in different psychiatric disorders. |
| Dadds et al. [29] | Australia | 195 | 10.52 (2.64) | M = 75.89% F = 24.11% | Oppositional Defiant Disorder or Conduct Disorder (ODD/CD), Predominately inattentive Attention Deficit Disorder or combined Attention DeficitHyperactivity Disorder (ADD and ADHD) | Child Adjustment on the Strengths and Difficulties Questionnaire (SDQ), Family and Child Experiences Survey (FACES), Griffith Empathy Measure (GEM) | Recognition of emotions as part of the transdiagnostic treatment based on the Emotional Regulation Trait: Emotional callus | Training in recognition of emotions had little impact on behavioral problems. Training in emotion recognition has a favorable impact on children on the autism spectrum. Children with high emotional callus showed little response to training in emotion recognition, although the empathic response increased. |
| Jonhson et al. [30] | USA | 312 | 18.77 (1.90) | M = 31% F = 69% | Externalizing symptoms of anger, hostility and physical aggression. Alcohol Use Disorder. | Aggression Questionnaire short Form (AQ), Mood and Anxiety Symptoms Questionnaire -Somatic Arousal subscale (MASQ-SA), Alcohol Use Disorder Identification Test (AUDIT), McLean Screening Instrument for Borderline Personality. Disorder (MSI-BPD) | Impulsive Reactivity (negative generalization, impulsive tendency, positive urgency, persistent lack of self-control, low scrupulosity, low reflective reaction) | Reactivity to emotion correlates with the externalizing symptoms of anger, hostility, and aggression, in the internalizing type with anxiety. The authors emphasize that emotional regulation is focused on decreasing impulsivity in the psychopathologies of both spectra. No association with alcoholism was found. |
| Masi et al. [31] | Italy | 108 | 9–15 years ODD 10.37 (1.8) CD 10.27 (1.9) | M = 83.33% F = 16.66% | Oppositional Defiant Disorder and Conduct Disorder (ODD/CD) | Schedule of Affective Disorders and Schizophrenia for School-Age Children Present and Lifetime Version (K-SADS-PL), Child Behavior Checklist (CBCL), Antisocial Process Screening. Device Parent version (APSD), Alabama Parenting. Questionnaire (APQ), Clinical Global Impression Severity (CGI-S), Children’s Global Assessment Scale (C-GAS). | Emotional dysregulation. Emotional callouses. | Participants with an Emotional dysregulation profile (low tolerance to frustration, impatience, immediate anger, rapid arousal by emotional reactions) scored higher on isolation, social problems, rule-breaking, and somatic complaints at CBCL. Higher scores appeared for narcissism and impulsivity, though not for emotional callouses. |
| Mclaughlin et al. [32] | USA | 1065 | 11–14 | M = 51.2% F = 48.8% | Aggressive behavior | Children’s Depression Inventory (CDI), Multidimensional Anxiety Scale for Children (MASC), Revised Peer Experiences Questionnaire (RPEQ), Children’s Eating Attitudes Test (ChEAT), Emotion Expression Scale for Children (EESC), Children’s Sadness Management Scale (CSMS), Anger Management Scale (CAMS), Children’s Response Styles Questionnaire (CRSQ). | Emotional dysregulation | They found that emotional dysregulation predicted aggression (β = 0.18, p < 0.001). In turn, psychopathology does not predict the appearance of emotional dysregulation; this provides evidence on the causal direction of this transdiagnostic variable in adolescent psychopathology. |
| Poon et al. [33] | USA | 134 | 12–14 years 12.61 (0.50) | M = 55% F = 45% | Substance abuse, Conduct Disorder (CD), Attention-Deficit/ Hyperactivity Disorder (ADHD), Oppositional-Defiant Disorder (ODD) | Salivary cortisol levels, Difficulties in Emotion Regulation Scale (DERS), Youth Risk Behavior Survey questionnaire (YRBS), Children’s Depression Inventory (CDI), Revised Children’s Manifest Anxiety Scale (RCMAS), Child Symptom Inventory (CSI) | Emotional dysregulation | Difficulties in emotional regulation and high cortisol predict substance abuse behaviors (β = −0.36, p < 0.001), although with a small effect size (OR = 0.70). These difficulties also predict the appearance of externalizing symptoms, in ODD (β = −0.74, p < 0.001), and ADHD (β = −1.15, p < 0.001), in CD or ADHD was not significant. |
| Shea et al. [34] | USA | 58 | 12.26 (0.98) | F = 100% | Externalizing disorders (Aggressive Behavior and Rule-Breaking Behavior) | Revised-Social Experiences Questionnaire-Self Report (SEQ), Child Behavior Checklist—Youth Self-Report (YSR), Avoidance and Fusion Questionnaire for Youth (AFQ-Y) | Experiential avoidance | Experiential avoidance is related to the victimization of relational peer aggression. It explains 8.3% of the variance in the externalizing problems (r = 0.36). These data indicate that experiential avoidance increases the risk of victimization in adolescent women. The study found more evidence for internalizing disorders (34.3% of variance); the authors suggest that this may be a form of avoidance behavior. |
| Fahlgren et al. [35] | USA | 492 | 18–55 M = 25.97(9.57) | F = 66.86% M = 33.14 | Intermittent explosive disorder | Structured diagnostic interview for DSM-IV (SCID-I), Structured interview for DSM-IV personality disorders (SIDP), IED interview (IED-I), Sadness and anger rumination inventory (SARI), Ruminative response scale (RRS-10), Toronto alexithymia scale (TAS-20), Reading the mind in the eyes task (RMET), Basic empathy scale (BES), Quality of life enjoyment and satisfaction questionnaire – short form (Q-LES-Q-SF), Life history of aggression interview (LHA) | Emotional dysregulation and anger-rumination | Intermittent explosive problems are associated with deficits in the regulation of emotions, with cognitive processes involved as altered processing in recognition of emotion, which is associated with aggressive, alexithymic responses and difficulty in empathy in recognition of emotions. |
| Authors | Country | N | Age in Years M(SD) | Male and Female % | AD Assessed | Measure | Transdiagnostic Variable | Key Findings |
|---|---|---|---|---|---|---|---|---|
| Conway et al. [36] | Australia | 705 | 20 | M = 86.5% F = 13.5% | Alcohol abuse/dependence Drug abuse/dependence | Structured Clinical Interview for DSM-IV (SCID), Structured Clinical Interview for DSM-IV Axis II Personality Disorders, Version 2.0 (SCID-II), Longitudinal Interval Follow-Up Examination (LIFE), Aggression, and Delinquency subscales of the Young Adult Self Report (YASR) | Perceptual biases: Cognitive Risk Marker | Perceptual biases, in response to stressors or emotional events, predict both internalizing and externalizing traits. Hyposensitivity to stressors increases the levels of the externalizing spectrum. Biases, aimed at decreasing the impact of stressor, increase externalizing symptoms (antisocial behavior and substance abuse). |
| Mclaughlin et al. [37] | USA | 1065 | 11–14 | M = 51.2% F = 48.8% | Aggressive behavior | Children’s Response Styles Questionnaire (CRSQ), Peer Experiences. Questionnaire (RPEQ), Children’s Depression Inventory (CDI), Multidimensional Anxiety Scale for Children (MASC). | Rumination | The study found that rumination is a mechanism to explain the appearance of internalizing symptoms and subsequent aggressive behavior in males. Rumination predicts aggressive behavior and vice versa. Thus, rumination underlies the transition from aggressive behavior to anxiety, but it also explains the emergence of aggressive behavior in adolescents with anxiety and depression. |
| Murray et al. [38] | Switzerland | 1306 | 17 | M = 50.45% F = 49.55% | Aggressive behavior, Attention deficit hyperactivity disorder (ADHD) | Violent Ideations Scale (VIS), Social Behaviour Questionnaire (SBQ) | Violent ideation (thoughts of killing, hitting, intimidation, causing pain and humiliation) | Violent ideations had moderate correlations with ADHD, proactive/indirect aggression, and reactive/physical aggression. However, the ADHD measure was the only one that did not correlate with mental health measures. The authors stress that they do not appear to be directly associated with the other externalizing problems and should, therefore, be considered a marker for mental health difficulties. |
| du Pont et al. [39] | USA | 764 | 22.8 (1.3) | M = 47.38% F = 52.62% | Externalizing Psychopathology | Rumination-Reflection Questionnaire (RRQ), Anger Rumination Scale (ARS), and nine EF laboratory tasks; Diagnostic Interview Schedule–IV (DIS-IV), Composite International Diagnostic Interview–Substance Abuse Module (CIDI-SAM). | Anger rumination, depressive rumination, inhibition, and executive function | Anger rumination is a set of cognitive skills represented in second-order thoughts that allow explaining the overlaps in the different psychopathologies, mainly the executive functions in externalizing disorders. |
| Studies | ST | SS | PS | RVI | TV | EP | MSA | TMD | TMTR | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Carragher et al. [21] | 3 | No | No | Yes | No | Yes | Yes | Yes | 7 | Mean |
| Castellanos-Ryan et al. [22] | 3 | No | Yes | Yes | No | Yes | Yes | No | 7 | Mean |
| Conway et al. [36] | 2 | No | No | Yes | No | No | Yes | No | 4 | Low |
| Conway et al. [23] | 3 | No | No | Yes | No | No | Yes | No | 5 | Low |
| Copeland et al. [28] | 2 | No | Yes | Yes | Yes | No | No | No | 5 | Low |
| Dadds et al. [29] | 3 | No | Yes | Yes | Yes | Yes | Yes | No | 8 | Mean |
| Hamilton et al. [24] | 3 | Yes | Yes | Yes | Yes | No | Yes | Yes | 9 | High |
| Hankin et al. [25] | 3 | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 | High |
| Hawes et al. [26] | 3 | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 | High |
| Jonhson et al. [30] | 2 | No | No | Yes | Yes | No | Yes | No | 5 | Low |
| Fahlgren et al. [35] | 3 | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 | High |
| Masi et al. [31] | 1 | No | Yes | Yes | Yes | Yes | Yes | Yes | 7 | Mean |
| Mclaughlin et al. [32] | 3 | No | Yes | Yes | Yes | No | Yes | No | 7 | Mean |
| Mclaughlin et al. [37] | 3 | No | Yes | Yes | Yes | No | Yes | No | 7 | Mean |
| Murray et al. [38] | 3 | Yes | Yes | Yes | Yes | Yes | Yes | No | 9 | High |
| Poon et al. [33] | 2 | No | Yes | Yes | Yes | Yes | Yes | No | 7 | Mean |
| Shea et al. [34] | 2 | No | Yes | Yes | Yes | No | No | No | 5 | Low |
| South et al. [27] | 3 | No | Yes | Yes | Yes | No | Yes | Yes | 8 | Mean |
| du Pont et al. [39] | 3 | No | Yes | Yes | Yes | Yes | Yes | Yes | 9 | High |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toro, R.; García-García, J.; Zaldívar-Basurto, F. Antisocial Disorders in Adolescence and Youth, According to Structural, Emotional, and Cognitive Transdiagnostic Variables: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3036. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093036
Toro R, García-García J, Zaldívar-Basurto F. Antisocial Disorders in Adolescence and Youth, According to Structural, Emotional, and Cognitive Transdiagnostic Variables: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(9):3036. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093036
Chicago/Turabian StyleToro, Ronald, Juan García-García, and Flor Zaldívar-Basurto. 2020. "Antisocial Disorders in Adolescence and Youth, According to Structural, Emotional, and Cognitive Transdiagnostic Variables: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 9: 3036. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093036