Five Challenges When Managing Mass Casualty or Disaster Situations: A Review Study



Abstract
:1. Introduction
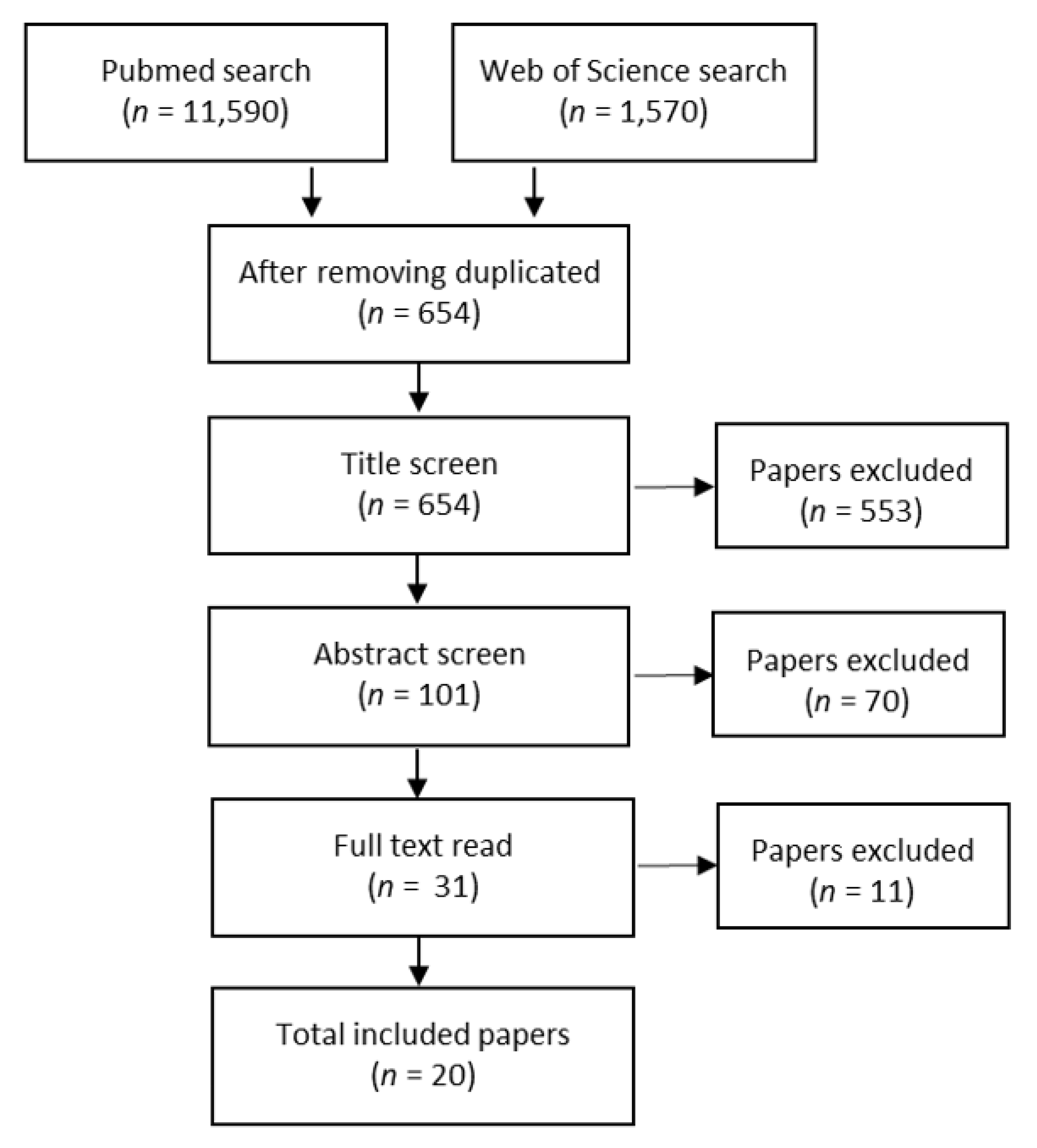
2. Method
3. Results
3.1. Challenge 1: To Identify the Situation and Deal with Uncertainty
3.2. Challenge 2: To Balance the Mismatch Between the Disaster Contingency Plan and the Reality
3.3. Challenge 3: To Establish a Functional Crisis Organisation
3.4. Challenge 4: To Adapt the Medical Response to the Actual and Overall Situation
3.5. Challenge 5: To Ensure a Resilient Response
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Centre for Research on the Epidemiology of Disasters (CRED). The Emergency Events Database; Institute Health and Society, Université Catholique de Louvain: Brussels, Belgium, 2016. Available online: https://www.emdat.be (accessed on 28 October 2019).
- Boin, A. Crises Management, 2nd ed.; Sage Publications: London, UK, 2008. [Google Scholar]
- Birnbaum, M.L.; Daily, E.K.; O´Rourke, A.O.; Loretti, A. Research and Evaluations of the Health Aspects of Disasters, Part 1: An Overview. Prehosp. Disaster Med. 2015, 30, 512–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimstad, R.; Braut, G.S. Literature review on medical incident commander. Prehosp. Disaster Med. 2015, 30, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Watson, S.K.; Rudge, J.W.; Coker, R. Health systems’ "surge capacity": state of the art and priorities for future research. Milbank Q. 2013, 91, 78–122. [Google Scholar] [CrossRef] [Green Version]
- Hick, J.L.; Koenig, K.L.; Barbisch, D.; Bey, T.A. Surge capacity concepts for health care facilities: the CO-S-TR model for initial incident assessment. Disaster Med. Public Health Prep. 2008, 2 (Suppl. 1), S51–S57. [Google Scholar] [CrossRef] [PubMed]
- Busby, S.; Witucki-Brown, J. Theory development for situational awareness in multi-casualty incidents. J. Emerg. Nurs. 2011, 37, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Hammad, K.S.; Arbon, P.; Gebbie, K.; Hutton, A. Moments of disaster response in the emergency department [ED]. Australas. Emerg. Nurs. J. 2017, 20, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Tranfield, D.; Denyer, D.; Smart, P. Towards a methodology for developing evidence-informed management knowledge by means of systematic review. Br. J. Manag. 2003, 14, 207–222. [Google Scholar] [CrossRef]
- Ardagh, M.W.; Richardson, S.K.; Robinson, V.; Than, M.; Gee, P.; Henderson, S.; Khodaverdi, L.; McKie, J.; Robertson, G.; Schroeder, P.P.; et al. The Initial Health-System Response to the Earthquake in Christchurch, New Zealand, in February, 2011. Lancet 2012, 379, 2109–2115. [Google Scholar] [CrossRef]
- Campion, E.M.; Juillard, C.; Knudson, M.M.; Dicker, R.; Cohen, M.J.; Mackersie, R.; Callcut, R.A. Reconsidering the Resources Needed for Multiple Casualty Events: Lessons Learned From the Crash of Asiana Airlines Flight 214. JAMA Surg. 2016, 151, 512–517. [Google Scholar] [CrossRef] [Green Version]
- Carli, P.T.; Telion, C. Paris City Disaster: Response to the Recent Terror Attacks and Lessons Learned. Curr. Trauma Rep. 2018, 4, 96–102. [Google Scholar] [CrossRef]
- Carli, P.; Pons, F.; Levraut, J.; Millet, B.; Tourtier, J.-P.; Ludes, B.; Lafont, A.; Riou, B. The French Emergency Medical Services After the Paris and Nice Terrorist Attacks: What Have We Learnt? Lancet 2017, 390, 2735–2738. [Google Scholar] [CrossRef]
- Chandler, T.; Abramson, D.M.; Panigrahi, B.; Schlegelmilch, J.; Frye, N. Crisis Decision-Making During Hurricane Sandy: An Analysis of Established and Emergent Disaster Response Behaviors in the New York Metro Area. Disaster Med. Public Health Prep. 2016, 10, 436–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Sayed, M.; Chami, A.F.; Hitti, E. Developing a Hospital Disaster Preparedness Plan for Mass Casualty Incidents: Lessons Learned From the Downtown Beirut Bombing. Disaster Med. Public Health Prep. 2018, 12, 379–385. [Google Scholar] [CrossRef]
- Hugelius, K.; Adolfsson, A.; Ortenwall, P.; Gifford, M. Being both helpers and victims; Health professionals’ experiences of working during a natural disaster. Prehospital Disaster Med. 2017, 32, 117–123. [Google Scholar] [CrossRef]
- Johal, S.; Mounsey, Z.; Brannelly, P.; Johnston, D. Nurse Perspectives on the Practical, Emotional, and Professional Impacts of Living and Working in Post-Earthquake Canterbury, New Zealand. Prehospital Disaster Med. 2015, 31, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Safi-Keykaleh, M.; Sohrabizadeh, S. The Emergency Medical System (EMS) Response to Iraqi pilgrims’ Bus Crash in Iran: A Case Report. BMC Emerg. Med. 2019, 19, 38. [Google Scholar] [CrossRef]
- Lesaffre, X.; Tourtier, J.-P.; Violin, Y.; Frattini, B.; Rivet, C.; Stibbe, O.; Faure, F.; Godefroy, A.; Gallet, J.-C.; Ausset, S. Remote Damage Control During the Attacks on Paris. J. Trauma Acute Care Surg. 2017, 82, S107–S113. [Google Scholar] [CrossRef]
- Lyon, R.; Sanders, J. The Swiss Bus Accident on 13 March 2012: Lessons for Pre-Hospital Care. Crit. Care 2012, 16, 138. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.; Powell, D. Special Considerations for Mass Violence Events in Senior Living Facilities: A Case Report on the Pinelake Health and Rehab Center Shooting. Disaster Med. Public Health Prep. 2017, 11, 150–152. [Google Scholar] [CrossRef] [Green Version]
- Massalou, D.; Ichai, C.; Mariage, D.; Baque, P. Terrorist attack in Nice- The expereince of general surgeons. J. Visc. Surg. 2019, 156, 17–22. [Google Scholar] [CrossRef]
- Nakagawa, A.; Furukawa, H.; Konishi, R.; Kudo, D.; Matsumura, T.; Sato, D.; Abe, Y.; Washio, T.; Arafune, T.; Yamanouchi, S.; et al. The Great East Japan Earthquake. Lessons learned at Tokohu Univeristy Hospital During the First 72 Hours. IEEE Pulse Mag. 2013, 4, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Sabah, S.A.; Alsharqawi, N.; Haddad, E.A. The aftermath of the Kuwait mosque bombing: A retrospective cohort analysis and lessons learned. Int. J. Surg. 2018, 56, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Solla, F.; Carboni, J.; Breaud, J.; Babe, P.; Brezac, G.; Chivoret, N.; Dupont, A.; Fernandez, A. July 14, 2016, Terror Attack in Nice, France. Acad. Pediatr. 2018, 18, 361–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sollid, S.J.M.; Rimstad, R.; Rehn, M.; Nakstad, A.R.; Tomlinson, A.-E.; Strand, T.; Heimdal, H.J.; Nilsen, J.E.; Sandberg, M. Oslo Government District Bombing and Utøya Island Shooting July 22, 2011: The Immediate Prehospital Emergency Medical Service Response. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 3. [Google Scholar] [CrossRef] [Green Version]
- Subedi, S.; Sharma, G.N.; Dahal, S.; Banjara, M.R.; Pandey, B.D. The Health Sector Response to the 2015 Earthquake in Nepal. Disaster Med. Public Health Prep. 2018, 12, 543–547. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, Y.; Liu, X.; Zhang, Y. Rescue Efforts Management and Characteristics of Casualties of the Wenchuan Earthquake in China. Emerg. Med. J. 2011, 28, 618–622. [Google Scholar] [CrossRef]
- Zhang, J.-J.; Wang, T.-B.; Fan, D.; Zhang, J.; Jiang, B.-G. Medical Response to the Tianjin Explosions: Lessons Learned. Disaster Med. Public Health Prep. 2018, 12, 411–414. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Moynihan, D.P. Learning under Uncertainty: Networks in Crisis Management. Public Adm. Rev. 2008, 68, 350–365. [Google Scholar] [CrossRef] [Green Version]
- Paté-Cornell, E. On “Black Swans” and “Perfect Storms”: Risk Analysis and Management When Statistics Are Not Enough. Risk Anal. 2012, 32, 1823–1833. [Google Scholar] [CrossRef]
- Quarantelli, E. Disaster Crisis Management; Disaster Research Center, University of Delaware: Newark, DE, USA, 1986. [Google Scholar]
- Coppola, D.P. Introduction to International Disaster Management, 2nd ed.; Elsevier Inc.: Burlington, VT, USA, 2011; p. 9. [Google Scholar]
- Glick, J.A.; Barbera, J.A.; Barbara, J.A. Moving from Situational Awareness to Decisions During Disaster Response: Transition to Decision Making. J. Emerg. Manag. 2013, 11, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.G.; Trelles, M.; Dominguez, L.; Gupta, S.; Burnham, G.; Kushner, A.L. Surgical Skills Needed for Humanitarian Missions in Resource-Limited Settings: Common Operative Procedures Performed at Médecins Sans Frontières Facilities. Surgery 2014, 156, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Brewin, C.R.; Kaniasty, K.; La Greca, A.M. Weighing the Costs of Disaster. Psychol. Sci. Public Interest 2010, 11, 1–49. [Google Scholar] [CrossRef] [Green Version]
- Nomura, S.; Parsons, A.J.; Hirabayashi, M.; Kinoshita, R.; Liao, Y.; Hodgson, S. Social Determinants of Mid- to Long-Term Disaster Impacts on Health: A Systematic Review. Int. J. Disaster Risk Reduct. 2016, 16, 53–67. [Google Scholar] [CrossRef]
- Boris, B.; Katherine, P.O.; John, M.; Sabah, A.; Ratnasabapathipillai, K.; Kathryn, B. Up Scaling Mental Health and Psychosocial Services in a Disaster Context: Lessons Learnt from the Philippine Region Hardest Hit by Typhoon Haiyan. Int. J. Med. Med. Sci. 2016, 8, 112–119. [Google Scholar] [CrossRef] [Green Version]
- North, C.S.; Pfefferbaum, B. Mental Health Response to Community Disasters. JAMA 2013, 310, 507–518. [Google Scholar] [CrossRef]
- Quevillon, R.P.; Gray, B.L.; Erickson, S.E.; Gonzalez, E.D.; Jacobs, G.A. Helping the Helpers: Assisting Staff and Volonteer Workers Before, During, and After Disaster Relief Operations. J. Clin. Psychol. 2016, 72, 1348–1363. [Google Scholar] [CrossRef] [PubMed]
- International Society for Traumatic Stress Studies [ISTSS]. Posttraumatic Stress Disorder Prevention and Treatment Guidelines. Methodology and Recommendations. Available online: https://istss.org/getattachment/Treating-Trauma/New-ISTSS-Prevention-and-Treatment-Guidelines/ISTSS_PreventionTreatmentGuidelines_FNL-March-19-2019.pdf.aspx. 2019 (accessed on 19 March 2019).
- Rose, S.C.; Bisson, J.; Churchill, R.; Wessly, S. Pshycological debriefing for preventing post traumatic stress disorder (PTSD). Cochrane Database Syst. Rev. 2002, CD000560. [Google Scholar] [CrossRef]
- Gowing, J.; Walker, K.N.; Elmer, S.; Cummings, E. Disaster Preparedness Among Health Professionals and Support Staff: What Is Effective? An Integrative Literature Review. Prehospital Disaster Med. 2017, 32, 321–328. [Google Scholar] [CrossRef]
- Christensen, T.; Laegreid, P.; Rykkja, L.H.; Lægreid, P. After a Terrorist Attack: Challenges for Political and Administrative Leadership in Norway. J. Conting. Crisis Manag. 2013, 21, 167–177. [Google Scholar] [CrossRef] [Green Version]
- Donahue, S.; Tuohy, R.V. Lessons We Don´t Learn; A Study of the Lessons from Disasters, Why we repeat them, and how we can learn them. Homel. Secirity Aff. 2006, 2, 1–28. [Google Scholar]
- Smit, D.; Elliot, D. Exploring the Barriers to Learning from Crises; Organiztional Learning and Crizes. Manag. Learn. 2007, 38, 519–538. [Google Scholar] [CrossRef]
- Gerdin, M.; Clarke, M.; Allen, C.; Kayabu, B.; Summerskill, W.; DeVane, D.; MacLachlan, M.; Spiegel, P.; Ghosh, A.; Zachariah, R.; et al. Optimal Evidence in Difficult Settings: Improving Health Interventions and Decision Making in Disasters. PLoS Med. 2014, 11, e1001632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steigenberger, N. Organizing for the Big One: A Review of Case Studies and a Research Agenda for Multi-Agency Disaster Response. J. Conting. Crisis Manag. 2016, 24, 60–72. [Google Scholar] [CrossRef]


{kind=link}
| Database | Search Terms | Number of Records |
|---|---|---|
| PubMed database 11 October 2019 Language: English Publication dates: 2009–2019 | S1: (disaster OR mass-casualty incident) | 31,844 |
| S2: S1 AND (case-report OR lessons learned) | 1118 | |
| S4: (terrorist attack *) AND (experience *) OR (case-report OR lessons learned OR experience) | 19 | |
| S5: (flight crash) AND (experience *) OR (case-report OR lessons learned) | 9 | |
| S6: (bus accident) AND (experience *) OR (case-report OR lessons learned) | 13 | |
| In total | 1159 | |
| Web of Science 11 October 2019 Language: English Source: Article Publication dates: 2009–2019 | S1: (disaster OR mass-casualty incident) | 35,271 |
| S2: S1 AND (case-report OR lessons learned) | 1500 | |
| S4: (terrorist attack *) AND (experience *) OR (case-report OR lessons learned OR experience) | 29 | |
| S5: (flight crash) AND (experience *) OR (case-report OR lessons learned) | 23 | |
| S6: (bus accident) AND (experience *) OR (case-report OR lessons learned) | 18 | |
| In total | 1570 | |
| After reducing duplicates | 654 |
| Authors * | Year of Publication | Type of Event | Number of Affected (Dead/Injured/Not Injured) ** | Country | Type of Paper *** | Quality Appraisal **** |
|---|---|---|---|---|---|---|
| Ardagh et al. [10] | 2012 | Earthquake | 182/6659/NA | New Zealand | Review | HQ |
| Campion et al. [11] | [11] 2016 | Airplane crash | 3/192/112 | USA | Original research | AQ |
| Carli et al. [12] | 2018 | Explosion and shooting | 96/115/NA | France | Case report | AQ |
| Carli et al. [13] | 2017 | Explosion, shooting and vehicle-ramming attack | 137/413/NA and 87/458/NA | France | Viewpoint | AQ |
| Chandler [14] | 2016 | Storm | 130/NA/NA | USA | Original research | HQ |
| El Sayed et al. [15] | 2018 | Explosion | 3/32/NA | Lebanon | Concept paper | AQ |
| Hugelius et al. [16] | 2017 | Storm | 8000/45,000/NA | The Philippines | Original paper | AQ |
| Johal et al. [17] | 2016 | Earthquake | 187/6000/NA | New Zealand | Original Paper | |
| Safi Keykaleh [18] | 2019 | Bus accident | 11/35/NA | Iran | Case report | AQ |
| Lesaffre et al. [19] | 2017 | Explosion and shooting | 130/495/NA | France | Commentary | AQ |
| Lyon & Sanders [20] | 2012 | Bus accident | 28/24/0 | Switzerland | Commentary | AQ |
| Martin et al. [21] | 2017 | Shooting | 7/3/110 | USA | Report from the field | AQ |
| Massalou et al. [22] | 2019 | Vehicle-ramming attack | 86/458/NA | France | Original paper | HQ |
| Nakagawa et al. [23] | 2013 | Earthquake and tsunami | 9512/3792/NA | Japan | Lessons learned | AQ |
| Sabah et al. [24] | 2018 | Explosion | 27/227/NA | Saudi Arabia | Original research | AQ |
| Solla et al. [25] | 2018 | Vehicle-ramming attack | 86/500/NA | France | Commentary | AQ |
| Sollid et al. [26] | 2012 | Explosion and shooting | 77/NA/NA | Norway | Original research | HQ |
| Subedi et al [27] | 2018 | Earthquake | 8790/22,300/NA | Nepal | Report from the field | AQ |
| Zhang et al. [28] | 2011 | Earthquake | 69,000/NA/NA | China | Original research | HQ |
| Zhang et al. [29] | 2018 | Explosion | 173/798/4000 | China | Report from the field | AQ |
| Author (year) * | Challenge 1: To Identify the Situation and Deal with Uncertainty | Challenge 2: To Balance the Mismatch Between the Contingency Plan and the Reality | Challenge 3: To Establish a Functional Crisis Organisation | Challenge 4: To Adapt the Medical Response to the Actual and Overall Situation | Challenge 5: To Ensure a Resilient Response |
|---|---|---|---|---|---|
| Ardagh et al. (2012) [10] | X | X | X | X | X |
| Campion et al. (2016) [11] | X | ||||
| Carli et al. (2018) [12] | X | X | X | X | X |
| Carli et al. (2017) [13] | X | X | X | ||
| Chandler et al. (2016) [14] | X | X | X | X | |
| El Sayed et al. (2018) [15] | X | X | X | X | X |
| Hugelius et al. (2017) [16] | X | X | X | X | |
| Johal et al. (2016) [17] | X | X | |||
| Safi Keykaleh (2019) [18] | X | X | |||
| Lesaffre et al. (2017) [19] | X | X | |||
| Lyon & Sanders (2012) [20] | X | X | |||
| Martin et al. (2017) [21] | X | X | |||
| Massalou et al. (2019) [22] | X | X | |||
| Nakagawa et al. (2013) [23] | X | X | X | X | X |
| Sabah (2018) [24] | X | X | X | X | X |
| Solla et al. (2018) [25] | X | X | X | ||
| Sollid et al. (2012) [26] | X | X | X | X | X |
| Subedi et al. (2018) [27] | X | X | X | ||
| Zhang et al. (2011) [28] | X | X | X | X | |
| Zhang et al. (2018) [29] | X | X |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hugelius, K.; Becker, J.; Adolfsson, A. Five Challenges When Managing Mass Casualty or Disaster Situations: A Review Study. Int. J. Environ. Res. Public Health 2020, 17, 3068. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093068
Hugelius K, Becker J, Adolfsson A. Five Challenges When Managing Mass Casualty or Disaster Situations: A Review Study. International Journal of Environmental Research and Public Health. 2020; 17(9):3068. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093068
Chicago/Turabian StyleHugelius, Karin, Julia Becker, and Annsofie Adolfsson. 2020. "Five Challenges When Managing Mass Casualty or Disaster Situations: A Review Study" International Journal of Environmental Research and Public Health 17, no. 9: 3068. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093068