Risk Factors for Duty-Related Posttraumatic Stress Disorder among Police Officers in the Mt. Ontake Eruption Disaster-Support Task Force



Abstract
:1. Introduction
2. Participants and Methods
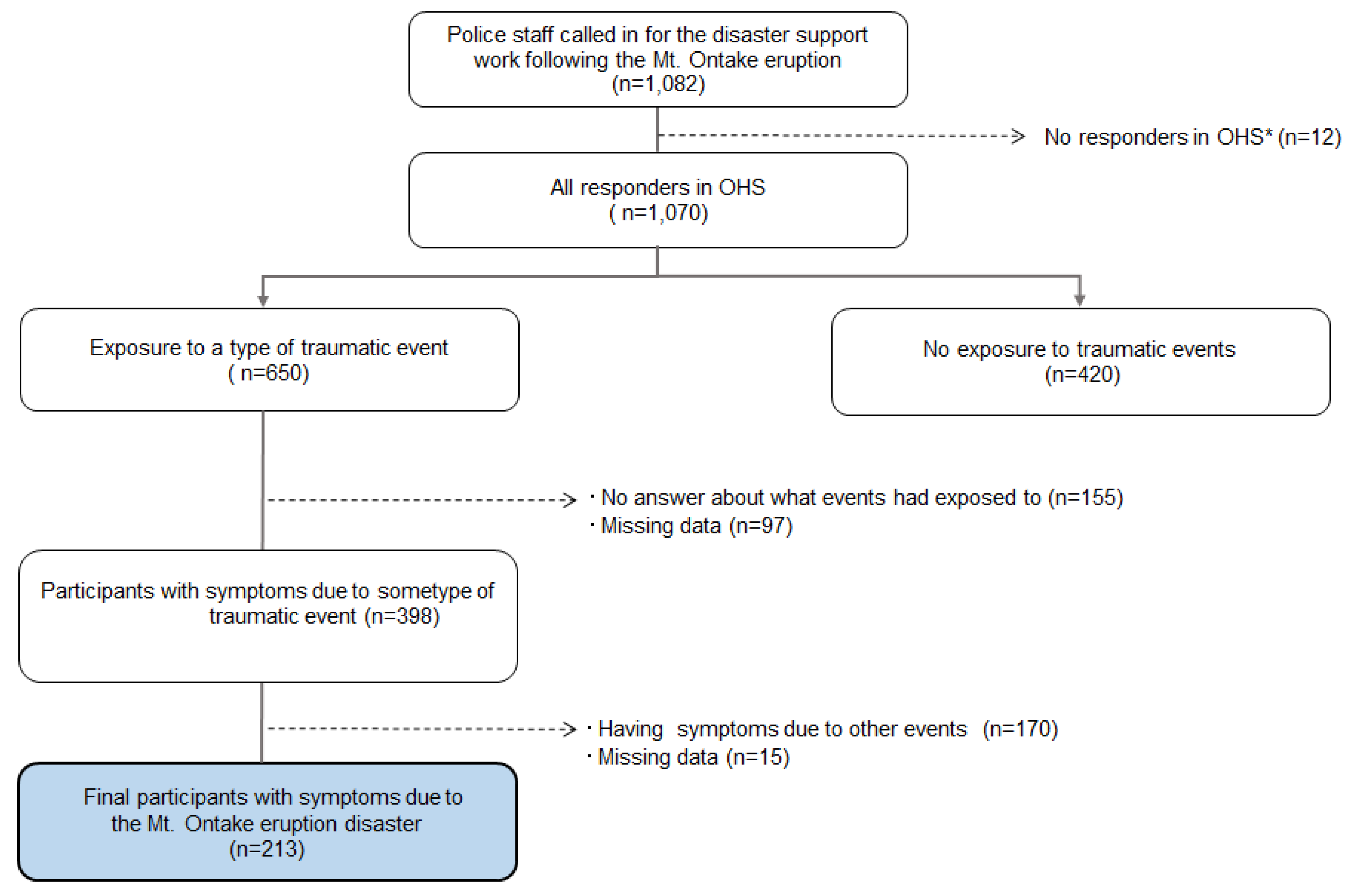
2.1. Setting and Participants
2.2. Measures
2.2.1. Traumatic Events and PTSD Symptom Severity
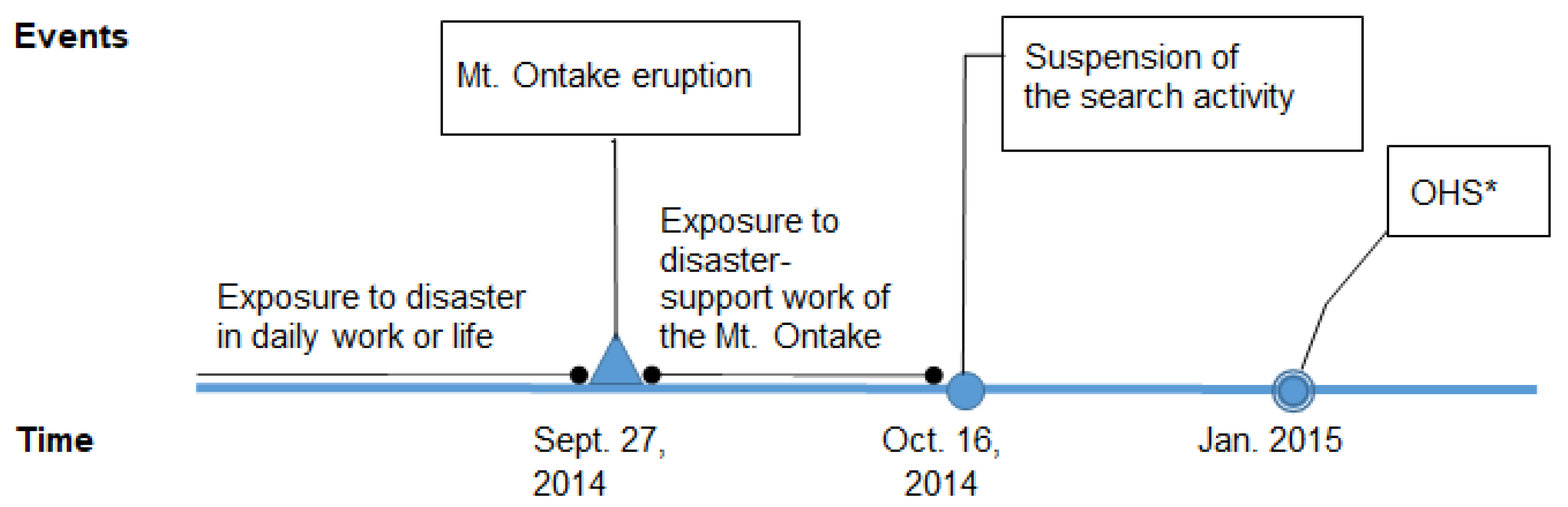
2.2.2. The Peritraumatic Situations of the Participants with PTSD Symptoms from the Mt. Ontake Eruption Disaster
2.2.3. Resilience
2.3. Sociodemographic Factors
2.4. Statistical Analyses
2.5. Ethical Approval
3. Results
3.1. The Participants’ Characteristics
3.2. The Relationship between PTSD Symptoms and the Participants’ Peritraumatic Situations
4. Discussion
4.1. The Severity of the PTSD Indicated by the PDS
4.2. The Relationship between PTSD Symptoms Due to the Mt. Ontake Eruption Disaster and the Participants’ Peritraumatic Disaster-Support Work
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Oshiro, K.; Watanabe, Y. Medical Problems of Casualties and Rescurers on Mt.Ontake Volcanic Eruption. Jpn. J. Mt. Med. 2015, 35, 21–28. [Google Scholar]
- West, C.; Bernard, B.; Mueller, C.; Kitt, M.; Driscoll, R.; Tak, S. Mental health outcomes in police personnel after Hurricane Katrina. J. Occup. Environ. Med. 2008, 50, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Epstein, R.S.; Fullerton, C.S.; Ursano, R.J. Posttraumatic stress disorder following an air disaster: A prospective study. Am. J. Psychiatry 1998, 155, 934–938. [Google Scholar] [CrossRef] [PubMed]
- Fullerton, C.S.; Ursano, R.J.; Wang, L.M. Acute stress disorder posttraumatic stress disorder, and depression in disaster or rescue workers. Am. J. Psychiat. 2004, 161, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Berger, W.; Coutinho, E.S.; Figueira, I.; Marques-Portella, C.; Luz, M.P.; Neylan, T.C.; Marmar, C.R.; Mendlowicz, M.V. Rescuers at risk: A systematic review and meta-regression analysis of the worldwide current prevalence and correlates of PTSD in rescue workers. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Marmar, C.R.; McCaslin, S.E.; Metzler, T.J.; Best, S.; Weiss, D.S.; Fagan, J.; Liberman, A.; Pole, N.; Otte, C.; Yehuda, R.; et al. Predictors of posttraumatic stress in police and other first responders. Ann. N. Y. Acad. Sci. 2006, 1071, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Davidson, J.R.; Hughes, D.; Blazer, D.G.; George, L.K. Post-traumatic stress disorder in the community: An epidemiological study. Psychol. Med. 1991, 21, 713–721. [Google Scholar] [CrossRef]
- Kessler, R.C.; Sonnega, A.; Bromet, E.; Hughes, M.; Nelson, C.B. Posttraumatic-Stress-Disorder In the National Comorbidity Survey. Arch. Gen. Psychiatry 1995, 52, 1048–1060. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.S.; Brunet, A.; Best, S.R.; Metzler, T.J.; Liberman, A.; Pole, N.; Fagan, J.A.; Marmar, C.R. Frequency and Severity Approaches to Indexing Exposure to Trauma: The Critical Incident History Questionnaire for Police Officers. J. Trauma. Stress 2010, 23, 734–743. [Google Scholar] [CrossRef] [Green Version]
- Chopko, B.A.; Palmieri, P.A.; Adams, R.E. Critical Incident History Questionnaire Replication: Frequency and Severity of Trauma Exposure Among Officers From Small and Midsize Police Agencies. J. Trauma. Stress 2015, 28, 157–161. [Google Scholar] [CrossRef]
- Liberman, A.M.; Best, S.R.; Metzler, T.J.; Fagan, J.A.; Weiss, D.S.; Marmar, C.R. Routine occupational stress and psychological distress in police. Policing Int. J. Police Strat. Manag. 2002, 25, 421–439. [Google Scholar] [CrossRef]
- Maguen, S.; Metzler, T.J.; McCaslin, S.E.; Inslicht, S.S.; Henn-Haase, C.; Neylan, T.C.; Marmar, C.R. Routine Work Environment Stress and PTSD Symptoms in Police Officers. J. Nerv. Ment. Dis. 2009, 197, 754–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Read, J.P.; Griffin, M.J.; Wardell, J.D.; Ouimette, P. Coping, PTSD symptoms, and alcohol involvement in trauma-exposed college students in the first three years of college. Psychol. Addict. Behav. 2014, 28, 1052–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chopko, B.A.; Palmieri, P.A.; Adams, R.E. Associations Between Police Stress and Alcohol Use: Implications for Practice. J. Loss Trauma 2013, 18, 482–497. [Google Scholar] [CrossRef]
- Noda, T.; Aso, K.; Tsujimoto, S. Alcohol related problems following a disaster: Knowledge gained from the Great 1995 Hanshin Earthquake. Jpn. J. Clin. Psychiatry 2012, 41, 1285–1291. [Google Scholar]
- Matsushita, S.; Higuchi, S. Alcohol Consumption and Alcohol Use Disorders after Disasters. Jpn. J. Trauma. Stress 2013, 10, 175–181. [Google Scholar]
- Zvolensky, M.J.; Farris, S.G.; Kotov, R.; Schechter, C.B.; Bromet, E.; Gonzalez, A.; Vujanovic, A.; Pietrzak, R.H.; Crane, M.; Kaplan, J.; et al. Posttraumatic stress symptoms and smoking among World Trade Center disaster responders: A longitudinal investigation. Compr. Psychiatry 2015, 63, 46–54. [Google Scholar] [CrossRef]
- Bonanno, G.A. Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Bonanno, G.A.; Westphal, M.; Mancini, A.D. Resilience to Loss and Potential Trauma. In Annual Review of Clinical Psychology; NolenHoeksema, S., Cannon, T.D., Widiger, T., Eds.; Annual Reviews: Palo Alto, CA, USA, 2011; Volume 7, pp. 511–535. [Google Scholar]
- Fushimi, M. Posttraumatic stress in professional firefighters in Japan: Rescue efforts after the Great East Japan Earthquake (Higashi Nihon Dai-Shinsai). Prehosp. Disaster Med. 2012, 27, 416–418. [Google Scholar] [CrossRef]
- Benedek, D.M.; Fullerton, C.; Ursano, R.J. First responders: Mental health consequences of natural and human-made disasters for public health and public safety workers. Annu. Rev. Public Health 2007, 28, 55–68. [Google Scholar] [CrossRef]
- Foa, E.B.; Cashman, L.; Jaycox, L.; Perry, K. The validation of a self-report measure of posttraumatic stress disorder: The Posttraumatic Diagnostic Scale. Psychol. Assess. 1997, 9, 445–451. [Google Scholar] [CrossRef]
- McCarthy, S. Post-traumatic Stress Diagnostic Scale (PDS). Occup. Med. (Lond.) 2008, 58, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagae, N.; Hirohata, S.; Shimura, Y.; Yamada, S.; Foa, E.B.; Nedate, K.; Kim, Y. Development of the Japanese version of the Posttraumatic Diagnostic Scale: Ascertaining its Reliability and Validity Among University Student. Japanese J. Trauma. Stress 2007, 5, 51–56. [Google Scholar]
- Figley, C.R. Compassion fatigue as secondary traumatic stress disorder: An overview. In Compassion fatigue: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized; Brunner/Mazel Psychological Stress Series, No. 23; Brunner/Mazel, P., Ed.; Brunner-Routledge: New York, NY, USA, 1995; pp. 1–20. [Google Scholar]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Ito, M.; Nakajima, S.; Akemi, S.; Yoshiharu, K. Reliability and validity of Japanese version of Conner-Davidson Resilience scale(CD-RISC): Consideration among general adults and university students. Natl. Inst. Ment. Health Natl. Cent. Neurol. Psychiatry 2009 2010, 22, 294. [Google Scholar]
- Kessler, R.C. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, N.; Tsuchiya, M.; Umeda, M.; Koenen, K.C.; Kessler, R.C.; World Mental Health Japan Survey. Trauma and posttraumatic stress disorder in Japan: Results from the World Mental Health Japan Survey. J. Psychiatr Res. 2014, 53, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.; Muller, J.; Maercker, A. Trauma and posttraumatic reactions in German development aid workers: Prevalences and relationship to social acknowledgement. Int. J. Soc. Psychiatry 2006, 52, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Howgego, I.M.; Owen, C.; Meldrum, L.; Yellowlees, P.; Dark, F.; Parslow, R. Posttraumatic stress disorder: An exploratory study examining rates of trauma and PTSD and its effect on client outcomes in community mental health. BMC Psychiatry 2005, 5, 17. [Google Scholar] [CrossRef] [Green Version]
- Fullerton, C.S.; McCarroll, J.E.; Ursano, R.J.; Wright, K.M. Psychological responses of rescue workers: Fire fighters and trauma. Am. J. Orthopsychiatry 1992, 62, 371–378. [Google Scholar] [CrossRef]
- Galea, S.; Nandi, A.; Vlahov, D. The epidemiology of post-traumatic stress disorder after disasters. Epidemiol. Rev. 2005, 27, 78–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Bromet, E.J.; Hobbs, M.J.; Clouston, S.A.; Gonzalez, A.; Kotov, R.; Luft, B.J. DSM-IV post-traumatic stress disorder among World Trade Center responders 11-13 years after the disaster of 11 September 2001 (9/11). Psychol. Med. 2016, 46, 771–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osawa, T.; Kato, H. Effect of Critical Incident Stress among rescue workers who were dispatched to the Great East Japan Earthquake distress area. Jpn. Bull. Trauma. Stress Stud. 2011, 7, 25–32. [Google Scholar]
- Nojima, M.; Okamoto, H.; Kamiyama, M.; Wada, T.; Tsunoda, T. Cross-sectional study of critical incident stress and mental health among firefighters dispatched to areas affected by the Great East Japan Earthquake. J. Kyorin Med. Soc. 2013, 44, 13–23. [Google Scholar]
- Nishi, D.; Koido, Y.; Nakaya, N.; Sone, T.; Noguchi, H.; Hamazaki, K.; Hamazaki, T.; Matsuoka, Y. Peritraumatic distress, watching television, and posttraumatic stress symptoms among rescue workers after the Great East Japan earthquake. PLoS ONE 2012, 7, e35248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolin, D.F.; Foa, E.B. Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychol. Bull. 2006, 132, 959–992. [Google Scholar] [CrossRef]
- Olff, M.; Langeland, W.; Draijer, N.; Gersons, B.P. Gender differences in posttraumatic stress disorder. Psychol. Bull. 2007, 133, 183–204. [Google Scholar] [CrossRef]
- Bowler, R.M.; Han, H.; Gocheva, V.; Nakagawa, S.; Alper, H.; DiGrande, L.; Cone, J.E. Gender differences in probable posttraumatic stress disorder among police responders to the 2001 World Trade Center terrorist attack. Am. J. Ind. Med. 2010, 53, 1186–1196. [Google Scholar] [CrossRef]
- Greinacher, A.; Derezza-Greeven, C.; Herzog, W.; Nikendei, C. Secondary traumatization in first responders: A systematic review. Eur J. Psychotraumatol. 2019, 10, 1562840. [Google Scholar] [CrossRef] [Green Version]
- Kato, H.; Asukai, N. A Large Scale Survey of Fire Fighters following the 1995 Kobe Earthquake. Jpn. J. Trauma. Stress 2004, 2. [Google Scholar]
- Hargrave, P.A.L. Sudden death: The impact of the immediate aftermath on police officers, victim support workers, and bereaved survivors. Ph.D. Thesis, Massey University, Wellington, New Zealand, 2010. [Google Scholar]
- Nagamine, M.; Shigemura, J.; Fujiwara, T.; Waki, F.; Tanichi, M.; Saito, T.; Toda, H.; Yoshino, A.; Shimizu, K. The relationship between dispositional empathy, psychological distress, and posttraumatic stress responses among Japanese uniformed disaster workers: A cross-sectional study. BMC Psychiatry 2018, 18, 328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, E.; Avalos, G.; Dowling, M. Secondary traumatic stress among emergency nurses: A cross-sectional study. Int. Emerg. Nurs. 2015, 23, 53–58. [Google Scholar] [CrossRef]
- Kunst, M.J.; Saan, M.C.; Bollen, L.J.; Kuijpers, K.F. Secondary traumatic stress and secondary posttraumatic growth in a sample of Dutch police family liaison officers. Stress Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Hatzenbuehler, M.L.; Grant, B.F.; Hasin, D.S. Stress and Alcohol Epidemiologic Evidence. Alcohol Res. Curr. Rev. 2012, 34, 391–400. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Category | n | (%) | |
|---|---|---|---|---|
| Sociodemographic factors | ||||
| Sex | ||||
| Male | 194 | (91.1) | ||
| Female | 19 | (8.9) | ||
| Age | ||||
| 20–29 | 63 | (29.6) | ||
| 30–39 | 87 | (40.8) | ||
| 40–49 | 45 | (21.1) | ||
| 50+ | 18 | (8.5) | ||
| Marital status: | ||||
| Married | 83 | (39.0) | ||
| Unmarried | 128 | (60.1) | ||
| Bereavement or divorced | 2 | (0.9) | ||
| No answer | 0 | (0.0) | ||
| Living situation: | ||||
| Living alone | 96 | (45.1) | ||
| Living with someone | 117 | (54.9) | ||
| Job title: | ||||
| Police officer | 179 | (84.0) | ||
| Office staff | 27 | (12.7) | ||
| No answer | 7 | (3.3) | ||
| Years of work experience: | ||||
| 1–9 | 103 | (48.4) | ||
| 10–19 | 72 | (33.8) | ||
| 20+ | 38 | (17.8) | ||
| PTSD symptom severity rating: | ||||
| No rating, 0 | 156 | (73.2) | ||
| Mild, 1–10 | 55 | (25.8) | ||
| Moderate, 11–20 | 2 | (0.9) | ||
| Moderate to severe, 21–35 | 0 | (0.0) | ||
| Severe, 36+ | 0 | (0.0) | ||
| Peritraumatic situations | ||||
| Disaster support duties: | ||||
| Search and rescue or transportation or autopsy | None | 100 | (46.9) | |
| Yes | 113 | (53.1) | ||
| Support for the victim’s family or the remains of victims | None | 139 | (65.3) | |
| Yes | 74 | (34.7) | ||
| Cumulative days on the work | <7 days | 90 | (42.3) | |
| ≥7 days | 123 | (57.7) | ||
| Stressors and supports before the disaster: | ||||
| Work stress | None | 170 | (79.8) | |
| Have | 43 | (20.2) | ||
| Family or personal stress | None | 161 | (75.6) | |
| Have | 52 | (24.4) | ||
| Supporter for usual work | None | 37 | (17.4) | |
| Yes | 176 | (82.6) | ||
| Supporter for family life or personal problems | None | 46 | (21.6) | |
| Yes | 167 | (78.4) | ||
| Stress relief behavior after the disaster: | ||||
| Conversation with family or colleagues | None | 64 | (30.0) | |
| Yes | 149 | (70.0) | ||
| Drinking or smoking | None | 164 | (77.0) | |
| Yes | 49 | (23.0) | ||
| Resilience | ||||
| CD-RISC score: | ||||
| High, 62+ | 68 | (31.9) | ||
| Medium, 50–61 | 83 | (39.0) | ||
| Low, <50 | 62 | (29.1) | ||
| CD-RISC: Connor–Davidson Resilience Scale | ||||
| Variable | Category | Crude Model | Adjusted Model | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | OR | (95%CI) | p-Value | p for Trend | OR | (95%CI) | p-Value | p for Trend | ||
| Sociodemographic factors | ||||||||||
| Sex | ||||||||||
| Male | 194 | 1.00 | 1.00 | |||||||
| Female | 19 | 3.48 | (1.33–9.06) | 0.01 | 3.58 | (1.19–10.77) | 0.02 | |||
| Living situation | ||||||||||
| Live alone | 96 | 1.00 | 1.00 | |||||||
| Live with someone | 117 | 0.80 | (0.44–1.47) | 0.44 | 0.79 | (0.38–1.65) | 0.53 | |||
| Years of work experience | ||||||||||
| 1–9 | 103 | 1.00 | 1.00 | |||||||
| 10–19 | 72 | 0.96 | (0.49–1.90) | 0.96 | 0.90 | 0.91 | (0.40–2.09) | 0.82 | 0.89 | |
| 20+ | 38 | 0.96 | (0.41–2.22) | 0.96 | 0.94 | (0.35–2.55) | 0.90 | |||
| Peritraumatic situations | ||||||||||
| Disaster support duties: | ||||||||||
| Search and rescue, transportation or autopsy | None | 100 | 1.00 | 1.00 | ||||||
| Yes | 113 | 0.89 | (0.48–1.63) | 0.70 | 1.35 | (0.61–2.99) | 0.46 | |||
| Support for the victim’s family or the remains of victims | None | 139 | 1.00 | 1.00 | ||||||
| Yes | 74 | 2.09 | (1.12–3.89) | 0.02 | 1.99 | (0.95–4.21) | 0.07 | |||
| Cumulative days at work | <7 days | 90 | 1.00 | 1.00 | ||||||
| ≥7 days | 123 | 2.31 | (1.20–4.46) | 0.01 | 2.47 | (1.21–5.06) | 0.01 | |||
| Stressor and supports before the disaster: | ||||||||||
| Work stress | None | 170 | 1.00 | 1.00 | ||||||
| Have | 43 | 2.12 | (1.05–4.31) | 0.04 | 1.58 | (0.66–3.79) | 0.30 | |||
| Family or personal stress | None | 161 | 1.00 | 1.00 | ||||||
| Have | 52 | 1.01 | (0.50–2.05) | 0.98 | 0.76 | (0.33–1.76) | 0.52 | |||
| Supporter for usual work | None | 37 | 1.00 | 1.00 | ||||||
| Yes | 176 | 0.53 | (0.25–1.12) | 0.97 | 0.51 | (0.18–1.40) | 0.19 | |||
| Supporter for family life or personal problems | None | 46 | 1.00 | 1.00 | ||||||
| Yes | 167 | 0.61 | (0.30–1.23) | 0.12 | 1.02 | (0.39–2.65) | 0.97 | |||
| Stress relief behavior after the disaster: | ||||||||||
| Conversation with family or colleagues | None | 64 | 1.00 | 1.00 | ||||||
| Yes | 149 | 0.73 | (0.38–1.39) | 0.33 | 0.85 | (0.40–1.80) | 0.66 | |||
| Drinking or smoking | None | 164 | 1.00 | 1.00 | ||||||
| Yes | 49 | 1.65 | (0.83–3.28) | 0.16 | 2.35 | (1.09–5.04) | 0.03 | |||
| Resilience | ||||||||||
| CD-RISC score | High, 62+ | 68 | 1.00 | 1.00 | ||||||
| Medium, 50–61 | 83 | 0.96 | (0.45–2.06) | 0.93 | 0.13 | 0.98 | (0.43–2.25) | 0.96 | 0.44 | |
| Low, <50 | 62 | 1.79 | (0.83–3.84) | 0.14 | 1.42 | (0.59–3.42) | 0.43 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamijo, T.; Tsukahara, T.; Shimazu, A.; Nomiyama, T. Risk Factors for Duty-Related Posttraumatic Stress Disorder among Police Officers in the Mt. Ontake Eruption Disaster-Support Task Force. Int. J. Environ. Res. Public Health 2020, 17, 3134. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093134
Kamijo T, Tsukahara T, Shimazu A, Nomiyama T. Risk Factors for Duty-Related Posttraumatic Stress Disorder among Police Officers in the Mt. Ontake Eruption Disaster-Support Task Force. International Journal of Environmental Research and Public Health. 2020; 17(9):3134. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093134
Chicago/Turabian StyleKamijo, Tomoko, Teruomi Tsukahara, Akihito Shimazu, and Tetsuo Nomiyama. 2020. "Risk Factors for Duty-Related Posttraumatic Stress Disorder among Police Officers in the Mt. Ontake Eruption Disaster-Support Task Force" International Journal of Environmental Research and Public Health 17, no. 9: 3134. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093134