Unplanned Readmission within 28 Days of Hospital Discharge in a Longitudinal Population-Based Cohort of Older Australian Women


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Hospital Data
2.3. Covariates
2.4. Statistical Analysis
2.5. Ethical Clearance
3. Results
Predictors of Unplanned Readmission within 28 Days of Discharge
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Australian Institute of Health and Welfare (AIHW). Australia’s Hospitals 2016–17 at A Glance; Australian Institute of Health and Welfare: Canberra, Australia, 2017.
- McCusker, J.; Ionescu-Ittu, R.; Ciampi, A.; Vadeboncoeur, A.; Roberge, D.; Larouche, D.; Verdon, J.; Pineault, R. Hospital characteristics and emergency department care of older patients are associated with return visits. Acad. Emerg. Med. 2007, 14, 426–433. [Google Scholar] [CrossRef] [PubMed]
- McCusker, J.; Ardman, O.; Bellavance, F.; Belzile, E.; Cardin, S.; Verdon, J. Use of community services by seniors before and after an emergency visit. Can. J. Aging/La Rev. Can. Du Vieil. 2001, 20, 193–210. [Google Scholar] [CrossRef]
- Baillie, C.A.; VanZandbergen, C.; Tait, G.; Hanish, A.; Leas, B.; French, B.; William Hanson, C.; Behta, M.; Umscheid, C.A. The readmission risk flag: Using the electronic health record to automatically identify patients at risk for 30-day readmission. J. Hosp. Med. 2013, 8, 689–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Considine, J.; Fox, K.; Plunkett, D.; Mecner, M.; O’Reilly, M.; Darzins, P. Factors associated with unplanned readmissions in a major Australian health service. Aust. Health Rev. 2019, 43, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Considine, J.; Berry, D.; Newnham, E.; Jiang, M.; Fox, K.; Plunkett, D.; Mecner, M.; Darzins, P.; O’Reilly, M. Factors associated with unplanned readmissions within 1 day of acute care discharge: A retrospective cohort study. BMC Health Serv. Res. 2018, 18, 713. [Google Scholar] [CrossRef] [PubMed]
- Sharma, Y.; Miller, M.; Kaambwa, B.; Shahi, R.; Hakendorf, P.; Horwood, C.; Thompson, C. Factors influencing early and late readmissions in Australian hospitalised patients and investigating role of admission nutrition status as a predictor of hospital readmissions: A cohort study. BMJ Open 2018, 8, e022246. [Google Scholar] [CrossRef] [PubMed]
- Mudge, A.M.; Shakhovskoy, R.; Karrasch, A. Quality of transitions in older medical patients with frequent readmissions: Opportunities for improvement. Eur. J. Intern. Med. 2013, 24, 779–783. [Google Scholar] [CrossRef]
- McLean, R.; Mendis, K.; Canalese, J. A ten-year retrospective study of unplanned hospital readmissions to a regional Australian hospital. Aust. Health Rev. 2008, 32, 537–547. [Google Scholar] [CrossRef] [Green Version]
- Dahlberg, L.; Agahi, N.; Schön, P.; Lennartsson, C. Planned and unplanned hospital admissions and their relationship with social factors: Findings from a national, prospective study of people aged 76 years or older. Health Serv. Res. 2018, 53, 4248–4267. [Google Scholar] [CrossRef] [Green Version]
- Manzano, J.-G.M.; Luo, R.; Elting, L.S.; George, M.; Suarez-Almazor, M.E. Patterns and predictors of unplanned hospitalization in a population-based cohort of elderly patients with GI cancer. J. Clin. Oncol. 2014, 32, 3527. [Google Scholar] [CrossRef] [Green Version]
- Schairer, W.W.; Sing, D.C.; Vail, T.P.; Bozic, K.J. Causes and frequency of unplanned hospital readmission after total hip arthroplasty. Clin. Orthop. Relat. Res. 2014, 472, 464–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, T.; O’Connell, B.; Lakhan, P. Hospital readmission among older adults with congestive heart failure. Aust. Health Rev. 2013, 37, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.D.; Witham, M.D. Causes and correlates of 30 day and 180 day readmission following discharge from a Medicine for the Elderly Rehabilitation unit. BMC Geriatr. 2018, 18, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickinson, K.J.; Taswell, J.B.; Allen, M.S.; Blackmon, S.H.; Nichols, F.C., III; Shen, R.; Wigle, D.A.; Cassivi, S.D. Unplanned Readmission After Lung Resection: Complete Follow-Up in a 1-Year Cohort With Identification of Associated Risk Factors. Ann. Thorac. Surg. 2017, 103, 1084–1091. [Google Scholar] [CrossRef] [Green Version]
- Khavanin, N.; Bethke, K.P.; Lovecchio, F.C.; Jeruss, J.S.; Hansen, N.M.; Kim, J.Y. Risk factors for unplanned readmissions following excisional breast surgery. Breast J. 2014, 20, 288–294. [Google Scholar] [CrossRef]
- Navin Cristina, T.J.; Stewart Williams, J.A.; Parkinson, L.; Sibbritt, D.W.; Byles, J.E. Identification of diabetes, heart disease, hypertension and stroke in mid-and older-aged women: Comparing self-report and administrative hospital data records. Geriatr. Gerontol. Int. 2016, 16, 95–102. [Google Scholar] [CrossRef]
- Giorda, C.B.; Avogaro, A.; Maggini, M.; Lombardo, F.; Mannucci, E.; Turco, S.; Alegiani, S.S.; Raschetti, R.; Velussi, M.; Ferrannini, E.; et al. Recurrence of cardiovascular events in patients with type 2 diabetes: Epidemiology and risk factors. Diabetes Care 2008, 31, 2154–2159. [Google Scholar] [CrossRef] [Green Version]
- Bianco, A.; Molè, A.; Nobile, C.G.; Di Giuseppe, G.; Pileggi, C.; Angelillo, I.F. Hospital readmission prevalence and analysis of those potentially avoidable in southern Italy. PLoS ONE 2012, 7, e48263. [Google Scholar] [CrossRef] [Green Version]
- Horwitz, L.I.; Lin, Z.; Herrin, J.; Bernheim, S.; Drye, E.E.; Krumholz, H.M.; Ross, J.S. Association of hospital volume with readmission rates: A retrospective cross-sectional study. BMJ 2015, 350, h447. [Google Scholar] [CrossRef] [Green Version]
- Cui, Y.; Metge, C.; Ye, X.; Moffatt, M.; Oppenheimer, L.; Forget, E.L. Development and validation of a predictive model for all-cause hospital readmissions in Winnipeg, Canada. J. Health Serv. Res. Policy 2015, 20, 83–91. [Google Scholar] [CrossRef]
- Australian Longitudinal Study on Women’s Health (ALSWH). Available online: https://www.alswh.org.au/ (accessed on 25 November 2019).
- Wendy, J.; Brown, L.B.; Byles, J.E.; Dobson, A.J.; Lee, C.; Mishra, G.; Schofield, M. Women’s Health Australia: Recruitment for a national longintudinal cohort study. Women Health 1998, 28, 23–40. [Google Scholar]
- Byles, J.; Curryer, C.; Vo, K.; Forder, P.; Loxton, D.; McLaughlin, D. Changes in housing among older women: Latent class analysis of housing patterns in older Australian women. Urban Stud. 2018, 55, 917–934. [Google Scholar] [CrossRef]
- National Centre for Classification in Health (NCCH). The International Statistical Classification of Diseases and Health Related Problems; Tenth Revision, Australian Modification (ICD-10-AM); Australia, 2006. Available online: https://www.ihpa.gov.au/what-we-do/icd-10-am-achi-acs-classification (accessed on 30 April 2020).
- GISCA; Department of Health and Aged Care. Measuring Remoteness: Accessibility/Remoteness Index of Australia (ARIA); New Series No. 6; Department of Health and Aged Care: Canberra, Australia, 2001.
- WHO. Obesity: Preventing and Managing the Global Epidemic Report of a WHO Consultation (WHO Technical Report Series 894); WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Britt, H.; Miller, G.C.; Charles, J.; Henderson, J.; Bayram, C.; Pan, Y.; Valenti, L.; Harrison, C.; Fahridin, S.; O’Halloran, J. General Practice Activity in Australia 2008–09; Australian Institute of Health and Welfare: Canberra, Australia, 2009.
- Azfredrick, E.C. Using Anderson’s model of health service utilization to examine use of services by adolescent girls in south-eastern Nigeria. Int. J. Adolesc. Youth 2016, 21, 523–529. [Google Scholar] [CrossRef]
- Collett, D. Modelling Survival Data in Medical Research; Chapman and Hall/CRC: Boca Raton, FL, USA, 2015. [Google Scholar]
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection—A review and recommendations for the practicing statistician. Biom. J. 2018, 60, 431–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolevich, Z. Unplanned Hospital Readmissions Where to from Here? NSW Ministry of Health: New South Wales, Australia, 2015.
- Hamar, G.B.; Coberley, C.; Pope, J.E.; Cottrill, A.; Verrall, S.; Larkin, S.; Rula, E.Y. Effect of post-hospital discharge telephonic intervention on hospital readmissions in a privately insured population in Australia. Aust. Health Rev. 2017, 42, 241–247. [Google Scholar] [CrossRef]
- Finlayson, K.; Chang, A.M.; Courtney, M.D.; Edwards, H.E.; Parker, A.W.; Hamilton, K.; Pham, T.D.X.; O’Brien, J. Transitional care interventions reduce unplanned hospital readmissions in high-risk older adults. BMC Health Serv. Res. 2018, 18, 956. [Google Scholar] [CrossRef] [Green Version]
- Hasan, M. Readmission of patients to hospital: Still ill defined and poorly understood. Int. J. Qual. Health Care 2001, 13, 177–179. [Google Scholar] [CrossRef]
- Riegel, B.; Carlson, B.; Glaser, D.; Romero, T. Randomized controlled trial of telephone case management in Hispanics of Mexican origin with heart failure. J. Card. Fail. 2006, 12, 211–219. [Google Scholar] [CrossRef]
- Anderson, C.; Deepak, B.; Amoateng-Adjepong, Y.; Zarich, S. Benefits of comprehensive inpatient education and discharge planning combined with outpatient support in elderly patients with congestive heart failure. Congest. Heart Fail. 2005, 11, 315–321. [Google Scholar] [CrossRef]
- Linertová, R.; García-Pérez, L.; Vázquez-Díaz, J.R.; Lorenzo-Riera, A.; Sarría-Santamera, A. Interventions to reduce hospital readmissions in the elderly: In-hospital or home care. A systematic review. J. Eval. Clin. Pract. 2011, 17, 1167–1175. [Google Scholar] [CrossRef]
- Maali, Y.; Perez-Concha, O.; Coiera, E.; Roffe, D.; Day, R.O.; Gallego, B. Predicting 7-day, 30-day and 60-day all-cause unplanned readmission: A case study of a Sydney hospital. BMC Med. Inform. Decis. Mak. 2018, 18, 1. [Google Scholar] [CrossRef] [Green Version]
- Pimouguet, C.; Rizzuto, D.; Lagergren, M.; Fratiglioni, L.; Xu, W. Living alone and unplanned hospitalizations among older adults: A population-based longitudinal study. Eur. J. Public Health 2017, 27, 251–256. [Google Scholar] [CrossRef]
- Cafferata, G.L. Marital status, living arrangements, and the use of health services by elderly persons. J. Gerontol. 1987, 42, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.L.; Dolja-Gore, X.; Kendig, H.; Byles, J.E. First incident hospitalisation for Australian women aged 70 and beyond: A 10 year examination using competing risks. Arch. Gerontol. Geriatr. 2016, 64, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare (AIHW). Australian Institute of Health and Welfare 2018. In Australia’s Health 2018; Australian Institute of Health and Welfare: Canberra, Australia, 2018. [Google Scholar]
- Ngai, K.M.; Grudzen, C.R.; Lee, R.; Tong, V.Y.; Richardson, L.D.; Fernandez, A. The association between limited English proficiency and unplanned emergency department revisit within 72 hours. Ann. Emerg. Med. 2016, 68, 213–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabayan, G.Z.; Sarkisian, C.A.; Liang, L.J.; Sun, B.C. Predictors of admission after emergency department discharge in older adults. J. Am. Geriatr. Soc. 2015, 63, 39–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gusmano, M.; Rodwin, V.; Weisz, D.; Cottenet, J.; Quantin, C. Comparison of rehospitalization rates in France and the United States. J. Health Serv. Res. Policy 2015, 20, 18–25. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | No Readmission (n = 1693) n (%) | Planned Readmission (n = 134) n (%) | Unplanned Readmission (n = 229) n (%) | p-Value |
|---|---|---|---|---|
| Predisposing factors | ||||
| Age at index admission, mean ± SD | 82.11 ± 3.95 | 81.65.00 ± 3.75 | 82.00 ± 4.18 | 0.546 |
| Marital status | ||||
| Partnered | 687 (40.67) | 46 (34.33) | 66 (28.82) | 0.001 |
| Not partnered | 1002 (59.33) | 88 (65.67) | 163 (71.18) | |
| Missing | 4 | |||
| English speaking | ||||
| No | 1452 (90.02) | 110 (84.09) | 185 (84.09) | 0.015 |
| Yes | 161 (9.98) | 18 (14.06) | 35 (15.91) | |
| Missing | 80 | 6 | 229 | |
| Enabling factors | ||||
| Area | ||||
| Metropolitan | 709 (41.88) | 61 (45.52) | 77 (33.62) | 0.130 |
| Inner regional | 696 (41.11) | 53 (39.55) | 105 (45.85) | |
| Outer regional/remote/very remote | 288 (17.01) | 20 (14.93) | 47 (20.52) | |
| Education | ||||
| Less than High school | 1248 (77.52) | 95 (74.80) | 169 (77.17) | 0.676 |
| School certificate | 222 (13.79) | 16 (12.60) | 29 (13.24) | |
| Higher/above school certificate | 140 (8.7) | 16 (12.60) | 21 (9.59) | |
| Missing | 83 | 7 | 10 | |
| Private insurance | ||||
| No | 1046 (62.37) | 75 (56.39) | 154 (67.84) | 0.087 |
| Yes | 631 (37.63) | 58 (43.61) | 73 (32.16) | |
| Missing | 16 | 1 | 2 | |
| Need factors | ||||
| Smoking | ||||
| Non-smoker | 1035 (65.46) | 76 (61.29) | 140 (64.81) | 0.038 |
| Ex-smoker | 444 (28.08) | 31 (25.00) | 57 (26.39) | |
| Current smoker | 102 (6.45) | 17 (13.71) | 19 (8.80) | |
| Missing | 112 | 10 | 13 | |
| LOS index | ||||
| ≤3 days | 764 (45.13) | 59 (44.03) | 85 (37.12) | 0.073 |
| >3 days | 929 (54.87) | 75 (55.97) | 144 (62.88) | |
| BMI | ||||
| Underweight | 71 (4.41) | 2 (1.56) | 9 (4.04) | 0.137 |
| Normal weight | 806 (50.06) | 68 (53.13) | 103 (46.19) | |
| Overweight | 495 (30.75) | 48 (37.50) | 77 (34.53) | |
| Obese | 238 (14.78) | 10 (7.81) | 34 (15.25) | |
| Missing | 83 | 6 | 6 | |
| Perceived general health | ||||
| Good/excellent | 1075 (64.29) | 86 (64.66) | 147 (64.19) | 0.995 |
| Poor/not good | 597 (35.71) | 47 (35.34) | 82 (35.81) | |
| Missing | 21 | 1 | ||
| GP or family doctor visit | ||||
| ≤4 | 554 (36.76) | 42 (34.15) | 81 (41.97) | 0.287 |
| >4 | 953 (63.24) | 81 (65.85) | 112 (58.03) | |
| Missing | 186 | 11 | 36 | |
| Chronic disease | ||||
| No | 526 (34.90) | 44 (35.77) | 51 (25.89) | 0.026 |
| 1–2 | 636 (42.20) | 56 (45.53) | 106 (53.81) | |
| >2 | 345 (22.89) | 23 (18.70) | 40 (20.30) | |
| Missing | 186 | 11 | 32 |
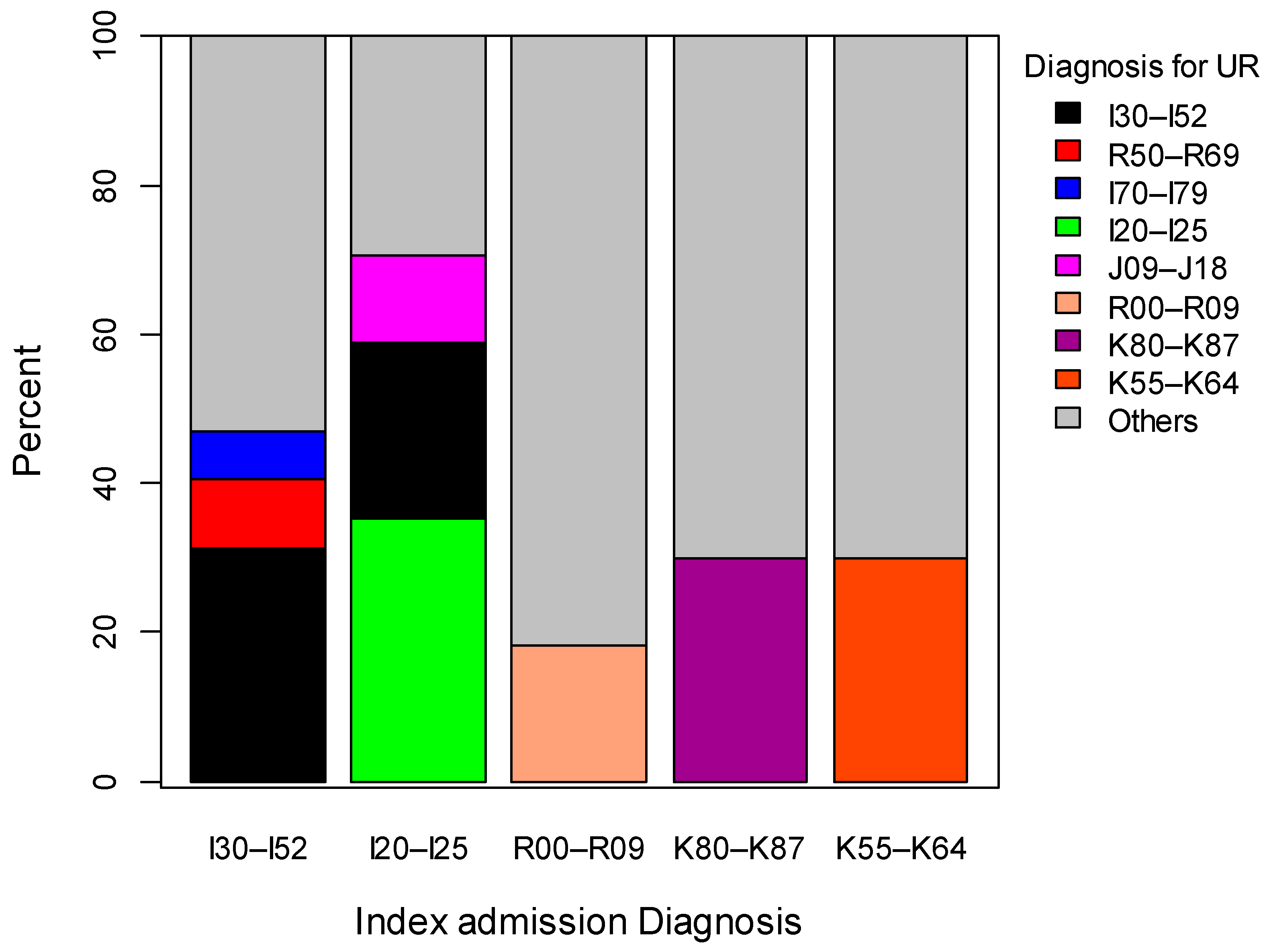
| Top Five Index Admission | Unplanned Readmission | Definition |
|---|---|---|
| I30–I52 (13.98%) | I30–I52 (31.25%) | Other forms of heart disease |
| R50–R69 (9.38%) | General symptoms and signs | |
| I70–I79 (6.25%) | Arterial embolism and thrombosis | |
| Other (53.13%) | ||
| I20–I25 (7.42%) | I20–I25 (35.29%) | Ischaemic heart disease |
| I30–I52 (23.53%%) | Other forms of heart disease | |
| J09–J18 (11.76%) | Influenza and pneumonia | |
| Other (29.42%) | ||
| R00–R09 (4.80%) | R00–R09 (18.18%) | Symptoms and signs involving the circulatory and respiratory systems |
| Other (81.82%) | ||
| K80–K87 (4.37%) | K80–K87 (33.33%) | Disorder of gallbladder, biliary tract and pancreas |
| Other (76.67%) | ||
| K55–K64 (4.37%) | K55–K64 (33.33%) | Other diseases of intestines |
| Other (76.67%) |
| Characteristics | Unplanned Readmission n (%) (n = 229) | Univariate Analysis HR (95% CI) | p-Value | Multivariate Analysis AHR (95% CI) |
|---|---|---|---|---|
| Predisposing factors | ||||
| Age | 82.30 ± 4.18 | 1.01 (0.98, 1.05) | 0.584 | 1.02 (0.98, 1.06) |
| Marital status (Ref: Partnered) | 66 (28.82) | 1 | <0.01 | 1 |
| Not Partnered | 163 (71.18) | 1.61 (1.21, 2.14) ** | 1.43 (1.05, 1.95) * | |
| English speaking (Ref: Yes) | 185 (84.09) | 1 | 0.012 | 1 |
| No | 35 (15.91) | 1.59 (1.11, 2.28) * | 1.62 (1.07, 2.47) * | |
| Enabling factor | ||||
| Area (Ref: Metropolitan) | 77 (33.62) | 1 | 0.043 | 1 |
| Inner regional | 105 (45.85) | 1.37 (1.02, 1.84) * | 1.28 (0.92, 1.78) | |
| Outer regional/remote/very remote | 47 (20.52) | 1.50 (1.04, 2.15) * | 1.47 (0.97, 2.22) | |
| Education (Ref: Higher/above school certificate) | 169 (77.17) | 1 | 0.947 | |
| School certificate | 238 (13.24) | 0.97 (0.65, 1.44) | ||
| Less than high school | 21 (9.59) | 1.07 (0.68, 1.68) | ||
| Private insurance (Ref: Yes) | 154 (67.84) | 1 | 0.085 | 1 |
| No | 73 (32.16) | 0.78 (0.59, 1.04) | 0.79 (0.58, 1.08) | |
| Need factors | ||||
| Smoking (Ref: Non-smoker) | 140 (64.81) | 1 | 0.609 | |
| Ex-smoker | 57 (26.39) | 0.96 (0.71, 1.31) | ||
| Current smoker | 19 (8.80) | 1.25 (0.77, 2.01) | ||
| LOS in index (Ref: ≤3) | 85 (37.12) | 1 | 0.026 | 1 |
| Greater than 3 | 144 (62.88) | 1.36 (1.04, 1.77) * | 1.41(1.04, 1.90) * | |
| BMI (Ref: Normal weight) | 10 (4.48) | 1 | 0.709 | |
| Underweight | 100 (44.84) | 0.95 (0.48, 1.88) | ||
| Overweight | 78 (34.98) | 1.13 (0.56, 2.25) | ||
| Obese | 35 (15.70) | 1.09 (0.52, 2.27) | ||
| Perceived general health (Ref: Good/excellent) | 127 (64.47) | 1 | 0.971 | |
| Poor/not good | 70 (35.53) | 1.01 (0.77, 1.31) | ||
| GP/family doctor visit (Ref: ≤4) | 81 (41.97) | 1 | 0.123 | 1 |
| >4 | 112 (58.03) | 0.81 (0.63, 1.06) | 0.82 (0.61, 1.11) | |
| Chronic disease (Ref: No) | 51 (25.89) | 1 | 0.007 | 1 |
| 1–2 | 106 (53.81) | 1.66 (1.19, 2.32) * | 1.68 (1.19, 2.36) * | |
| >2 | 40 (20.30) | 1.21 (0.79, 1.83) | 1.18 (0.77, 1.83) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shebeshi, D.S.; Dolja-Gore, X.; Byles, J. Unplanned Readmission within 28 Days of Hospital Discharge in a Longitudinal Population-Based Cohort of Older Australian Women. Int. J. Environ. Res. Public Health 2020, 17, 3136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093136
Shebeshi DS, Dolja-Gore X, Byles J. Unplanned Readmission within 28 Days of Hospital Discharge in a Longitudinal Population-Based Cohort of Older Australian Women. International Journal of Environmental Research and Public Health. 2020; 17(9):3136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093136
Chicago/Turabian StyleShebeshi, Dinberu S., Xenia Dolja-Gore, and Julie Byles. 2020. "Unplanned Readmission within 28 Days of Hospital Discharge in a Longitudinal Population-Based Cohort of Older Australian Women" International Journal of Environmental Research and Public Health 17, no. 9: 3136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093136