Ageism, Healthy Life Expectancy and Population Ageing: How Are They Related?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Dependent Variables
2.3. Individual-Level Variables
2.4. Country-Level Variables
2.5. Statistical Analysis
3. Results
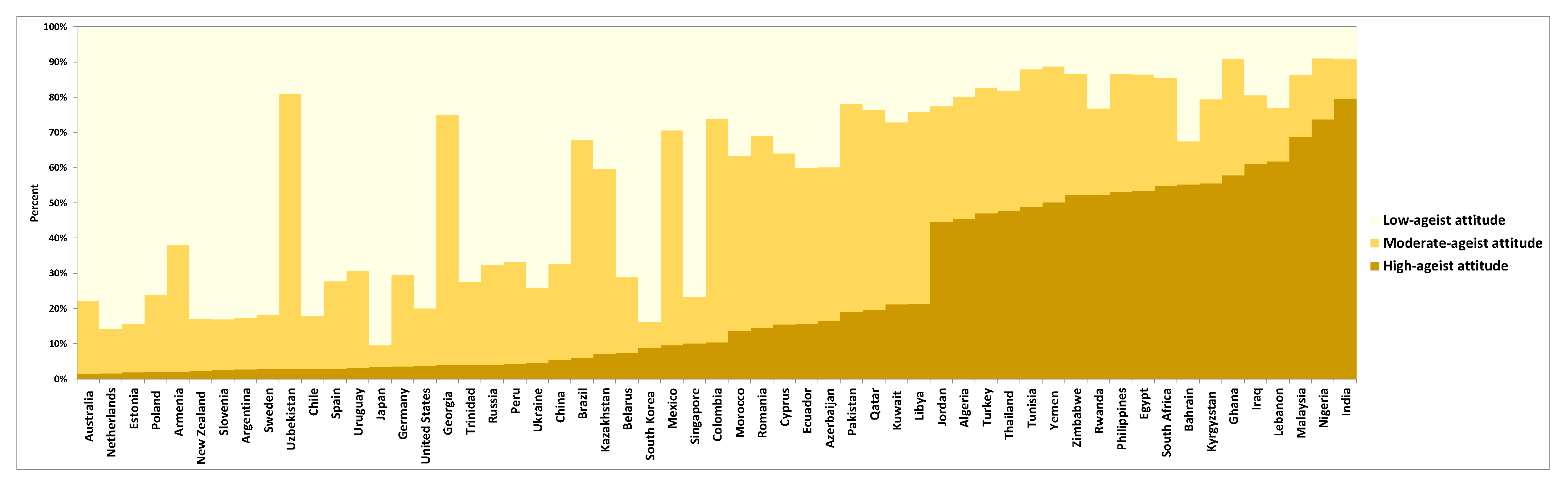
3.1. Individual Latent Classes of Ageism
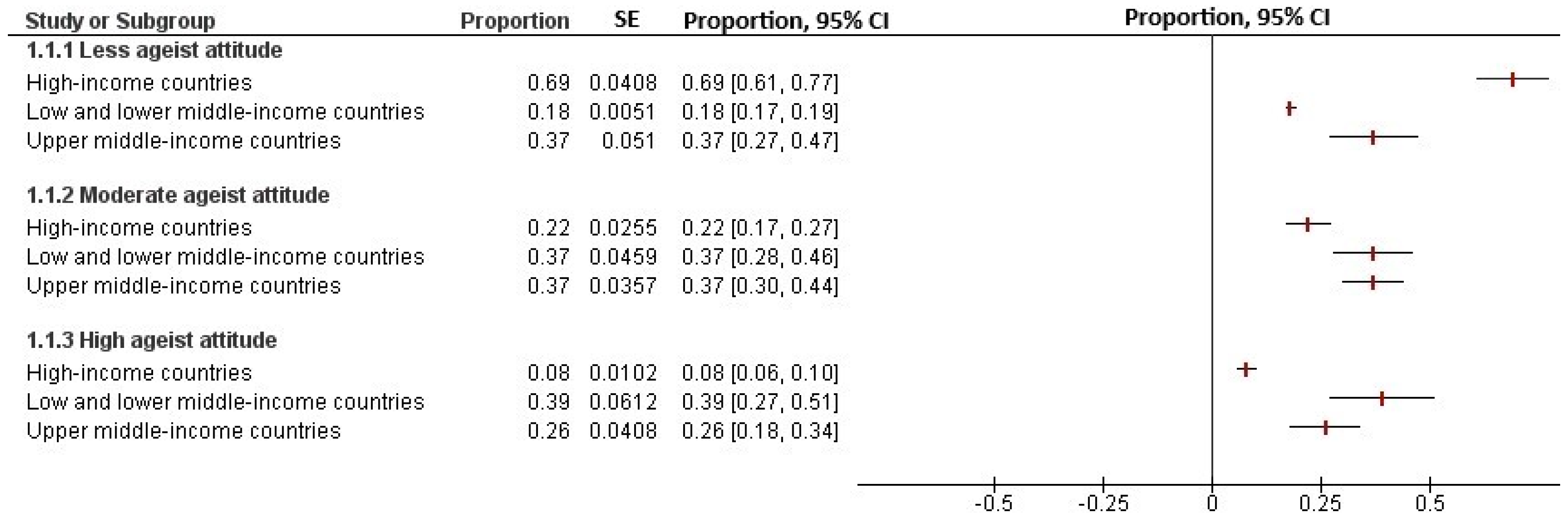
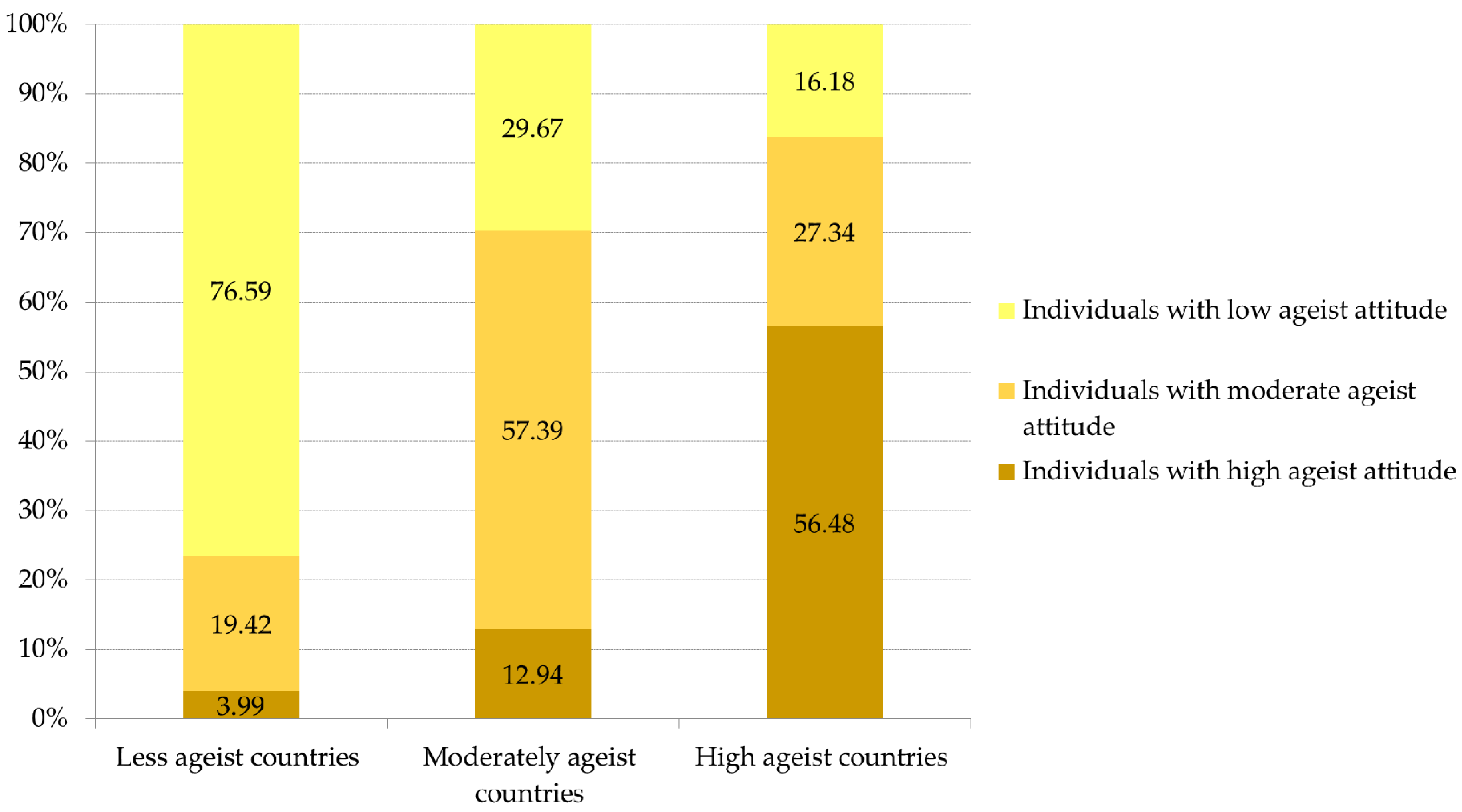
3.2. Country Latent Classes of Ageism
3.3. Individual-Level and Country-Level Covariate Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- United Nations. World Population Prospects: The 2017 Revision, World Population 2017 Wallchart; Department of Economic and Social Affairs: New York, NY, USA, 2017. [Google Scholar]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Officer, A.; de la Fuente-Núñez, V. A global campaign to combat ageism. Bull. World Health Organ. 2018, 96, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Kite, M.; Stockdale, G.; Whitley, B.; Johnson, B. Attitudes toward younger and older adults: An updated meta-analytic review. J. Soc. Issues 2005, 61, 241–266. [Google Scholar] [CrossRef]
- Levy, B.; Banaji, M. Implicit ageism. In Ageism: Stereotyping and Prejudice against Older Persons; Nelson, T., Ed.; MIT Press: Cambridge, MA, USA, 2002; pp. 127–128. [Google Scholar]
- Zebrowitz, L.M.; Montepare, J.M. Too young, too old: Stigmatizing adolescents and elders. In The Social Psychology of Stigma; Heatherton, T.F., Kleck, R.E., Hebl, M.R., Hull, J.G., Eds.; Guildford Press: New York, NY, USA, 2000; pp. 334–373. [Google Scholar]
- Lloyd-Sherlock, P.G.; Ebrahim, S.; McKee, M.; Prince, M.J. Institutional ageism in global health policy. BMJ 2016, 354, i4514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, P.G.; Weeks, L.E.; van Den Bergh, G.; Doucet, S. Gerontology across the professions and the Atlantic: Development and evaluation of an interprofessional and international course on aging and health. Gerontol. Geriatr. Educ. 2017, 38, 141–157. [Google Scholar] [CrossRef]
- Lamont, R.S.; Swift, H.J.; Abrams, D. A review and meta-analysis of age-based stereotype threat: Negative stereotypes, not facts, do the damage. Psychol. Aging 2015, 30, 180–193. [Google Scholar] [CrossRef]
- Levy, B. Stereotype Embodiment: A Psychosocial Approach to Aging. Curr. Dir. Psychol. Sci. 2009, 18, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Levy, B. Mind matters: Cognitive and physical effects of aging self-stereotypes. J. Gerontol. B Psychol. Sci. Soc. Sci. 2003, 58, P203–P211. [Google Scholar] [CrossRef] [Green Version]
- Peterson, L.; Ralston, M. Valued elders or societal burden: Cross-national attitudes toward older adults. Int. Sociol. 2017, 32, 731–754. [Google Scholar] [CrossRef]
- Lockenhoff, C.; De Fruyt, F.; Terracciano, A.; McCrae, R.; De Bolle, M.; Costa, P.; Aguilar-Vafaie, M.; Ahn, C.; Ahn, H.; Alcalay, L.; et al. Perceptions of Aging Across 26 Cultures and Their Culture-Level Associates. Psychol. Aging 2009, 24, 941–954. [Google Scholar] [CrossRef] [Green Version]
- North, M.S.; Fiske, S.T. Modern Attitudes Toward Older Adults in the Aging World: A Cross-Cultural Meta-Analysis. Psychol. Bull. 2015, 141, 993–1021. [Google Scholar] [CrossRef] [Green Version]
- Abrams, D.; Russell, P.S.; Vauclair, C.M.; Swift, H. Ageism in Europe: Findings from the European Social Survey; Age UK: London, UK, 2011. [Google Scholar]
- World Values Survey. Round Six—Country-Pooled Datafile Version. Available online: http://www.worldvaluessurvey.org/WVSDocumentationWV6.jsp (accessed on 20 January 2018).
- World Health Organization. WHO Methods and Data Sources for Life Table 1990 Table 1991 Table 1992 Table 1993 Table 1994 Table 1995 Table 1996 Table 1997 Table 1998 Table 1999 Table 2000 Table 2001 Table 2002 Table 2003 Table 2004 Table 2005 Table 2006 Table 2007 Table 2008 Table 2009 Table 2010 Table 2011 Table 2012 Table 2013 Table 2014 Table 2015; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- UNDP. Technical Notes: Calculating the Human Development Indices: Human Development Report 2015; United Nations: New York, NY, USA, 2015. [Google Scholar]
- United Nations. World Population Prospects 2017. Available online: https://population.un.org/wpp/DataQuery/ (accessed on 15 August 2018).
- Fantom, N.; Serajuddin, U. The World Bank’s Classification of Countries by Income; World Bank Group: Washington, DC, USA, 2016. [Google Scholar]
- Henry, K.L.; Muthen, B. Multilevel Latent Class Analysis: An Application of Adolescent Smoking Typologies with Individual and Contextual Predictors. Struct. Equ. Model. 2010, 17, 193–215. [Google Scholar] [CrossRef] [Green Version]
- Abrams, D.; Vauclair, M.; Swift, H. Predictors of Attitudes to Age across Europe; Department for Work and Pensions: London, UK, 2011.
- Levy, B.; Zonderman, A.; Slade, M.; Ferrucci, L. Age stereotypes held earlier in life predict cardiovascular events in later life. Psychol. Sci. 2009, 20, 296–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, B.; Ferrucci, L.; Zonderman, A.; Slade, M.; Troncoso, J.; Resnick, S. A culture-brain link: Negative age stereotypes predict Alzheimer’s disease biomarkers. Psychol. Aging 2016, 31, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Myers, L. Preventive health behaviors influenced by self-perceptions of aging. Prev. Med. 2004, 39, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Sarkisian, C.; Hays, R.; Mangione, C. Do older adults expect to age successfully? The association between expectations regarding aging and beliefs regarding healthcare seeking among older adults. J. Am. Geriatr. Soc. 2002, 50, 1837–1843. [Google Scholar] [CrossRef] [Green Version]
- Abrams, D.; Crisp, R.; Marques, S.; Fagg, E.; Bedford, L.; Provias, D. Threat Inoculation: Experienced and Imagined Intergenerational Contact Prevents Stereotype Threat Effets on Older People’s Math Performance. Psychol. Aging 2008, 23, 934–939. [Google Scholar] [CrossRef]
- Levy, B.; Slade, M.; Kunkel, S.; Kasl, S. Longevity increased by positive self-perceptions of aging. J. Pers. Soc. Psychol. 2002, 83, 261–270. [Google Scholar] [CrossRef]
- Maier, H.; Smith, J. Psychological predictors of mortality in old age. J. Gerontol. B Psychol. Sci. Soc. Sci. 1999, 54, P44–P54. [Google Scholar] [CrossRef]
- Chopik, W.J.; Giasson, H.L. Age Differences in Explicit and Implicit Age Attitudes across the Life Span. Gerontologist 2017, 57, S169–S177. [Google Scholar] [CrossRef]
- Christian, J.; Turner, R.; Holt, N.; Larkin, M.; Cotler, J. Does intergenerational contact reduce Ageism: When and how contact interventions actually work? J. Arts Humanit. 2014, 3, 1–15. [Google Scholar]
- Bodner, E.; Bergman, Y.; Cohen-Fridel, S. Different dimensions of ageist attitudes among men and women: A multigenerational perspective. Int. Psychogeriatr. 2012, 24, 895–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnes, D.; Sheppard, C.; Henderson, C.R., Jr.; Wassel, M.; Cope, R.; Barber, C.; Pillemer, K. Interventions to Reduce Ageism Against Older Adults: A Systematic Review and Meta-Analysis. Am. J. Public Health 2019, 109, e1–e9. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predictors | Comparison: High Ageist Attitude vs. Low Ageist Attitude | Comparison: Moderate Ageist Attitude vs. Low Ageist Attitude | |||||
|---|---|---|---|---|---|---|---|
| Model 1 a | Model 2 b | Model 3 c | Model 1 a | Model 2 b | Model 3 c | ||
| Odds Ratio (95% CI) | Odds Ratio (95% CI) | Odds Ratio (95% CI) | Odds Ratio (95% CI) | Odds Ratio (95% CI) | Odds Ratio (95% CI) | ||
| Individual characteristics | |||||||
| Age | 0.97 (0.96–0.98) ** | - | 0.98 (0.97–0.99) ** | 0.98 (0.97–0.99) ** | - | 1.0 (0.99–1.01) | |
| Sex | Female | Ref | - | Ref | Ref | - | Ref |
| Male | 1.2 (1.1–1.3) ** | - | 1.2 (1.1–1.3) ** | 1.2 (1.1–1.3) ** | - | 1.0 (0.96–1.2) | |
| Education | None or incomplete primary | Ref | - | Ref | Ref | - | Ref |
| Complete primary | 0.46 (0.43–0.50) ** | - | 0.90 (0.84–0.97) ** | 0.55 (0.51–0.59) ** | - | 0.84 (0.78–0.90) ** | |
| At least some secondary | 0.27 (0.25–0.29) ** | - | 0.61 (0.57–0.67) ** | 0.47 (0.44–0.51) ** | - | 0.79 (0.74–0.84) ** | |
| University education | 0.18 (0.17–0.20) ** | - | 0.57 (0.53–0.61) ** | 0.37 (0.35–0.39) ** | - | 0.70 (0.66–0.74) ** | |
| Income (higher) | 1.2 (0.99–1.4) | - | - | 1.1 (0.87–1.38) | - | - | |
| Contextual factors | |||||||
| Healthy life expectancy | - | 0.56 (0.43–0.73) ** | 0.87 (0.82–0.93) ** | - | 0.70 (0.54–0.90) ** | 0.91 (0.86–0.97) ** | |
| Population health status as self-reported | - | 1.0 (0.98–1.02) | - | - | 1.01 (0.99–1.03) | - | |
| Income inequality | - | 1.02 (0.99–1.03) | - | - | 1.01 (0.98–1.04) | - | |
| Proportion of older people | - | 0.21 (0.20–0.22) ** | 0.32 (0.30–0.34) ** | - | 0.45 (0.44–0.46) ** | 0.52 (0.51–0.53) ** | |
| Predictors | Comparison: Highly Ageist Countries vs. Not Very Ageist Countries | Comparison: Moderately Ageist Countries vs. Not Very Ageist Countries | ||
|---|---|---|---|---|
| Model 1 a | Model 2 b | Model 1 a | Model 2 b | |
| Contextual factors | Odds ratio (95% CI) | Odds ratio (95% CI) | Odds ratio (95% CI) | Odds ratio (95% CI) |
| Healthy life expectancy | 0.55 (0.42–0.73) ** | 0.73 (0.71–0.74) ** | 0.70 (0.54–0.90) ** | 0.91 (0.90–0.92) ** |
| Proportion of older people | 0.72 (0.71–0.73) ** | 0.68 (0.67–0.69) ** | 0.60 (0.59–0.61) ** | 0.74 (0.73–0.75) ** |
| Population health status (self-reported) | 0.97 (0.971–0.972) ** | 1.0 (0.80–1.02) | 0.94 (0.93–0.95) ** | 1.0 (0.9–1.03) |
| Income inequality | 0.97 (0.88–1.05) | - | 0.97 (0.89–1.04) | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Officer, A.; Thiyagarajan, J.A.; Schneiders, M.L.; Nash, P.; de la Fuente-Núñez, V. Ageism, Healthy Life Expectancy and Population Ageing: How Are They Related? Int. J. Environ. Res. Public Health 2020, 17, 3159. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093159
Officer A, Thiyagarajan JA, Schneiders ML, Nash P, de la Fuente-Núñez V. Ageism, Healthy Life Expectancy and Population Ageing: How Are They Related? International Journal of Environmental Research and Public Health. 2020; 17(9):3159. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093159
Chicago/Turabian StyleOfficer, Alana, Jotheeswaran Amuthavalli Thiyagarajan, Mira Leonie Schneiders, Paul Nash, and Vânia de la Fuente-Núñez. 2020. "Ageism, Healthy Life Expectancy and Population Ageing: How Are They Related?" International Journal of Environmental Research and Public Health 17, no. 9: 3159. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093159