Healthcare Providers’ Knowledge and Attitude Towards Abortions in Thailand: A Pre-Post Evaluation of Trainings on Safe Abortion


 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Ethics Approval
2.3. Data Collection and Measures
2.4. Analysis
2.5. Descriptive Statistics
2.6. Bivariate Analysis
2.7. Multivariable Analysis
3. Results
3.1. Demographics Characteristics and Work Experience
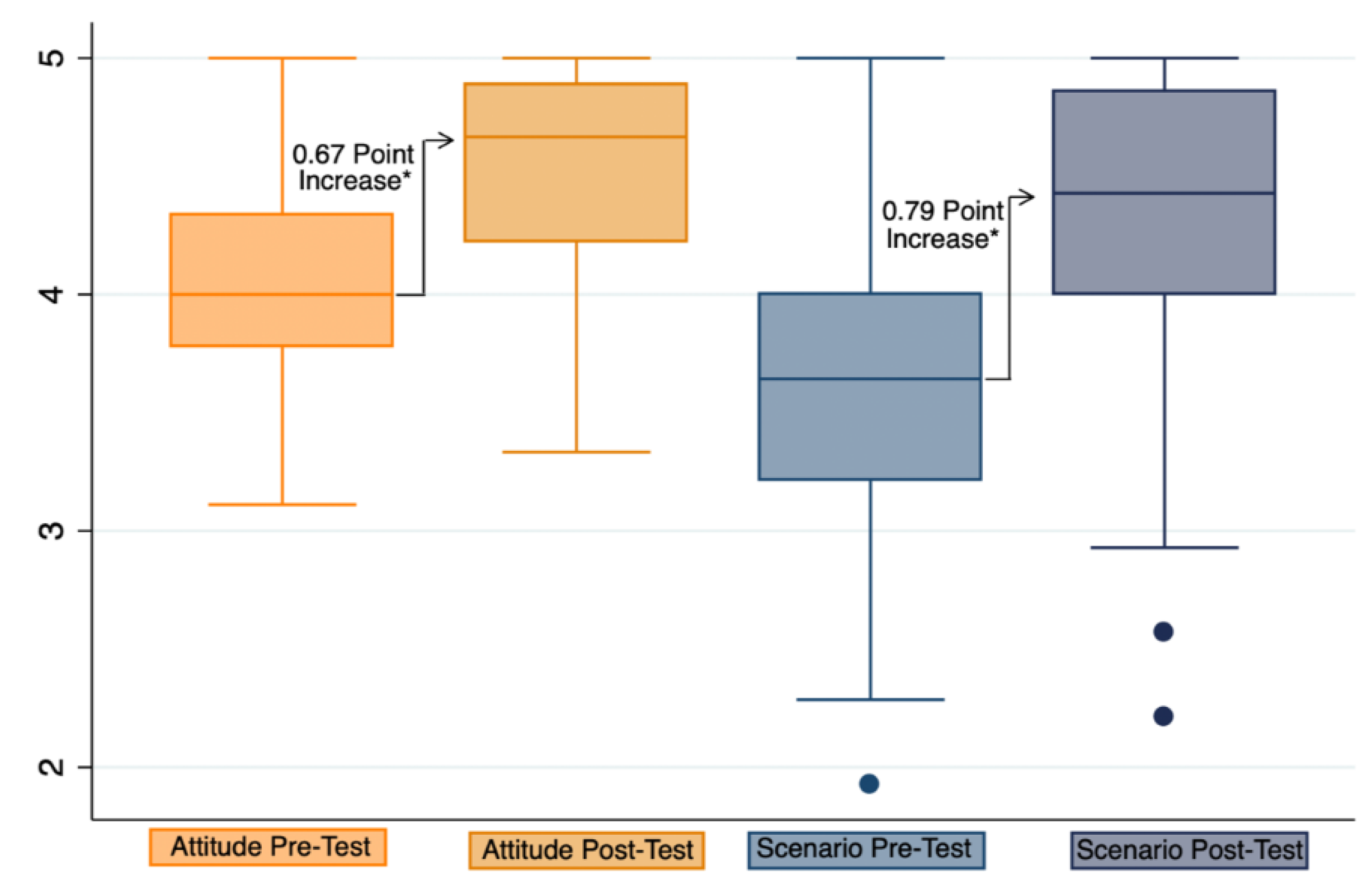
3.2. Comparison of Pre-post Results on Attitudes towards Adolescents and Women Experiencing Unplanned Pregnancies and Unsafe Abortions
3.3. Comparison of Pre-post Results on Attitudes towards Various Scenarios for Abortions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Haddad, L.B.; Nour, N.M. Unsafe abortion: Unnecessary maternal mortality. Rev. Obstet. Gynecol. 2009, 2, 122–126. [Google Scholar] [PubMed]
- World Health Organization. The Prevention and Management of Unsafe Abortion: Report of a Technical Working Group, Geneva, 12–15 April 1992; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Ganatra, B.; Gerdts, C.; Rossier, C.; Johnson, B.R., Jr.; Tunçalp, Ö.; Assifi, A.; Sedgh, G.; Singh, S.; Bankole, A.; Popinchalk, A.; et al. Global, regional, and subregional classification of abortions by safety, 2010–2014: Estimates from a Bayesian hierarchical model. Lancet 2017, 390, 10110. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Preventing Unsafe Abortion: WHO. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/preventing-unsafe-abortion (accessed on 30 March 2020).
- World Health Organization. Department of Reproductive Health and Research. Reproductive Health Strategy to Accelerate Progress Towards the Attainment of International Development Goals and Targets; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Warakamin, S.; Boonthai, N.; Tangcharoensathien, V. Induced abortion in Thailand: Current situation in public hospitals and legal perspectives. Reprod. Health Matters 2004, 12 (Suppl. 24), 147–156. [Google Scholar] [CrossRef] [Green Version]
- Srinil, S. Factors associated with severe complications in unsafe abortion. J. Med Assoc. Thail. 2011, 94, 408. [Google Scholar]
- Chunuan, S.; Kosunvanna, S.; Sripotchanart, W.; Lawantrakul, J.; Lawantrakul, J.; Pattrapakdikul, U.; Somporn, J. Characteristics of Abortions in Southern Thailand. Pacific Rim Int. J. Nurs. Res. 2012, 16, 97–112. [Google Scholar]
- Chaturachinda, K. Unsafe abortion in Thailand: Roles of RTCOG. Thai J. Obstet. Gynaecol. 2014, 2014, 2–7. [Google Scholar]
- Olukoya, A.; Kaya, A.; Ferguson, B.; AbouZahr, C. Unsafe abortion in adolescents. Int. J. Gynecol. Obstet. 2001, 75, 137–147. [Google Scholar] [CrossRef]
- World Health Organization. World health statistics 2019: Monitoring health for the SDGs, sustainable development goals; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Ministry of Public Health. Public Health Statistics A.D.2017. In Nonthaburi: Strategy and Planning Division; Ministry of Public Health: Bangkok, Thailand, 2017. [Google Scholar]
- Whittaker, A. Abortion, Sin and the State in Thailand; Routledge Curzon: New York, NY, USA, 2004. [Google Scholar]
- Chaturachinda, K.; Boonthai, N. Unsafe Abortion: An Inequity in Health Care. Thail. Perspect. J. Popul. Soc. Stud. 2017, 25, 287–297. [Google Scholar] [CrossRef]
- Praditpan, P.; Chaturachinda, K. Doctors must Heed Abortion Needs; Bangkok Post: Bangkok, Thailand, 2016. [Google Scholar]
- World Health Organization. Clinical Practice Handbook for Safe Abortion; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Madziyire, M.G.; Ann, M.; Taylor, R.; Elizabeth, S.; Tsungai, C. Knowledge and attitudes towards abortion from health care providers and abortion experts in Zimbabwe: A cross sectional study. Pan. Afr. Med. J. 2019, 34, 94. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.; Dickson, K.; Blanchard, K.; Cullingworth, L.; Mavimbela, N.; von Mollendorf, C.; van Bogaert, L.; Winikoff, B. Medical Abortion: The Possibilities for Introduction in the Public Sector in South Africa. Reprod. Health Matters 2005, 13, 35–43. [Google Scholar] [CrossRef]
- Loi, U.R.; Kristina, G.-D.; Elisabeth, F.; Marie, K.-A. Health care providers’ perceptions of and attitudes towards induced abortions in sub-Saharan Africa and Southeast Asia: A systematic literature review of qualitative and quantitative data. BMC Public Health 2015, 15, 139. [Google Scholar]
- Sullivan, G.M.; Artino, A.R., Jr. Analyzing and interpreting data from likert-type scales. J. Grad. Med. Educ. 2013, 5, 541–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Total (n = 247) |
|---|---|
| Sex (male/female) (%) | 15.4/84.6 |
| Age (Year) (Mean ± SD) [Min–Max] | 35.9 ± 8.8 [23–58] |
| Profession (%) | |
| Doctor (n = 137) (% of total participants) | 43.7 |
| General (% of doctors) | 52.8 |
| Obstetrics and gynaecology (% of doctors) | 36.1 |
| Family medicine (% of doctors) | 4.6 |
| Preventative medicine (% of doctors) | 1.9 |
| Others (% of doctors) | 4.6 |
| Nurse (% of total participants) | 55.5 |
| Pharmacist (% of total participants) | 0.4 |
| Welfare workers (% of total participants) | 0.4 |
| Prior experience counselling for unplanned pregnancies (% with experience) | 63.16 |
| Prior experience treating for unplanned pregnancies (% with experience) | 80.57 |
| Knowledge of regulations of the Medical Council on the Practices Regarding the Termination of Medical Pregnancies (% with knowledge) | 52.46 |
| Manual vacuum aspirations (MVA) | |
| Know of MVA (%) | 65.23 |
| Knowledge of requirements for medical professionals for the use of MVA (%) | 64.00 |
| Seen MVA (%) | 67.21 |
| Used MVA (%) | 50.21 |
| Questions | Pre-Test | Post-Test |
|---|---|---|
| Mean (SD), Median [IQR] | Mean (SD), Median [IQR] | |
| 1. At the present, unplanned pregnancies and unsafe abortions are a major public health problem that should be addressed. | 4.62 (0.50), | 4.76 (0.43), |
| 5 [1] | 5 [0] | |
| 2. In your area, unplanned pregnancies and unsafe abortions are a major public health problem, that should be addressed. | 4.10 (0.71), | 4.39 (0.68), |
| 4 [1] | 4 [1] | |
| 3. One reason for unsafe abortions is the limited options for pregnant women and the societal pressures pregnant women face. | 4.02 (0.78), | 4.64 (0.54), |
| 4 [1] | 5 [1] | |
| 4. Family and society should help unplanned pregnancies. | 4.50 (0.54), | 4.74 (0.46), |
| 5 [1] | 5 [1] | |
| 5. Women with unplanned pregnancies should have the right to decide and choose whether to continue or terminate the pregnancy. | 4.00 (0.82), | 4.61 (0.59), |
| 4 [1] | 5 [1] | |
| 6. Women that need to terminate their pregnancies, according to the criteria set by the Regulations of Medical Council of Thailand, should receive safe abortion, with the same level of services and benefits as other health problems. | 4.38 (0.59), | 4.72 (0.46), |
| 4 [1] | 5 [1] | |
| 7. Doctors and healthcare providers play a major role in addressing unplanned pregnancies and unsafe abortions. | 4.49 (0.54), | 4.72 (0.48), |
| 5 [1] | 5 [1] | |
| 8. You are happy to help, advise and provide consultations regarding abortions and places to obtain safe abortion services for those with unplanned pregnancies. | 4.05 (0.84), | 4.53 (0.58), |
| 4 [1] | 5 [1] | |
| 9. Thailand should allow the sale of medical abortion drugs as well as emergency contraceptives at pharmacies. | 2.38 (1.24), | 3.74 (1.20), |
| 2 [2] | 4 [2] | |
| Average Score of all questions | 4.06 (0.42), | 4.54(0.41), |
| 4 [1.6] | 4.67 [0.6] |
| Characteristics | Attitudes towards Adolescents and Women Experiencing Unplanned Pregnancies, and Unsafe Abortions | Change in Response to Examples of Scenarios on Abortions |
|---|---|---|
| Sex | p = 0.863 | p = 0.217 |
| Female | 0.48 (0.43), 0.44 [0.55] | 0.75 (0.58), 0.71 [0.71] |
| Male | 0.46 (0.38), 0.44 [0.55] | 0.61 (0.40), 0.64 [0.5] |
| Age | p = 0.821 | p = 0.900 |
| Less than 35 | 0.46 (0.44), 0.44 [0.55] | 0.71 (0.52), 0.71 [0.64] |
| More than 35 | 0.49 (0.40), 0.44 [0.55] | 0.74 (0.60), 0.71 [0.64] |
| Career | p = 0.013 * | p < 0.001 * |
| OBGYN | 0.32 (0.38), 0.33 [0.44] | 0.54 (0.46), 0.42 [0.64] |
| Other doctor | 0.46 (0.38), 0.44 [0.44] | 0.59 (0.44), 0.57 [0.57] |
| Non-doctor | 0.53 (0.44), 0.55 [0.66] | 0.84 (0.61), 0.86 [0.71] |
| Knowledge of MVA | p = 0.248 | p = 0.507 |
| Knowledge of regulation | p = 0.004 * | p = 0.189 |
| Prior knowledge | 0.55 (0.43), 0.55 [0.61] | |
| No prior knowledge | 0.42 (0.39), 0.33 [0.55] | |
| Experience in treating | p = 0.071 | p = 1.000 |
| Experience in counselling | p = 0.087 | p = 0.157 |
| Experience in using MVA | p = 0.846 | p = 0.698 |
| (Reference: OBGYN) | Coef. (95% CI) | p-Value |
|---|---|---|
| Non-OBGYN doctor | 0.095 (−0.074, 0.264) | 0.269 |
| Non-doctor | 0.165 (0.006, 0.323) | 0.041 |
| Prior knowledge of regulation | −0.067 (−0.182, 0.047) | 0.247 |
| Experience in treating | −0.102 (−0.236, 0.032) | 0.134 |
| Experience in counselling | 0.002 (−0.002, 0.007) | 0.317 |
| Constant | 0.475 (0.279, 0.671) | 0.000 |
| Questions | Pre-Test | Post-Test |
|---|---|---|
| Mean (SD), Median [IQR] | Mean (SD), Median [IQR] | |
| 1. If the pregnant woman has underlying diseases and the pregnancy poses serious harm to their health or life. | 4.56 (0.59), 5 [1] | 4.85 (0.39), 5 [0] |
| 2. If the pregnant woman has physical or intellectual disabilities hindering their ability to care for themselves. | 4.45 (0.66), 5 [1] | 4.81 (0.49), 5 [0] |
| 3. If the pregnant woman has HIV/AID. | 3.40 (1.23), 3 [3] | 3.74 (1.25), 4 [2] |
| 4. If the pregnant woman has rubella. | 4.03 (0.89), 4 [1] | 4.50 (0.71), 5 [1] |
| 5. If the foetus has anomalies that can result in being physically or intellectually disabled. | 4.31 (0.81), 4 [1] | 4.74 (0.52), 5 [0] |
| 6. If the foetus has genetic disorders or serious diseases. | 4.38 (0.81), 4 [1] | 4.78 (0.49), 5 [0] |
| 7. If the pregnant woman’s mental health is at risk. | 3.71 (0.97), 4 [2] | 4.53 (0.65), 5 [1] |
| 8. If the pregnant woman is under the age of 15. | 3.33 (1.07), 3 [1] | 4.32 (0.83), 5 [1] |
| 9. If the pregnant woman is under the age of 20 and still in school. | 3.01 (1.04), 3 [2] | 3.97 (0.93), 4 [2] |
| 10. If the pregnancy is a result of rape. | 4.34 (0.76), 4 [1] | 4.78 (0.47), 5 [0] |
| 11. If the pregnancy is a result of incest. | 3.39 (1.03), 3 [1] | 4.24 (0.91), 5 [1] |
| 12. If the pregnancy is a result of contraceptive failure. | 2.97 (1.15), 3 [2] | 4.19 (0.87), 4 [1] |
| 13. If the pregnant woman is facing economic problems. | 2.76 (1.08), 3 [1] | 4.11 (0.93), 4 [1] |
| 14. If the pregnant woman is unmarried. | 2.67 (1.11), 3 [1] | 3.91 (0.99), 4 [2] |
| Average Score of all questions | 3.67 (0.64), 3.64 [0.79] | 4.39 (0.53), 4.43 [0.86] |
| (Reference: OBGYN) | Coef. (95% CI) | p-Value |
|---|---|---|
| Non-OBGYN doctor | 0.064 (−0.159, 0.288) | 0.573 |
| Non-doctor | 0.323 (0.112, 0.534) | 0.003 * |
| Prior knowledge of regulation | 0.041 (−0.109, 0.191) | 0.54 |
| Experience in counselling | 0.003 (−0.004, 0.009) | 0.437 |
| Constant | 0.489 (0.227, 0.751) | 0.000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanitya, R.; Marshall, A.I.; Saengruang, N.; Julchoo, S.; Sinam, P.; Suphanchaimat, R.; Phaiyarom, M.; Tangcharoensathien, V.; Boonthai, N.; Chaturachinda, K. Healthcare Providers’ Knowledge and Attitude Towards Abortions in Thailand: A Pre-Post Evaluation of Trainings on Safe Abortion. Int. J. Environ. Res. Public Health 2020, 17, 3198. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093198
Sanitya R, Marshall AI, Saengruang N, Julchoo S, Sinam P, Suphanchaimat R, Phaiyarom M, Tangcharoensathien V, Boonthai N, Chaturachinda K. Healthcare Providers’ Knowledge and Attitude Towards Abortions in Thailand: A Pre-Post Evaluation of Trainings on Safe Abortion. International Journal of Environmental Research and Public Health. 2020; 17(9):3198. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093198
Chicago/Turabian StyleSanitya, Rugsapon, Aniqa Islam Marshall, Nithiwat Saengruang, Sataporn Julchoo, Pigunkaew Sinam, Rapeepong Suphanchaimat, Mathudara Phaiyarom, Viroj Tangcharoensathien, Nongluk Boonthai, and Kamheang Chaturachinda. 2020. "Healthcare Providers’ Knowledge and Attitude Towards Abortions in Thailand: A Pre-Post Evaluation of Trainings on Safe Abortion" International Journal of Environmental Research and Public Health 17, no. 9: 3198. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093198